
Firefighters’ Occupational Exposure in Preparation for Wildfire Season: Addressing Biological Impact

 , , ,
, , ,  ,
,  ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Particulate Matter Monitoring
2.3. Inhalation Dose Assessment
2.4. BMCyt Assay
2.4.1. Reagents
2.4.2. Collection of Exfoliated Buccal Mucosa
2.4.3. BMCyt Assay
2.5. Statistical Analysis
3. Results
3.1. Population Characterization
3.2. PM Inhaled Doses vs. Effect Biomarker
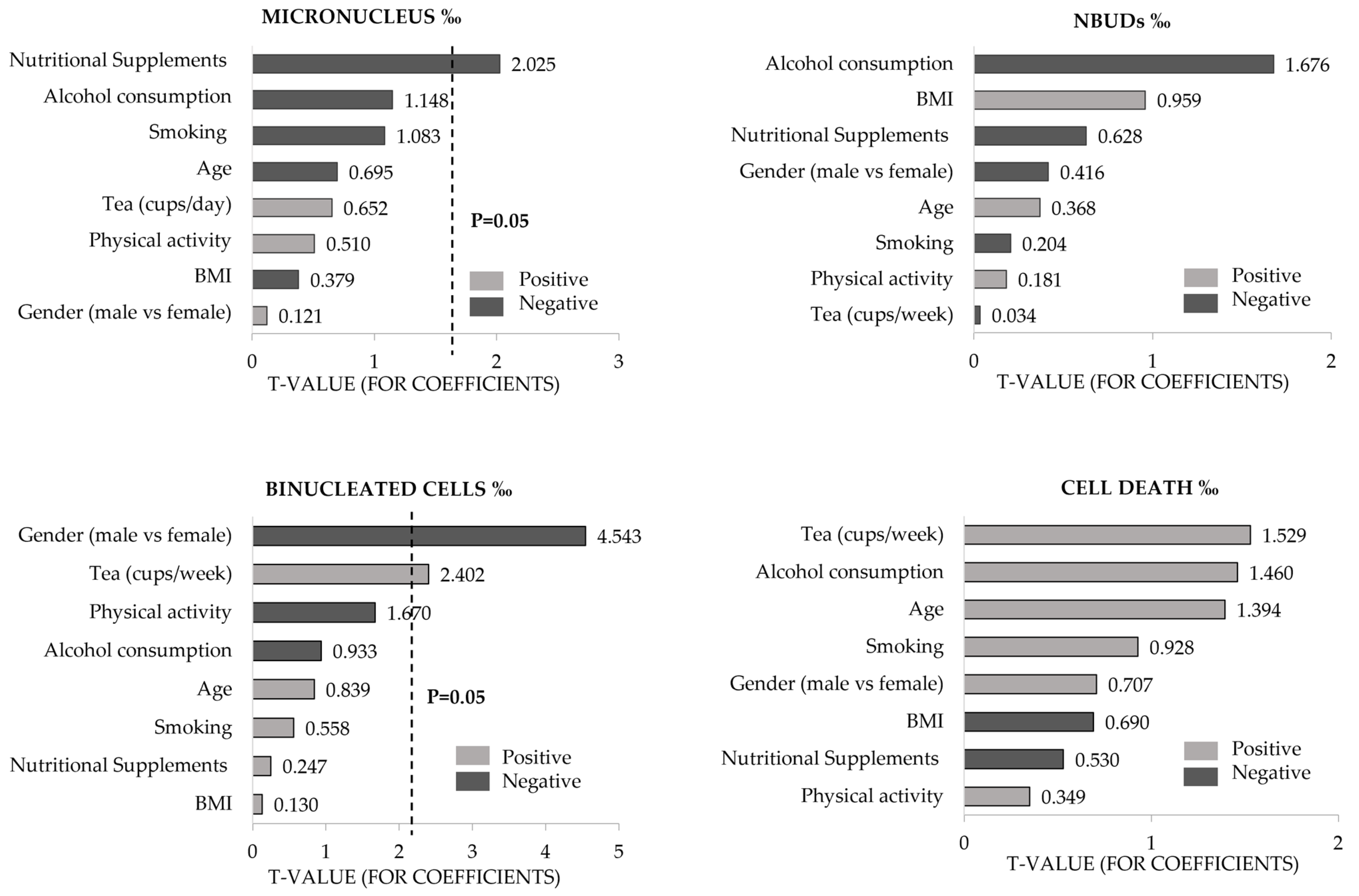
3.3. Influence of Demographic, Occupational, and Lifestyle Variables on Effect Biomarker Endpoints
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Demers, P.A.; DeMarini, D.M.; Fent, K.W.; Glass, D.C.; Hansen, J.; Adetona, O.; Andersen, M.H.; Freeman, L.E.; Caban-Martinez, A.J.; Robert, D.; et al. Carcinogenicity of occupational exposure as a firefighter. Lancet Oncol. 2022, 23, 985–986. [Google Scholar] [CrossRef]
- IARC. Occupational Exposure as a Firefighter. In IARC Monographs on the Identification of Carcinogenic Hazards to Humans; International Agency for Research on Cancer: Lyon, France, 2023; Volume 132, pp. 1–730. [Google Scholar]
- Esteves, F.; Madureira, J.; Teixeira, J.P.; Costa, S. The Role of Biomarkers in the Assessment of Potential Health Risks of Wildland Firefighters’ Occupational Exposure: An Overview. In Essential Guide to Occupational Exposure; Morais, S., Oliveira, M., Rodrigues, F., Eds.; Nova Science Publishers, Inc.: New York, NY, USA, 2022. [Google Scholar]
- Bott, R.C.; Kirk, K.M.; Logan, M.B.; Reid, D.A. Diesel particulate matter and polycyclic aromatic hydrocarbons in fire stations. Environ. Sci. Process Impacts 2017, 19, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Santibáñez-Andrade, M.; Quezada-Maldonado, E.M.; Osornio-Vargas, Á.; Sánchez-Pérez, Y.; García-Cuellar, C.M. Air pollution and genomic instability: The role of particulate matter in lung carcinogenesis. Environ. Pollut. 2017, 229, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Kabir, E.; Kabir, S. A review on the human health impact of airborne particulate matter. Environ. Int. 2015, 74, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Von Klot, S.; Peters, A.; Aalto, P.; Bellander, T.; Berglind, N.; D’Ippoliti, D.; Elosua, R.; Hörmann, A.; Kulmala, M.; Lanki, T.; et al. Ambient air pollution is associated with increased risk of hospital cardiac readmissions of myocardial infarction survivors in five European cities. Circulation 2005, 112, 3073–3079. [Google Scholar] [CrossRef]
- Mott, J.A.; Meyer, P.; Mannino, D.; Redd, S.C.; Smith, E.M.; Gotway-Crawford, C.; Chase, E. Wildland forest fire smoke: Health effects and intervention evaluation, Hoopa, California, 1999. West J. Med. 2002, 176, 157. [Google Scholar] [CrossRef]
- Cascio, W.E. Wildland fire smoke and human health. Sci. Total Environ. 2018, 624, 586–595. [Google Scholar] [CrossRef]
- Du, Y.; Xu, X.; Chu, M.; Guo, Y.; Wang, J. Air particulate matter and cardiovascular disease: The epidemiological, biomedical and clinical evidence. J. Thorac. Dis. 2016, 8, E8. [Google Scholar]
- Oliveira, M.; Slezakova, K.; Alves, M.J.; Fernandes, A.; Teixeira, J.P.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Polycyclic aromatic hydrocarbons at fire stations: Firefighters’ exposure monitoring and biomonitoring, and assessment of the contribution to total internal dose. J. Hazard. Mater. 2017, 323, 184–194. [Google Scholar] [CrossRef]
- Rogula-Kozłowska, W.; Bralewska, K.; Rogula-Kopiec, P.; Makowski, R.; Majder-Łopatka, M.; Łukawski, A.; Brandyk, A.; Majewski, G. Respirable particles and polycyclic aromatic hydrocarbons at two Polish fire stations. Build. Environ. 2020, 184, 107255. [Google Scholar] [CrossRef]
- Sparer, E.H.; Prendergast, D.; Apell, J.N.; Bartzak, M.R.; Wagner, G.R.; Adamkiewicz, G.; Hart, J.E.; Sorensen, G. Assessment of ambient exposures firefighters encounter while at the fire station: An exploratory study. J. Occup. Environ. Med. 2017, 59, 1017. [Google Scholar] [CrossRef]
- Bolognesi, C. Genotoxicity of pesticides: A review of human biomonitoring studies. Mutat. Res./Rev. Mutat. Res. 2003, 543, 251–272. [Google Scholar] [CrossRef]
- Gajski, G.; Gerić, M.; Oreščanin, V.; Garaj-Vrhovac, V. Cytokinesis-block micronucleus cytome assay parameters in peripheral blood lymphocytes of the general population: Contribution of age, sex, seasonal variations and lifestyle factors. Ecotoxicol. Environ. Saf. 2018, 148, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Hopf, N.B.; Bolognesi, C.; Danuser, B.; Wild, P. Biological monitoring of workers exposed to carcinogens using the buccal micronucleus approach: A systematic review and meta-analysis. Mutat. Res./Rev. Mutat. Res. 2019, 781, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Albertini, R.J.; Anderson, D.; Douglas, G.R.; Hagmar, L.; Hemminki, K.; Merlo, F.; Natarajan, A.T.; Norppa, H.; Shuker, D.E.; Tice, R.; et al. IPCS guidelines for the monitoring of genotoxic effects of carcinogens in humans. Mutat. Res./Rev. Mutat. Res. 2000, 463, 111–172. [Google Scholar] [CrossRef]
- Torres-Bugarín, O.; Ramos-Ibarra, M.L. Utilidad de la prueba de micronúcleos y anormalidades nucleares en células exfoliadas de mucosa oral en la evaluación de daño genotóxico y citotóxico. Int. J. Morphol. 2013, 31, 650–657. [Google Scholar] [CrossRef]
- Ceppi, M.; Biasotti, B.; Fenech, M.; Bonassi, S. Human population studies with the exfoliated buccal micronucleus assay: Statistical and epidemiological issues. Mutat. Res./Rev. Mutat. Res. 2010, 705, 11–19. [Google Scholar] [CrossRef]
- Nersesyan, A.; Kundi, M.; Fenech, M.; Stopper, H.; da Silva, J.; Bolognesi, C.; Mišík, M.; Knasmueller, S. Recommendations and quality criteria for micronucleus studies with humans. Mutat. Res./Rev. Mutat. Res. 2022, 789, 108410. [Google Scholar] [CrossRef] [PubMed]
- Esteban, M.; Castaño, A. Non-invasive matrices in human biomonitoring: A review. Environ. Int. 2009, 35, 438–449. [Google Scholar] [CrossRef]
- Costa, S.; Brandão, F.; Coelho, M.; Costa, C.; Coelho, P.; Silva, S.; Porto, B.; Teixeira, J.P. Micronucleus frequencies in lymphocytes and buccal cells in formaldehyde exposed workers. WIT Trans. Biomed. Health 2013, 16, 83–94. [Google Scholar]
- Thomas, P.; Holland, N.; Bolognesi, C.; Kirsch-Volders, M.; Bonassi, S.; Zeiger, E.; Knasmueller, S.; Fenech, M. Buccal micronucleus cytome assay. Nat. Protoc. 2009, 4, 825. [Google Scholar] [CrossRef] [PubMed]
- Bolognesi, C.; Knasmueller, S.; Nersesyan, A.; Thomas, P.; Fenech, M. The HUMNxl scoring criteria for different cell types and nuclear anomalies in the buccal micronucleus cytome assay–An update and expanded photogallery. Mutat. Res./Rev. Mutat. Res. 2013, 753, 100–113. [Google Scholar] [CrossRef] [PubMed]
- WMA. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.R. The Declaration of Helsinki and public health. Bull. World Health Organ. 2008, 86, 650–652. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, S.; Li, Y. Modelling of the indoor environment–particle dispersion and deposition. Indoor Air. 1998, 8, 113–122. [Google Scholar] [CrossRef]
- Jin, H.; He, C.; Lu, L.; Fan, J. Numerical investigation of the wall effect on airborne particle dispersion in a test chamber. Aerosol Air Qual. Res. 2013, 13, 786–794. [Google Scholar] [CrossRef]
- Rivas, I.; Mazaheri, M.; Viana, M.; Moreno, T.; Clifford, S.; He, C.; Bischof, O.F.; Martins, V.; Reche, C.; Alastuey, A. Identification of technical problems affecting performance of DustTrak DRX aerosol monitors. Sci. Total Environ. 2017, 584, 849–855. [Google Scholar] [CrossRef]
- Slezakova, K.; Peixoto, C.; Oliveira, M.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Indoor particulate pollution in fitness centres with emphasis on ultrafine particles. Environ. Pollut. 2018, 233, 180–193. [Google Scholar] [CrossRef]
- USEPA. Exposure Factors Handbook 2011 Edition (Final); U.S. Environmental Protection Agency: Washingtom, DC, USA, 2011.
- World Health Organization (WHO). Body Mass Index—BMI. 2022. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 20 October 2022).
- CDC. Adult Tobacco Use Information—Glossary. Center for Disease Prevention and Control. 2017. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 25 October 2023).
- Slezakova, K.; Esteves, F.; Vaz, J.; Alves, M.J.; Madureira, J.; Costa, S.; Fernandes, A.; Teixeira, J.P.; Morais, S.; Pereira, M.C. Occupational Exposure of Firefighters in Non-fire Settings. In Occupational and Environmental Safety and Health IV; Springer: Berlin/Heidelberg, Germany, 2022; pp. 79–88. [Google Scholar]
- O’Callaghan-Gordo, C.; Fthenou, F.; Pedersen, M.; Espinosa, A.; Chatzi, L.; Beelen, R.; Chalkiadaki, G.; Decordier, I.; Hoek, G.; Merlo, D.F.; et al. Outdoor air pollution exposures and micronuclei frequencies in lymphocytes from pregnant women and newborns in Crete, Greece (Rhea cohort). Environ. Res. 2015, 143, 170–176. [Google Scholar] [CrossRef]
- Secretaria de Estado da Saúde e Ambiente e Ação Climática. Portaria No. 138-G/2021; Diário da República: Lisbon, Portugal, 2021.
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2. 5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide: Executive Summary; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240034228. [Google Scholar]
- Bonassi, S.; Coskun, E.; Ceppi, M.; Lando, C.; Bolognesi, C.; Burgaz, S.; Holland, N.; Kirsh-Volders, M.; Knasmueller, S.; Cavallo, D.; et al. The HUman MicroNucleus project on eXfoLiated buccal cells (HUMNXL): The role of life-style, host factors, occupational exposures, health status, and assay protocol. Mutat. Res./Rev. Mutat. Res. 2011, 728, 88–97. [Google Scholar] [CrossRef]
- Bolognesi, C.; Bonelli, L.; Compalati, A.; Ferla, V.; Stagnaro, L.; Ubezio, G.; Bruzzi, P. “Normal values” for the lymphocyte cytokinesis-block micronucleus cytome parameters: Repeatability and reproducibility in a healthy reference population. Sci. Total Environ. 2019, 652, 513–522. [Google Scholar] [CrossRef]
- Bolognesi, C.; Bruzzone, M.; Ceppi, M.; Kirsch-Volders, M. The lymphocyte cytokinesis block micronucleus test in human populations occupationally exposed to vinyl chloride: A systematic review and meta-analysis. Mutat. Res./Rev. Mutat. Res. 2017, 774, 1–11. [Google Scholar] [CrossRef]
- Ceppi, M.; Gallo, F.; Bonassi, S. Study design and statistical analysis of data in human population studies with the micronucleus assay. Mutagenesis 2011, 26, 247–252. [Google Scholar] [CrossRef]
- Hopf, N.B.; Danuser, B.; Bolognesi, C.; Wild, P. Age related micronuclei frequency ranges in buccal and nasal cells in a healthy population. Environ. Res. 2020, 180, 108824. [Google Scholar] [CrossRef]
- Haveric, A.; Haveric, S.; Ibrulj, S. Micronuclei frequencies in peripheral blood and buccal exfoliated cells of young smokers and non-smokers. Toxicol. Mech. Methods 2010, 20, 260–266. [Google Scholar] [CrossRef]
- Ferraz, G.A.; Neto, A.O.C.; Cerqueira, E.M.M.; Meireles, J.R.C. Effects of age on the frequency of micronuclei and degenerative nuclear abnormalities. Rev. Bras. Geriatr. E Gerontol. 2016, 19, 627–634. [Google Scholar] [CrossRef]
- Burgaz, S.; Karahalil, B.; Bayrak, P.; Taşkin, L.; Yavuzaslan, F.; Bökesoy, I.; Anzion, R.B.; Bos, R.P.; Platin, N. Urinary cyclophosphamide excretion and micronuclei frequencies in peripheral lymphocytes and in exfoliated buccal epithelial cells of nurses handling antineoplastics. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 1999, 439, 97–104. [Google Scholar] [CrossRef]
- Perroni, F.; Cardinali, L.; Cignitti, L.; Gobbi, E.; Grugni, F.; Amatori, S.; Rocchi, M.B.L.; Grandinetti, L.; Lunetta, F.; Stocchi, V.; et al. Are there sex differences in physiological parameters and reaction time responses to overload in firefighters? PLoS ONE 2021, 16, e0249559. [Google Scholar] [CrossRef] [PubMed]
- Idolo, A.; Grassi, T.; Bagordo, F.; Panico, A.; De Giorgi, M.; Serio, F.; Guido, M.; Piscitelli, P.; De Filippis, G.; Raho, A. Micronuclei in exfoliated buccal cells of children living in a cluster area of Salento (Southern Italy) with a high incidence of lung cancer: The IMP. AIR Study. Int. J. Environ. Res. Public. Health 2018, 15, 1659. [Google Scholar] [CrossRef] [PubMed]
- Ernst, B.; Setayesh, T.; Nersesyan, A.; Kundi, M.; Fenech, M.; Bolognesi, C.; Mišík, M.; Ghane, M.; Mousavi, S.F.; Knasmüller, S. Investigations concerning the impact of consumption of hot beverages on acute cytotoxic and genotoxic effects in oral mucosa cells. Sci. Rep. 2021, 11, 23014. [Google Scholar] [CrossRef] [PubMed]
- Pappas, R.; Polzin, G.M.; Zhang, L.; Watson, C.H.; Paschal, D.C.; Ashley, D.L. Cadmium, lead, and thallium in mainstream tobacco smoke particulate. Food Chem. Toxicol. 2006, 44, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Bloching, M.; Hofmann, A.; Lautenschläger, C.; Berghaus, A.; Grummt, T. Exfoliative cytology of normal buccal mucosa to predict the relative risk of cancer in the upper aerodigestive tract using the MN-assay. Oral. Oncol. 2000, 36, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Lucero, L.; Pastor, S.; Suárez, S.; Gómez, C.; Parrón, T.; Creus, A.; Marcos, R. Cytogenetic biomonitoring of Spanish greenhouse workers exposed to pesticides: Micronuclei analysis in peripheral blood lymphocytes and buccal epithelial cells. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2000, 464, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Bonassi, S.; Neri, M.; Lando, C.; Ceppi, M.; Lin, Y.; Chang, W.; Holland, N.; Kirsch-Volders, M.; Zeiger, E.; Fenech, M. Effect of smoking habit on the frequency of micronuclei in human lymphocytes: Results from the Human MicroNucleus project. Mutat. Res./Rev. Mutat. Res. 2003, 543, 155–166. [Google Scholar] [CrossRef]
- Fenech, M.; Bonassi, S. The effect of age, gender, diet and lifestyle on DNA damage measured using micronucleus frequency in human peripheral blood lymphocytes. Mutagenesis 2011, 26, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.; Linhares, D.; Amaral, A.F.S.; Rodrigues, A.S. Exposure of thermoelectric power-plant workers to volatile organic compounds from fuel oil: Genotoxic and cytotoxic effects in buccal epithelial cells. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2012, 747, 197–201. [Google Scholar] [CrossRef]
- Hallare, A.; Gervasio, M.K.R.; Gervasio, P.L.G.; Acacio-Claro, P.J.B. Monitoring genotoxicity among gasoline station attendants and traffic enforcers in the City of Manila using the micronucleus assay with exfoliated epithelial cells. Environ. Monit. Assess. 2009, 156, 331–341. [Google Scholar] [CrossRef]
- Martínez-Valenzuela, C.; Gómez-Arroyo, S.; Villalobos-Pietrini, R.; Waliszewski, S.; Calderón-Segura, M.E.; Félix-Gastélum, R.; Alvarez-Torres, A. Genotoxic biomonitoring of agricultural workers exposed to pesticides in the north of Sinaloa State, Mexico. Environ. Int. 2009, 35, 1155–1159. [Google Scholar] [CrossRef]
- Çelik, A.; Çavaş, T.; Ergene-Gözükara, S. Cytogenetic biomonitoring in petrol station attendants: Micronucleus test in exfoliated buccal cells. Mutagenesis 2003, 18, 417–421. [Google Scholar] [CrossRef]
- Corrêa, N.S.; Bassan, J.S.; Cunha, C.J.; Fernández, R.R.; Bachettini, P.S.; Garcias, G.L.; Martino-Roch, M.G. Monitoring the genotoxic action in shoe workers by micronucleus test, Pelotas, Rio Grande do Sul State/Monitoramento da acao genotoxica em trabalhadores de sapatarias atraves do teste de micronucleos, Pelotas, Rio Grande do Sul. Ciência Saúde Coletiva 2009, 14, 2251–2261. [Google Scholar] [CrossRef]
- IARC. Drinking Coffee, Mate, and Very Hot Beverages. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Research on Cancer: Lyon, France, 2018; Volume 116. [Google Scholar]
- Iko Afé, O.H.; Kpoclou, Y.E.; Douny, C.; Anihouvi, V.B.; Igout, A.; Mahillon, J.; Hounhouigan, D.J.; Scippo, M.-L. Chemical hazards in smoked meat and fish. Food Sci. Nutr. 2021, 9, 6903–6922. [Google Scholar] [CrossRef] [PubMed]
- Fenech, M.; Baghurst, P.; Luderer, W.; Turner, J.; Record, S.; Ceppi, M.; Bonassi, S. Low intake of calcium, folate, nicotinic acid, vitamin E, retinol, β-carotene and high intake of pantothenic acid, biotin and riboflavin are significantly associated with increased genome instability—Results from a dietary intake and micronucleus index survey in South Australia. Carcinogenesis 2005, 26, 991–999. [Google Scholar] [PubMed]
- Thomas, P.; Wu, J.; Dhillon, V.; Fenech, M. Effect of dietary intervention on human micronucleus frequency in lymphocytes and buccal cells. Mutagenesis 2011, 26, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Fenech, M. Genome health nutrigenomics and nutrigenetics–diagnosis and nutritional treatment of genome damage on an individual basis. Food Chem. Toxicol. 2008, 46, 1365–1370. [Google Scholar] [CrossRef]
- Ray, M.R.; Basu, S.; Mukherjee, S.; Roychowdhury, S.; Lahiri, T. Micronucleus frequencies and nuclear anomalies in exfoliated buccal epithelial cells of firefighters. Int. J. Hum. Genet. 2005, 5, 45–48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study Participant Characteristics | Total (n = 172) | Subgroup (n = 80) | |||
|---|---|---|---|---|---|
| mv * | mv * | ||||
| Sociodemographic | |||||
| Gender, n (%) | - | - | |||
| Females | 31 (18.0%) | 12 (15.0%) | |||
| Males | 141 (82.0%) | 68 (85.0%) | |||
| Age (years) ** | 2 | 37.5 ± 10.9 (19.0–65.0) | - | 37.6 ± 11.9 (19.0–65.0) | |
| BMI (kg m−2) ** | 11 | 27.4 ± 4.1 (18.5–41.3) | - | 27.7 ± 4.0 (18.5–41.3) | |
| Occupational exposure: | |||||
| Years of service (as a firefighter) ** | 7 | 15.9 ± 10.3 (1.0–43.0) | 3 | 16.2 ± 11.5 (1.0–43.0) | |
| Environmental exposure: | |||||
| Secondhand smoke exposure, n (%) | 7 | 144 (87.3%) | 1 | 69 (87.3) | |
| X-ray exposure last year, n (%) | 7 | 68 (41.2%) | 1 | 32 (40.5%) | |
| Lifestyle characterization: | |||||
| Alcohol intake, n (%) | 3 | 53 (31.4%) | - | 26 (32.5%) | |
| Smoking habits | 2 | - | |||
| Non-smoker, n (%) | 74 (43.5%) | 37 (46.3%) | |||
| Ex-smoker, n (%) | 34 (20.0%) | 25 (22.5%) | |||
| Current smoker, n (%) | 62 (36.5%) | 25 (31.3%) | |||
| Physical activity, n (%) | 3 | 128 (75.7%) | - | 60 (75.0%) | |
| Diet | |||||
| Vegetable intake | 23 | 8 | |||
| Never, n (%) | 12 (8.1%) | 8 (11.1%) | |||
| Daily, n (%) | 101 (67.8%) | 50 (69.4%) | |||
| Weekly, n (%) | 36 (24.2%) | 14 (19.4%) | |||
| Coffee intake, n (%) | 1 | 147 (86.0%) | - | 71 (88.8%) | |
| Nº times/week ** | 57 | 23.6 ± 13.4 (3.0–70.0) | 24 | 23.2 ± 12.3 (3.0–56.0) | |
| Tea intake, n (%) | 1 | 70 (40.7%) | - | 32 (40.0%) | |
| Nº times/week ** | 5.2 ± 5.7 (1.0–28.0) | 5.8 ± 6.6 (1.0–28.0) | |||
| Smoked food consumption, n (%) | 1 | 129 (75.4%) | - | 61 (76.3%) | |
| Nº times/week ** | 3.1 ± 4.5 (1.0–35.0) | 2.3 ± 3.1 (1.0–14.0) | |||
| Nutritional supplements intake, n (%) | 4 | 19 (11.3%) | - | 11 (13.8%) | |
| Mean ± SD | Min.–Max. | Median | P25–P75 | ||
|---|---|---|---|---|---|
| Inhaled Dose PM10 (µg kg−1) | 1.73 ± 0.43 | 0.85–2.70 | 1.68 | 1.45–2.02 | |
| Contribution of Indoor (%) | 18.12 ± 4.08 | 10.67–26.79 | 18.00 | 17.06–17.95 | |
| Contribution of Outdoor (%) | 81.87 ± 4.08 | 73.21–89.33 | 82.42 | 82.05–82.94 | |
| Inhaled Dose PM2.5 (µg kg−1) | 0.53 ± 0.21 | 0.22–1.09 | 0.49 | 0.37–0.72 | |
| Contribution of Indoor (%) | 49.09 ± 9.09 | 26.22–57.69 | 54.00 | 44.74–53.94 | |
| Contribution of Outdoor (%) | 50.90 ± 9.09 | 42.31–73.78 | 46.39 | 46.05–55.26 | |
| Variables | β | t | p-Value | 95% CI |
|---|---|---|---|---|
| Inhaled dose (µg kg−1) | ||||
| PM10 | −0.01 | −0.04 | 0.97 | −0.08 to 0.78 |
| PM2.5 | 0.07 | 0.29 | 0.77 | −0.42 to 0.57 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteves, F.; Slezakova, K.; Madureira, J.; Vaz, J.; Fernandes, A.; Morais, S.; do Carmo Pereira, M.; Teixeira, J.P.; Costa, S. Firefighters’ Occupational Exposure in Preparation for Wildfire Season: Addressing Biological Impact. Toxics 2024, 12, 201. https://doi.org/10.3390/toxics12030201
Esteves F, Slezakova K, Madureira J, Vaz J, Fernandes A, Morais S, do Carmo Pereira M, Teixeira JP, Costa S. Firefighters’ Occupational Exposure in Preparation for Wildfire Season: Addressing Biological Impact. Toxics. 2024; 12(3):201. https://doi.org/10.3390/toxics12030201
Chicago/Turabian StyleEsteves, Filipa, Klara Slezakova, Joana Madureira, Josiana Vaz, Adília Fernandes, Simone Morais, Maria do Carmo Pereira, João Paulo Teixeira, and Solange Costa. 2024. "Firefighters’ Occupational Exposure in Preparation for Wildfire Season: Addressing Biological Impact" Toxics 12, no. 3: 201. https://doi.org/10.3390/toxics12030201
APA StyleEsteves, F., Slezakova, K., Madureira, J., Vaz, J., Fernandes, A., Morais, S., do Carmo Pereira, M., Teixeira, J. P., & Costa, S. (2024). Firefighters’ Occupational Exposure in Preparation for Wildfire Season: Addressing Biological Impact. Toxics, 12(3), 201. https://doi.org/10.3390/toxics12030201