
Urinary Naphthol as a Biomarker of Exposure: Results from an Oral Exposure to Carbaryl and Workers Occupationally Exposed to Naphthalene

Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Volunteer Study
2.3. Sample Preparation
2.4. Sample Analysis
2.5. Creatinine Analysis
2.6. Urine Naphthol Isomers in Exposed Workers
3. Results
4. Discussion
Acknowledgments
Conflicts of Interest
References
- Gunasekara, A.S.; Rubin, A.L.; Goh, K.S.; Spurlock, F.C.; Tjeerdema, R.S. Environmental fate and toxicology of carbaryl. Rev. Environ. Contam. Toxicol. 2008, 196, 95–121. [Google Scholar] [PubMed]
- EPA. Amended Reregistration Eligibility Decision (RED) for Carbaryl. Available online: http://www.archive.epa.gov/pesticides/reregistration/web/pdf/carbaryl-red-amended.pdf (accessed on 1 November 2015).
- Bjorling-Poulsen, M.; Andersen, H.R.; Grandjean, P. Potential developmental neurotoxicity of pesticides used in Europe. Environ. Health 2008, 7, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, L.G.; Giordano, G.; Guizzetti, M.; Vitalone, A. Neurotoxicity of pesticides: A brief review. Front. Biosci. 2008, 13, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Band, P.R.; Abanto, Z.; Bert, J.; Lang, B.; Fang, R.; Gallagher, R.P.; Le, N.D. Prostate cancer risk and exposure to pesticides in British Columbia farmers. Prostate 2011, 71, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Weichenthal, S.; Moase, C.; Chan, P. A review of pesticide exposure and cancer incidence in the Agricultural Health Study cohort. Environ. Health Perspect. 2010, 118, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- JMPR. Pesticide Residues in Food—2002. In Report of the Joint Meeting of the FAO Panel of Experts on Pesticide Residues in Food and the Environment and the WHO Core Assessment Group on Pesticide Residues, Rome, Italy, 16–25 September 2002; Available online: http://www.fao.org/fileadmin/templates/agphome/documents/Pests_Pesticides/JMPR/Reports_1991–2006/Report_2002.pdf (accessed on 1 November 2015).
- Knaak, J.B. Biological and nonbiological modifications of carbamates. Bull. World Health Organ. 1971, 44, 121–131. [Google Scholar] [PubMed]
- Bouchard, M.; Carrier, G.; Brunet, R.C. Assessment of absorbed doses of carbaryl and associated health risks in a group of horticultural greenhouse workers. Int. Arch. Occup. Environ. Health 2008, 81, 355–370. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.B.; Yoon, M.; Young, B.; Tan, Y.M. Analysis of biomarker utility using a PBPK/PD model for carbaryl. Front. Pharmacol. 2014, 5, 246. [Google Scholar] [CrossRef] [PubMed]
- Shealy, D.B.; Barr, J.R.; Ashley, D.L.; Patterson, D.G., Jr.; Camann, D.E.; Bond, A.E. Correlation of environmental carbaryl measurements with serum and urinary 1-naphthol measurements in a farmer applicator and his family. Environ. Health Perspect. 1997, 105, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Cocker, J. A perspective on biological monitoring guidance values. Toxicol. Lett. 2014, 231, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Preuss, R.; Drexler, H.; Bottcher, M.; Wilhelm, M.; Bruning, T.; Angerer, J. Current external and internal exposure to naphthalene of workers occupationally exposed to polycyclic aromatic hydrocarbons in different industries. Int. Arch. Occup. Environ. Health 2005, 78, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Vu, A.T.; Taylor, K.M.; Holman, M.R.; Ding, Y.S.; Hearn, B.; Watson, C.H. Polycyclic Aromatic Hydrocarbons in the Mainstream Smoke of Popular U.S. Cigarettes. Chem. Res. Toxicol. 2015, 28, 1616–1626. [Google Scholar] [CrossRef] [PubMed]
- Meeker, J.D.; Barr, D.B.; Serdar, B.; Rappaport, S.M.; Hauser, R. Utility of urinary 1-naphthol and 2-naphthol levels to assess environmental carbaryl and naphthalene exposure in an epidemiology study. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Bevan, R.; Jones, K.; Cocker, J.; Assem, F.L.; Levy, L.S. Reference ranges for key biomarkers of chemical exposure within the UK population. Int. J. Hyg. Environ. Health 2013, 216, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Butler, A.R. The Jaffe reaction. Identification of the coloured species. Clin. Chim. Acta 1975, 59, 227–232. [Google Scholar] [CrossRef]
- Cocker, J.; Mason, H.J.; Warren, N.D.; Cotton, R.J. Creatinine adjustment of biological monitoring results. Occup. Med. Oxf. 2011, 61, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Petropoulou, S.S.E.; Gikas, E.; Tsarbopoulos, A.; Siskos, P.A. Gas chromatographic-tandem mass spectrometric method for the quantitation of carbofuran, carbaryl and their main metabolites in applicators’ urine. J. Chrom. A 2006, 1108, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, M.; Pinsonneault, L.; Tremblay, C.; Weber, J.P. Biological monitoring of environmental exposure to polycyclic aromatic hydrocarbons in subjects living in the vicinity of a creosote impregnation plant. Int. Arch. Occup. Environ. Health 2001, 74, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Third National Report on Human Exposure to Environmental Chemicals; Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2005; pp. 349–384. [Google Scholar]
- Wilhelm, M.; Hardt, J.; Schulz, C.; Angerer, J. New reference value and the background exposure for the PAH metabolites 1-hydroxypyrene and 1-and 2-naphthol in urine of the general population in Germany: Basis for validation of human biomonitoring data in environmental medicine. Int. J. Hyg. Environ. Health 2008, 211, 447–453. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Code | Gender | Age | Height (m) | Weight (kg) | BMI |
|---|---|---|---|---|---|
| A | F | 35 | 1.715 | 77 | 26.2 |
| B | M | 55 | 1.71 | 94 | 32.1 |
| C | F | 23 | 1.75 | 107 | 34.9 |
| D | M | 26 | 1.76 | 102 | 32.9 |
| E | M | 54 | 1.895 | 96 | 26.7 |
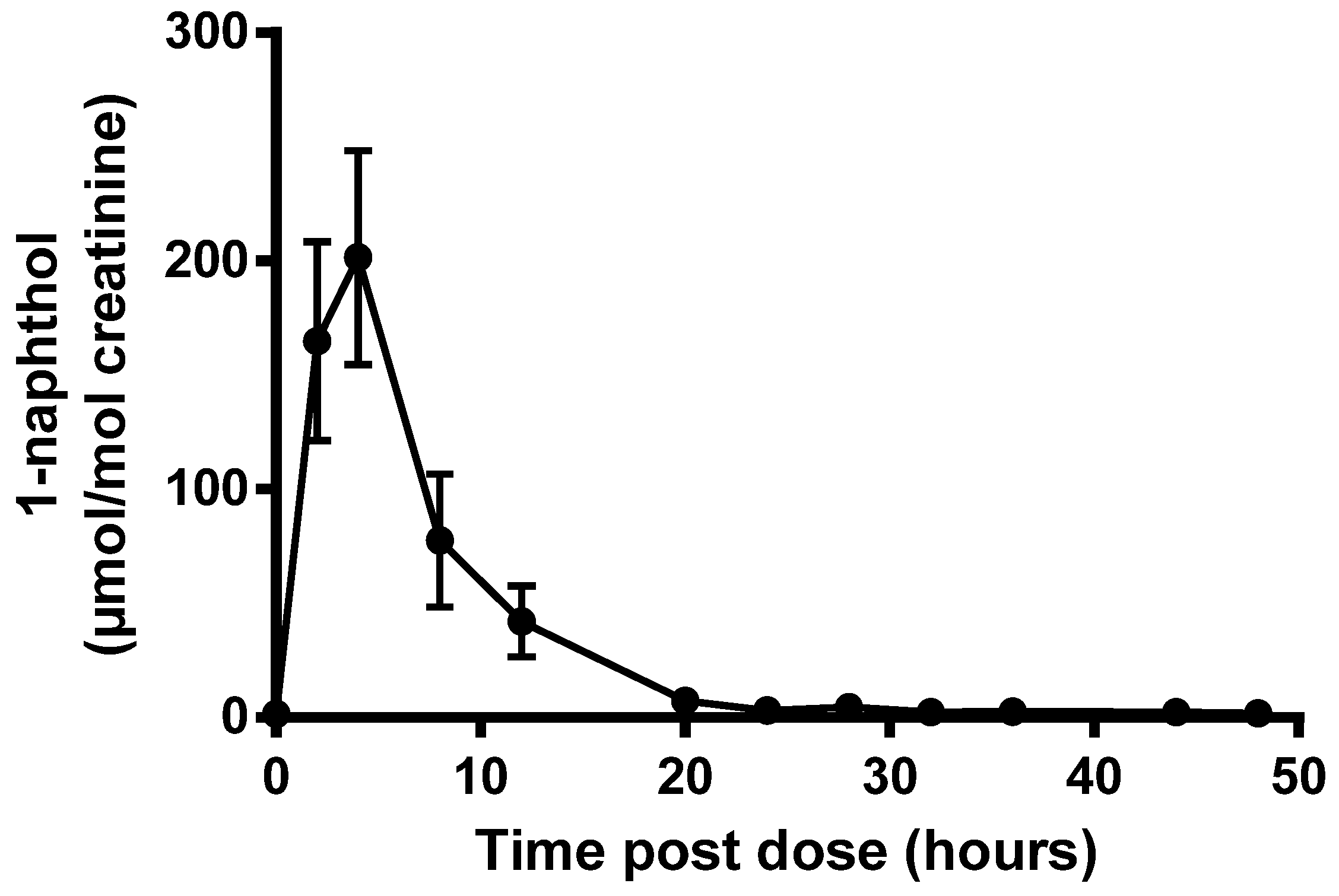
| Code | Excretion Half-Life (h) | 24 h Recovery (%) | Urinary 1-Naphthol (24 h Total) | |
|---|---|---|---|---|
| nmol/L | µmol/mol Creatinine | |||
| A | 2.5 | 43 | 572 | 84.3 |
| B | 3.3 | 27 | 397 | 48.1 |
| C | 2.7 | 11 | 588 | 57.9 |
| D | 4.7 | 11 | 308 | 21.3 |
| E | 4.8 | 17 | 216 | 30.3 |
| Mean | 3.6 | 22 | 416 | 48.4 |
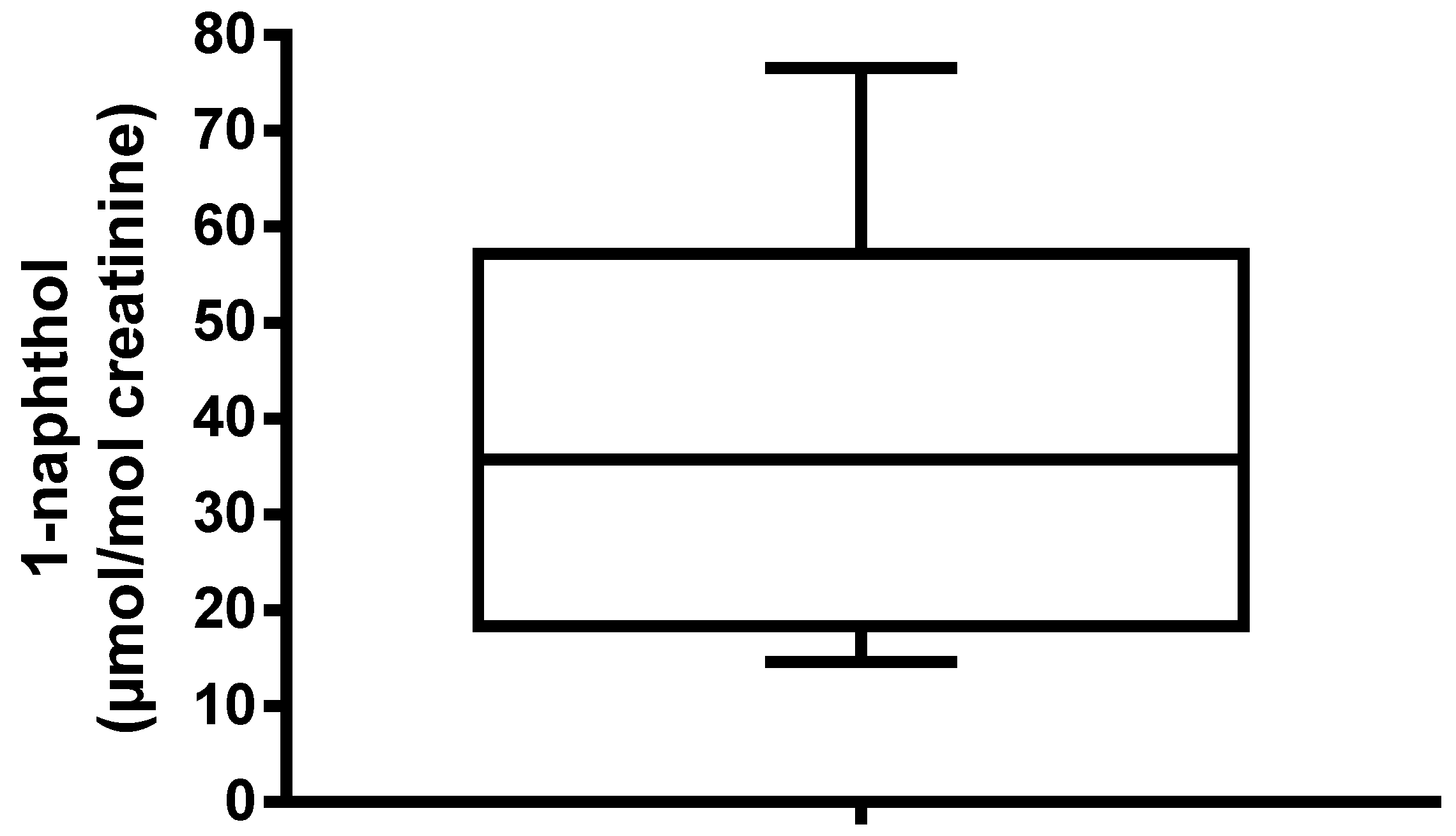
| Statistics | 1-Naphthol | 2-Naphthol | Ratio 1-/2-Naphthol a | Ratio 1-/2-Naphthol b |
|---|---|---|---|---|
| Min | <LoD | <LoD | 0.07 | 0.07 |
| 25th percentile | <LoD | 1.9 | 0.8 | 0.7 |
| Median | 4.2 | 4.0 | 1.4 | 1.3 |
| 75th percentile | 13.4 | 8.6 | 3.0 | 2.8 |
| Maximum | 1027 | 153 | 33.6 | 14.2 |
| Mean | 27.2 | 8.1 | - | - |
| Std deviation | 105 | 14.8 | - | - |
| n | 327 | 327 | 233 | 87 |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sams, C. Urinary Naphthol as a Biomarker of Exposure: Results from an Oral Exposure to Carbaryl and Workers Occupationally Exposed to Naphthalene. Toxics 2017, 5, 3. https://doi.org/10.3390/toxics5010003
Sams C. Urinary Naphthol as a Biomarker of Exposure: Results from an Oral Exposure to Carbaryl and Workers Occupationally Exposed to Naphthalene. Toxics. 2017; 5(1):3. https://doi.org/10.3390/toxics5010003
Chicago/Turabian StyleSams, Craig. 2017. "Urinary Naphthol as a Biomarker of Exposure: Results from an Oral Exposure to Carbaryl and Workers Occupationally Exposed to Naphthalene" Toxics 5, no. 1: 3. https://doi.org/10.3390/toxics5010003
APA StyleSams, C. (2017). Urinary Naphthol as a Biomarker of Exposure: Results from an Oral Exposure to Carbaryl and Workers Occupationally Exposed to Naphthalene. Toxics, 5(1), 3. https://doi.org/10.3390/toxics5010003