

Future Health Risk Assessment of Exposure to PM2.5 in Different Age Groups of Children in Northern Thailand


Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of Study Area
2.2. Data of Future PM2.5 Concentration

2.3. Health Risk Assessment

{kind=link}
{kind=link}
{kind=link}
| Factor | Exposure Frequency (EF) (Days/Year) | Exposure Duration (ED) (Years) | Averaging Time (AT) (Days) |
|---|---|---|---|
| Value | 350 | 12 | 4380 |
| Reference | Morakinyo et al. [28]; Olufemi et al. [29] | Morakinyo et al. [28]; Olufemi et al. [29] | Liang et al. [27] |
| Cohort/Age (Years) | Body Weight (kg) | Inhalation (m3/day) |
|---|---|---|
| Infant (<1) | 7.6 | 4.5 |
| 1–2 | 13.0 | 6.8 |
| 3–5 | 18.0 | 8.3 |
| 6–8 | 26.0 | 10 |
| Male | ||
| 9–11 | 36.0 | 14 |
| 12–14 | 50.0 | 15 |
| 15–18 | 66.0 | 17 |
| Female | ||
| 9–11 | 36.0 | 13 |
| 12–14 | 49.0 | 12 |
| 15–18 | 56.0 | 12 |
3. Results
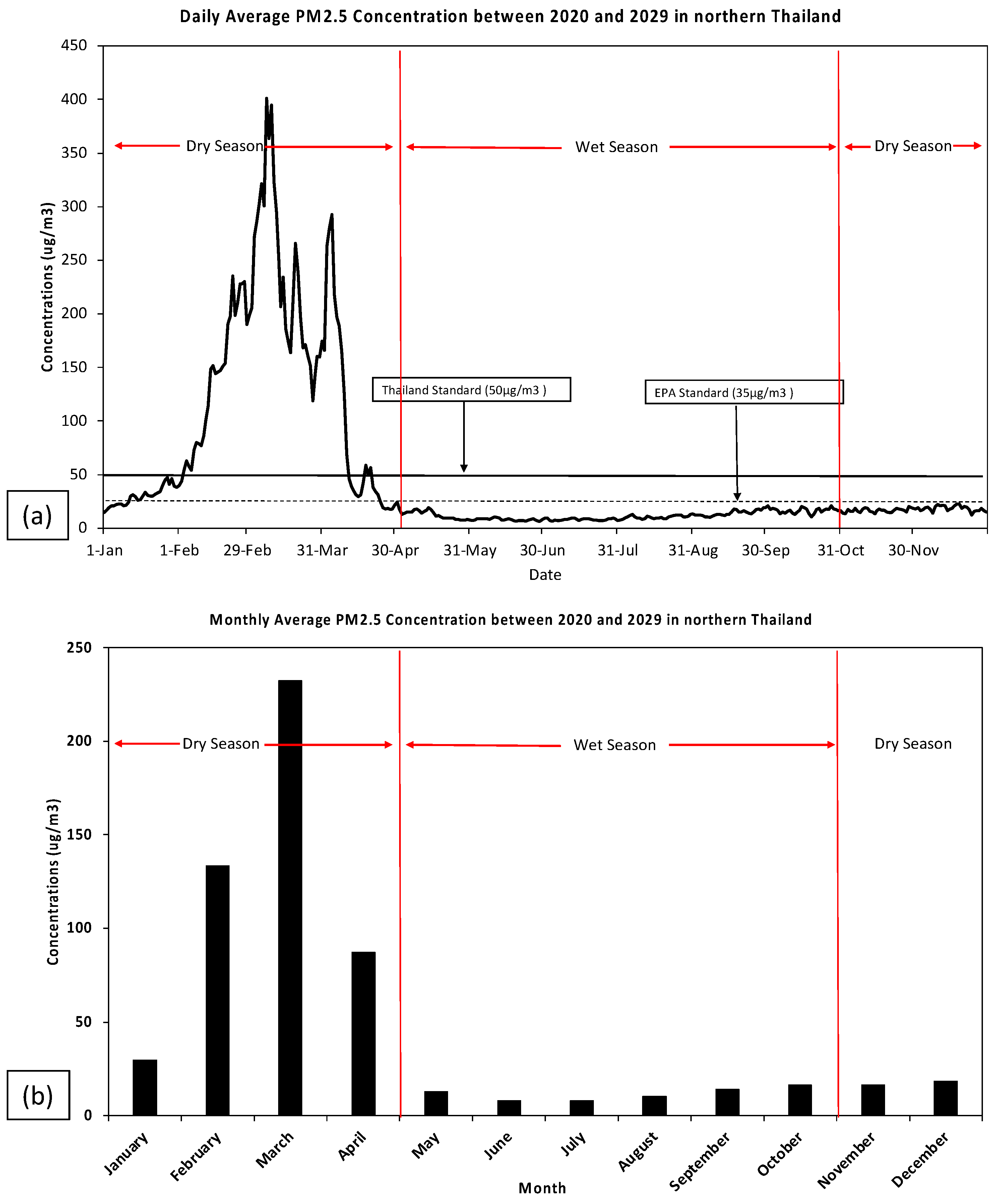
3.1. Situation of PM2.5 Concentrations between 2020 and 2029
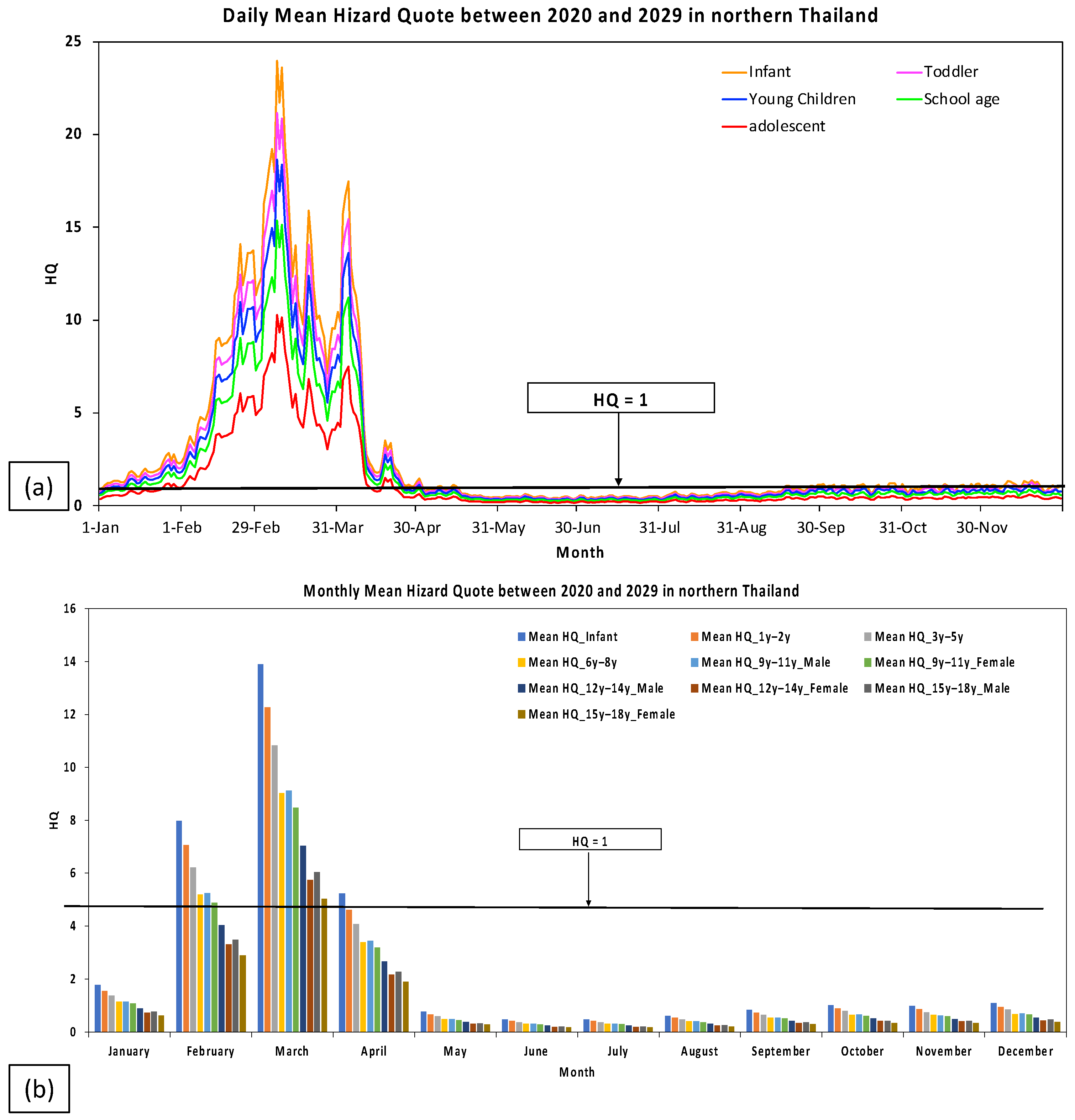
3.2. Hazard Quote in Different Age Groups of Children in Northern Thailand between 2020 and 2029
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amnuaylojaroen, T.; Parasin, N.; Limsakul, A. Health risk assessment of exposure near-future PM2. 5 in Northern Thailand. Air Qual. Atmos. Health 2022, 15, 1963–1979. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, X.; Bae, J. Does trade openness affect CO2 emissions: Evidence from ten newly industrialized countries? Environ. Sci. Pollut. Res. 2017, 24, 17616–17625. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhang, Y.; Zhang, L.; Huang, M.; Zhong, L.; Chen, D.; Wang, X. Trends of outdoor air pollution and the impact on premature mortality in the Pearl River Delta region of southern China during 2006–2015. Sci. Total Environ. 2019, 690, 248–260. [Google Scholar] [CrossRef]
- Lelieveld, J.; Barlas, C.; Giannadaki, D.; Pozzer, A. Model calculated global, regional and megacity premature mortality due to air pollution. Atmos. Chem. Phys. 2013, 13, 7023–7037. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Matsunaga, T.; Yamaguchi, Y.; Zhao, A.; Li, Z.; Gu, X. Long-term trends and spatial patterns of PM2.5-induced premature mortality in South and Southeast Asia from 1999 to 2014. Sci. Total Environ. 2018, 631, 1504–1514. [Google Scholar] [CrossRef]
- Amnuaylojaroen, T.; Inkom, J.; Janta, R.; Surapipith, V. Long range transport of southeast asian PM2.5 pollution to northern Thailand during high biomass burning episodes. Sustainability 2020, 12, 10049. [Google Scholar] [CrossRef]
- Khodmanee, S.; Amnuaylojaroen, T. Impact of biomass burning on ozone, carbon monoxide, and nitrogen dioxide in Northern Thailand. Front. Environ. Sci. 2021, 8, 641877. [Google Scholar] [CrossRef]
- Parasin, N.; Amnuaylojaroen, T.; Saokaew, S. Effect of air pollution on obesity in children: A systematic review and meta-analysis. Children 2021, 8, 327. [Google Scholar] [CrossRef]
- U.S. EPA. Child-Specific Exposure Factors Handbook; EPA: Washington, DC, USA, 2008.
- Liu, J.; Kiesewetter, G.; Klimont, Z.; Cofala, J.; Heyes, C.; Schöpp, W.; Zhu, T.; Cao, G.; Sanabria, A.G.; Sander, R.; et al. Mitigation pathways of air pollution from residential emissions in the Beijing-Tianjin-Hebei region in China. Environ. Int. 2019, 125, 236–244. [Google Scholar] [CrossRef]
- Lien, W.-H.; Owili, P.O.; Muga, M.A.; Lin, T.-H. Ambient particulate matter exposure and under-five and maternal deaths in Asia. Int. J. Environ. Res. Public Health 2019, 16, 3855. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, N.; Junger, W.L.; Romieu, I.; Cifuentes, L.A.; de Leon, A.P.; Vera, J.; Strappa, V.; Hurtado-Díaz, M.; Miranda-Soberanis, V.; Rojas-Bracho, L.; et al. Effects of air pollution on infant and children respiratory mortality in four large Latin-American cities. Environ. Pollut. 2018, 232, 385–391. [Google Scholar] [CrossRef]
- Sarkodie, S.A.; Strezov, V.; Jiang, Y.; Evans, T. Proximate determinants of particulate matter (PM2.5) emission, mortality and life expectancy in Europe, Central Asia, Australia, Canada and the US. Sci. Total Environ. 2019, 683, 489–497. [Google Scholar] [CrossRef]
- Chowdhury, S.; Dey, S.; Smith, K.R. Ambient PM2.5 exposure and expected premature mortality to 2100 in India under climate change scenarios. Nat. Commun. 2018, 9, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huggins, F.E.; Huffman, G.P.; Robertson, J.D. Speciation of elements in NIST particulate matter SRMs 1648 and 1650. J. Hazard. Mater. 2000, 74, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Majestic, B.J.; Schauer, J.J.; Shafer, M.M. Development of a manganese speciation method for atmospheric aerosols in biologically and environmentally relevant fluids. Aerosol Sci. Technol. 2007, 41, 925–933. [Google Scholar] [CrossRef]
- Kulkarni, N.; Grigg, J. Effect of air pollution on children Paediatr. Child Health 2008, 18, 238–243. [Google Scholar] [CrossRef]
- Bruce, N.G.; Dherani, M.K.; Das, J.K.; Balakrishnan, K.; Adair-Rohani, H.; Bhutta, Z.A.; Pope, D. Control of household air pollution for child survival: Estimates for intervention impacts. BMC Public Health 2013, 13, S8. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Xu, X.; Yekeen, T.A.; Zhang, Y.; Chen, A.; Kim, S.S.; Dietrich, K.N.; Ho, S.-M.; Lee, S.-A.; Reponen, T.; et al. Ambient air heavy metals in PM2.5 and potential human health risk assessment in an informal electronic-waste recycling site of China. Aerosol Air Qual. Res. 2016, 16, 388–397. [Google Scholar] [CrossRef] [Green Version]
- Anwar, A.; Ayub, M.; Khan, N.; Flahault, A. Nexus between air pollution and neonatal deaths: A case of Asian countries. Int. J. Environ. Res. Public Health 2019, 16, 4148. [Google Scholar] [CrossRef] [Green Version]
- Amnuaylojaroen, T.; Surapipith, V.; Macatangay, R.C. Projection of the near-future PM2.5 in Northern Peninsular Southeast Asia under RCP8.5. Atmosphere 2022, 13, 305. [Google Scholar] [CrossRef]
- Zheng, N.; Liu, J.; Wang, Q.; Liang, Z. Health risk assessment of heavy metals exposure to street dust in the zinc smelting district, Northeast of China. Sci. Total Environ. 2010, 408, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Yarmohammadi, H.; Poursadeghiyan, M.; Shorabi, Y.; Ebrahimi, M.H.; Rezaei, G.; Biglari, H.; Rostami, R. Risk assessment in a wheat winnowing factory based on ET and BA method. J. Eng. Appl. Sci. 2016, 11, 334–338. [Google Scholar]
- Ghaderpoori, M.; Paydar, M.; Zarei, A.; Alidadi, H.; Najafpoor, A.A.; Gohary, A.H.; Shams, M. Health risk assessment of fluoride in water distribution network of Mashhad, Iran. Hum. Ecol. Risk Assess. Int. J. 2019, 25, 851–862. [Google Scholar] [CrossRef]
- Layton, D.W. Metabolically consistent breathing rates for use in dose assessments. Health Phys. 1993, 64, 22–36. [Google Scholar] [CrossRef]
- Liang, B.; Li, X.-L.; Ma, K.; Liang, S.-X. Pollution characteristics of metal pollutants in PM2.5 and comparison of risk on human health in heating and non-heating seasons in Baoding, China. Ecotoxicol. Environ. Saf. 2019, 170, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Morakinyo, O.M.; Adebowale, A.S.; Mokgobu, M.I.; Mukhola, M.S. Health risk of inhalation exposure to sub-10 µm particulate matter and gaseous pollutants in an urban-industrial area in South Africa: An ecological study. BMJ Open 2017, 7, e013941. [Google Scholar] [CrossRef]
- Olufemi, A.C.; Mji, A.; Mukhola, M.S. Health risks of exposure to air pollutants among students in schools in the vicinities of coal mines. Energy Explor. Exploit. 2019, 37, 1638–1656. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.; Yang, Y.; Xu, Z. PM10 and PM2. 5 and health risk assessment for heavy metals in a typical factory for cathode ray tube television recycling. Environ. Sci. Technol. 2013, 47, 12469–12476. [Google Scholar] [CrossRef]
- Feng, S.; Gao, D.; Liao, F.; Zhou, F.; Wang, X. The health effects of ambient PM2.5 and potential mechanisms. Ecotoxicol. Environ. Saf. 2016, 128, 67–74. [Google Scholar] [CrossRef]
- Militaru, M.; Martinovici, D. Our experience in pediatric sepsis. J. Pediatrului 2005, 8, 29–30. [Google Scholar]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannan, S.; Misra, D.P.; Dvonch, J.T.; Krishnakumar, A. Exposures to airborne particulate matter and adverse perinatal outcomes: A biologically plausible mechanistic framework for exploring potential effect modification by nutrition. Environ. Health Perspect. 2006, 114, 1636–1642. [Google Scholar] [CrossRef]
- Valentino, S.A.; Tarrade, A.; Aioun, J.; Mourier, E.; Richard, C.; Dahirel, M.; Rousseau-Ralliard, D.; Fournier, N.; Aubrière, M.-C.; Lallemand, M.-S.; et al. Maternal exposure to diluted diesel engine exhaust alters placental function and induces intergenerational effects in rabbits. Part. Fibre Toxicol. 2015, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Wick, P.; Malek, A.; Manser, P.; Meili, D.; Maeder-Althaus, X.; Diener, L.; Diener, P.-A.; Zisch, A.; Krug, H.F.; von Mandach, U. Barrier capacity of human placenta for nanosized materials. Environ. Health Perspect. 2010, 118, 432–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, L. Defining critical windows in the development of the human immune system. Hum. Exp. Toxicol. 2002, 21, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Persaud, T.V.N.; Torchia, M.G. Before We are Born E-Book: Essentials of Embryology and Birth Defects with Student Consult Online Access; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Schittny, J.C. Development of the lung. Cell Tissue Res. 2017, 367, 427–444. [Google Scholar] [CrossRef] [Green Version]
- Selevan, S.G.; Kimmel, C.A.; Mendola, P. Identifying critical windows of exposure for children’s health. Environ. Health Perspect. 2000, 108 (Suppl. 3), 451–455. [Google Scholar] [PubMed]
- Xia, T.; Fang, F.; Montgomery, S.; Fang, B.; Wang, C.; Cao, Y. Sex differences in associations of fine particulate matter with non-accidental deaths: An ecological time-series study. Air Qual. Atmos. Health 2021, 14, 863–872. [Google Scholar] [CrossRef]
- Berhane, K.; McConnell, R.; Gilliland, F.; Islam, T.; James Gauderman, W.; Avol, E.; London, S.J.; Rappaport, E.; Margolis, H.G.; Peters, J.M. Sex-specific effects of asthma on pulmonary function in children. Am. J. Respir. Crit. Care Med. 2000, 162, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Clougherty, J.E. A growing role for gender analysis in air pollution epidemiology. Environ. Health Perspect. 2010, 118, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Drevenstedt, G.L.; Crimmins, E.M.; Vasunilashorn, S.; Finch, C.E. The rise and fall of excess male infant mortality. Proc. Natl. Acad. Sci. USA 2008, 105, 5016–5021. [Google Scholar] [CrossRef] [Green Version]
- Torday, J.S.; Nielsen, H.C.; Fencl, M.D.M.; Avery, M.E. Sex differences in fetal lung maturation. Am. Rev. Respir. Dis. 1981, 123, 205–208. [Google Scholar]
- Winckelmans, E.; Vrijens, K.; Tsamou, M.; Janssen, B.G.; Saenen, N.D.; Roels, H.A.; Kleinjans, J.; Lefebvre, W.; Vanpoucke, C.; de Kok, T.M.; et al. Newborn sex-specific transcriptome signatures and gestational exposure to fine particles: Findings from the ENVIRONAGE birth cohort. Environ. Health 2017, 16, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodovici, M.; Bigagli, E. Oxidative stress and air pollution exposure. J. Toxicol. 2011, 2011, 487074. [Google Scholar] [CrossRef]
- Gauderman, W.J.; Vora, H.; McConnell, R.; Berhane, K.; Gilliland, F.; Thomas, D.; Lurmann, F.; Avol, E.; Kunzli, N.; Jerrett, M.; et al. Effect of exposure to traffic on lung development from 10 to 18 years of age: A cohort study. Lancet 2007, 369, 571–577. [Google Scholar] [CrossRef]
- Gehring, U.; Cyrys, J.; Sedlmeir, G.; Brunekreef, B.; Bellander, T.; Fischer, P.; Bauer, C.P.; Reinhardt, D.; Wichmann, H.E.; Heinrich, J. Traffic-related air pollution and respiratory health during the first 2 yrs of life. Eur. Respir. J. 2002, 19, 690–698. [Google Scholar] [CrossRef] [Green Version]
- Peters, J.M.; Avol, E.; Navidi, W.; London, S.J.; Gauderman, W.J.; Lurmann, F.; Linn, W.S.; Margolis, H.; Rappaport, E.; Gong, H.; et al. A study of twelve Southern California communities with differing levels and types of air pollution: I. Prevalence of respiratory morbidity. Am. J. Respir. Crit. Care Med. 1999, 159, 760–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas-Martinez, R.; Perez-Padilla, R.; Olaiz-Fernandez, G.; Mendoza-Alvarado, L.; Moreno-Macias, H.; Fortoul, T.; McDonnell, W.; Loomis, D.; Romieu, I. Lung function growth in children with long-term exposure to air pollutants in Mexico City. Am. J. Respir. Crit. Care Med. 2007, 176, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Becklake, M.R.; Kauffmann, F. Gender differences in airway behaviour over the human life span. Thorax 1999, 54, 1119–1138. [Google Scholar] [CrossRef] [Green Version]
- Polgar, G.; Weng, T.R. The functional development of the respiratory system: From the period of gestation to adulthood. Am. Rev. Respir. Dis. 1979, 120, 625–695. [Google Scholar]
- Phairuang, W.; Suwattiga, P.; Hongtieab, S.; Inerb, M.; Furuuchi, M.; Hata, M. Characteristics, sources, and health risks of ambient nanoparticles (PM0.1) bound metal in Bangkok Thailand. Atmos. Environ. X 2021, 12, 100141. [Google Scholar] [CrossRef]
- Phairuang, W.; Inerb, M.; Hata, M.; Furuuchi, M. Characteristics of trace elements bound to ambient nanoparticles (PM0.1) and a health risk assessment in southern Thailand. J. Hazard. Mater. 2022, 425, 127986. [Google Scholar] [CrossRef] [PubMed]
- Insian, W.; Yabueng, N.; Wiriya, W.; Chantara, S. Size-fractionated PM- bound PAHs in urban and rural atmospheres of Northern Thailand for respiratory health risk assessment. Environ. Pollut. 2022, 293, 118488. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhao, X.; Wang, J.; Yin, B.; Geng, C.; Niu, D.; Yang, W.; Yu, H.; Li, W. Chemical composition of PM2.5 and its impact on inhalation health risk evaluation in a city with light industry in central China. Atmosphere 2020, 11, 340. [Google Scholar] [CrossRef] [Green Version]


| Month | Mean | Max | Min | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Infants | Toddlers | Young Children | School Age | Adolescents | Infants | Toddlers | Young Children | School Age | Adolescents | Infants | Toddlers | Young Children | School Age | Adolescents | |
| January | 1.77 | 1.57 | 1.38 | 1.14 | 0.76 | 2.83 | 2.50 | 2.21 | 1.82 | 1.22 | 0.86 | 0.76 | 0.67 | 0.55 | 0.37 |
| February | 7.98 | 7.05 | 6.21 | 5.12 | 3.43 | 14.07 | 12.43 | 10.96 | 9.03 | 6.04 | 2.37 | 2.09 | 1.84 | 1.52 | 1.02 |
| March | 13.89 | 12.27 | 10.82 | 8.91 | 5.96 | 23.96 | 21.16 | 18.66 | 15.37 | 10.28 | 7.12 | 6.29 | 5.55 | 4.57 | 3.06 |
| April | 5.23 | 4.62 | 4.07 | 3.36 | 2.25 | 17.48 | 15.44 | 13.61 | 11.21 | 7.50 | 1.05 | 0.93 | 0.82 | 0.67 | 0.45 |
| May | 0.77 | 0.68 | 0.60 | 0.49 | 0.33 | 1.47 | 1.29 | 1.14 | 0.94 | 0.63 | 0.44 | 0.39 | 0.34 | 0.28 | 0.19 |
| June | 0.48 | 0.42 | 0.37 | 0.31 | 0.21 | 0.63 | 0.56 | 0.49 | 0.41 | 0.27 | 0.38 | 0.34 | 0.30 | 0.24 | 0.16 |
| July | 0.49 | 0.43 | 0.38 | 0.31 | 0.21 | 0.57 | 0.50 | 0.44 | 0.37 | 0.24 | 0.39 | 0.34 | 0.30 | 0.25 | 0.17 |
| August | 0.62 | 0.55 | 0.48 | 0.40 | 0.27 | 0.80 | 0.70 | 0.62 | 0.51 | 0.34 | 0.44 | 0.39 | 0.34 | 0.28 | 0.19 |
| September | 0.84 | 0.74 | 0.66 | 0.54 | 0.36 | 1.15 | 1.01 | 0.89 | 0.73 | 0.49 | 0.58 | 0.51 | 0.45 | 0.37 | 0.25 |
| October | 1.02 | 0.89 | 0.81 | 0.65 | 0.43 | 1.20 | 1.03 | 1.05 | 0.79 | 0.53 | 0.67 | 0.67 | 0.57 | 0.48 | 0.32 |
| November | 0.99 | 0.88 | 0.76 | 0.64 | 0.42 | 1.20 | 1.10 | 0.97 | 0.74 | 0.49 | 0.65 | 0.58 | 0.54 | 0.49 | 0.34 |
| December | 1.10 | 0.95 | 0.86 | 0.69 | 0.47 | 1.38 | 1.27 | 1.12 | 0.86 | 0.59 | 0.71 | 0.70 | 0.69 | 0.53 | 0.35 |
| Mean | 2.93 ± 1.20 | 2.59 ± 1.06 | 2.28 ± 0.93 | 1.88 ± 0.77 | 1.26 ± 0.51 | 5.56 ± 2.34 | 4.92 ± 2.07 | 4.35 ± 1.82 | 3.56 ± 1.50 | 2.39 ± 1.01 | 1.31 ± 0.55 | 1.17 ± 0.49 | 1.03 ± 0.43 | 0.85 ± 0.35 | 0.57 ± 0.24 |
| Month | <1 y | 1 y–2 y | 3 y–5 y | 6 y–8 y | 9 y–11 y | 12 y–14 y | 15 y–18 y | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |||||
| January | 1.77 | 1.57 | 1.38 | 1.15 | 1.16 | 1.08 | 0.90 | 0.73 | 0.77 | 0.64 |
| February | 7.98 | 7.05 | 6.21 | 5.18 | 5.24 | 4.87 | 4.04 | 3.30 | 3.47 | 2.89 |
| March | 13.89 | 12.27 | 10.82 | 9.02 | 9.12 | 8.47 | 7.04 | 5.74 | 6.04 | 5.03 |
| April | 5.23 | 4.62 | 4.07 | 3.40 | 3.44 | 3.19 | 2.65 | 2.16 | 2.28 | 1.89 |
| May | 0.77 | 0.68 | 0.60 | 0.50 | 0.50 | 0.47 | 0.39 | 0.32 | 0.33 | 0.28 |
| June | 0.48 | 0.42 | 0.37 | 0.31 | 0.32 | 0.29 | 0.24 | 0.20 | 0.21 | 0.17 |
| July | 0.49 | 0.43 | 0.38 | 0.32 | 0.32 | 0.30 | 0.25 | 0.20 | 0.21 | 0.18 |
| August | 0.62 | 0.55 | 0.48 | 0.40 | 0.41 | 0.38 | 0.31 | 0.26 | 0.27 | 0.22 |
| September | 0.84 | 0.74 | 0.66 | 0.55 | 0.55 | 0.51 | 0.43 | 0.35 | 0.37 | 0.31 |
| October | 1.02 | 0.89 | 0.81 | 0.65 | 0.68 | 0.62 | 0.51 | 0.42 | 0.43 | 0.36 |
| November | 0.99 | 0.88 | 0.76 | 0.65 | 0.64 | 0.60 | 0.50 | 0.41 | 0.43 | 0.35 |
| December | 1.10 | 0.95 | 0.86 | 0.69 | 0.70 | 0.66 | 0.55 | 0.44 | 0.48 | 0.40 |
| Mean | 2.93 ± 1.20 | 2.59 ± 1.06 | 2.28 ± 0.93 | 1.90 ± 0.78 | 1.92 ± 0.79 | 1.79 ± 0.73 | 1.48 ± 0.61 | 1.21 ± 0.50 | 1.27 ± 0.52 | 1.06 ± 0.43 |
| Month | <1 y | 1 y–2 y | 3 y–5 y | 6 y–8 y | 9 y–11 y | 12 y–14 y | 15 y–18 y | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |||||
| January | 0.86 | 0.76 | 0.67 | 0.56 | 0.57 | 0.53 | 0.44 | 0.36 | 0.38 | 0.31 |
| February | 2.37 | 2.09 | 1.84 | 1.54 | 1.55 | 1.44 | 1.20 | 0.98 | 1.03 | 0.86 |
| March | 7.12 | 6.29 | 5.55 | 4.63 | 4.68 | 4.34 | 3.61 | 2.95 | 3.10 | 2.58 |
| April | 1.05 | 0.93 | 0.82 | 0.68 | 0.69 | 0.64 | 0.53 | 0.43 | 0.46 | 0.38 |
| May | 0.44 | 0.39 | 0.34 | 0.29 | 0.29 | 0.27 | 0.22 | 0.18 | 0.19 | 0.16 |
| June | 0.38 | 0.34 | 0.30 | 0.25 | 0.25 | 0.23 | 0.19 | 0.16 | 0.17 | 0.14 |
| July | 0.39 | 0.34 | 0.30 | 0.25 | 0.25 | 0.24 | 0.20 | 0.16 | 0.17 | 0.14 |
| August | 0.44 | 0.39 | 0.34 | 0.29 | 0.29 | 0.27 | 0.22 | 0.18 | 0.19 | 0.16 |
| September | 0.58 | 0.51 | 0.45 | 0.38 | 0.38 | 0.35 | 0.29 | 0.24 | 0.25 | 0.21 |
| October | 0.67 | 0.67 | 0.57 | 0.46 | 0.47 | 0.46 | 0.33 | 0.30 | 0.33 | 0.26 |
| November | 0.65 | 0.58 | 0.54 | 0.51 | 0.47 | 0.47 | 0.39 | 0.32 | 0.30 | 0.28 |
| December | 0.71 | 0.70 | 0.69 | 0.55 | 0.50 | 0.47 | 0.43 | 0.33 | 0.36 | 0.28 |
| Mean | 1.31 ± 2.34 | 1.17 ± 2.07 | 1.03 ± 1.82 | 0.86 ± 1.52 | 0.87 ± 1.54 | 0.81 ± 1.43 | 0.67 ± 1.19 | 0.55 ± 0.97 | 0.58 ± 1.02 | 0.48 ± 0.85 |
| Month | <1 y | 1 y–2 y | 3 y–5 y | 6 y–8 y | 9 y–11 y | 12 y–14 y | 15 y–18 y | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |||||
| January | 2.83 | 2.50 | 2.21 | 1.84 | 1.86 | 1.73 | 1.43 | 1.17 | 1.23 | 1.02 |
| February | 14.07 | 12.43 | 10.96 | 9.14 | 9.24 | 8.58 | 7.13 | 5.82 | 6.12 | 5.09 |
| March | 23.96 | 21.16 | 18.66 | 15.56 | 15.73 | 14.61 | 12.14 | 9.91 | 10.42 | 8.67 |
| April | 17.48 | 15.44 | 13.61 | 11.35 | 11.48 | 10.66 | 8.86 | 7.23 | 7.60 | 6.33 |
| May | 1.47 | 1.29 | 1.14 | 0.95 | 0.96 | 0.89 | 0.74 | 0.61 | 0.64 | 0.53 |
| June | 0.63 | 0.56 | 0.49 | 0.41 | 0.41 | 0.39 | 0.32 | 0.26 | 0.27 | 0.23 |
| July | 0.57 | 0.50 | 0.44 | 0.37 | 0.37 | 0.35 | 0.29 | 0.24 | 0.25 | 0.21 |
| August | 0.80 | 0.70 | 0.62 | 0.52 | 0.52 | 0.49 | 0.40 | 0.33 | 0.35 | 0.29 |
| September | 1.15 | 1.01 | 0.89 | 0.74 | 0.75 | 0.70 | 0.58 | 0.47 | 0.50 | 0.41 |
| October | 1.20 | 1.03 | 1.05 | 0.83 | 0.84 | 0.76 | 0.64 | 0.50 | 0.56 | 0.48 |
| November | 1.20 | 1.10 | 0.97 | 0.79 | 0.77 | 0.78 | 0.61 | 0.49 | 0.51 | 0.44 |
| December | 1.38 | 1.27 | 1.12 | 0.86 | 0.90 | 0.82 | 0.75 | 0.56 | 0.64 | 0.50 |
| Mean | 5.56 ± 0.55 | 4.92 ± 0.49 | 4.35 ± 0.43 | 3.61 ± 0.36 | 3.66 ± 0.36 | 3.40 ± 0.33 | 2.82 ± 0.28 | 2.30 ± 0.23 | 2.42 ± 0.24 | 2.02 ± 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amnuaylojaroen, T.; Parasin, N. Future Health Risk Assessment of Exposure to PM2.5 in Different Age Groups of Children in Northern Thailand. Toxics 2023, 11, 291. https://doi.org/10.3390/toxics11030291
Amnuaylojaroen T, Parasin N. Future Health Risk Assessment of Exposure to PM2.5 in Different Age Groups of Children in Northern Thailand. Toxics. 2023; 11(3):291. https://doi.org/10.3390/toxics11030291
Chicago/Turabian StyleAmnuaylojaroen, Teerachai, and Nichapa Parasin. 2023. "Future Health Risk Assessment of Exposure to PM2.5 in Different Age Groups of Children in Northern Thailand" Toxics 11, no. 3: 291. https://doi.org/10.3390/toxics11030291
APA StyleAmnuaylojaroen, T., & Parasin, N. (2023). Future Health Risk Assessment of Exposure to PM2.5 in Different Age Groups of Children in Northern Thailand. Toxics, 11(3), 291. https://doi.org/10.3390/toxics11030291