The Chemistry and Toxicology of Depleted Uranium

Abstract
:1. Introduction
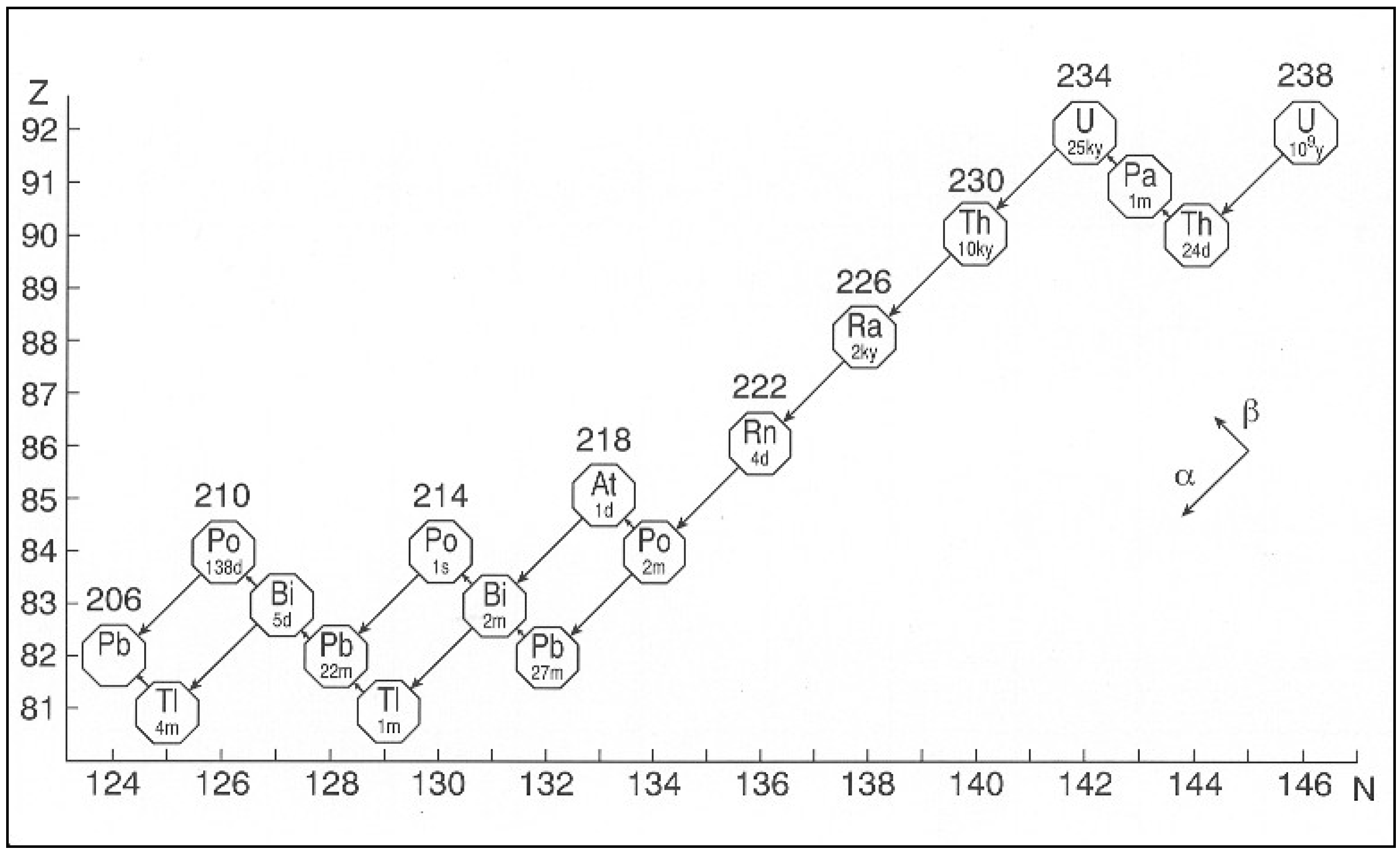
2. Occurrence of Uranium

{kind=link}
{kind=link}
{kind=link}
| Naturally occurring isotopes | |||
|---|---|---|---|
| Isotope | Abundance * | Half life | Principle decay |
| 234U | 0.00054% | 2.455 × 105 years | α: 4776 MeV |
| 235U | 0.07204% | 4.468 × 108 years | α: 4.398 MeV |
| 238U | 99.2742% | 4.468 × 109 years | α: 4.197 MeV |
| Other known isotopes | |||
| Isotope | Half life | Principle decay | |
| 217U | 16 ms | α | |
| 218U | 1.5 ms a | α: 8.27 MeV | |
| 218U | 0.51 ms b | α | |
| 218mU | 0.56 ms | α | |
| 219U | ~42 μs | α: 9.68 MeV | |
| 220U | |||
| 221U | 700 ns b | ||
| 223U | 18 μs | α: 8.78 MeV | |
| 224U | 0.7 ms | α: 8.47 MeV | |
| 224U | 0.9 ms b | α | |
| 225U | 95 ms | α: 7.88, 7.82 MeV | |
| 226U | 0.2 s | α: 7.57, 7.42 MeV | |
| 226U | 0.35 s b | α | |
| 227U | 1.1 min | α: 6.86, 7.06, 6.74 MeV | |
| 228U | 9.1 min | α: 6.68, 6.59 MeV | |
| 229U | 58 min | α: 6.36, 6.33, 6.30 MeV | |
| 230U | 20.8 days | α: 5.89, 5.82 MeV | |
| 231U | 4.2 days | α: 5.46, 5.47, 5.40 MeV | |
| 232U | 68.9 years | α: 5.32, 5.26 MeV | |
| 233U | 1.59 × 105 years | α: 4.82, 4.78 MeV | |
| 234U | 2.46 × 105 years | α: 4.77, 4.72 MeV | |
| 235U | 7.04 × 108 years | α: 4.40 MeV | |
| 236U | 2.34 × 107 years | α: 4.49, 4.45 MeV | |
| 237U | 6.75 days | β−: 0.2 MeV | |
| 238U | 4.47 × 109 years | α: 4.20 MeV | |
| 239U | 23.5 min | β−: 1.2. 1.3 MeV | |
| 240U | 14.1 h | β−: 0.4 MeV | |
| 242U | 16.8 min | β−: 1.2 MeV | |
| Some primary uranium minerals | |
|---|---|
| Branneritem | UTi2O6 |
| Coffinite | U(SiO4)1-4(OH)4-1 |
| Davidite | (REE)(Y,U)(Ti,Fe)20O38 |
| Pitchblende | U3O8 |
| Urainnite | UO2 |
| Some secondary uranium minerals | |
| Autunite | Ca(UO2)2(PO4)4·(8 to 12)H2O |
| Camolite | K2(UO2)2(VO4)2·(1 to 3)H2O |
| Seleeite | Mg(UO2)2(PO4)2·10H2O |
| Torbernite | Cu(UO2)2(PO4)2·12H2O |
| Tyuyamunite | Ca(UO2)2(VO4)2·(5 to 8)H2O |
| Uranocircite | Ba(UO2)2(PO4)2·(8 to 10)H2O |
| Uranophane | Ca(UO2)2(HSiO4)2·5H2O |
| Zeunerite | Cu(UO2)2(AsO4)2·(8 to 10)H2O |
3. Physical Properties of Uranium
| Natural uranium | |||
|---|---|---|---|
| 234U | 235U | 238U | |
| Mass % | 0.0053 | 0.711 | 99.284 |
| Radioactivity % | 48.9 | 2.2 | 48.9 |
| Activity, Bq g U−1 | 12356 | 568 | 12356 |
| Enriched (3.5%) uranium | |||
| 234U | 235U | 238U | |
| Mass % | 0.02884 | 3.5 | 96.471 |
| Radioactivity % | 81.8 | 3.4 | 14.7 |
| Activity, Bq g U−1 | 66703 | 2800 | 12500 |
| Depleted uranium | |||
| 234U | 235U | 238U | |
| Mass % | 0.0008976 | 0.2 | 99.799 |
| Radioactivity % | 14.2 | 1.1 | 84.7 |
| Activity, Bq g U−1 | 2076 | 160 | 12420 |
| Density (highly purified) | 19.05 ± 0.02 gm cm−3 |
| Density (industrial grade) | 18.85 ± 0.20 gm cm−3 |
| Melting Point | 1132 ± l °C |
| Boiling Point | 3811 ± 3 °C |
| Heat of Fusion | 19.7 J mole−1 |
| Vapor Pressure at 1600 °C | 10−4 mm |
| Thermal Conductivity at 70 °C | 0.297 J (cm s °C)−1 |
| Electrical Resistivity at 25 °C | 35 × 106 ohm cm−3 |
| Enthalpy at 25 °C | 6364 J mole−1 |
| Entropy at 25 °C | 58.2 ± 0.2 J (mole °C)−1 |
4. Chemical Properties of Uranium
| Acidic solution | Gindler [10] | Grenthe et al. [12] |
|---|---|---|
| UO22+ + e → UO21+ | 0.05 V | 0.0878 ± 0.0013 V |
| UO21+ + 4 H1+ + e → U4+ + 2 H2O | 0.62 V | |
| UO22+ + 4 H1+ + 2 e → U4+ + 2 H2O | 0.334 V | 0.2673 ± 0.0012 V |
| U4+ + e → U3+ | −0.61 V | −0.553 ± 0.004 V |
| U3+ + 3 e → U | −1.80 V | |
| U4+ + 4 e → U | −1.38 V | |
| Alkaline solution | ||
| UO2(OH)2 + 2 e → UO2 | −0.3 V | |
| UO2 + e → U(OH)3 | −2.6 V | |
| U(OH)3 + 3 e → U | −2.17 V | |

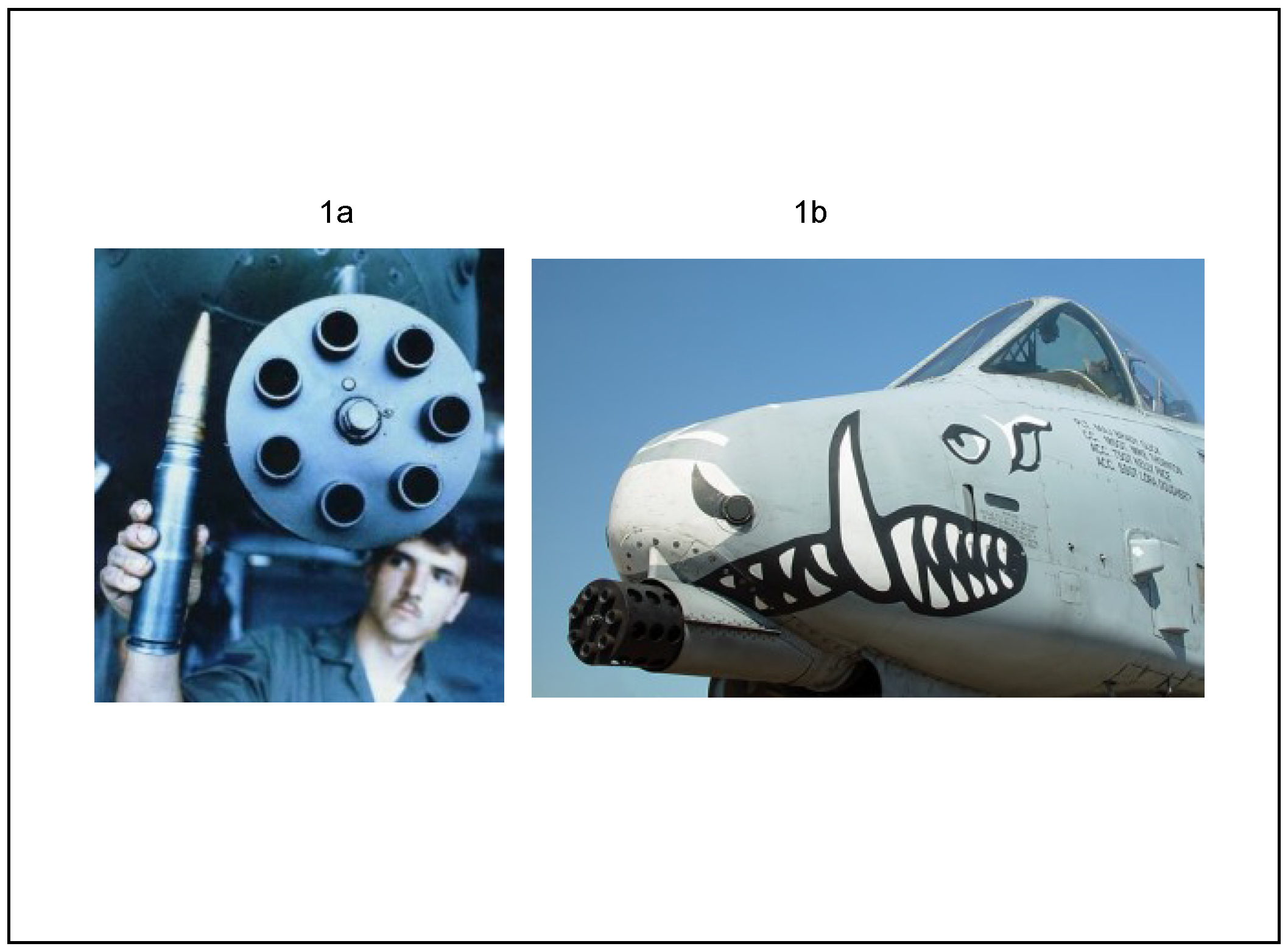
5. Depleted Uranium Penetrators

| Action | Munitions | Total mass, tons |
|---|---|---|
| 1991 Iraq-Kuwait | US Air Force 30 mm rounds | 259 |
| 1991 Iraq-Kuwait | US Army 120 mm tank rounds | 50 |
| 1991 Iraq-Kuwait | US Marine aviation rounds | 11 |
| 1991 Iraq-Kuwait | UK 120 mm tank rounds | 1 |
| 1995 Bosnia-Herzegovina | NATO 30 mm rounds | 3 |
| 1999 Kosovo-Serbia | NATO 30 mm rounds | 10 |
6. Exposure to Depleted Uranium

6.1. The Inhalation Route
6.2. The Ingestion Route
6.3. The Dermal Route
6.4. The Subcutaneous Route
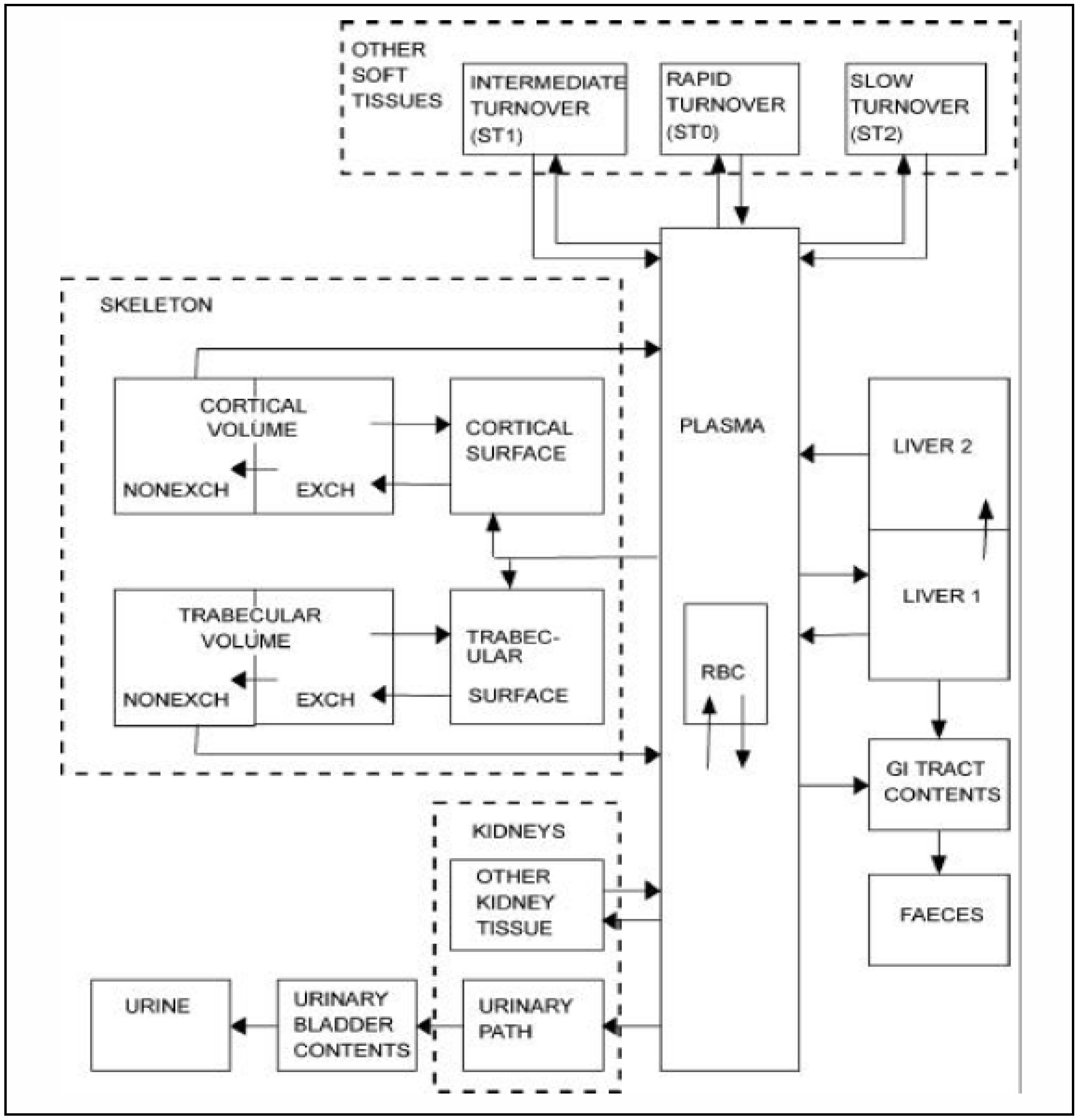
7. Toxicokinetics of Depleted Uranium

8. Toxicology of Depleted Uranium
8.1. Toxicity to the Lung
8.2. Renal Toxicity
8.3. Neurological Toxicity
8.4. Reproductive/Developmental Toxicity
8.5. Carcinogenicity
8.6. Twenty-Year Surveillance
8.7. Collateral Injuries
9. Some Concluding Comments
Conflicts of Interest
References
- Uranium and Depleted Uranium. Available online: http://www.world-nuclear.org/info./Nuclear-Fuel-Cycle/Uranium-Resources/Uranium-and-Depleted-Uranium/ (accessed on 31 December 2013).
- Legget, R.W.; Pellmar, T.C. The biokinetics of uranium migrating from embedded DU fragments. J. Environ. Radioact. 2003, 64, 205–225. [Google Scholar] [CrossRef]
- Bleise, A.; Danesi, P.R.; Burkart, W. Properties, use and health effects of depleted uranium (DU): A general overview. J. Environ. Radioact. 2003, 64, 93–112. [Google Scholar] [CrossRef]
- Craft, E.S.; Abu-Qare, A.W.; Flaherty, M.M.; Garofolo, M.C.; Rincavage, H.L.; Abou-Donia, M.B. Depleted and natural uranium: Chemistry and toxicological effects. J. Toxicol. Environ. Health B 2004, 7, 297–317. [Google Scholar] [CrossRef]
- Briner, W. The toxicity of depleted uranium. Int. J. Environ. Res. Public Health 2010, 7, 303–313. [Google Scholar] [CrossRef]
- Phennig, G.; Klewe-Nebenius, H.; Seelmann-Eggebert, W. Karlsruher Nuklidkarte, 6 Auflage 1995, korrigereten 1998; Institut für Instrumentelle Analytic: Karlsruhe, Germany, 1998. [Google Scholar]
- Sonzogi, A. Chart of the Nuclides. In Proceedings of the International Conference on Nuclear Data for Science and Technology, 22–27 April 2007; Bersillon, O., Gunsing, F., Bauge, E., Jacqmin, R., Leray, S., Eds.; EDP Science: Upton, NY, 2008; pp. 105–106. [Google Scholar]
- Emsley, J. The Elements; Clarendon Press: Oxford, UK, 1989; p. 197. [Google Scholar]
- Neghabian, R.A.; Becker, H.J.; Baran, A.; Binzel, H.-W. Verwendung von wiederaufgearbeitetem Uran und von abgreichertem Uran; NUKEM: Alzenau, Germany, 1991. [Google Scholar]
- Gindler, J.E. The Radiochemistry of Uranium; National Academy of Sciences, National Research Council: Washington, DC, USA, 1962. [Google Scholar]
- Roberts, R.A.; Choppin, G.R.; Wild, J.F. The Radiochemistry of Uranium, Neptunium and Plutonium; National Academy of Sciences, National Research Council: Washington, DC, USA, 1986. [Google Scholar]
- Grenthe, I.; Droźdźyński, J.; Fujino, T.; Buck, E.C.; Albrecht-Schmitt, T.E.; Wolf, S.F. Uranium, in The Chemistry of the Actinide and Transactinide Elements, 4th ed.; Morss, L.R., Edelstein, N.M., Fuger, J., Katz, J.J., Eds.; Springer: Dordrect, the Netherlands, 2011. [Google Scholar]
- Emsley, J. The Elements; Oxford Press: Oxford, UK, 1989; p. 202. [Google Scholar]
- Gutowski, K.E.; Cocalia, V.A.; Griffin, S.T.; Bridges, N.J.; Dixon, D.A.; Rodgers, R.D. Interactions of 1-methylimidazole with UO2(CH3CO2)2 and UO2(NO3)2: Structural, spectroscopic and theoretical evidence of imidazole binding to the uranyl ion. J. Am. Chem. Soc. 2007, 129, 526–536. [Google Scholar]
- Vanengelen, M.R.; Szilagyi, R.Z.; Gerlach, R.; Lee, B.D.; Apel, W.A.; Peyton, B.M. Uranium exerts acute toxicity by binding to pyrroloquinole quinine cofactor. Environ. Sci. Techol. 2011, 45, 937–942. [Google Scholar] [CrossRef]
- Chinni, S.; Anderson, C.B.; Ulrich, K.-U.; Giammar, D.E.; Tebo, B.M. Indirect UO2 oxidation by Mn(II)-oxidizing spores of Bacillus sp. Strain SG-1 and the effect of U and Mn concentrations. Environ. Sci. Technol. 2008, 42, 8709–8714. [Google Scholar] [CrossRef]
- Pible, O.; Vidaud, C.; Plantevin, S.; Pellequer, J.-L.; Quéméneur, E. Predicting the disruption by UO22+ of a protein-ligand interaction. Protein Sci. 2010, 19, 2219–2230. [Google Scholar]
- Roof, I.P.; Smith, M.D.; zur Loye, H.-C. Crystal growth of uranium-containing complex oxides: Ba2Na0.83U1.17O6, BaK4U3O12 and Na3Ca1.5UO6. Solid State Sci. 2010, 12, 1941–1947. [Google Scholar]
- Barnard, R.; Bullock, J.I.; Gellatly, B.J.; Larkworthy, L.F. The chemistry of the trivalent actinides. Part II, uranium (III) double chlorides and some complexes with organic ligands. J. Chem. Soc. Dalton Trans 1972, 1932–1938. [Google Scholar]
- Office of the Special Assistant for Gulf War Illness, Department of Defense. Environmental Exposure Report: Depleted Uranium in the Gulf. 1998. Available online: http://www.gulflink.osd.mil.du (accessed on 31 December 2013).
- Mitchel, R.E.; Sunder, S. Depleted uranium dust from fired munitions: Physical, chemical and biological properties. Health Phys. 2004, 87, 57–67. [Google Scholar] [CrossRef]
- Salbu, B.; Janssans, K.; Lind, O.C.; Proost, K.; Gijsels, L.; Danesi, P.R. Oxidation state of uranium in depleted uranium particles from Kuwait. J. Environ. Radioact. 2005, 78, 125–135. [Google Scholar]
- Sajih, M.; Livens, F.R.; Alvarez, R.; Morgan, M. Physiochemical characterization of depleted uranium (DU) particles at a UK firing test range. Sci. Total Environ. 2010, 408, 5990–5996. [Google Scholar] [CrossRef]
- Yousefi, H.; Najafi, A. Assessment of depleted uranium in South-Western Iran. J. Environ. Radioact. 2013, 124, 160–162. [Google Scholar] [CrossRef]
- Parliamentary Office of Science and Technology. Depleted Uranium. 2001. Available online: www.parliament.uk/post/home.htm (accessed on 31 December 2013).
- Tasat, D.R.; Orona, N.S.; Bozal, C.; Ubios, A.M.; Cabrini, R.L. Intercellular Metabolism of Uranium and the Effects of Bisphosphonates on Its Toxicity. In Cell Metabolism-Cell Homeostasis and Stress Response; Bubulya, P., Ed.; Tech Publishers: Rijeka, Yugoslavia, 2012. [Google Scholar]
- United States Environmental Protection Agency, Office of Radiation and Indoor Air Radiation Protection Division. Depleted Uranium, Technical Brief; US EPA: Washington, DC, USA, 2006.
- WHO. Health Effects of Depleted Uranium; A54/19; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Sahoo, S.K.; Matsumoto, M.; Shiraishi, K.; Cuknic, O.; Zunic, Z.S. Dose effect for South Serbians due to 238U in natural drinking water. Radiat. Prot. Dosimetry 2007, 127, 407–420. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Uranium; U.S. Department of Health and Human Services, Agency for Toxic Substances and Disease Registry, Division of Toxicology and Human Health Sciences, Environmental Toxicology Branch: Atlanta, GA, USA, 2013.
- Shavrtsbeyn, M.; Tuchinda, P.; Gaitens, J.; Squibb, K.S.; McDiarmid, M.A.; Gaspari, A. Patch testing with uranyl acetate in veterans exposed to depleted uranium during the 1991 Gulf War and the Iraqi conflict. Dermatitis 2011, 22, 33–39. [Google Scholar]
- McDiarmid, M.A.; Engelhardt, S.M.; Oliver, M.; Gucer, P.; Wilson, P.D.; Kane, R.; Kabat, M.; Kaup, B.; Anderson, L.; Hoover, D.; et al. Biological monitoring and surveillance results of Gulf War I veterans exposed to depleted uranium. Int. Arch. Occup. Environ. Health A 2005, 72, 14–29. [Google Scholar]
- Durakovic, A.; Horan, P.; Dietz, L.A.; Zimmerman, I. Estimate of the time zero lung burden of depleted uranium in persian Gulf War veterans by the 24-hour urinary excretion and exponential decay analysis. Mil. Med. 2003, 186, 600–605. [Google Scholar]
- Valdéz, M. Estimating the lung burden from exposures to aerosols of depleted uranium. Radiat. Prot. Dosimetry 2009, 134, 23–29. [Google Scholar] [CrossRef]
- Karpas, Z.; Lorber, A.; Sela, H.; Paz-Tal, O.; Hagag, Y.; Kurttio, P.; Salonen, L. Measurement of the 234U/238U ratio by MC-ICPMS in drinking water, hair, nails and urine as an indicator of uranium exposure source. Health Phys. 2005, 89, 315–321. [Google Scholar] [CrossRef]
- Kurttio, P.; Harmoinen, A.; Saha, H.; Solomen, L.; Karpas, Z.; Komulinen, H.; Auvinen, A. Kidney toxicity of ingested uranium from drinking water. Am. J. Kidney Dis. 2006, 47, 972–982. [Google Scholar]
- Lind, O.C.; Salbu, B.; Skipperud, L.; Janssens, K.; Jaroszewicz, J.; de Nolf, W. Solid state speciation and potential bioavailability of depleted uranium particles from Kosovo and Kuwait. J. Environ. Radioact. 2009, 100, 301–307. [Google Scholar] [CrossRef]
- McClain, D.E.; Benson, K.A.; Dalton, T.K.; Ejnik, J.; Emond, C.A.; Hodge, S.J.; Kalinch, J.F.; Landauer, M.A.; Miller, A.C.; Pellmar, T.C.; et al. Biological effects of embedded depleted uranium (DU): Summary of armed forces radiobiology research institute research. Sci. Total Environ. 2001, 274, 115–118. [Google Scholar] [CrossRef]
- Hooper, F.J.; Squibb, K.S.; Siegel, E.L.; McPhaul, K.; Keogh, J.P. Elevated urine uranium excretion by soldiers with retained uranium shrapnel. Health Phys. 1999, 77, 512–519. [Google Scholar] [CrossRef]
- Leggett, R.W. Basis for the ICRP’s age-specific biokinetic model for uranium. Health Phys. 1994, 67, 589–610. [Google Scholar] [CrossRef]
- ICRP. Human respiratory tract model for radiological protection. Ann. ICRP 1994, 24, 1–3. [Google Scholar]
- ICRP. Age dependent doses to members of the public from intake of radionuclides-Part 3 ingestion dose coefficients. Ann. ICRP 1995, 25, 1. [Google Scholar]
- Leggett, R.W.; Harrison, J.D. Fractional absorption of ingested uranium in humans. Health Phys. 1995, 68, 484–498. [Google Scholar] [CrossRef]
- Leggett, R.W. The behavior and chemical toxicity of U in the kidney: A reassessment. Health Phys. 1989, 57, 365–385. [Google Scholar] [CrossRef]
- Miller, A.C.; Xu, J.; Stewart, M.; Brooks, K.; Hodge, S.; Shi, L.; Page, N.; McClain, D. Observation of radiation-induced damage in human cells exposed to depleted uranium: Dicentric frequency and neoplastic transformation as endpoints. Radiat. Prot. Dosimetry 2002, 99, 275–278. [Google Scholar] [CrossRef]
- Barron, E.S.; Muntz, J.A.; Gasvoda, B. Regulatory mechanisms of cellular respiration; The role of cell membranes; Uranium inhibition of cellular respiration. J. Gen. Physiol. 1948, 32, 163–178. [Google Scholar] [CrossRef]
- McQueney, M.S.; Markham, G.D. Investigation of monovalent cation activation of S-adenosylymethionine synthetase using mutagenesis and uranyl inhibitor. J. Biol. Chem. 1995, 207, 18277–18284. [Google Scholar]
- Renault, S.; Faiz, H.; Gadet, R.; Ferrier, B.; Martin, G.; Baveral, G.; Conjard-Duplany, A. Uranyl nitrate inhibits lactate gluconeogenesis in isolated human and mouse renal proximal tubules; A 13C-NMR study. Toxicol. Appl. Pharmacol. 2010, 242, 9–17. [Google Scholar] [CrossRef]
- Gueguen, Y.; Rouas, C.; Monin, A.; Manens, L.; Stefani, J.; Delissen, O.; Grison, S.; Dublineau, I. Molecular, cellular and tissue impact of depleted uranium on xenobiotic-metabolizing enzymes. Arch. Toxicol. 2013. [Google Scholar] [CrossRef]
- Pititot, F.; Lestaevel, P.; Tourionias, E.; Mazzucco, C.; Jacquinot, S.; Dhieux, B.; Delissen, O.; Toumier, B.B.; Gensdarmes, F.; Beaunier, P.; Dublineau, I. Inhalation of uranium nanoparticles: Respiratory tract deposition and translocation to secondary target organs in rats. Toxicol. Lett. 2013, 217, 217–225. [Google Scholar] [CrossRef]
- Tirmarche, M.; Baysson, H.; Telle-Amberton, M. Uranium exposure and cancer risk: A review of epidemiological studies. Rev. Epidemiol. Sante Publique 2004, 52, 81–90. [Google Scholar]
- Periyakaruppan, A.; Kumar, F.; Sarkar, S.; Sharma, C.S.; Ramesh, G.T. Uranium induces oxidative stress in lung epithelial cells. Arch. Toxicol. 2007, 81, 389–395. [Google Scholar] [CrossRef]
- Xie, H.; LeCerte, C.; Thompson, W.D.; Wise, J.P. Depleted uranium induces neoplastic transformation in human lung epithelial cells. Chem. Res. Toxicol. 2010, 23, 373–378. [Google Scholar] [CrossRef]
- Orona, N.S.; Tasat, D.R. Uranyl nitrate-exposed rat alveolar macrophages cell death: Influence of superoxide anion and TNF α mediators. Toxicol. Appl. Pharmacol. 2012, 261, 309–316. [Google Scholar] [CrossRef]
- Stradling, N.; Hodgson, A.; Ansobrolo, E.; Berard, P.; Etherington, G.; Fell, T.; Rance, E.; le Guen, B. Industrial Uranium Compounds: Exposure Limits, Assessment of Intake and Toxicity after Inhalation; National Radiologicl Protection Board: Chilton, UK, 2002; p. 10. [Google Scholar]
- Arzuaga, X.; Rieth, S.H.; Bathija, A.; Cooper, G.S. Renal effects of exposure to natural and depleted uranium: A review of the epidemiological and experimental data. J. Toxicol. Environ. Health B 2010, 13, 527–545. [Google Scholar] [CrossRef]
- Squibb, K.S.; Leggett, R.W.; McDiarmid, M.A. Prediction of renal concentrations of depleted uranium and rdaiayion dose in Gulf War veterans with embedded shrapnel. Health Phys. 2005, 89, 267–273. [Google Scholar] [CrossRef]
- Zhu, G.; Xiang, X.; Chen, X.; Wang, L.; Hu, H.; Weng, S. Renal dysfunction induced by long-term exposure to depleted uranium in rats. Arch. Toxicol. 2009, 83, 37–46. [Google Scholar] [CrossRef]
- Zhu, G.; Tan, M.; Li, X.; Xiang, X.; Hu, H.; Zhao, S. Accumulation and distribution of uranium in rats after implantation of depleted uranium fragments. J. Radiat. Res. 2009, 50, 183–192. [Google Scholar] [CrossRef]
- Shaki, F.; Pourahmad, J.; Hosseine, M.; Ghazi-Khansari, M. Toxicity of depleted uranium on isolated rat kidney mitochondria. Res. Pharm. Sci. 2012. [Google Scholar] [CrossRef]
- Shaki, F.; Pourahmad, J. Mitochondrial toxicity of depleted uranium: Protection by beta-glucan. Iran J. Pharm. Res. 2013, 12, 131–140. [Google Scholar]
- Roszell, L.E.; Hahn, F.F.; Lee, R.B.; Parkhurst, M.A. Assessing the renal toxicity of capstone depleted uranium oxides and other uranium compounds. Health Phys. 2009, 96, 343–351. [Google Scholar] [CrossRef]
- Lestaevel, P.; Romero, E.; Dhieux, B.; Soussan, H.B.; Berradi, H.; Dublineau, I.; Voisin, P.; Gourmelon, P. Different patterns of brain pro-/anti-oxidant activity between depleted and enriched uranium in chronically exposed rats. Toxicology 2009, 258, 1–9. [Google Scholar] [CrossRef]
- Houpert, P.; Lestaevel, P.; Busby, C.; Paquet, F.; Gourmelon, P. Enriched but not depleted uranium affects central nervous system in long-term exposed rat. Neuro Biol. 2005, 6, 1015–1020. [Google Scholar]
- Jiang, G.C.-T.; Aschner, M. eurotoxicity of depleted uranium; Reasons for increased concern. Biol. Trace Elements 2006, 110, 1–17. [Google Scholar] [CrossRef]
- Jiang, G.C.-T.; Tidwell, K.; McLaughlin, B.E.; Cai, J.; Gupta, R.C.; Milatovic, D.; Nuss, R.; Aschner, M. Neurotoxic potential of depleted uranium-effects in primary cortical neuron cultures and in Caenorhabditis elegand. Toxicological Sci. 2007, 99, 553–565. [Google Scholar] [CrossRef]
- Lestaevel, P.; Airault, F.; Racine, R.; Soussan, H.B.; Dhieux, B.; Delissen, O.; Manens, L.; Aigueperse, J.; Voisin, P.; Souidi, H. Influence of environmental enrichment and depleted uranium on behaviour, cholesterol and acetylcholine in apolioprotein E-defivient mice. J. Mol. Neurosci. 2013. [Google Scholar] [CrossRef]
- Arfsten, D.P.; Still, K.R.; Ritchie, G.D. A review of the effects of uranium and depleted uranium exposure on reproductive and fetal development. Toxicol. Ind. Health 2001, 17, 180–191. [Google Scholar] [CrossRef]
- Arfsten, D.P.; Bekkedal, M.; Wilfong, E.R.; Rossi, J.; Grasman, K.A.; Healey, L.B.; Rutkiewicz, J.M.; Johnson, E.W.; Thitoff, A.R.; Jung, A.E.; et al. Study of the reproductive effects in rats surgically implanted with depleted uranium for up to 90 days. J. Toxicol. Environ. Health A 2005, 68, 967–997. [Google Scholar] [CrossRef]
- Arfsten, D.P.; Still, K.R.; Wilfong, E.R.; Johnson, E.W.; McInturf, S.M.; Eggers, J.S.; Schaeffer, D.J.; Bekkedal, M.Y. Two-generation reproductive toxicity study of implanted depleted uranium (DU) in CD rats. J. Toxicol. Environ. Health 2009, 72, 410–427. [Google Scholar] [CrossRef]
- Miller, A.C.; Stewart, M.; Rivas, R. Perconceptional parental exposure to depleted uranium: Transmission of genetic damage of offspring. Health Phys. 2010, 99, 371–379. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Briggs, A.M.; Maconochie, N.; Hotopf, P.; Lunt, M. Incidence of cancer among UK Gulf War veterans: Cohort study. Brit. Med. J. 2003, 327, 1373–1378. [Google Scholar]
- Storm, H.H.; Jørgensen, H.O.; Kejs, A.M.; Engholm, G. Depleted uranium and cancer in Danish Balkan veterans deployed 1992–2001. Eur. J. Cancer 2006, 42, 2355–2358. [Google Scholar] [CrossRef]
- Legorio, S.; Grande, E.; Martina, L. Review of epidemiological studies of cancer risk among Gulf War and Balkans veterans. Epidemiol. Prev. 2008, 32, 145–155. [Google Scholar]
- Bogers, R.P.; van Leeuwen, F.E.; Grievink, L.; Schouten, L.J.; Kiememev, L.A.; Schram-Bijkerk, D. Cancer incidence in Dutch Balkan veterans. Cancer Epidemiol. 2013, 37, 550–555. [Google Scholar] [CrossRef]
- McDiarmid, M.A.; Squibb, K.S.; Engelhardt, S.; Oliver, M.; Gucer, P.; Wilson, P.D.; Kane, R.; Kabet, M.; Kaup, B.; Anderson, L.; et al. Surveillance of depleted uranium exposed Gulf War veterans: Health effects observed in an Engaged “friendly fire” cohort. J. Occ. Environ. Med. 2001, 43, 991–1000. [Google Scholar]
- McDiarmid, M.A.; Squibb, K.S.; Engelhard, S.M. Biologic monitoring for urinary uranium in Gulf War I veterans. Health Phys. 2004, 87, 51–56. [Google Scholar] [CrossRef]
- McDiarmid, M.A.; Engelhardt, S.M.; Oliver, M.; Gucer, P.; Wilson, P.D.; Kane, R.; Cernich, A.; Kaup, B.; Anderson, L.; Hoover, D.; et al. Health surveillance of Gulf War I veterans expose to depleted uranium: Updating the cohort. Health Phys. 2007, 93, 60–73. [Google Scholar] [CrossRef]
- McDiarmid, M.A.; Engelhard, S.M.; Dorsey, C.D.; Oliver, M.; Gucer, P.; Wilson, P.D.; Kane, R.; Cernich, A.; Kaup, B.; Anderson, L.; et al. Surveillance results of depleted uranium-exposed Gulf War I veterans: Sixteen years of follow up. J. Toxicol. Environ. Health A 2009, 72, 14–29. [Google Scholar]
- McDiarmid, M.A.; Engelhardt, S.M.; Dorsey, C.D.; Oliver, M.; Gucer, P.; Gaitens, J.M.; Kane, R.; Cernich, A.; Kaup, B.; Hoover, D.; et al. Longitudinal health surveillance in a cohort of Gulf War veterans 18 years after first exposure to depleted uranium. J. Toxicol. Environ. Health 2011, 74, 678–691. [Google Scholar] [CrossRef]
- Oliver, M.V.B.M.S.; McDiarmid, M.A.; Squibb, K.S.; Tucker, J.D. Long term depleted uranium exposure in Gulf War I veterans does not induce chromosome aberrations in peripheral blood lymphocytes. Mutat. Res. 2011, 720, 53–57. [Google Scholar] [CrossRef]
- Bakhmutsky, M.V.; Oliver, M.S.; McDiarmid, M.A.; Squibb, K.S.; Tucker, J.D. Long term depleted uranium exposure in Gulf War I veterans does not cause elevated numbers of micronuclei in peripheral blood lymphocytes. Mutat. Res. 2013, 757, 132–139. [Google Scholar] [CrossRef]
- Hines, S.E.; Gucer, P.; Klingerman, S.; Breyer, R.; Centeno, J.; Gaithers, J.; Oliver, M.; Engelhardt, S.M.; Squibb, K.S.; McDiarmid, M.A. Pulmonary health effects in Gulf War I service members exposed to depleted uranium. J. Occup. Environ. Med. 2013, 55, 937–944. [Google Scholar] [CrossRef]
- McDiarmid, M.A.; Gaithers, J.M.; Hines, S.; Breyer, R.; Wong-You-Cheong, J.J.; Engelhardt, S.M.; Oliver, M.; Gucer, P.; Kane, R.; Cernich, A.; et al. The Gulf War depleted uranium cohort at 20 years: Bioassay results and novel approaches to fragment surveillance. Health Phys. 2013, 104, 347–361. [Google Scholar] [CrossRef]
- Alaani, S.; Tafash, M.; Busby, C.; Hamden, M.; Blaurock-Busch, E. Uranium and other contaminants in hair from the parents of children with congenital abnormalities in Fallujah, Iraq. Confl. Health 2011, 5, 15. [Google Scholar] [CrossRef]
- Alaani, S.; Fallouji, M.A.A.; Busby, C.; Hamdan, M. Pilot study of congenital anomaly rates at Birth in Fallujah, Iraq, 2010. J. Islamic Med. Assoc. 2012, 44, 8–15. [Google Scholar]
- Al-Habithi, T.S.; Al-Diwan, J.K.; Abubakir, A.M.; Saleh, M.; Sabila, P. Birth defects in Iraq and plausibility of environmental exposure: A Review. Confl. Health 2012, 6, 3. [Google Scholar] [CrossRef]
- Butowinski, A.T.; DeScisciolo, C.; Conlin, A.M.; Ryan, M.A.K.; Sevick, C.J.; Smith, T.C. Birth defects in infants born in 1998–2004 to men and women serving in the U.S. military during the 1990–1991 Gulf War Era. Birth Defects Res. A 2012, 94, 721–728. [Google Scholar] [CrossRef]
- Busby, C.; Hamdan, M.; Ariabi, E. Cancer, infant mortality and birth sex-ratio in Fallujah, Iraq 2005–2009. Int. J. Res. Pub. Health 2010, 7, 2828–2837. [Google Scholar] [CrossRef]
- Al-Hamzawi, A.A.; Jaafar, M.S.; Tawfiq, N.F. Uranium concentration in uranium samples of Southern Iraqi leukemia patients using CR-39 track detector. J. Radioanal. Nuc. Chem. 2013. [Google Scholar] [CrossRef]
- Hagopian, A.; Lafta, R.; Hassan, J.; Davis, S.; Mirick, D.; Takaro, T. Trends in childhood leukemia in Basrah, Iraq, 1993–2007. Am. J. Pub. Health 2010, 100, 1081–1087. [Google Scholar] [CrossRef]
- Alrudainy, L.A.; Hassan, J.G.; Salih, H.M.; Abbas, M.K.; Majeed, A.A. Time trends and geographical distribution of childhood leukemia in Basrah, Iraq, from 2004 to 2009, Sultan Qaboos. Univ. Med. J. 2011, 11, 215–220. [Google Scholar]
- Greiser, E.; Hoffmann, W. Questionable increase of childhood leukemia in Basrah, Iraq. Am. J. Pub. Health. 2010, 100, 1556. [Google Scholar] [CrossRef]
- Hagopian, A.; Lafta, R.; Hassan, J.; Davis, S.; Mirick, D.; Takaro, T. Hagopian et al. Respond. Am. J. Pub. Health 2010, 100, 1557. [Google Scholar]
- Fathi, R.A.; Matti, L.Y.; Al-Salih, H.S.; Godbold, D. Environmental pollution by depleted uranium in Iraq with special reference to Mosul and possible effects on cancer and birth defect rates. Med. Confl. Surviv. 2013, 29, 7–25. [Google Scholar] [CrossRef]
- United Nations Environment Programmme. Depleted Uranium in Kosovo, Post-Conflict Environmental Assessment; United Nations Environment Programmme: Nairobi, Kenya, 2001. [Google Scholar]
- Nafezi, G.; Gregoric, A.; Vaupotic, J.; Bahtijari, M.; Kugali, M. Radon levels and doses in dwellings in two villages in Kosovo, affected by depleted uranium. Radiat. Prot. Dosimetry 2013. [Google Scholar] [CrossRef]
- United Nations Environment Programmme. Depleted Uranium in Serbia and Montenegro, Post-Conflict Environmental Assessment in the Republic of Yugoslavia; United Nations Environment Programmme: Nairobi, Kenya, 2002. [Google Scholar]
- United Nations Environment Programmme. Depleted Uranium in Bosnia and Herzegovina, Post-Conflict Environmental Assessment of Depleted Uranium in Bosnia and Herzegovina; United Nations Environment Programmme: Nairobi, Kenya, 2003. [Google Scholar]
- Handley-Sidhu, S.; Bryan, N.D.; Vaughan, P.J.; Livens, F.R.; Keith-Roach, M.J. Corrosion and transport of depleted uranium in sand-rich environments. Chempsphere 2009, 77, 143–149. [Google Scholar]
- Toque, C.; Milodowski, A.E.; Baker, A.C. The corrosion of depleted uranium in terrestrial and marine environments. J. Environ. Radioact. 2013. [Google Scholar] [CrossRef]
- Crean, D.E.; Livens, F.R.; Stennett, M.C.; Grolimund, D.; Borca, C.N.; Hyatt, N.C. Remediation of soil contaminated with particulate depleted uranium by multi stage chemical extraction. J. Hazard Mater. 2013. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Katz, S.A. The Chemistry and Toxicology of Depleted Uranium. Toxics 2014, 2, 50-78. https://doi.org/10.3390/toxics2010050
Katz SA. The Chemistry and Toxicology of Depleted Uranium. Toxics. 2014; 2(1):50-78. https://doi.org/10.3390/toxics2010050
Chicago/Turabian StyleKatz, Sidney A. 2014. "The Chemistry and Toxicology of Depleted Uranium" Toxics 2, no. 1: 50-78. https://doi.org/10.3390/toxics2010050
APA StyleKatz, S. A. (2014). The Chemistry and Toxicology of Depleted Uranium. Toxics, 2(1), 50-78. https://doi.org/10.3390/toxics2010050