
Right Place, Right Time: Preferences of Women with Ovarian Cancer for Delivery of CAM Education

Abstract
:1. Introduction
2. Material and Methods
2.1. Sample
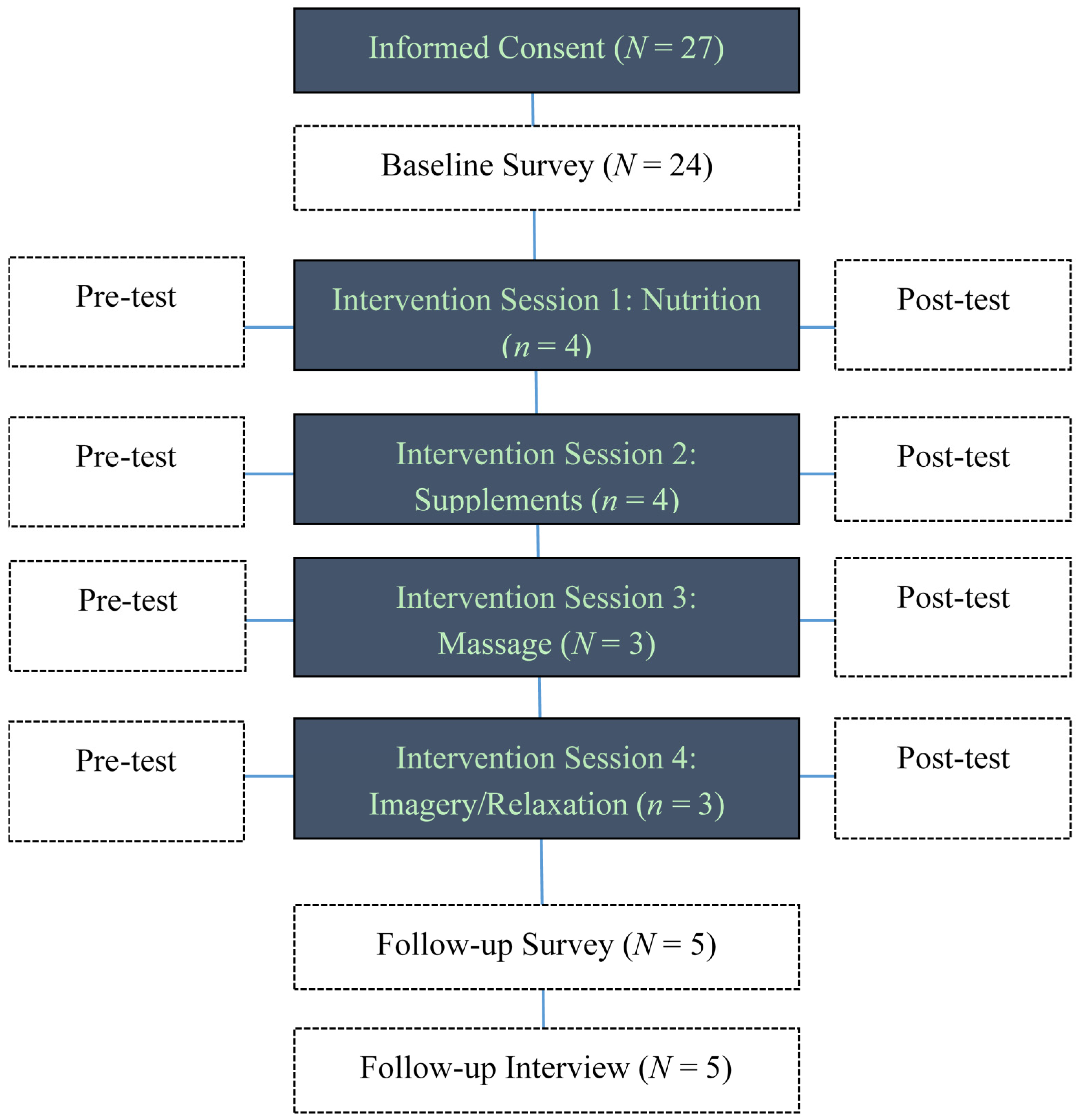
2.2. Intervention Design

{kind=link}
{kind=link}
| Topic | Presenter | Learning Objectives |
|---|---|---|
| Nutrition and Cancer: Separating Facts from Fiction | Registered Dietitian |
|
| Herbal Supplements and Their Impact on Cancer | PharmD expert on the impact of herbal supplements on cancer |
|
| The Benefits of Massage and Healing Touch | Licensed Massage Therapist |
|
| Guided Imagery and Relaxation Training | Integrative Medicine Program Leader |
|


2.3. Instruments and Measures
2.4. Data Analysis and Statistical Considerations
- Attendance and completion rates of ≥70% would have been seen as a positive indicator.
- A positive change in direction between pre- and post-test knowledge scores would have been interpreted as a positive indicator.
- Satisfaction scores would have been interpreted as follows: 0–2 = low, not worthy of pursuing; 2.1–3 = moderate, inconclusive and needs supportive qualitative data; 3.1–4 = high, worth pursuing on a larger scale.
3. Results
| Age, mean (std) | 61.0 (8.7) |
| Race | N (%) |
| White | 22 (91.7%) |
| Asian | 1 (4.2%) |
| Black | 1 (4.2%) |
| Employment status | N (%) |
| Full-time | 4 (16.7%) |
| Part-time | 3 (12.5%) |
| Unemployed | 1 (4.2%) |
| Retired | 13 (54.2%) |
| Disabled | 3 (12.5%) |
| Residential Classification | N (%) |
| Urban | 3 (12.5%) |
| Suburban | 17 (70.8%) |
| Small Town | 4 (16.7%) |
| Income Level | N (%) |
| Under 25,000 | 1 (4.2%) |
| 25,000–50,000 | 6 (25.0%) |
| 50,000–75,000 | 6 (25.0%) |
| 75,000–100,000 | 7 (29.2%) |
| Over 100,000 | 2 (8.3%) |
| Missing | 2 (8.3%) |
| Stage | N (%) |
| IIB | 1 (4.2%) |
| IIC | 1 (4.2%) |
| III | 1 (4.2%) |
| IIIC | 14 (58.3%) |
| III/IV | 1 (4.2%) |
| IV | 6 (25.0%) |
| Months from diagnosis at consent, mean (std) | 34.4 (23.9) |
| Active Treatment at Consent, N (%) | 16 (66.7%) |
| Number of Prior Treatments at Consent, mean (std) | 2.0 (1.2) |
| Attended Intervention Sessions, N (%) | 5 (20.8%) |
3.1. Topic and Time Preferences
3.2. Intervention Sessions
3.3. UCATS, FACT-O, and SMAS
3.4. Follow-Up Telephone Interviews
- “Nutrition and meditation, which helped when resuming chemotherapy.”
- “Meditation and imagery were helpful when faced with newly diagnosed breast cancer during the program.”
- “More attendees would have stimulated more discussion.”
- “It was held in a less-than-ideal location, an open atrium with periodic passersby.”
- “It helped just being with other women in a similar situation.”
- “The program validated that I was doing beneficial things for myself.”
- “Although it required traveling 40 min to attend, it was worth the travel time.”
4. Discussion
Implications for Practice
5. Conclusions
Acknowledgments
Author contribution
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures 2013; American Cancer Society: Atlanta, GA, USA, 2013. [Google Scholar]
- American Cancer Society. What Are the Key Statistics about Ovarian Cancer? 2014. Available online: http://www.cancer.org/cancer/ovariancancer/detailedguide/ovarian-cancer-key-statistics (accessed on 12 August 2014).
- Lockwood-Rayermann, S. Survivorship Issues in Ovarian Cancer: A Review. Oncol. Nurs. Forum 2006, 33, 553–562. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts and Figures 2006. Available online: http://www.cancer.org/ownloads/STT/CAFF2006PWSecured.pdf (accessed on 14 February 2007).
- Morgan, R.J., Jr.; Alvarez, R.D.; Armstrong, D.K.; Burger, R.A.; Chen, L.M.; Copeland, L.; Crispens, M.A.; Gershenson, D.M.; Gray, H.J.; Hakam, A.; et al. Ovarian Cancer, Version 2.2013. J. Natl. Compr. Cancer Netw. 2013, 11, 1199–1209. [Google Scholar]
- Taylor, K.; Shelby, R.; Gelmann, E.; McGuire, C. Quality of Life and Trial Adherence Among Participants in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. J. Natl. Cancer Inst. 2004, 96, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.C.; Ramirez, P.T.; Bodurka, D.C. Quality of Life for Patients with Epithelial Ovarian Cancer. Nat. Clin. Pract. Oncol. 2007, 4, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Zabora, J.; BrintzenhofeXzoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The Prevalence of Psychological Distress by Cancer Site. Psycho-Oncol. 2001, 10, 19–28. [Google Scholar] [CrossRef]
- McKenzie, H.; Crouch, M. Discordant Feelings in the Lifeworld of Cancer Survivors. Health 2004, 8, 139–157. [Google Scholar] [CrossRef] [PubMed]
- Mahon, S.; Casperson, D. Exploring the Psychosocial Meaning of Recurrent Cancer: A Descriptive Study. Cancer Nurs. 1997, 20, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Howell, D.; Fitch, M.; Deane, K. Impact of Ovarian Cancer Perceived by Women. Cancer Nurs. 2003, 26, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bodurka-Bevers, D.; Basen-Engquist, K.; Carmack, C.L.; Fitzgerald, M.A.; Wolf, J.K.; de Moor, C.; Gershenson, D.M. Depression, Anxiety, and Quality of Life in Patients with Epithelial Ovarian Cancer. Gynecol. Oncol. 2000, 78 Pt 1, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Cain, E.; Kohorn, E.I.; Quinlan, D.M.; Schwartz, P.E.; Latimer, K.; Rogers, L. Psychosocial Reactions to the Diagnosis of Gynecologic Cancer. Obstet. Gynecol. 1983, 62, 635–641. [Google Scholar] [PubMed]
- Ersek, M.; Ferrell, B.R.; Dow, K.H.; Melancon, C.H. Quality of Life in Women with Ovarian Cancer. West. J. Nurs. Res. 1997, 19, 334–350. [Google Scholar] [CrossRef] [PubMed]
- Kornblith, A.; Thaler, H.T.; Wong, G.; Vlamis, V.; Lepore, J.M.; Loseth, D.B.; Hakes, T.; Hoskins, W.J.; Portenoy, R.K. Quality of Life in Women with Ovarian Cancer. Gynecol. Oncol. 1995, 59, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Steginga, S.; Dunn, J. Women’s Experiences Following Treatment for Gynecologic Cancer. Oncol. Nurs. Forum 1997, 24, 1403–1408. [Google Scholar] [PubMed]
- Bachmann, G. Psychosexual Aspects of Hysterectomy. Women’s Health Issues 1990, 1, 41–49. [Google Scholar] [CrossRef]
- Guidozzi, F. Living with Ovarian Cancer. Gynecol. Oncol. 1993, 50, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, K.M.; Ladd, E.C.; Lammers, S.E.; Echenberg, R.J. In Your Skin You Are Different: Women Living with Ovarian Cancer During Childbearing Years. Qual. Health Res. 1999, 9, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Donovan, K.; Greene, P.G.; Shuster, J.L.; Partridge, E.E.; Tucker, D.C. Treatment Preferences in Recurrent Ovarian Cancer. Gynecol. Oncol. 2002, 86, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Pilkington, F.; Mitchell, G. Quality of Life for Women Living with a Gynecologic Cancer. Nurs. Sci. Q. 2004, 17, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.; Thaler, H.T.; Kornblith, A.B.; Lepore, J.M.; Friedlander-Klar, H.; Coyle, N.; Smart-Curley, T.; Kemeny, N.; Norton, L.; Hoskins, W.; et al. Symptom Prevalence, Characteristics and Distress in a Cancer Population. Qual. Life Res. 1994, 3, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Cassileth, B. Integrative oncology: Complementary Therapies for Pain, Anxiety, and Mood Disturbance. Complement. Altern. Methods 2005, 55, 109–116. [Google Scholar] [CrossRef]
- Lengacher, C.; Bennett, M.P.; Kip, K.E.; Gonzalez, L.; Jacobsen, P.; Cox, C.E. Relief of symptoms/side effects/psychological distress through use of CAM in women with breast cancer. Nurs. Oncol. Forum 2006, 33, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Lengacher, C.; Bennett, M.P.; Kip, K.E.; Keller, R.; LaVance, M.S.; Smith, L.S.; Cox, C.E. Frequency of use of complementary and alternative medicine in women with breast cancer. Oncol. Nurs. Forum 2002, 29, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Lekander, M.; Furst, C.J.; Rotstein, S.; Hursti, T.J.; Fredrikson, M. Immune Effects of Relaxation During Chemotherapy for Ovarian Cancer. Psychother. Psychosom. 1997, 66, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Muecke, R.; Schomburg, L.; Glatzel, M.; Berndt-Skorka, R.; Baaske, D.; Reichl, B.; Buentzel, J.; Kundt, G.; Prott, F.J.; Devries, A.; et al. Multicenter, phase 3 trial comparing selenium supplementation with observation in gynecologic radiation oncology. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Muecke, R.; Micke, O.; Schomburg, L.; Glatzel, M.; Reichl, B.; Kisters, K.; Schaefer, U.; Huebner, J.; Eich, H.T.; Fakhrian, K.; et al. Multicenter, phase III trial comparing selenium supplementation with observation in gynecologic radiation oncology: Follow-up analysis of the survival data 6 years after cessation of randomization. Integr. Cancer Ther. 2014, 13, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Sieja, K.; Talerczyk, M. Selenium as an Element in the Treatment of Ovarian Cancer in Women Receiving Chemotherapy. Gynecol. Oncol. 2004, 93, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Drisko, J.; Chapman, J.; Hunter, V. The Use of Antioxidants with First-Line Chemotherapy in Two Cases of Ovarian Cancer. J. Am. Coll. Nutr. 2003, 22, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Pace, A.; Savarese, A.; Picardo, M.; Maresca, V.; Pacetti, U.; Del Monte, G.; Biroccio, A.; Leonetti, C.; Jandolo, B.; Cognetti, F.; et al. Neuroprotective Effect of Vitamin E Supplementation in Patients Treated with Cisplatin Chemotherapy. J. Clin. Oncol. 2003, 21, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Gedlicka, C.; Kornek, G.V.; Schmid, K.; Scheithauer, W. Amelioration of Docetaxel/Cisplatin Induced Polyneuropathy by Alpha-Lipoic Acid. Ann. Oncol. 2003, 14, 339–340. [Google Scholar] [CrossRef] [PubMed]
- Vahdat, L.; Papadopoulos, K.; Lange, D.; Leuin, S.; Kaufman, E.; Donovan, D.; Frederick, D.; Baqiella, E.; Tiersten, A.; Nichols, G.; et al. Reduction of Paclitaxel-Induced Peripheral Neuropathy with Glutamine. Clin. Cancer Res. 2001, 2001, 1192–1197. [Google Scholar]
- Marwick, C. Complementary, Alternative Therapies Should Race Rigorous Testing, IOM Concludes. J. Natl. Cancer Inst. 2005, 97, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Lengacher, C.; Bennett, M.P.; Kipp, K.E.; Berarducci, A.; Cox, C.E. Design and testing of the use of a complementary and alternative therapies survey in women with breast cancer. Oncol. Nurs. Forum 2003, 30, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Basen-Engquist, K.; Bodurka-Bevers, D.; Fitzgerald, M.A.; Webster, K.; Cella, D.; Hu, S.; Gershenson, D.M. Reliability and validity of the Functional Assessment of Cancer Therapy—Ovarian. J. Clin. Oncol. 2001, 19, 1809–1817. [Google Scholar] [PubMed]
- Canada, A.; Parker, P.A.; Basen-Engquist, K.; de Moor, J.S.; Ramondetta, L.M.; Cohen, L. Active coping mediates the association between religion/spirituality and quality of life in ovarian cancer. Gynecol. Oncol. 2006, 101, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.; Thaler, H.T.; Kornblith, A.B.; Lepore, J.M.; Friedlander-Klar, H.; Kiyasu, E.; Sobel, K.; Coyle, N.; Kemeny, N.; Norton, L.; et al. The Memorial Symptom Assessment Scale: An instrument for the evaluation of symptom prevalence, characteristics and distress. Eur. J. Cancer 2000, 30, 1326–1336. [Google Scholar] [CrossRef]
- Chandwani, K.D.; Ryan, J.L.; Peppone, L.J.; Janelsins, M.M.; Sprod, L.K.; Devine, K.; Trevino, L.; Gewandter, J.; Morrow, G.R.; Mustain, K.M. Cancer-Related Stress and Complementary and Alternative Medicine: A Review. Evid.-Based Complement. Altern. Med. 2012, 2012, 15. [Google Scholar] [CrossRef] [PubMed]
- Lengacher, C.A.; Shelton, M.M.; Reich, R.R.; Barta, M.K.; Johnson-Mallard, V.; Moscoso, M.S.; Paterson, C.; Ramesar, S.; Budhrani, P.; Carranza, I.; et al. Mindfulness based stress reduction (MBSR(BC)) in breast cancer: Evaluating fear of recurrence (FOR) as a mediator of psychological and physical symptoms in a randomized control trial (RCT). J. Behav. Med. 2014, 37, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Von Gruenigen, V.E.; Huang, H.Q.; Gil, K.M.; Gibbons, H.E.; Mong, B.J.; Rose, P.G.; Armstrong, D.K.; Cella, D.; Wenzel, L. A comparison of quality-of-life domains and clinical factors in ovarian cancer patients: A Gynecologic Oncology Group study. J. Pain Symptom Manag. 2010, 39, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Center for Women’s Oncology; Moffitt Cancer Center. Teletalk Tracking Records, 2012–2013.
- O’Carroll Bantum, E.; Albright, C.L.; White, K.K.; Berenberg, J.L.; Layi, G.; Ritter, P.L.; Sarent, D.; Plant, K.; Lorig, K. Surviving and thriving with cancer using a Web-based health behavior change intervention: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e54. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebbert, J.A.; Donovan, K.A.; Lengacher, C.A.; Fabri, D.; Reich, R.; Daley, E.; Thompson, E.L.; Wenham, R.M. Right Place, Right Time: Preferences of Women with Ovarian Cancer for Delivery of CAM Education. Medicines 2015, 2, 236-250. https://doi.org/10.3390/medicines2030236
Ebbert JA, Donovan KA, Lengacher CA, Fabri D, Reich R, Daley E, Thompson EL, Wenham RM. Right Place, Right Time: Preferences of Women with Ovarian Cancer for Delivery of CAM Education. Medicines. 2015; 2(3):236-250. https://doi.org/10.3390/medicines2030236
Chicago/Turabian StyleEbbert, Judith Ann, Kristine A. Donovan, Cecile A. Lengacher, Donna Fabri, Richard Reich, Ellen Daley, Erika Lynne Thompson, and Robert M. Wenham. 2015. "Right Place, Right Time: Preferences of Women with Ovarian Cancer for Delivery of CAM Education" Medicines 2, no. 3: 236-250. https://doi.org/10.3390/medicines2030236
APA StyleEbbert, J. A., Donovan, K. A., Lengacher, C. A., Fabri, D., Reich, R., Daley, E., Thompson, E. L., & Wenham, R. M. (2015). Right Place, Right Time: Preferences of Women with Ovarian Cancer for Delivery of CAM Education. Medicines, 2(3), 236-250. https://doi.org/10.3390/medicines2030236