
Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design Sample and Data Collection
2.2.1. Questionnaire-Based Data Collection
2.2.2. Particulate Matter Measurement
2.2.3. Calibration of PM2.5 Measurements
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
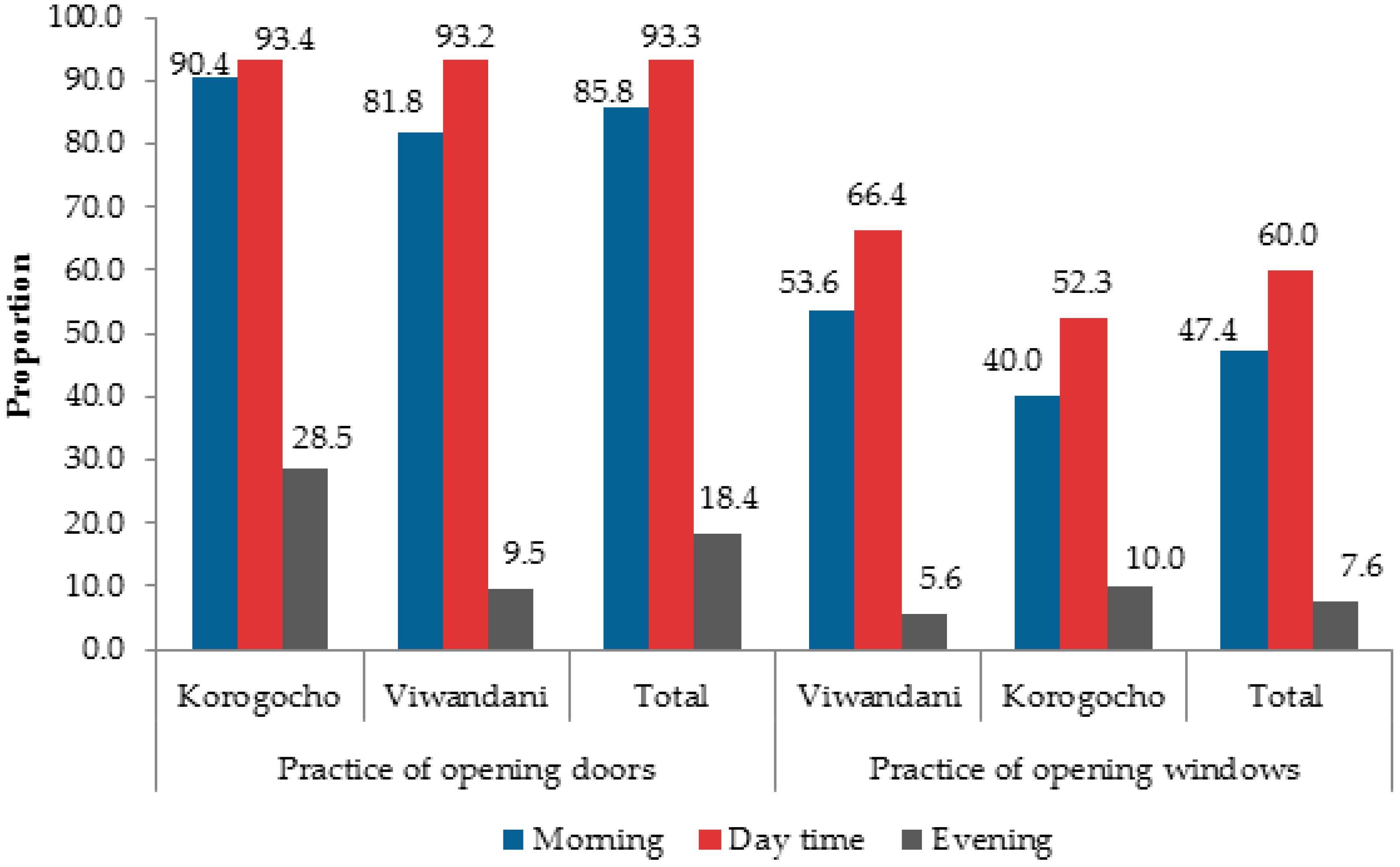
3.1. Fuels, Stoves and Ventilation
3.2. Exposure to Tobacco Smoke
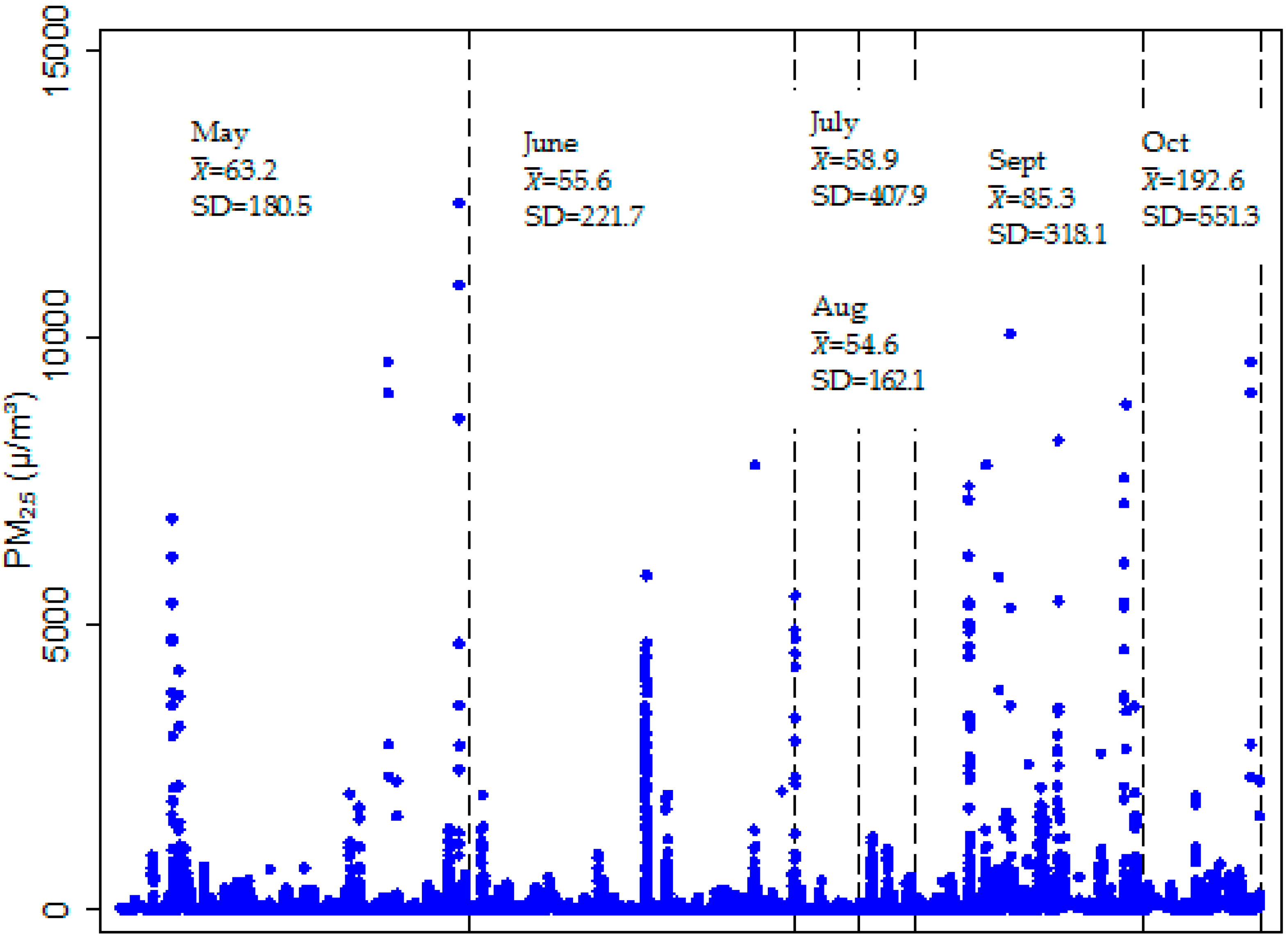
3.3. Household Air Quality: PM2.5 Levels
3.3.1. PM2.5 Concentrations by Main Fuel Used for Cooking and Lighting
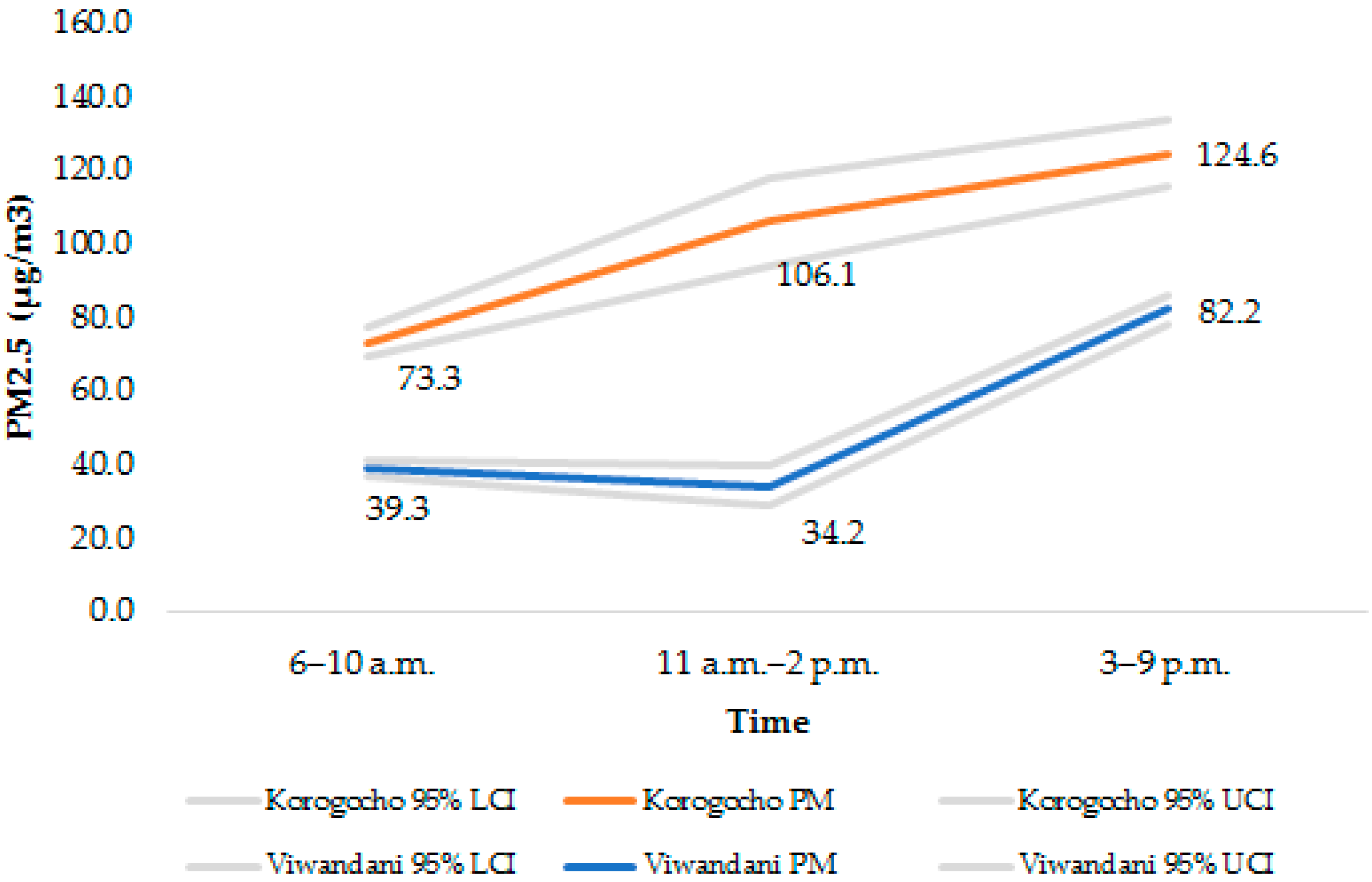
3.3.2. PM2.5 Concentrations at Different Times of the Day
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- International Agency for Research on Cancer. Outdoor Air Pollution a Leading Environmental Cause of Cancer Deaths; IARC: Lyon, France, 2013. [Google Scholar]
- World Health Organization. Burden of Disease from Ambient Air Pollution for 2012; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Burden of Disease from the Joint Effects of Household and Ambient Air Pollution for 2012; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Bernstein, J.A.; Alexis, N.; Barnes, C.; Bernstein, I.L.; Nel, A.; Peden, D.; Diaz-Sanchez, D.; Tarlo, S.M.; Williams, P.B. Health effects of air pollution. J. Allergy Clin. Immunol. 2004, 114, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.A.; Godri-Pollitt, K.; Villeneuve, P.J. PM2.5, oxidant defence and cardiorespiratory health: A review. Environ. Health 2013. [Google Scholar] [CrossRef] [PubMed]
- Bruce, N.; Pope, D.; Rehfuess, E.; Balakrishnan, K.; Adair-Rohani, H.; Dora, C. WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposure-risk functions. Atmos. Environ. 2015, 106, 451–457. [Google Scholar] [CrossRef]
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar] [PubMed]
- Dionisio, K.L.; Howie, S.R.; Dominici, F.; Fornace, K.M.; Spengler, J.D.; Adegbola, R.A.; Ezzati, M. Household concentrations and exposure of children to particulate matter from biomass fuels in the Gambia. Environ. Sci. Technol. 2012, 46, 3519–3527. [Google Scholar] [CrossRef] [PubMed]
- Duflo, E.; Greenstone, M.; Hanna, R. Cooking Stoves, Indoor Air Pollution and Respiratory Health in Rural Orissa, India. Econ. Political Weekly 2008, 43, 71–76. [Google Scholar]
- Ezzati, M.; Saleh, H.; Kammen, D.M. The contributions of emissions and spatial microenvironments to exposure to indoor air pollution from biomass combustion in Kenya. Environ. Health Perspect. 2000, 108, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Boy, E.; Bruce, N.; Delgado, H. Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ. Health Perspect. 2002, 110, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Kammen, D.M. Quantifying the effects of exposure to indoor air pollution from biomass combustion on acute respiratory infections in developing countries. Environ. Health Perspect. 2001, 109, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Pogodina, C.; Brunner Huber, L.R.; Racine, E.F.; Platonova, E. Smoke-free homes for smoke-free babies: The role of residential environmental tobacco smoke on low birth weight. J. Commun. Health 2009, 34, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Abusalah, A.; Gavana, M.; Haidich, A.B.; Smyrnakis, E.; Papadakis, N.; Papanikolaou, A.; Benos, A. Low birth weight and prenatal exposure to indoor pollution from tobacco smoke and wood fuel smoke: A matched case-control study in gaza strip. Mater. Child Health J. 2011, 16, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Amegah, A.K.; Jaakkola, J.J.K. Work as a street vendor, associated traffic-related air pollution exposures and risk of adverse pregnancy outcomes in Accra, Ghana. Int. J. Hyg. Environ. Health 2014, 217, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, A.R.; Rehfuess, E.A.; Weber, M.; Bruce, N.G. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, N.L.; Merialdi, M.; van Donkelaar, A.; Vadillo-Ortega, F.; Martin, R.V.; Betran, A.P.; Souza, J.P. Outdoor air pollution, preterm birth, and low birth weight: Analysis of the world health organization global survey on maternal and perinatal health. Environ. Health Perspect. 2014, 122, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Patelarou, E.; Kelly, F.J. Indoor exposure and adverse birth outcomes related to fetal growth, miscarriage and prematurity—A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 5904–5933. [Google Scholar] [CrossRef] [PubMed]
- Subramoney, S.; D’espaignet, E.T.; Gupta, P.C. Higher risk of stillbirth among lower and middle income women who do not use tobacco, but live with smokers. Acta Obstet. Gynecol. 2010, 89, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Kiyoshi, S.; Dan, N.; Yahong, M.; Eiji, S.; Michihiro, K.; Tetsuya, Y.; Yasuhiro, T. A comparison of indoor air pollutants in Japan and Sweden: Formaldehyde, nitrogen dioxide, and chlorinated volatile organic compounds. Environ. Res. 2004, 94, 75–85. [Google Scholar]
- Mu, L.; Liu, L.; Niu, R.; Zhao, B.; Shi, J.; Li, Y.; Swanson, M.; Scheider, W.; Su, J.; Chang, S.-C. Indoor air pollution and risk of lung cancer among chinese female non-smokers. Cancer Causes Control 2013, 24, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Zhiyong, H.; Rao, K.R. Particulate air pollution and chronic ischemic heart disease in the eastern united states: A county level ecological study using satellite aerosol data. Environ. Health 2009. [Google Scholar] [CrossRef]
- World Health Organization. Population using solid fuels (estimates): Data by country. Global Health Observatory Data Repository. Available online: http://apps.who.int/gho/data/node.main.135 (accessed on 2 October 2015).
- World Health Organization. Ambient (Outdoor) Air Pollution in Cities Database. 2014. Available online: http://www.who.int/phe/health_topics/outdoorair/databases/cities/en/ (accessed on 5 November 2015).
- Fullerton, D.G.; Semple, S.; Kalambo, F.; Suseno, A.; Malamba, R.; Henderson, G.; Ayres, J.G.; Gordon, S.B. Biomass fuel use and indoor air pollution in homes in malawi. Occup. Environ. Med. 2009, 66, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Majdan, M.; Svaro, M.; Bodo, J.; Taylor, M.; Muendo, R.M. Assessment of the biomass related indoor air pollution in kwale district in Kenya using short term monitoring. Afr. Health Sci. 2015, 15, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Teather, K.; Critchley, K.; Ross, E.; Symington, L.; Mirie, W.; Gibson, M.; Barnett, T.; Qadoumi, H. Air quality and children’s health in rural Kenya. Air Pollut. XXIII 2015, 198, 217–216. [Google Scholar]
- Van Vliet, E.D.; Asante, K.; Jack, D.W.; Kinney, P.L.; Whyatt, R.M.; Chillrud, S.N.; Abokyi, L.; Zandoh, C.; Owusu-Agyei, S. Personal exposures to fine particulate matter and black carbon in households cooking with biomass fuels in rural Ghana. Environ. Res. 2013, 127, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Muindi, K.; Egondi, T.; Kimani-Murage, E.; Rocklov, J.; Ng, N. “We are used to this”: A qualitative assessment of the perceptions of and attitudes towards air pollution amongst slum residents in Nairobi. BMC Public Health 2014. [Google Scholar] [CrossRef] [PubMed]
- African Population and Health Research Center. NUHDSS Indicators 2003–2013; APHRC: Nairobi, Kenya, 2014. [Google Scholar]
- Egondi, T.; Muindi, K.; Gatari, M.; Kyobutungi, C.; Ng, N.; Rocklov, J. Measuring exposure levels of inhalable airborne particles (PM2.5) in two socially deprived areas of Nairobi, Kenya. Environ. Res. 2016, 148, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Beguy, D.; Elung’ata, P.; Mberu, B.; Oduor, C.; Wamukoya, M.; Nganyi, B.; Ezeh, A. Health & demographic surveillance system profile: The Nairobi urban health and demographic surveillance system (nuhdss). Int. J. Epidemiol. 2015, 44, 462–471. [Google Scholar] [PubMed]
- Emina, J.; Beguy, D.; Zulu, E.; Ezeh, A.; Muindi, K.; Elung’ata, P.; Otsola, J.; Yé, Y. Monitoring of health and demographic outcomes in poor urban settlements: Evidence from the Nairobi urban health and demographic surveillance system. J. Urban Health 2011, 88, 200–218. [Google Scholar] [CrossRef] [PubMed]
- Kimani-Murage, E.W.; Kyobutungi, C.; Ezeh, A.C.; Wekesah, F.; Wanjohi, M.; Muriuki, P.; Musoke, R.N.; Norris, S.A.; Griffiths, P.; Madise, N.J. Effectiveness of personalised, home-based nutritional counselling on infant feeding practices, morbidity and nutritional outcomes among infants in Nairobi slums: Study protocol for a cluster randomised controlled trial. Trials 2013. [Google Scholar] [CrossRef] [PubMed]
- McNamara, M.L.; Noonan, C.W.; Ward, T.J. Correction factor for continuous monitoring of wood smoke fine particulate matter. Aerosol Air Qual. Res. 2011, 11, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Lam, N.L.; Chen, Y.; Weyant, C.; Venkataraman, C.; Sadavarte, P.; Johnson, M.A.; Smith, K.R.; Brem, B.T.; Arineitwe, J.; Ellis, J.E.; et al. Household light makes global heat: High black carbon emissions from kerosene wick lamps. Environ. Sci. Technol. 2012, 46, 13531–13538. [Google Scholar] [CrossRef] [PubMed]
- Titcombe, M.E.; Simcik, M. Personal and indoor exposure to PM2.5 and polycyclic aromatic hydrocarbons in the southern highlands of tanzania: A pilot-scale study. Environ. Monit. Assess. 2011, 180, 461–476. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M.B.; Bates, M.N.; Arora, N.K.; Balakrishnan, K.; Jack, D.W.; Smith, K.R. Household fuels, low birth weight, and neonatal death in india: The separate impacts of biomass, kerosene, and coal. Int. J. Hyg. Environ. Health 2013, 216, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Lam, N.L.; Smith, K.R.; Gauthier, A.; Bates, M.N. Kerosene: A review of household uses and their hazards in low- and middle-income countries. J. Toxicol. Environ. Health B Crit. Rev. 2012, 15, 396–432. [Google Scholar] [CrossRef] [PubMed]
- Hiemstra-van-der-Horst, G.; Hovorka, A.J. Reassessing the ‘‘energy ladder’’: Household energy use in Maun, Botswana. Energy Policy 2008, 36, 3333–3344. [Google Scholar] [CrossRef]
- Van-der-Kroon, B.; Brouwer, R.; van-Beukering, P.J.H. The energy ladder: Theoretical myth or empirical truth? Results from a meta-analysis. Renew. Sustain. Energy Rev. 2013, 20, 504–513. [Google Scholar] [CrossRef]
- Yamamoto, S.; Sie’, A.; Sauerborn, R. Cooking fuels and the push for cleaner alternatives: A case study from Burkina Faso. Glob. Health Act. 2009. [Google Scholar] [CrossRef] [PubMed]
- Semple, S.; Apsley, A.; Ibrahim, T.A.; Turner, S.W.; Cherrie, J.W. Fine particulate matter concentrations in smoking households: Just how much secondhand smoke do you breathe in if you live with a smoker who smokes indoors? Tob. Control 2015, 24, e205–e211. [Google Scholar] [CrossRef] [PubMed]
- Maina, W.K.; Nato, J.N.; Okoth, M.A.; Kiptui, D.J.; Ogwell, A.O. Prevalence of tobacco use and associated behaviours and exposures among the youth in Kenya: Report of the global youth tobacco survey in 2007. Public Health Res. 2013, 3, 43–49. [Google Scholar]
- Unfiltered, T. New Survey Shows Need for Kenya to Take Strong Action to Save Lives from Tobacco Use. Available online: http://www.tobaccofreekids.org/tobacco_unfiltered/post/2014_12_02_kenya (accessed on 28 November 2015).
- WHO Regional Office for Africa. Kenya Launches a National Anti-Smoking Mass Media Campaign. Available online: http://www.afro.who.int/en/kenya/press-materials/item/7222-kenya-launches-a-national-anti-smoking-mass-media-campaign.html (accessed on 28 November 2015).
- Peltzer, K. Early smoking initiation and associated factors among in-school male and female adolescents in seven African countries. Afr. Health Sci. 2011, 11, 320–328. [Google Scholar] [PubMed]
- Nichter, M.; Greaves, L.; Bloch, M.; Paglia, M.; Scarinci, I.; Tolosa, J.E.; Novotny, T.E. Tobacco use and secondhand smoke exposure during pregnancy in low- and middle-income countries: The need for social and cultural research. Acta Obstet. Gynecol. 2010, 89, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Semple, S.; Latif, N. How long does secondhand smoke remain in household air: Analysis of PM2.5 data from smokers’ homes. Nicot. Tob. Res. 2014, 16, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Leonardi-Bee, J.; Britton, J.; Venn, A. Secondhand smoke and adverse fetal outcomes in nonsmoking pregnant women: A meta-analysis. Pediatrics 2011, 127, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D. On behalf of the knowledge synthesis group. Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Chapter 5. Reproductive and Developmental Effects from Exposure to Second Hand Smoke; Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006. [Google Scholar]
- Essendi, H.; Mills, S.; Christophe, F.J. Barriers to formal emergency obstetric care services’ utilization. J. Urban Health 2010, 88, 356–369. [Google Scholar] [CrossRef] [PubMed]
- Mudege, N.N.; Zulu, E.M.; Izugbara, C. How insecurity impacts on school attendance and school drop out among urban slum children in Nairobi. Int. J. Confl. Violence 2008, 2, 98–112. [Google Scholar]
- Wilson, I.; Semple, S.; Mills, L.M.; Ritchie, D.; Shaw, A.; O’Donnell, R.; Bonella, P.; Turner, S.; Amos, A. Refresh-reducing families’ exposure to secondhand smoke in the home: A feasibility study. Tob. Control 2013. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Filter | Concentration (µg/m3) | Calibration Factor | |
|---|---|---|---|---|
| DustTrak | BGI 400 | |||
| 13–15 February 2013 | February 129 | 115 | 43 | 0.37 |
| 16–20 February 2013 | February 130 | 125 | 31 | 0.25 |
| Average Calibration Factor | 0.31 | |||
| Household Characteristics | Korogocho (%) (n = 499) | Viwandani (%) (n = 559) | Total (%) (n = 1058) | χ2 (p-Value) |
|---|---|---|---|---|
| Ventilation type | 2.06 (p = 0.15) | |||
| Door and window | 60.1 | 64.4 | 62.4 | |
| Door only | 39.9 | 35.6 | 37.6 | |
| Commonly used Cookstoves | 40.88 (p < 0.001) | |||
| Kerosene | 71.7 | 67.8 | 69.7 | |
| Charcoal/wood | 26.1 | 19.9 | 22.8 | |
| Gas/Electricity | 2.2 | 12.3 | 7.6 | |
| Range of stoves used | NA | |||
| Kerosene stove | 94.0 | 93.9 | 94.0 | |
| Metal/ceramic jiko | 76.2 | 73.2 | 74.6 | |
| Gas/electric stove | 3.6 | 18.4 | 11.4 | |
| Traditional 3-stone | 1.0 | 0.2 | 0.6 |
| Outcome | Korogocho (24) | Viwandani (48) | Total | Test Statistic (p-Value) |
|---|---|---|---|---|
| χ2 (p-value) | ||||
| Proportion of households using different cooking fuels (%) | 24.6 (p < 0.001) | |||
| Charcoal or wood | 62.5 | 14.6 | 30.6 | |
| Kerosene | 12.5 | 72.9 | 52.8 | |
| LPG/electricity | 25.0 | 12.5 | 16.7 | |
| PM2.5 mean levels for different cooking fuels (µg/m3) | t-statistic (p value) | |||
| Charcoal or wood | 126.5 | 75.7 | 110.0 | 6.59 (p < 0.001) |
| Kerosene | 109.6 | 58.7 | 61.9 | 7.43 (p < 0.001) |
| LPG/electricity | 72.0 | 45.6 | 59.1 | 10.04 (p < 0.001) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muindi, K.; Kimani-Murage, E.; Egondi, T.; Rocklov, J.; Ng, N. Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums. Toxics 2016, 4, 12. https://doi.org/10.3390/toxics4030012
Muindi K, Kimani-Murage E, Egondi T, Rocklov J, Ng N. Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums. Toxics. 2016; 4(3):12. https://doi.org/10.3390/toxics4030012
Chicago/Turabian StyleMuindi, Kanyiva, Elizabeth Kimani-Murage, Thaddaeus Egondi, Joacim Rocklov, and Nawi Ng. 2016. "Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums" Toxics 4, no. 3: 12. https://doi.org/10.3390/toxics4030012
APA StyleMuindi, K., Kimani-Murage, E., Egondi, T., Rocklov, J., & Ng, N. (2016). Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums. Toxics, 4(3), 12. https://doi.org/10.3390/toxics4030012