
Local Toxicity of Biocides after Direct and Aerosol Exposure on the Human Skin Epidermis and Airway Tissue Models

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Biocidal Substances and Other Chemicals
2.2. 3D Reconstructed Human Epidermis Model (KeraSkinTM)
2.3. 3D Reconstructed Human Airway Mucosa Model (SoluAirwayTM)
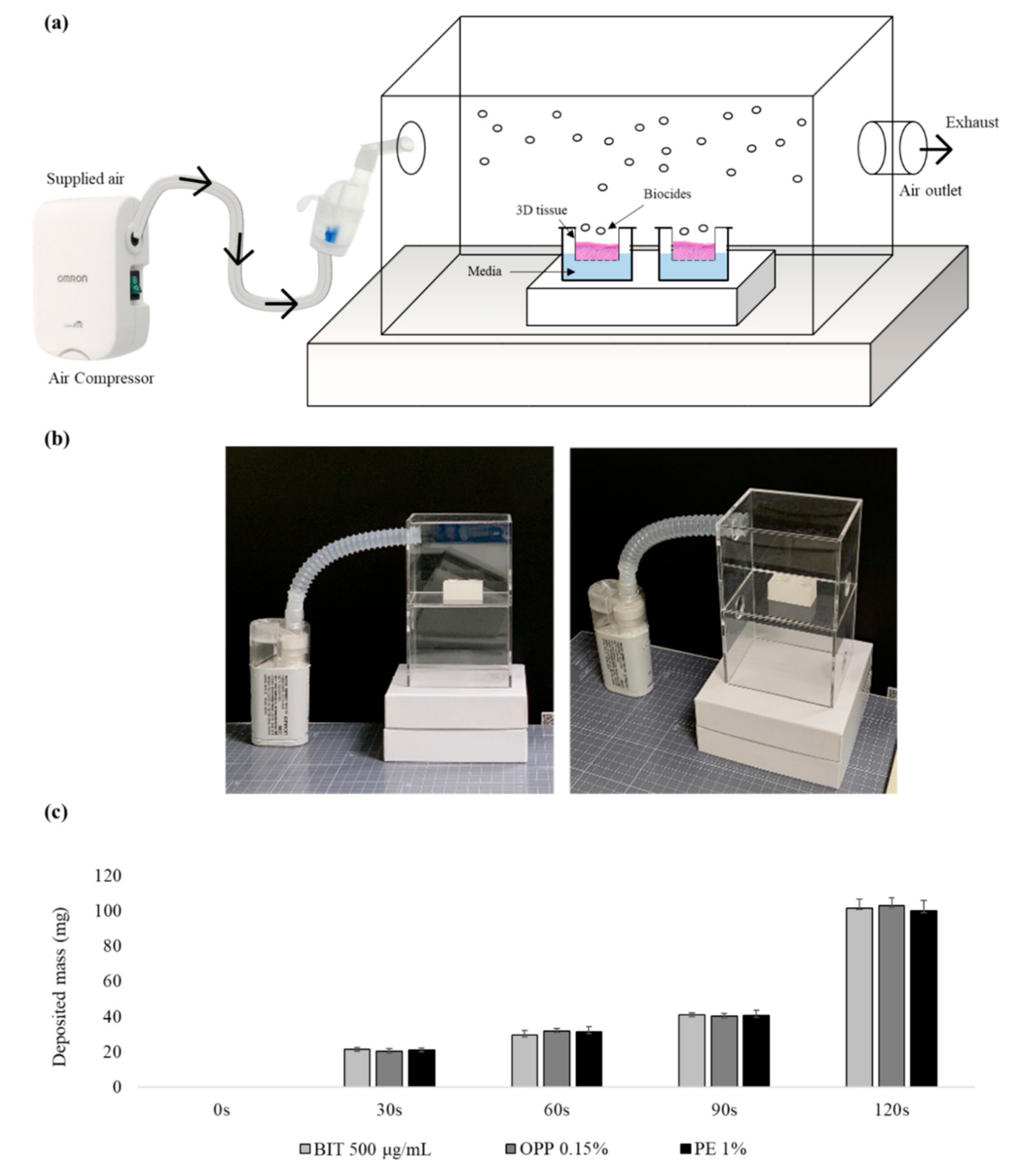
2.4. Aerosol Generation and Application
2.5. Analysis of Biocides in the Aerosol
2.5.1. LC-MS/MS Analysis
2.5.2. GC-MS Analysis
2.5.3. Analytical Validation
2.6. MTT Assay
2.7. Histological Analysis
2.8. Statistical Analysis
3. Results
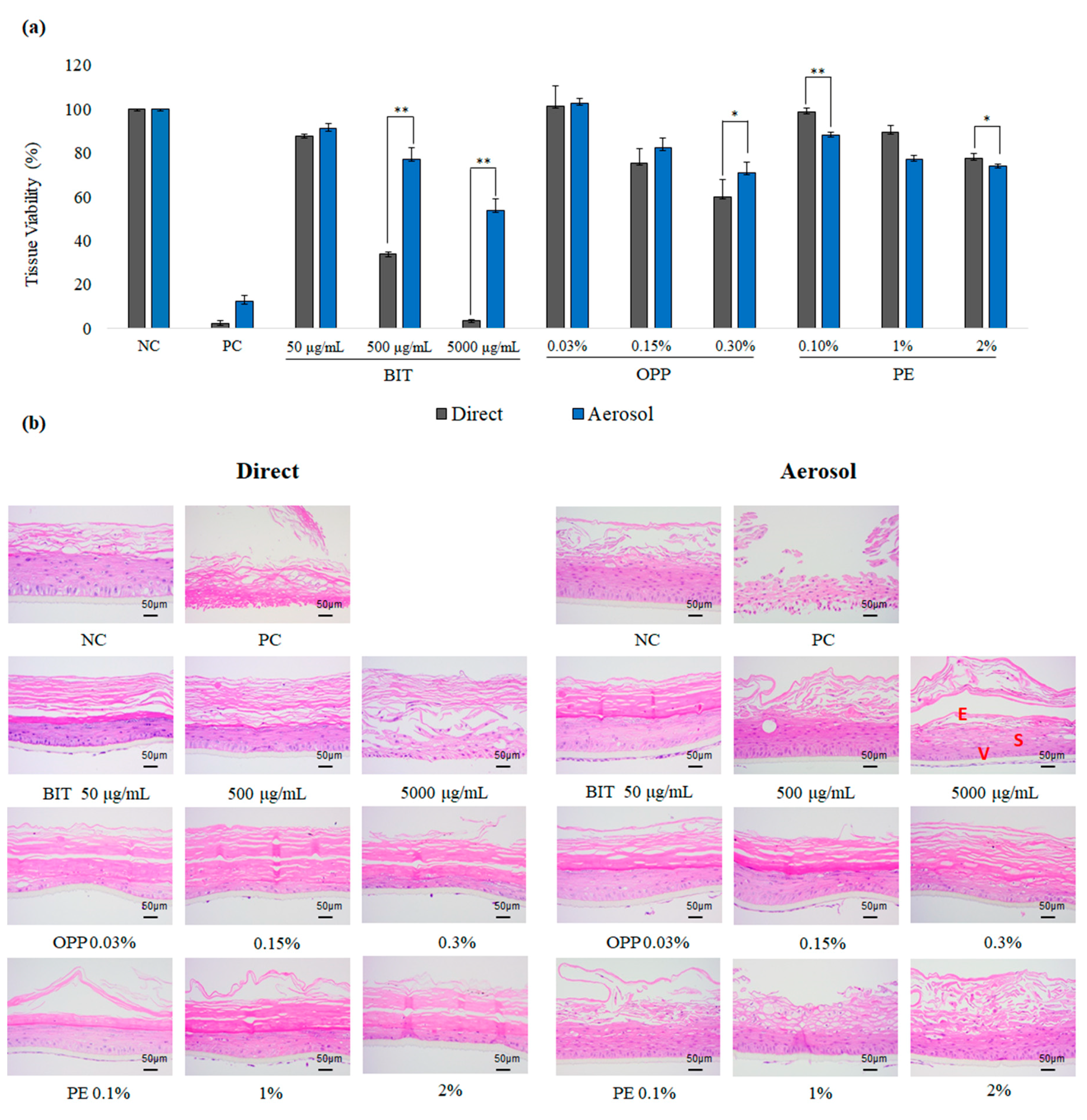
3.1. The Local Toxicity of Biocides after Direct or Aerosol Exposure on the Reconstructed Human Skin Epidermis Model, KeraSkinTM
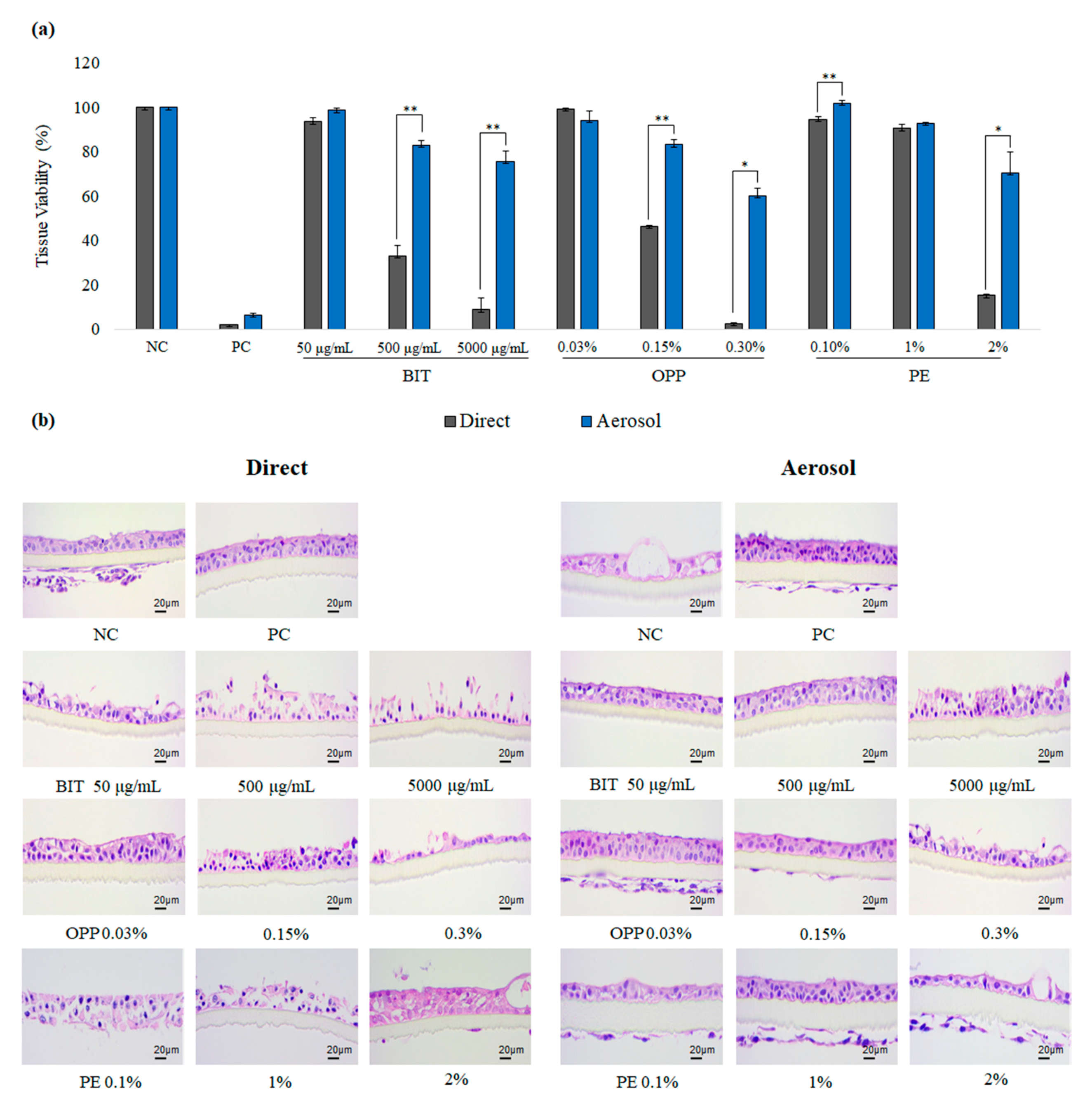
3.2. Comparison of Local Toxicity of Biocides after Direct or Aerosol Exposure on the Reconstructed Human Upper Airway Model, SoluAirwayTM
3.3. Concentrations of Biocides after Aerosolization
3.4. Effects of Aerosol Particle Sizes on the Local Toxicity of Biocides on SoluAirwayTM
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hahn, S.; Schneider, K.; Gartiser, S.; Heger, W.; Mangelsdorf, I. Consumer exposure to biocides-identification of relevant sources and evaluation of possible health effects. Environ. Health 2010, 9, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Kong, X.; Ma, S.; Liu, R.; Li, X.; Gao, S.; Ren, D.; Zheng, Y.; Tang, J. TGFβ/Smad mediated the polyhexamethyleneguanide areosol-induced irreversible pulmonary fibrosis in subchronic inhalation exposure. Inhal. Toxicol. 2020, 32, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Park, D. Review of humidifier lung cases caused by use of humidifier-focusing on probable environmental causal agents. J. Environ. Health Sci. 2013, 39, 105–116. [Google Scholar]
- Kim, H.R.; Lee, K.; Park, C.W.; Song, J.A.; Park, Y.J.; Chung, K.H. Polyhexamethylene guanidine phosphate aerosol particles induce pulmonary inflammatory and fibrotic responses. Arch. Toxicol. 2016, 90, 617–632. [Google Scholar] [CrossRef] [PubMed]
- Berardi, A.; Perinelli, D.R.; Merchant, H.A.; Bisharat, L.; Basheti, I.A.; Bonacucina, G.; Cespi, M.; Palmieri, G.F. Hand sanitisers amid CoViD-19: A critical review of alcohol-based products on the market and formulation approaches to respond to increasing demand. Int. J. Pharm. 2020, 584, 119431. [Google Scholar] [CrossRef] [PubMed]
- Emilie, D.S.; Jorid, B.S. Animal Testing for Acute Inhalation Toxicity: A Thing of the Past? Appl. In Vitro Toxicol. 2018, 4, 89–90. [Google Scholar]
- Kim, Y.S.; Lee, M.J.; Seo, D.S.; Kim, T.H.; Kim, M.H.; Lim, C.H. Thirteen-week inhalation toxicity study of 1-methylnaphthalene in F344 rats. Toxicol. Res. 2020, 36, 13–20. [Google Scholar] [CrossRef]
- Paur, H.-R.; Cassee, F.R.; Teeguarden, J.; Fissan, H.; Diabate, S.; Aufderheide, M.; Kreyling, W.G.; Hänninen, O.; Kasper, G.; Riediker, M. In-vitro cell exposure studies for the assessment of nanoparticle toxicity in the lung—A dialog between aerosol science and biology. J. Aerosol. Sci. 2011, 42, 668–692. [Google Scholar] [CrossRef]
- Movia, D.; Bruni-Favier, S.; Prina-Mello, A. In vitro Alternatives to Acute Inhalation Toxicity Studies in Animal Models—A Perspective. Front. Bioeng. Biotechnol. 2020, 8, 549. [Google Scholar] [CrossRef]
- Mülhopt, S.; Diabaté, S.; Krebs, T.; Weiss, C.; Paur, H. Lung toxicity determination by in vitro exposure at the air liquid interface with an integrated online dose measurement. J. Phys. Conf. Ser. 2009, 2009, 012008. [Google Scholar] [CrossRef] [Green Version]
- Ndika, J.; Ilves, M.; Kooter, I.M.; Gröllers-Mulderij, M.; Duistermaat, E.; Tromp, P.C.; Kuper, F.; Kinaret, P.; Greco, D.; Karisola, P. Mechanistic Similarities between 3D Human Bronchial Epithelium and Mice Lung, Exposed to Copper Oxide Nanoparticles, Support Non-Animal Methods for Hazard Assessment. Small 2020, 16, 2000527. [Google Scholar] [CrossRef] [PubMed]
- WilloughbySr, J.A. Predicting respiratory toxicity using a human 3D airway (EpiAirway™) model combined with multiple parametric analysis. Appl. In Vitro Toxicol. 2015, 1, 55–65. [Google Scholar] [CrossRef]
- Di Cristo, L.; Grimaldi, B.; Catelani, T.; Vázquez, E.; Pompa, P.; Sabella, S. Repeated exposure to aerosolized graphene oxide mediates autophagy inhibition and inflammation in a three-dimensional human airway model. Mater. Today Bio 2020, 6, 100050. [Google Scholar] [CrossRef] [PubMed]
- Tollstadius, B.F.; da Silva, A.C.G.; Pedralli, B.C.O.; Valadares, M.C. Carbendazim induces death in alveolar epithelial cells: A comparison between submerged and at the air-liquid interface cell culture. Toxicol. In Vitro 2019, 58, 78–85. [Google Scholar] [CrossRef]
- Steiner, S.; Majeed, S.; Kratzer, G.; Vuillaume, G.; Hoeng, J.; Frentzel, S. Characterization of the Vitrocell® 24/48 aerosol exposure system for its use in exposures to liquid aerosols. Toxicol. In Vitro 2017, 42, 263–272. [Google Scholar] [CrossRef]
- Talikka, M.; Kostadinova, R.; Xiang, Y.; Mathis, C.; Sewer, A.; Majeed, S.; Martin, F. The response of human nasal and bronchial organotypic tissue cultures to repeated whole cigarette smoke exposure. Int. J. Toxicol. 2014, 33, 506–517. [Google Scholar] [CrossRef]
- Schlage, W.K.; Iskandar, A.R.; Kostadinova, R.; Xiang, Y.; Sewer, A.; Majeed, S.; Kuehn, D.; Frentzel, S.; Talikka, M.; Geertz, M. In vitro systems toxicology approach to investigate the effects of repeated cigarette smoke exposure on human buccal and gingival organotypic epithelial tissue cultures. Toxicol. Mech. Methods 2014, 24, 470–487. [Google Scholar] [CrossRef] [Green Version]
- Sørli, J.B.; Huang, Y.; Da Silva, E.; Hansen, J.S.; Zuo, Y.Y.; Frederiksen, M.; Nørgaard, A.W.; Ebbehøj, N.E.; Larsen, S.T.; Hougaard, K.S. Prediction of acute inhalation toxicity using in vitro lung surfactant inhibition. ALTEX-Altern. Anim. Exp. 2018, 35, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.-M.; Lee, S.-H.; Jang, W.-H.; Jung, H.-S.; Heo, Y.; Park, Y.-H.; Bae, S.; Lim, K.-M.; Seok, S.H. KeraSkin™-VM: A novel reconstructed human epidermis model for skin irritation tests. Toxicol. In Vitro 2014, 28, 742–750. [Google Scholar] [CrossRef]
- OECD. Test No. 439: In Vitro Skin Irritation: Reconstructed Human Epidermis Test Method; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Jackson Jr, G.R.; Maione, A.G.; Klausner, M.; Hayden, P.J. Prevalidation of an acute inhalation toxicity test using the epiairway In Vitro human airway model. Appl. In Vitro Toxicol. 2018, 4, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Heo, J.J.; Kim, U.-J.; Oh, J.-E. Simultaneous quantitative analysis of four isothiazolinones and 3-iodo-2-propynyl butyl carbamate in hygienic consumer products. Environ. Eng. Res. 2019, 24, 137–143. [Google Scholar] [CrossRef]
- Varga, Z.; Nicol, E.; Bouchonnet, S. Photodegradation of benzisothiazolinone: Identification and biological activity of degradation products. Chemosphere 2020, 240, 124862. [Google Scholar] [CrossRef] [PubMed]
- Scheuch, G.; Stahlhofen, W. Deposition and dispersion of aerosols in the airways of the human respiratory tract: The effect of particle size. Exp. Lung Res. 1992, 18, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Rothen-Rutishauser, B.; Blank, F.; Mühlfeld, C.; Gehr, P. In vitro models of the human epithelial airway barrier to study the toxic potential of particulate matter. Expert Opin. Drug Metab. Toxicol. 2008, 4, 1075–1089. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y.; Izumi, H.; Yoshiura, Y.; Fujishima, K.; Yatera, K.; Yamamoto, K. Usefulness of Intratracheal Instillation Studies for Estimating Nanoparticle-Induced Pulmonary Toxicity. Int. J. Mol. Sci. 2016, 17, 165. [Google Scholar] [CrossRef] [Green Version]
- Brain, J.D.; Knudson, D.E.; Sorokin, S.P.; Davis, M.A. Pulmonary distribution of particles given by intratracheal instillation or by aerosol inhalation. Environ. Res. 1976, 11, 13–33. [Google Scholar] [CrossRef]
- Driscoll, K.E.; Costa, D.L.; Hatch, G.; Henderson, R.; Oberdorster, G.; Salem, H.; Schlesinger, R.B. Intratracheal instillation as an exposure technique for the evaluation of respiratory tract toxicity: Uses and limitations. Toxicol. Sci. 2000, 55, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Osier, M.; Oberörster, G. Intratracheal inhalation vs intratracheal instillation: Differences in particle effects. Toxicol. Sci. 1997, 40, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Henderson, R.; Driscoll, K.; Harkema, J.; Lindenschmidt, R.; Chang, I.-Y.; Maples, K.; Barr, E. A comparison of the inflammatory response of the lung to inhaled versus instilled particles in F344 rats. Fundam. Appl. Toxicol. 1995, 24, 183–197. [Google Scholar] [CrossRef]
- Balogh Sivars, K.; Sivars, U.; Hornberg, E.; Zhang, H.; Brändén, L.; Bonfante, R.; Huang, S.; Constant, S.; Robinson, I.; Betts, C.J. A 3D human airway model enables prediction of respiratory toxicity of inhaled drugs in vitro. Toxicol. Sci. 2018, 162, 301–308. [Google Scholar] [CrossRef]
- Corley, R.A.; Kabilan, S.; Kuprat, A.P.; Carson, J.P.; Minard, K.R.; Jacob, R.E.; Timchalk, C.; Glenny, R.; Pipavath, S.; Cox, T. Comparative computational modeling of airflows and vapor dosimetry in the respiratory tracts of rat, monkey, and human. Toxicol. Sci. 2012, 128, 500–516. [Google Scholar] [CrossRef] [Green Version]
- Corley, R.A.; Suffield, S.R.; Kabilan, S.; Kuprat, A.P. Chlorothalonil: Computational Modeling of Aerosol Dosimetry in the Respiratory Tracts of the Rat and Human; TK0253671; Syngenta Crop protection LLC: Greensboro, NC, USA, 2018; p. 40. [Google Scholar]
- U.S. Environmental Protection Agency. Integrated Science Assessment (ISA) for Particulate Matter; U.S. Environmental Protection Agency: Washington, DC, USA, 2009.
- Cassee, F.R.; Muijser, H.; Duistermaat, E.; Freijer, J.J.; Geerse, K.B.; Marijnissen, J.C.; Arts, J.H. Particle size-dependent total mass deposition in lungs determines inhalation toxicity of cadmium chloride aerosols in rats. Application of a multiple path dosimetry model. Arch. Toxicol. 2002, 76, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M.; Albert, R.E. The effect of particle size on the regional deposition of inhaled aerosols in the human respiratory tract. Am. Ind. Hyg. Assoc. J. 1969, 30, 257–275. [Google Scholar] [CrossRef] [PubMed]
- Novick, R.M.; Nelson, M.L.; Unice, K.M.; Keenan, J.J.; Paustenbach, D.J. Estimation of the safe use concentrations of the preservative 1, 2-benzisothiazolin-3-one (BIT) in consumer cleaning products and sunscreens. Food Chem. Toxicol. 2013, 56, 60–66. [Google Scholar] [CrossRef] [PubMed]
- EUROPEAN_COMMISSION. Regulation (EU) No 528/2012 of the European Parliament and of the Council of 22 May 2012 Concerning the Making Available on the Market and Use of Biocidal Products. 2012. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2012:167:0001:0123:EN:PDF (accessed on 8 January 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chemical | International Union of Pure and Applied Chemistry (IUPAC) Name | Maximum Permitted Concentration |
|---|---|---|
| BIT | 1,2-Benzothiazol-3-one | 0.05% in EU and USA |
| PE | 2-Phenoxyethanol | Cosmetics, 1% |
| OPP | 2-Phenylphenol | Cosmetics, 0.15% (as phenol) |
| Biocides | Indicated Conc. | After Nebulization | |
|---|---|---|---|
| 5 μm | 3 μm | ||
| BIT (1,2-Benzisothiazol- 3(2H)-one) | 50 μg/mL | 37.34 ± 19.85 | 44.70 ± 6.00 |
| 500 μg/mL | 394.39 ± 47.71 | 457.8 ± 86.73 | |
| 5000 μg/mL | 1144.11 ± 134.31 | 857.0 ± 69.18 | |
| OPP (2-phenylphenol) | 0.03% | 0.006 ± 0.004 | 0.021 ± 0.017 |
| 0.15% | 0.027 ± 0.01 | 0.103 ± 0.013 | |
| 0.3% | 0.048 ± 0.019 | 0.099 ± 0.009 | |
| PE (2-phenoxyethanol) | 0.1% | 0.04 ± 0.002 | 0.028 ± 0.012 |
| 1% | 0.49 ± 0.059 | 0.251 ± 0.099 | |
| 2% | 1.21 ± 0.259 | 0.523 ± 0.172 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Jang, D.Y.; Lee, D.H.; Jeong, H.; Nam, K.T.; Choi, D.-W.; Lim, K.-M. Local Toxicity of Biocides after Direct and Aerosol Exposure on the Human Skin Epidermis and Airway Tissue Models. Toxics 2021, 9, 29. https://doi.org/10.3390/toxics9020029
Lee N, Jang DY, Lee DH, Jeong H, Nam KT, Choi D-W, Lim K-M. Local Toxicity of Biocides after Direct and Aerosol Exposure on the Human Skin Epidermis and Airway Tissue Models. Toxics. 2021; 9(2):29. https://doi.org/10.3390/toxics9020029
Chicago/Turabian StyleLee, Nahyun, Dae Yong Jang, Do Hyeon Lee, Haengdueng Jeong, Ki Taek Nam, Dal-Woong Choi, and Kyung-Min Lim. 2021. "Local Toxicity of Biocides after Direct and Aerosol Exposure on the Human Skin Epidermis and Airway Tissue Models" Toxics 9, no. 2: 29. https://doi.org/10.3390/toxics9020029
APA StyleLee, N., Jang, D. Y., Lee, D. H., Jeong, H., Nam, K. T., Choi, D. -W., & Lim, K. -M. (2021). Local Toxicity of Biocides after Direct and Aerosol Exposure on the Human Skin Epidermis and Airway Tissue Models. Toxics, 9(2), 29. https://doi.org/10.3390/toxics9020029