Urinary Cadmium Threshold to Prevent Kidney Disease Development




Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Ascertainment of Long-Term Cadmium Exposure Levels
2.3. Clinical Kidney Function Measure and Assessment of Tubular and Glomerular Integrity
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Subjects
3.2. CKD Prevalence Associated with Tubular Dysfunction and Cadmium Exposure
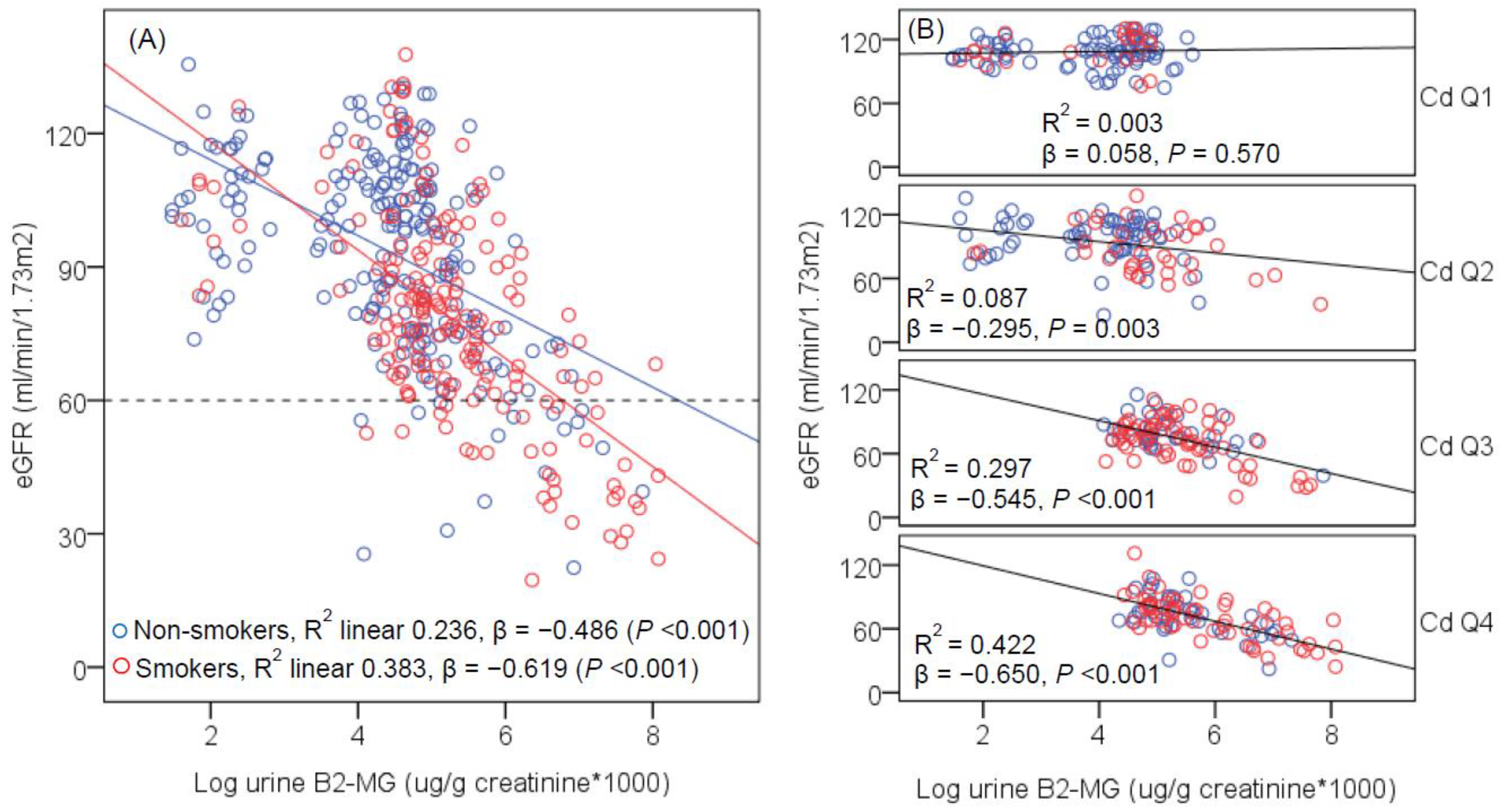
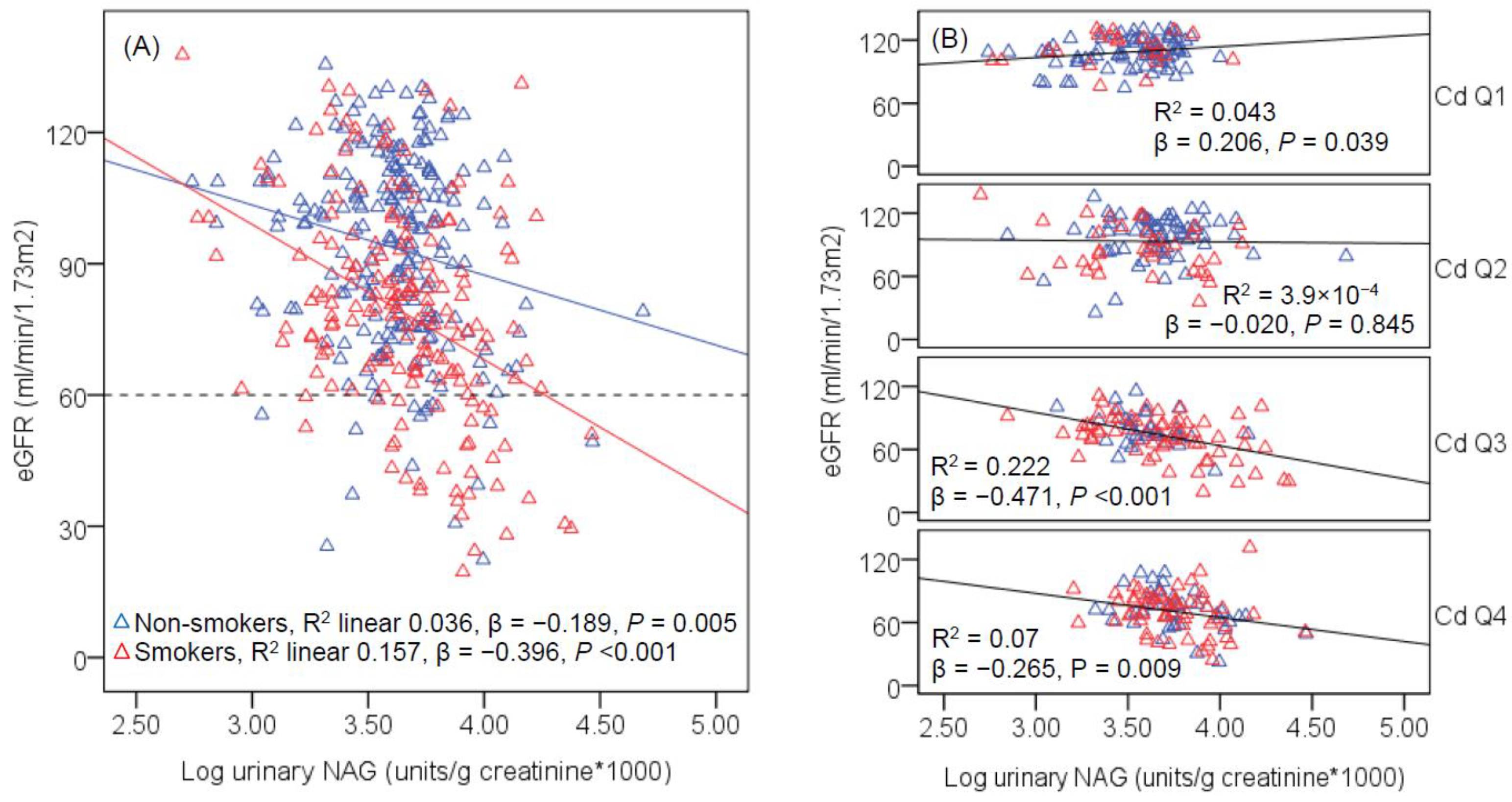
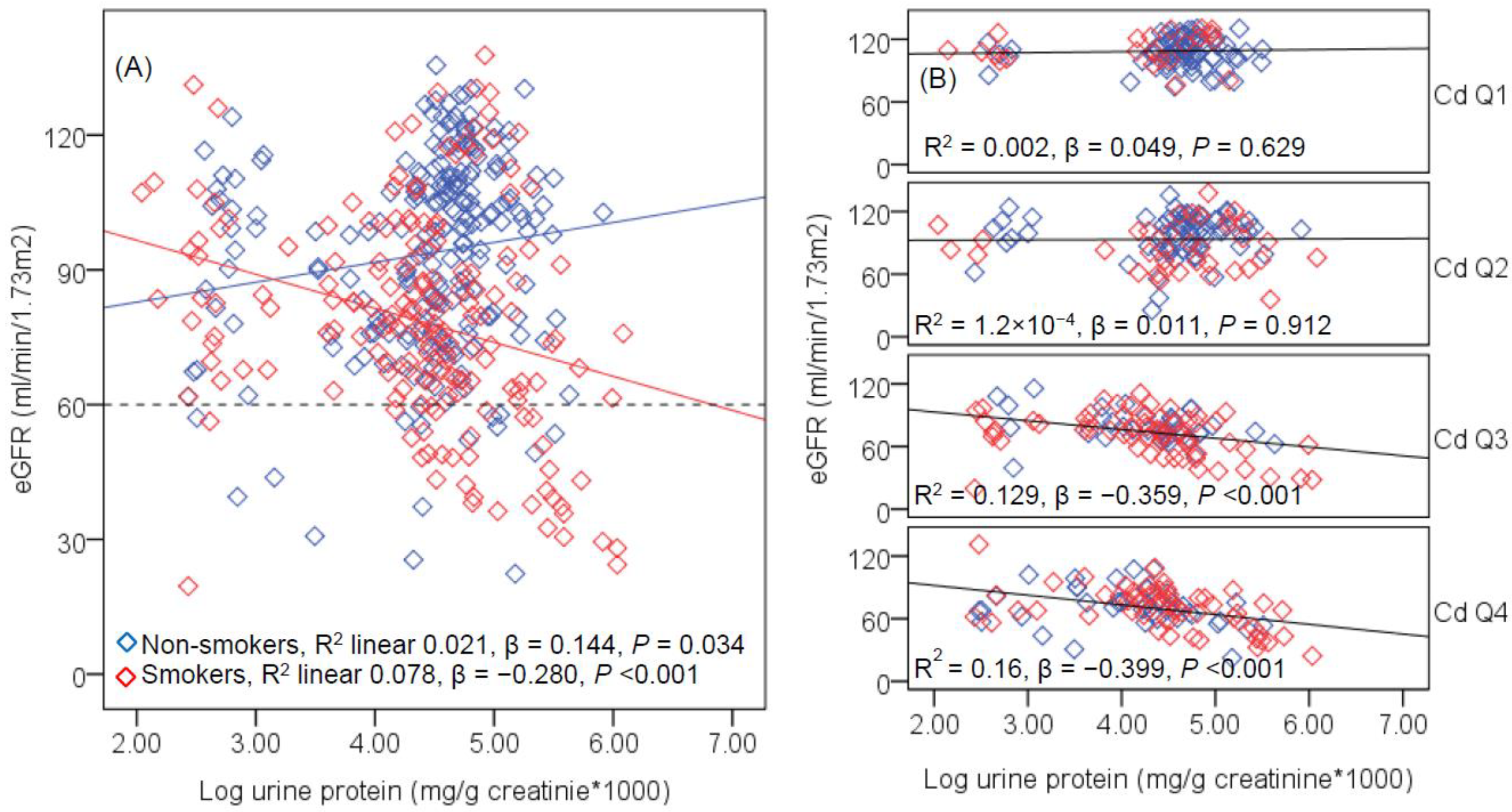
3.3. Effect Size Estimates
3.4. Evidence for Urinary Cd Threshold Level
4. Discussion
5. Conclusions
6. Strengths and Limitations
Author Contributions
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Cadmium, Department of Health and Humans Services, Public Health Service, Centers for Disease Control and Prevention, Atlanta, GA, USA. 2012. Available online: http://www.atsdr.cdc.gov/toxprofiles/tp5.pdf (accessed on 8 March 2018).
- Satarug, S. Dietary cadmium intake and its effects on kidneys. Toxics 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Current health risk assessment practice for dietary cadmium: Data from different countries. Food Chem. Toxicol. 2017, 106, 430–445. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Health risk assessment of dietary cadmium intake: Do current guidelines indicate how much is safe? Environ. Health Perspect. 2017, 125, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, O.; Tharaux, P.L.; Huber, T.B. Autophagy in kidney disease and aging: Lessons from rodent models. Kidney Int. 2016, 90, 950–964. [Google Scholar] [CrossRef] [PubMed]
- Gobe, G.; Crane, D. Mitochondria, reactive oxygen species and cadmium toxicity in the kidney. Toxicol. Lett. 2010, 198, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Lee, J.Y.; Tokumoto, M.; Satoh, M. Cadmium renal toxicity via apoptotic pathways. Biol. Pharm. Bull. 2012, 35, 1892–1897. [Google Scholar] [CrossRef] [PubMed]
- Buchet, J.P.; Lauwerys, R.; Roels, H.; Bernard, A.; Bruaux, P.; Claeys, F.; Ducoffre, G.; de Plaen, P.; Staessen, J.; Amery, A.; et al. Renal effects of cadmium body burden of the general population. Lancet 1990, 336, 699–702. [Google Scholar] [CrossRef]
- Wu, X.; Jin, T.; Wang, Z.; Ye, T.; Kong, Q.; Nordberg, G. Urinary calcium as a biomarker of renal dysfunction in a general population exposed to cadmium. J. Occup. Environ. Med. 2001, 43, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Nishijo, M.; Satarug, S.; Honda, R.; Tsuritani, I.; Aoshima, K. The gender differences in health effects of environmental cadmium exposure and potential mechanisms. Mol. Cell Biochem. 2004, 255, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Nishijo, M.; Ujjin, P.; Moore, M.R. Chronic exposure to low-level cadmium induced zinc-copper dysregulation. J. Trace Elem. Med. Biol. 2018, 46, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Teeyakasem, W.; Nishijo, M.; Honda, R.; Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W. Monitoring of cadmium toxicity in a Thai population with high-level environmental exposure. Toxicol. Lett. 2007, 169, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Honda, R.; Swaddiwudhipong, W.; Nishijo, M.; Mahasakpan, P.; Teeyakasem, W.; Ruangyuttikarn, W.; Satarug, S.; Padungtod, C.; Nakagawa, H. Cadmium induced renal dysfunction among residents of rice farming area downstream from a zinc-mineralized belt in Thailand. Toxicol. Lett. 2010, 198, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Li, M.; Han, T.X.; Chen, J.W.; Ye, L.X.; Wang, Q.; Zhou, Y.K. Benchmark dose estimation for cadmium-induced renal tubular damage among environmental cadmium-exposed women aged 35–54 years in two counties of China. PLoS ONE 2014, 9, e115794. [Google Scholar] [CrossRef] [PubMed]
- Wallin, M.; Sallsten, G.; Lundh, T.; Barregard, L. Low-level cadmium exposure and effects on kidney function. Occup. Environ. Med. 2014, 71, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Akerstrom, M.; Barregard, L.; Lundh, T.; Sallsten, G. The relationship between cadmium in kidney and cadmium in urine and blood in an environmentally exposed population. Toxicol. Appl. Pharmacol. 2013, 268, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Nakatsuka, H.; Watanabe, T.; Shimbo, S. Estimation of daily cadmium intake from cadmium in blood or cadmium in urine. Environ. Health Prev. Med. 2015, 20, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, E.; Suwazono, Y.; Uetani, M.; Kido, T.; Nishijo, M.; Nakagawa, H.; Nogawa, K. Tolerable level of lifetime cadmium intake estimated as a benchmark dose low, based on excretion of β2-microglobulin in the cadmium-polluted regions of the Kakehashi River Basin, Japan. Bull. Environ. Contam. Toxicol. 2006, 76, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Lei, L.; Nilsson, J.; Li, H.; Nordberg, M.; Bernard, A.; Nordberg, G.F.; Bergdahl, I.A.; Jin, T. Renal function after reduction in cadmium exposure: An 8-year follow-up of residents in cadmium-polluted areas. Environ. Health Perspect. 2012, 120, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, P.M.; Costanzi, S.; Naticchia, A.; Sturniolo, A.; Gambaro, G. Low level exposure to cadmium increases the risk of chronic kidney disease: Analysis of the NHANES 1999–2006. BMC Public Health 2010, 10, 304. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.S.; Ho, W.C.; Caffrey, J.L.; Sonawane, B. Low serum zinc is associated with elevated risk of cadmium nephrotoxicity. Environ. Res. 2014, 134, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood cadmium and lead and chronic kidney disease in US adults: A joint analysis. Am. J. Epidemiol. 2009, 170, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Hyun, Y.Y.; Lee, K.B.; Chang, Y.; Ryu, S.; Oh, K.H.; Ahn, C. Environmental heavy metal exposure and chronic kidney disease in the general population. J. Korean Med. Sci. 2015, 30, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Taylor, A.W.; Riley, M.; Byles, J.; Liu, J.; Noakes, M. Association between dietary patterns, cadmium intake and chronic kidney disease among adults. Clin. Nutr. 2017, 5614, 31366–31368. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Nishijo, M.; Ujjin, P.; Vanavanitkun, Y.; Moore, M.R. Cadmium-induced nephropathy in the development of high blood pressure. Toxicol. Lett. 2005, 157, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 12, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Bolton, K.; Culleton, B.; Harvey, K.S.; Ikizler, T.A.; Johnson, C.A.; Kausz, A.; Kimmel, P.L.; Kusek, J.; et al. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- European Food Safety Authority (EFSA). Statement on tolerable weekly intake for cadmium. EFSA J. 2011, 9. Available online: http://www.efsa.europa.eu/en/efsajournal/doc/1975.pdf (accessed on 8 March 2018).
- FAO/WHO. Food and Agriculture Organization of the United Nations. In Proceedings of the Seventy-third Meeting, Geneva, Switzerland, 8–17 June 2010; Summary and Conclusions. Available online: http://www.who.int/foodsafety/publications/chem/summary73.pdf (accessed on 8 March 2018).
- Nakhoul, N.; Batuman, V. Role of proximal tubules in the pathogenesis of kidney disease. Contrib. Nephrol. 2011, 169, 37–50. [Google Scholar] [PubMed]
- Dieterle, F.; Perentes, E.; Cordier, A.; Roth, D.R.; Verdes, P.; Grenet, O.; Pantano, S.; Moulin, P.; Wahl, D.; Mahl, A.; et al. Urinary clusterin, cystatin C, β2-microglobulin and total protein as markers to detect drug-induced kidney injury. Nat. Biotechnol. 2010, 28, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Kuwata, K.; Nakamura, I.; Ide, M.; Sato, H.; Nishikawa, S.; Tanaka, M. Comparison of changes in urinary and blood levels of biomarkers associated with proximal tubular injury in rat models. J. Toxicol. Pathol. 2015, 28, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.H.; Roumelioti, M.E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering beta-2 microglobulin as a biomarker across the spectrum of kidney diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef] [PubMed]
- Kudo, K.; Konta, T.; Mashima, Y.; Ichikawa, K.; Takasaki, S.; Ikeda, A.; Hoshikawa, M.; Suzuki, K.; Shibata, Y.; Watanabe, T.; et al. The association between renal tubular damage and rapid renal deterioration in the Japanese population: The Takahata study. Clin. Exp. Nephrol. 2011, 15, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Mashima, Y.; Konta, T.; Kudo, K.; Takasaki, S.; Ichikawa, K.; Suzuki, K.; Shibata, Y.; Watanabe, T.; Kato, T.; Kawata, S.; et al. Increases in urinary albumin and beta2-microglobulin are independently associated with blood pressure in the Japanese general population: The Takahata Study. Hypertens. Res. 2011, 34, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Hwangbo, Y.; Weaver, V.M.; Tellez-Plaza, M.; Guallar, E.; Lee, B.K.; Navas-Acien, A. Blood cadmium and estimated glomerular filtration rate in Korean adults. Environ. Health Perspect. 2011, 119, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Buser, M.C.; Ingber, S.Z.; Raines, N.; Fowler, D.A.; Scinicariello, F. Urinary and blood cadmium and lead and kidney function: NHANES 2007–2012. Int. J. Hyg. Environ. Health 2016, 219, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, G.L. Cadmium risk assessment in relation to background risk of chronic kidney disease. J. Toxicol. Environ. Health 2012, 75, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Akesson, A.; Lundh, T.; Vahter, M.; Bjellerup, P.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Strömberg, U.; Skerfving, S. Tubular and glomerular kidney effects in Swedish women with low environmental cadmium exposure. Environ. Health Perspect. 2005, 113, 1627–1631. [Google Scholar] [CrossRef] [PubMed]
- Haswell-Elkins, M.; Imray, P.; Satarug, S.; Moore, M.R.; O’dea, K. Urinary excretion of cadmium among Torres Strait Islanders (Australia) at risk of elevated dietary exposure through traditional foods. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 372–377. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptors/Variables | All Subjects n = 395 | Men n = 193 | Women n = 202 | p Values |
| Age (years) | 48.8 ± 14.0 | 47.4 ± 15.8 | 50.1 ± 12.0 | 0.024 |
| BMI (kg/m2) | 22.2 ± 3.8 | 22.0 ± 3.4 | 22.4 ± 4.1 | 0.387 |
| Smoking prevalence (%) a | 45.1 | 66.8 | 24.3 | <0.001 |
| Hypertension (%) b | 21.7 | 24.2 | 19.3 | 0.240 |
| eGFR (mL/min/1.73 m2) | 86.9 ± 24.2 | 87.2 ± 25.0 | 86.6 ± 23.5 | 0.717 |
| CKD prevalence (%) | 12.7 | 13 | 12.4 | 0.863 |
| Exposure indicators | ||||
| Urinary creatinine (mg/dL) | 100.2 ± 67.7 | 115.1 ± 71.7 | 85.8 ± 60.5 | <0.001 |
| Urinary Cd concentration (μg/L) | 6.65 ± 10.70 | 7.48 ± 12.71 | 5.87 ± 8.29 | 0.930 |
| Urinary Cd (μg/g creatinine) | 5.93 ± 7.69 | 5.43 ± 7.60 | 6.41 ± 7.77 | 0.061 |
| Urinary Cd >1 μg/g creatinine (%) c | 55.9 | 53.4 | 58.4 | 0.312 |
| Urinary Cd >5.24 μg/g creatinine (%) d | 40.3 | 37.3 | 43.1 | 0.243 |
| Renal pathology markers | ||||
| β2-MG (mg/g creatinine) | 2.68 ± 12.43 | 3.35 ± 13.87 | 2.04 ± 10.88 | 0.973 |
| β2-MG ≥ 1 mg/g creatinine (%) e | 14.2 | 17.1 | 11.4 | 0.104 |
| NAG (Units/ g creatinine) | 5.31 ± 4.26 | 4.98 ± 3.50 | 5.63 ± 4.86 | 0.103 |
| Total protein (mg/g creatinine) | 75.6 ± 142 | 74.7 ± 144 | 76.4 ± 141 | 0.200 |
| Reported health status (%) | ||||
| No disease | 66.7 | 67.4 | 66.0 | 0.901 |
| Anemia | 6.2 | 4.7 | 7.6 | 0.221 |
| Hypertension | 15.5 | 16.3 | 14.7 | 0.796 |
| Diabetes | 2.8 | 3.2 | 2.5 | 0.763 |
| Osteoporosis | 3.1 | 0.5 | 5.6 | 0.004 |
| Kidney disease | 3.1 | 4.7 | 1.5 | 0.083 |
| Urinary stones | 1.6 | 1.6 | 1.5 | 1.000 |
| Others | 1.0 | 1.6 | 0.5 | 0.317 |
| Independent Variables | POR of CKD | 95% CI for POR | p Values | |
|---|---|---|---|---|
| Lower | Upper | |||
| Gender | 0.771 | 0.317 | 1.876 | 0.566 |
| Age (years) | 1.119 | 1.070 | 1.170 | <0.001 |
| BMI (kg/m2) | 1.188 | 1.071 | 1.318 | 0.001 |
| Smoking | 1.002 | 0.378 | 2.661 | 0.996 |
| Tubular dysfunction a | 5.324 | 2.035 | 13.928 | 0.001 |
| Log urine Cd (μg/g creatinine) | 2.978 | 1.066 | 8.317 | 0.037 |
| Log urine NAG (units/g creatinine) | 1.340 | 0.231 | 7.770 | 0.744 |
| Log urine protein (mg/g creatinine) | 1.900 | 1.093 | 3.302 | 0.023 |
| Factors and Covariates | Degree of Freedom | eGFR (mL/min/1.73 m2) | ||
|---|---|---|---|---|
| F | p | η2 | ||
| Corrected Model | 19 | 43.715 | <0.001 | 0.689 |
| Intercept | 1 | 219.823 | <0.001 | 0.370 |
| Age (years) | 1 | 214.578 | <0.001 | 0.364 |
| BMI (kg/m2) | 1 | 10.484 | 0.001 | 0.027 |
| Smoking | 1 | 0.082 | 0.775 | 0.000 |
| Gender | 1 | 1.347 | 0.247 | 0.004 |
| Log urine β2-MG (μg/g creatinine) | 1 | 12.800 | <0.001 | 0.033 |
| Log urine NAG (units/g creatinine) | 1 | 0.275 | 0.600 | 0.001 |
| Log urine protein (mg/g creatinine) | 1 | 2.405 | 0.122 | 0.006 |
| Urinary Cd quartiles | 3 | 6.765 | <0.001 | 0.051 |
| Gender × smoking | 1 | 3.161 | 0.076 | 0.008 |
| Urinary Cd quartiles × smoking | 3 | 3.747 | 0.011 | 0.029 |
| Urinary Cd quartiles × gender | 3 | 0.890 | 0.446 | 0.007 |
| Urinary Cd quartiles × gender × smoking | 2 | 2.032 | 0.133 | 0.011 |
| Error | 375 | |||
| Total | 395 | |||
| Corrected Total | 394 | |||
| Independent Variables | eGFR (mL/min/1.73 m2) | |||
|---|---|---|---|---|
| Standardized | 95% CI for β | p Value | ||
| β coefficients | Lower | Upper | ||
| Age (years) | −0.548 | −1.084 | −0.812 | <0.001 |
| BMI (kg/m2) | −0.105 | −1.068 | −0.288 | 0.001 |
| Gender | 0.066 | −0.017 | 6.435 | 0.051 |
| Smoking | −0.002 | −3.543 | 3.397 | 0.967 |
| Log urine Cd (μg/g creatinine) | −0.234 | −10.900 | −4.976 | <0.001 |
| Log urine β2-MG (μg/g creatinine) | −0.178 | −4.773 | −1.808 | <0.001 |
| Log urine NAG (units/g creatinine) | 0.004 | −5.042 | 5.780 | 0.893 |
| Log urine protein (mg/g creatinine) | −0.037 | −2.982 | 0.736 | 0.236 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satarug, S.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Urinary Cadmium Threshold to Prevent Kidney Disease Development. Toxics 2018, 6, 26. https://doi.org/10.3390/toxics6020026
Satarug S, Ruangyuttikarn W, Nishijo M, Ruiz P. Urinary Cadmium Threshold to Prevent Kidney Disease Development. Toxics. 2018; 6(2):26. https://doi.org/10.3390/toxics6020026
Chicago/Turabian StyleSatarug, Soisungwan, Werawan Ruangyuttikarn, Muneko Nishijo, and Patricia Ruiz. 2018. "Urinary Cadmium Threshold to Prevent Kidney Disease Development" Toxics 6, no. 2: 26. https://doi.org/10.3390/toxics6020026
APA StyleSatarug, S., Ruangyuttikarn, W., Nishijo, M., & Ruiz, P. (2018). Urinary Cadmium Threshold to Prevent Kidney Disease Development. Toxics, 6(2), 26. https://doi.org/10.3390/toxics6020026