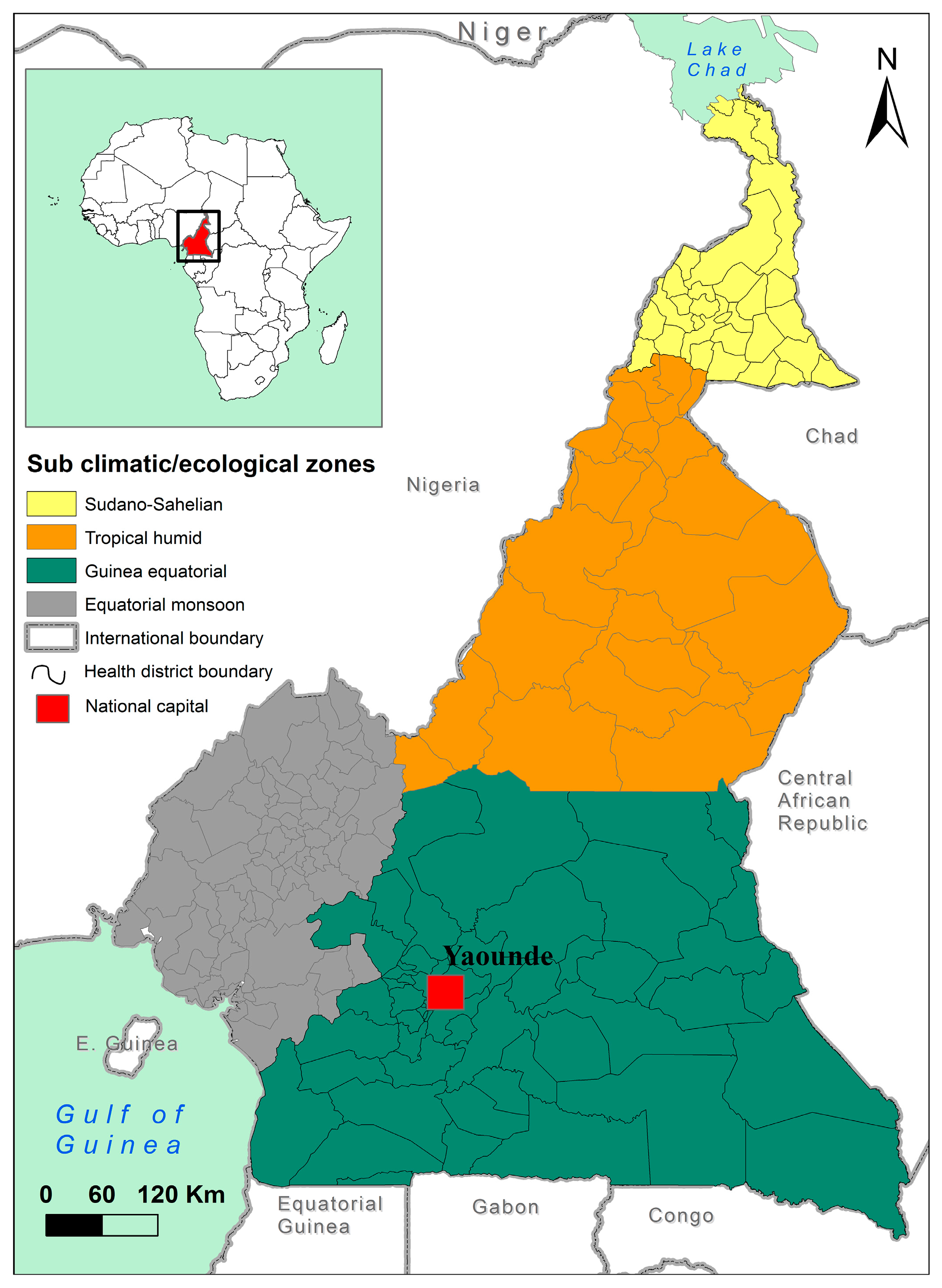
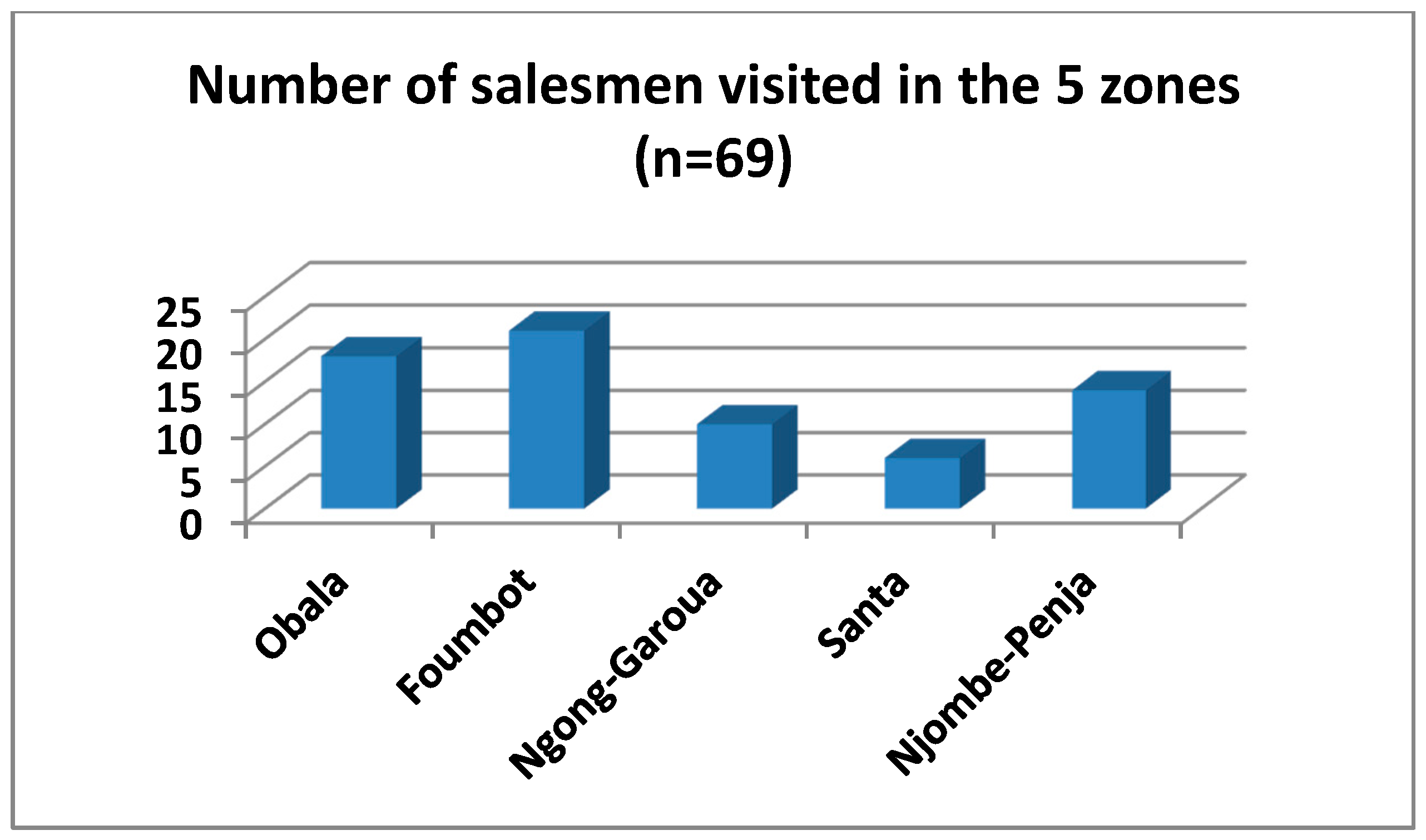
3.1. Distributors
In total, 69 pesticide sale-points were visited in the five agro-ecological zones (
Figure 2). Of the 69 persons surveyed, 35 were shop assistants and 17 shop owners. The west region had the greatest concentration of pesticide distributors (21), as many importers have a representation there.
In the northern regions, approved pesticides are difficult to find because of the absence of importers and the proximity with Nigeria. In this part of the country, pesticides are sold during the market day. Therefore, salesmen travel to different villages according to the markets’ calendar in the area. National regulation prohibits the sale of pesticides as goods; unfortunately, it is the most common sales strategy in the northern part of the country.
Pesticide vendors indicated that 16% of products sold are returned by farmers, dissatisfaction with the product efficacy accounting for 15% of returns and defective wrapping paper for 1.4%.
In total, 55% of pesticide shops do not have any store or warehouse. In practice, they have limited quantities, and newly supplied products stay in a corner of the shop. So, they have no knowledge on good storage practices as stipulated by the regulations that regulate the sale and distribution of phytosanitary products in Cameroon. In the same vein, the regulations stipulate that sale-points should be dedicated only to phytosanitary products; unfortunately, more than 50% of sale-points visited were not specialized. They all had a mixture of hardware, cosmetic and phytosanitary products, or often, a typical shop with different kinds of food products, and a corner for phytosanitary products.
In total, 65% of salesmen did not have a registration form for carrying inventory and for product traceability, and 76% had no security information MSDSs (Material Safety Data Sheets) for the products they had. In the northern part of the country, more than half of the sale-points repack pesticides into a new bottle. In total, 17% were confirmed to repack pesticides in small quantities to meet farmers’ demands.
Overall, 94% of sellers were aware of the harmful effects of pesticides, but only 55% were able to cite some of these effects.
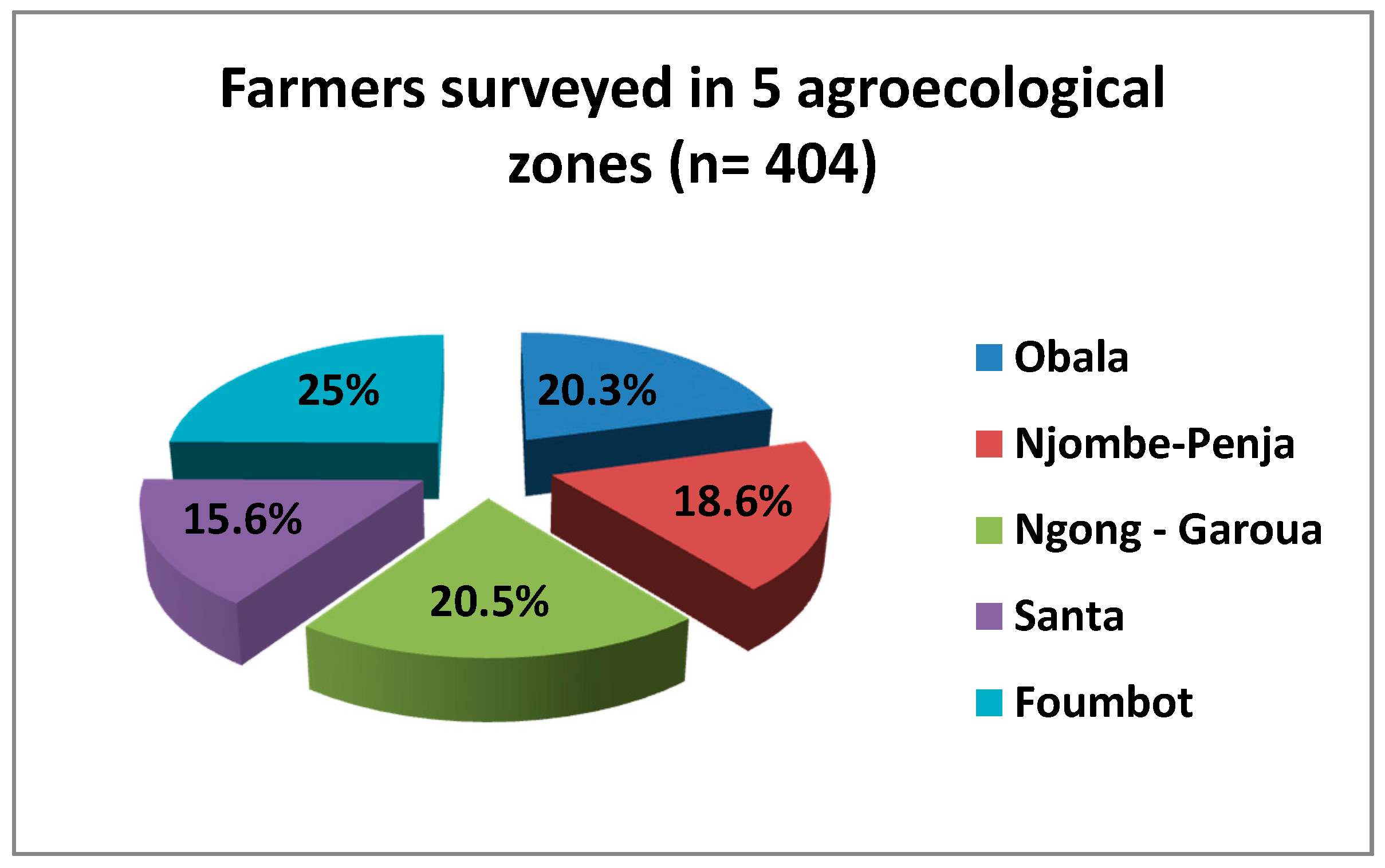
3.2. Farmers
A total of 404 farmers were surveyed in the five agro-ecological zones visited, as indicate in
Figure 3.
Farmers were interviewed in their farms, homes, headquarters of their union and market places. Farmers’ ages varied between 20- and 79-years old.
Table 3 gives the mean, minimum and maximum age of farmers surveyed.
In total, 69% of farmers visited were women. They are involved in all steps of the farm work. It was noticed that, in the northern part of the country, more than 94% of pesticide application is carried out by men. In total, 51% of farmers stopped their education at the primary-school level, and only 10% attended university. Moreover, 80% of persons interviewed indicated farming as their sole activity. In total, 62% of them use less than two hectares of farming land, with less than five workers, who most often are members of the same family.
3.2.1. Main Cultures
Agricultural products vary between villages within the same zones and between agro-ecological zones; however, the five main crops represent between 62% and 81.5% of the overall produce, as seen in
Table 4.
3.2.2. Most Used Pesticides
The most widely-used pesticide is related to the main agricultural products in the main surveyed sites and surrounding villages.
Table 5 is a synopsis of the most used pesticides (top 5). The cumulative percentage of these top-five pesticides represents from 40% to 80% of the overall pesticides in circulation in those zones. In Obala sites, where cocoa is the main culture, fungicides containing metalaxyl (Ridomil, Callomil and Plantomil) are the most used products, followed by insecticides (Actara, Onex, Parastar and Lamida Gold). Some of the active substances are metalaxyl and imidaclopride. It was also noted that the insecticide Lamida Gold is used in the Obala zone, while the product is homologated for use on tomatoes; this may suggest possible misuse. In the four other zones, Gramoxone and Roundup appear to be the most used pesticides. However, it was noted that Gramoxone was no longer approved for use in Cameroon. However, because Gramoxone has been used for a long time by certain farmers, when purchasing their pesticides, some farmers continued to request Gramoxone, without knowing that it is no longer in circulation. Salesmen say that in such cases, they provide farmers with a paraquat equivalent.
Glyphosate products are the most used herbicide in each zone (Roundup and Glyphader). It was difficult to identify certain products used by farmers because many did not remember the name of the pesticide, and they used local names such as “timides” to generally designate insecticides.
The specificity of phytosanitaries and pesticides used in the northern part of the country is quite obvious compared to other regions, but reflects the particularities of their production. Atrazine and Diuron are mostly used here, but they are not found elsewhere; both products are used for cotton production.
3.2.3. Pesticide Risk Perceptions by Farmers
Concerning health risks related to pesticide exposure, 78% of farmers (n = 399) were said to be aware. In total, 15% of them consider that the most important risks are cutaneous problems, 13% by ingestion, 10% ocular difficulties. Cutaneous diseases are perceived as the most important problem in Obala, where cocoa is the most dominant crop and where atomizers are used for spraying; and also in Njombe–Penja, where aerial sprays are made by certain industries. In Foumbot, Santa and Ngong, inhalation and ingestion came first.
In total, 49% (n = 281) of farmers declared that pesticides are useful for a good production; 4.2% were aware that they can be hazardous for human health and 2% that they can be hazardous for the environment.
When a pesticide is opened and not fully used, 59% of farmers keep the rest at home for reuse, and 16% kept in the farm. In total, 46% of farmers (n = 389) dispose of empty packages of pesticides on their farms, 7.2% bury them on the farm, 27.5% burn them, 6.2% keep them at home and 3% reuse empty packages for domestic purposes.
The labelling of these pesticide products encourages users to return empty packages to the distributors, but unfortunately, no mechanism in place to help farmers, who are mostly in rural areas and own small farms in Cameroon. In total, 90% (n = 373) of farmers indicated that they have no incentive to return empty pesticide packages.
In total, 80% of farms are near to a water point (river, well, backwater), and 63% of these water points are less than 25 m from farms. In total, 41% of farmers used water from these water points for domestic uses. After pesticide treatment, the rest of the products are poured in the nearby water points and sprayers are also washed there. As possible effects of pesticide disposal on their farm, 56% had witnessed the disappearance of certain living organisms: birds, fish, lizards, spiders, snakes, caterpillars, locusts, squirrels, butterflies, flies, grasshoppers, wasps, ants, frogs, snails, bees, mice, rats, antelopes, partridges, monkeys and guinea-fowls.
3.2.4. Suspected Poisoning Cases
In relation to the question of whether they have ever experienced a pesticide poisoning situation, 40.3% of farmers (
n = 395) reported having had at least one case. Cutaneous (eye and skin) and inhalation problems appear to be most common, as shown in
Table 6.
Once exposed to a pesticide, farmers based in rural areas declared using different types of first-aid measures, depending on the case. It was noted that they were not aware of the warning and measures written on the product label. Commonly used actions include the following: for cutaneous contact, wash the contaminated part with clean water or clean water and soap; for ingestion, swallow red oil or drink milk, local white wine or citrus juice; for eye contact, wash with water. After these first-aid actions, they may consider going to the hospital depending on the evolution of the case.
In total, 32.8% of farmers interviewed (n = 381) asserted to have witnessed a pesticide accident. In total, 85% of victims were male, with age ranging from 2 to 84 years old. In total, 54.3% of cases were cutaneous problems, against 26.7% ingestion and 17.2% inhalation.
3.2.5. Most Incriminated Pesticides
Concerning themselves, 158 farmers interviewed declared to have experienced at least one case of pesticide accident during manipulation, as shown in
Figure 4.
Each of the agro-ecological zones was affected, and 80% of persons involved were male.
In Ngong–Garoua, 24 cases were declared by farmers, Roundup herbicide was cited six times (five cutaneous and one inhalation), Gramoxone in four cases (two inhalation, one cutaneous and one eye contact), three cases for Atrazine (two cutaneous and one inhalation) and four cases for Thioral (cutaneous). In seven other cases, farmers were not able to identify the product.
Table 7 gives a synopsis of the most incriminated pesticides by farmers and by agro-ecological zones.
Among the most frequent signs and symptoms that appear after exposure to pesticides are itching and irritation, skin and eye problems, respiratory stress, tiredness, headache, vomiting and diarrhea.
Only 51.8% of farmers wear personal protective equipment, and moreover, even this equipment is incomplete or inappropriate. For example, 11.7% wore only boots. For plant treatment, 85% used a sprayer of 15 liters, 2% atomizers and 2% hand sprayer (2 liters). In total, 70% of farmers sprayed less than 10 liters per hectare, after dilution with water (89%). Pesticide treatments are done early in the morning, before 10 a.m. (for 87% of farmers). First treatments are applied between March and May for 60% of them, and last treatment between August and November for 58%.
Concerning the number of years they have been using pesticides, 33% of farmers said between 10 and 19 years, 32% between 1 and 9 years, 22% between 20 and 29 years, 20% between 30 and 39 years, 4% between 40 to 49 years and 1% for more than 50 years. Moreover, 57% affirmed not to be aware of good agricultural practices.
Despite their understanding of health risks from pesticide handling and previous cases of accidents experienced, 80% of farmers did not have any medical follow-up. Some of the farmers working with enterprises, specifically in the Njombe–Penja and Ngong–Garoua regions, were affiliated to a local health center where they were admitted for medical examination. In addition, few enterprises were found to have a health center for first-aid treatment and medical follow-up.
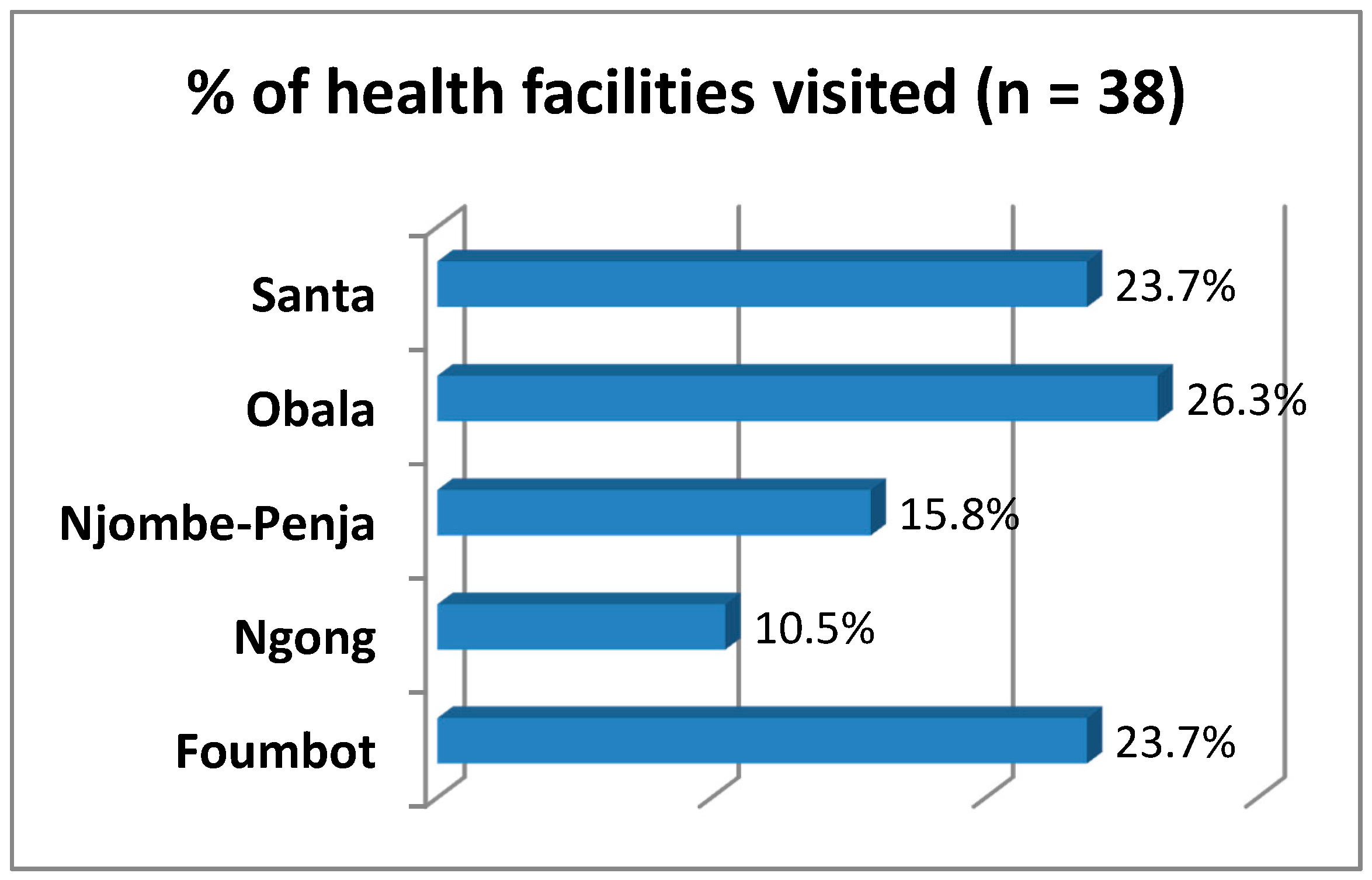
3.2.6. Health Personnel
To understand the level of preparedness of local healthcare centers and hospitals to manage pesticide poisoning cases, 38 health establishments in 24 villages of the five agro-ecological zones were visited (
Figure 5).
In each locality where farmers were interviewed, nearby healthcare centers were also included and health personnel interviewed. In accordance with the organization of the Cameroonian health system, 38 healthcare establishments visited belonged to three categories: 40% were hospitals, 34% were classified health centers and 26% were integrated health centers.
Each time the survey team entered a healthcare establishment, an authorization letter signed by the Minister of Public Health was presented to the head of the structure. Then, a preliminary interview was done to understand the itinerary of patients and particularly patients complaining or showing signs and symptoms of pesticide poisoning. Thereafter, one to two health personnel suspected of being part of this chain were interviewed to gather information from their experience; where possible, registrations and archives for suspected cases were consulted. Overall, 42% of health personnel were medical doctors, and 21% nurses. The remaining personnel were nursing auxiliaries (8%), heads of the health centers (11%), pharmacists (3%) and midwives (2%).
In total, 61% of health personnel were not able to cite the name of at least one pesticide used by farmers of the locality. Others could cite, even using the common names, one to four of them. In total, 38 health workers from the 24 villages cited only 17 pesticide formulations out of the 600 approved for use in the country (Actara, Dursban, Diuron, Gramoxone, glyphosate, Roundup, Lamida, Manisan, Mocab cethomophos, Pyriforce, oxaplant, Ridomil, callomil, timide, Manozan, Kung-fu). In total, 4% cited names of fertilizers instead of pesticides.
In total, 79% of health workers claimed to have never followed a course or training module on pesticide poisoning management, even in the medical studies curriculum. Some had done courses on the management of food intoxications and snake bites.
For all the healthcare settings visited, 56 cases of pesticide poisoning were declared between 2011 and September 2016. In addition, 58% (n = 38) of health personnel interviewed claimed to be aware of other suspected poisoning cases in other health facilities with which they collaborated. In total, 78% of poisoning cases were accidental, 12% suicide attempts, 4% criminal (in the area of Njombe–Penja, thieves, when arrested, are injected with Gramoxone).
In more than 60% of cases, the pesticide products suspected to be the cause of the accidents could not be identified. The most frequently identified pesticide active ingredients in poisoning cases were cypermethrin, glyphosate, paraquat and metalaxyl. The most recurrent product names were Roundup (16%), Gramoxone (13%) and “Timides” (11%). “Timides” can also be considered as a non-identified product, as it is a common name used to designate insecticides in general.
With regard to the age of patients (n = 31), 19% were children, 26% adolescents and 55% adults. As for the gender, 73% of suspected patients of pesticide poisoning were male.
Circumstances of poisoning vary: 27% during spraying, 20% by ingestion (drinking, food contaminated by hands that have been used to manipulate pesticides), 13% occurred at home, 7% in the kitchen, and 3% during fishing.
Clinical signs said to be shown by patients included vomiting (18%), salivation (11%), indistinct vision (11%), respiratory difficulties (9%), convulsions (7%), asthenia (7%), dizziness (6%), headache (6%) and stomach problems (6%), among others.
In total, 71% of cases were hospitalized between 1 and 14 days, with 79% who recovered and 21% who died.
Treatment varied from case to case depending on the situation of the patients, category of the centers, the level of preparedness of the healthcare center and the knowledge of the health worker who handled the patient. A synopsis of recurrent treatments and drugs delivered to 32 patients in the health settings visited included (i) administration of antihistamine, antibiotic and anti-inflammatory; (ii) administration of atropine, stomach washing; (iii) drip, administration of dexamethasone and atropine; (iv) administration of bicarbonate and rehydration salts; (v) administration of corticoids and antibiotic drugs; (vi) dexamethasone, anti-inflammatory drugs and amoxicillin; (vii) dexamethasone and non-sugar milk; (viii) red oil administration; (ix) use of a ringer solution and cymethidin injection. Because of the absence of standardized management procedures, health personnel act according to their understanding of the case. We found that certain rural health centers collected empty packages of some pesticides used by farmers in their localities and used them to identify suspected products when a patient arrived.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}