Figure 1.
Schematics and actual photographs showing the regions of interest in the dorsal arm, ventral arm, lateral arm, medial arm, dorsal hand, and ventral hand of the upper limbs. The red dots represent each region of interest, and the related numbers are the serial numbers assigned to each regions of interest.
Figure 1.
Schematics and actual photographs showing the regions of interest in the dorsal arm, ventral arm, lateral arm, medial arm, dorsal hand, and ventral hand of the upper limbs. The red dots represent each region of interest, and the related numbers are the serial numbers assigned to each regions of interest.
Figure 2.
Comparison of the average temperatures of each ROI in the six regions. ROI: region of interest; and ⸰ indicates a label out of range.
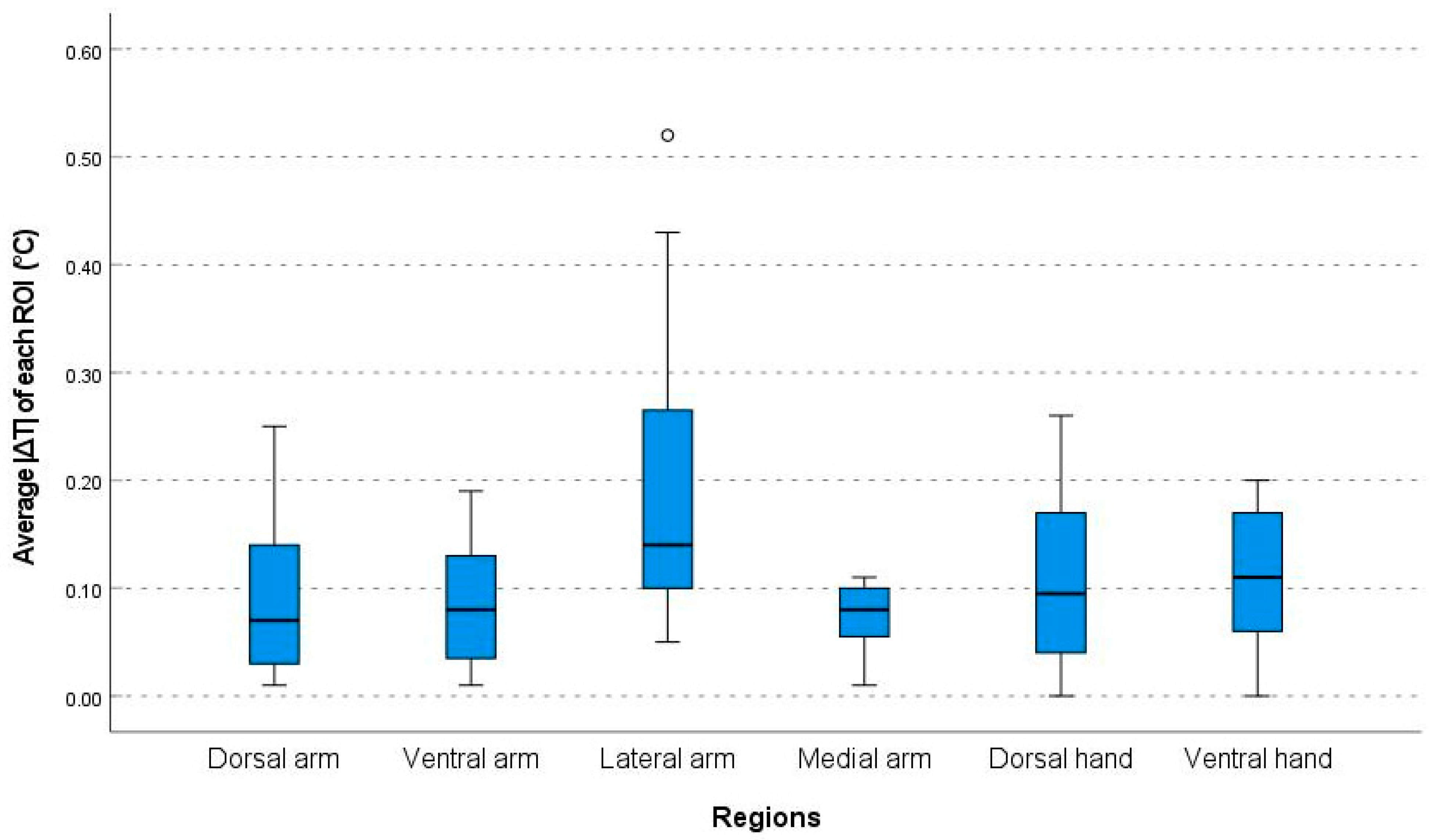
Figure 3.
Comparison of the absolute value of the temperature discrepancies between the right and left side (|ΔT|) of each ROI in the six regions. ROI: region of interests; and ⸰ indicates a label out of range.
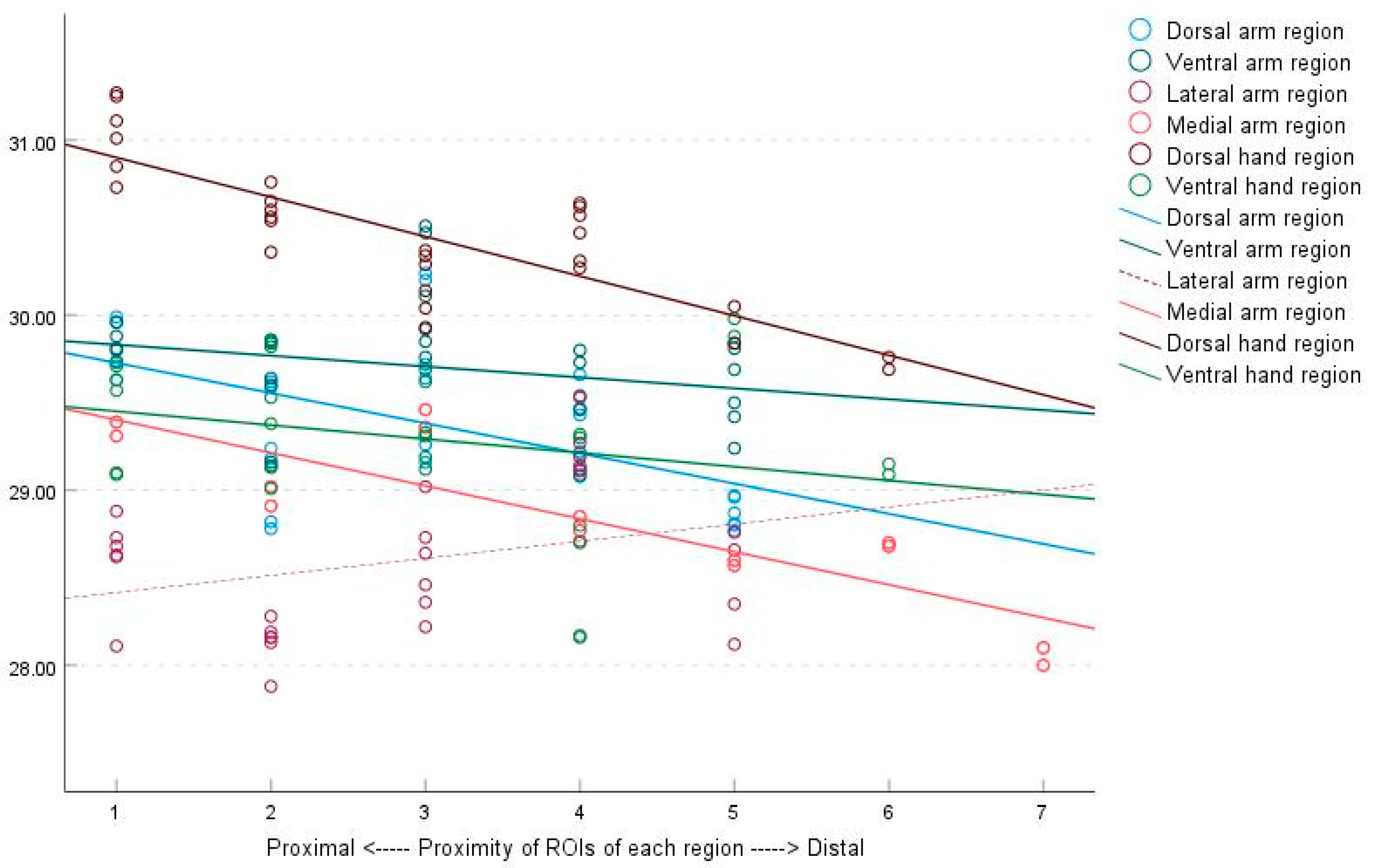
Figure 4.
Correlation between the average temperatures of each ROI and the proximity of ROIs to the body core of the six regions, as determined by linear regression analysis. The trend observed in the figure demonstrates a gradual decrease in surface temperature from proximal to distal for each ROI, except for the lateral arm region. ROIs, regions of interest.
Figure 4.
Correlation between the average temperatures of each ROI and the proximity of ROIs to the body core of the six regions, as determined by linear regression analysis. The trend observed in the figure demonstrates a gradual decrease in surface temperature from proximal to distal for each ROI, except for the lateral arm region. ROIs, regions of interest.
Figure 5.
Correlation between right to left temperature discrepancies and the proximity of ROIs to the body core of the six regions, as determined by linear regression analysis. No perceptible correlation was observed between the absolute temperature difference (|ΔT|) and the proximity of each ROI. ROIs, regions of interest.
Figure 5.
Correlation between right to left temperature discrepancies and the proximity of ROIs to the body core of the six regions, as determined by linear regression analysis. No perceptible correlation was observed between the absolute temperature difference (|ΔT|) and the proximity of each ROI. ROIs, regions of interest.
Figure 6.
The average regional temperatures in men and women.
Figure 7.
Relationship between the average regional temperatures and subject age.
Table 1.
The average temperature of each region of interest in the dorsal arm region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 29.63 | 5.88 | 11.78 | 0.00 | | | | |
| 1_2 | 29.74 | 5.93 | 11.88 | −0.10 | 0.55 | −0.22 | 0.01 | 1.35 |
| 2_1 | 29.96 | 5.93 | 11.88 | 0.00 | | | | |
| 2_2 | 29.99 | 5.97 | 11.96 | −0.03 | 0.54 | −0.14 | 0.08 | 1.33 |
| 3_1 | 28.78 | 5.76 | 11.54 | 0.00 | | | | |
| 3_2 | 28.82 | 5.77 | 11.56 | −0.04 | 0.52 | −0.15 | 0.06 | 1.30 |
| 4_1 | 29.18 | 5.80 | 11.62 | 0.00 | | | | |
| 4_2 | 29.24 | 5.80 | 11.63 | −0.06 | 0.49 | −0.16 | 0.04 | 1.24 |
| 5_1 | 29.59 | 5.81 | 11.63 | 0.00 | | | | |
| 5_2 | 29.62 | 5.82 | 11.67 | −0.02 | 0.45 | −0.12 | 0.07 | 1.17 |
| 6_1 | 29.26 | 5.81 | 11.64 | 0.00 | | | | |
| 6_2 | 29.16 | 5.80 | 11.62 | 0.10 | 0.51 | 0.00 | 0.21 | 1.26 |
| 7_1 | 29.64 | 5.87 | 11.76 | 0.00 | | | | |
| 7_2 | 29.72 | 5.94 | 11.90 | −0.08 | 0.64 | −0.21 | 0.06 | 1.48 |
| 8_1 | 30.24 | 5.90 | 11.82 | 0.00 | | | | |
| 8_2 | 30.20 | 5.86 | 11.74 | 0.04 | 0.65 | −0.09 | 0.17 | 1.49 |
| 9_1 | 29.66 | 5.86 | 11.74 | 0.00 | | | | |
| 9_2 | 29.43 | 5.82 | 11.66 | 0.23 | 0.50 | 0.12 | 0.33 | 1.26 |
| 10_1 | 29.47 | 5.81 | 11.65 | 0.00 | | | | |
| 10_2 | 29.21 | 5.77 | 11.56 | 0.25 | 0.48 | 0.15 | 0.35 | 1.22 |
| 11_1 | 29.22 | 5.73 | 11.48 | 0.00 | | | | |
| 11_2 | 29.09 | 5.71 | 11.45 | 0.14 | 0.41 | 0.05 | 0.22 | 1.10 |
| 12_1 | 28.87 | 5.61 | 11.25 | 0.00 | | | | |
| 12_2 | 28.77 | 5.61 | 11.24 | 0.11 | 0.52 | 0.00 | 0.21 | 1.28 |
| 13_1 | 28.97 | 5.62 | 11.26 | 0.00 | | | | |
| 13_2 | 28.80 | 5.61 | 11.23 | 0.17 | 0.43 | 0.08 | 0.26 | 1.14 |
| 14_1 | 28.96 | 5.58 | 11.19 | 0.00 | | | | |
| 14_2 | 28.81 | 5.56 | 11.14 | 0.15 | 0.43 | 0.06 | 0.23 | 1.13 |
| 15_1 | 28.56 | 5.42 | 10.87 | 0.00 | | | | |
| 15_2 | 28.59 | 5.43 | 10.89 | −0.03 | 0.42 | −0.11 | 0.06 | 1.12 |
| 16_1 | 28.75 | 5.44 | 10.90 | 0.00 | | | | |
| 16_2 | 28.69 | 5.43 | 10.89 | 0.06 | 0.44 | −0.03 | 0.15 | 1.14 |
| 17_1 | 28.85 | 5.44 | 10.90 | 0.00 | | | | |
| 17_2 | 28.72 | 5.43 | 10.89 | 0.13 | 0.44 | 0.03 | 0.22 | 1.15 |
| 18_1 | 28.88 | 5.49 | 11.01 | 0.00 | | | | |
| 18_2 | 28.90 | 5.51 | 11.05 | −0.01 | 0.47 | −0.11 | 0.08 | 1.20 |
| Mean | 29.22 | 5.71 | 11.44 | 0.06 | 0.49 | −0.05 | 0.16 | 1.24 |
Table 2.
The average temperature of each region of interest in the ventral arm region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 29.81 | 5.90 | 11.82 | | | | | |
| 1_2 | 29.80 | 5.91 | 11.83 | 0.01 | 0.43 | −0.08 | 0.10 | 1.13 |
| 2_1 | 29.88 | 5.91 | 11.84 | | | | | |
| 2_2 | 29.96 | 5.94 | 11.90 | −0.08 | 0.44 | −0.17 | 0.01 | 1.14 |
| 3_1 | 29.14 | 5.74 | 11.51 | | | | | |
| 3_2 | 29.16 | 5.73 | 11.48 | −0.03 | 0.49 | −0.13 | 0.07 | 1.23 |
| 4_1 | 29.60 | 5.77 | 11.57 | | | | | |
| 4_2 | 29.64 | 5.80 | 11.62 | −0.04 | 0.46 | −0.13 | 0.06 | 1.18 |
| 5_1 | 29.84 | 5.84 | 11.69 | | | | | |
| 5_2 | 29.86 | 5.88 | 11.78 | −0.01 | 0.49 | −0.11 | 0.09 | 1.24 |
| 6_1 | 29.76 | 5.83 | 11.67 | | | | | |
| 6_2 | 29.85 | 5.87 | 11.75 | −0.08 | 0.54 | −0.19 | 0.03 | 1.31 |
| 7_1 | 30.51 | 6.00 | 12.03 | | | | | |
| 7_2 | 30.47 | 5.96 | 11.94 | 0.04 | 0.51 | −0.06 | 0.15 | 1.26 |
| 8_1 | 30.11 | 5.93 | 11.89 | | | | | |
| 8_2 | 29.92 | 5.84 | 11.71 | 0.19 | 0.54 | 0.07 | 0.30 | 1.32 |
| 9_1 | 29.12 | 5.70 | 11.42 | | | | | |
| 9_2 | 29.08 | 5.69 | 11.41 | 0.04 | 0.39 | −0.04 | 0.12 | 1.07 |
| 10_1 | 29.46 | 5.70 | 11.43 | | | | | |
| 10_2 | 29.54 | 5.77 | 11.57 | −0.07 | 0.42 | −0.16 | 0.01 | 1.12 |
| 11_1 | 29.80 | 5.83 | 11.68 | | | | | |
| 11_2 | 29.73 | 5.83 | 11.67 | 0.08 | 0.41 | −0.01 | 0.16 | 1.11 |
| 12_1 | 29.24 | 5.57 | 11.16 | | | | | |
| 12_2 | 29.42 | 5.65 | 11.33 | −0.18 | 0.49 | −0.29 | −0.08 | 1.24 |
| 13_1 | 29.81 | 5.75 | 11.52 | | | | | |
| 13_2 | 29.84 | 5.77 | 11.57 | −0.02 | 0.42 | −0.11 | 0.07 | 1.13 |
| 14_1 | 29.69 | 5.76 | 11.55 | | | | | |
| 14_2 | 29.50 | 5.70 | 11.43 | 0.18 | 0.43 | 0.10 | 0.27 | 1.14 |
| 15_1 | 29.37 | 5.61 | 11.24 | | | | | |
| 15_2 | 29.53 | 5.65 | 11.32 | −0.16 | 0.54 | −0.27 | −0.05 | 1.30 |
| 16_1 | 29.69 | 5.66 | 11.34 | | | | | |
| 16_2 | 29.59 | 5.63 | 11.28 | 0.10 | 0.52 | −0.01 | 0.21 | 1.28 |
| 17_1 | 29.45 | 5.58 | 11.18 | | | | | |
| 17_2 | 29.27 | 5.49 | 11.00 | 0.18 | 0.59 | 0.06 | 0.30 | 1.39 |
| 18_1 | 29.45 | 5.51 | 11.04 | | | | | |
| 18_2 | 29.43 | 5.51 | 11.05 | 0.02 | 0.53 | −0.09 | 0.13 | 1.30 |
| 19_1 | 29.42 | 5.50 | 11.02 | | | | | |
| 19_2 | 29.32 | 5.47 | 10.96 | 0.10 | 0.66 | −0.03 | 0.24 | 1.51 |
| Mean | 29.63 | 5.74 | 11.51 | 0.01 | 0.49 | −0.09 | 0.12 | 1.23 |
Table 3.
The average temperature of each region of interest in the lateral arm region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 28.68 | 5.76 | 11.55 | | | | | |
| 1_2 | 28.88 | 5.88 | 11.79 | −0.20 | 0.76 | −0.36 | −0.04 | 1.69 |
| 2_1 | 28.73 | 5.85 | 11.72 | | | | | |
| 2_2 | 28.62 | 5.86 | 11.75 | 0.12 | 0.56 | 0.00 | 0.23 | 1.34 |
| 3_1 | 28.63 | 5.84 | 11.70 | | | | | |
| 3_2 | 28.11 | 5.73 | 11.49 | 0.52 | 0.78 | 0.36 | 0.68 | 1.72 |
| 4_1 | 28.13 | 5.70 | 11.42 | | | | | |
| 4_2 | 28.19 | 5.74 | 11.51 | −0.06 | 0.67 | −0.19 | 0.08 | 1.52 |
| 5_1 | 28.28 | 5.73 | 11.48 | | | | | |
| 5_2 | 28.16 | 5.72 | 11.47 | 0.11 | 0.42 | 0.02 | 0.19 | 1.12 |
| 6_1 | 28.16 | 5.74 | 11.51 | | | | | |
| 6_2 | 27.88 | 5.67 | 11.37 | 0.28 | 0.56 | 0.16 | 0.40 | 1.35 |
| 7_1 | 28.64 | 5.81 | 11.63 | | | | | |
| 7_2 | 28.36 | 5.73 | 11.48 | 0.27 | 0.76 | 0.12 | 0.43 | 1.69 |
| 8_1 | 29.02 | 5.89 | 11.79 | | | | | |
| 8_2 | 28.73 | 5.83 | 11.68 | 0.29 | 0.63 | 0.16 | 0.42 | 1.46 |
| 9_1 | 28.46 | 5.79 | 11.60 | | | | | |
| 9_2 | 28.22 | 5.77 | 11.56 | 0.23 | 0.79 | 0.07 | 0.39 | 1.75 |
| 10_1 | 29.14 | 5.86 | 11.74 | | | | | |
| 10_2 | 28.71 | 5.79 | 11.61 | 0.43 | 0.67 | 0.29 | 0.57 | 1.54 |
| 11_1 | 29.53 | 5.90 | 11.82 | | | | | |
| 11_2 | 29.27 | 5.89 | 11.80 | 0.26 | 0.42 | 0.17 | 0.35 | 1.12 |
| 12_1 | 29.19 | 5.88 | 11.79 | | | | | |
| 12_2 | 29.11 | 5.90 | 11.82 | 0.07 | 0.59 | −0.05 | 0.19 | 1.39 |
| 13_1 | 28.35 | 5.64 | 11.31 | | | | | |
| 13_2 | 28.12 | 5.61 | 11.25 | 0.22 | 0.71 | 0.07 | 0.37 | 1.59 |
| 14_1 | 28.76 | 5.71 | 11.44 | | | | | |
| 14_2 | 28.66 | 5.71 | 11.45 | 0.10 | 0.60 | −0.03 | 0.22 | 1.41 |
| 15_1 | 28.47 | 5.65 | 11.32 | | | | | |
| 15_2 | 28.56 | 5.72 | 11.47 | −0.10 | 0.70 | −0.24 | 0.05 | 1.58 |
| 16_1 | 27.73 | 5.40 | 10.82 | | | | | |
| 16_2 | 27.59 | 5.39 | 10.80 | 0.14 | 0.65 | 0.01 | 0.28 | 1.49 |
| 17_1 | 28.01 | 5.44 | 10.90 | | | | | |
| 17_2 | 27.91 | 5.42 | 10.86 | 0.10 | 0.46 | 0.00 | 0.20 | 1.19 |
| 18_1 | 27.70 | 5.47 | 10.96 | | | | | |
| 18_2 | 27.63 | 5.44 | 10.91 | 0.06 | 0.69 | −0.08 | 0.21 | 1.57 |
| 19_1 | 28.43 | 5.50 | 11.03 | | | | | |
| 19_2 | 28.37 | 5.50 | 11.03 | 0.05 | 0.45 | −0.05 | 0.14 | 1.17 |
| Mean | 28.45 | 5.71 | 11.44 | 0.15 | 0.62 | 0.02 | 0.28 | 1.46 |
Table 4.
The average temperature of each region of interest in the medial arm region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 28.60 | 5.48 | 10.98 | | | | | |
| 1_2 | 28.57 | 5.47 | 10.97 | 0.03 | 0.49 | −0.07 | 0.13 | 1.24 |
| 2_1 | 28.68 | 5.43 | 10.88 | | | | | |
| 2_2 | 28.70 | 5.45 | 10.93 | −0.01 | 0.45 | −0.11 | 0.08 | 1.17 |
| 3_1 | 29.46 | 5.79 | 11.60 | | | | | |
| 3_2 | 29.36 | 5.76 | 11.54 | 0.10 | 0.45 | 0.01 | 0.20 | 1.17 |
| 4_1 | 28.85 | 5.57 | 11.16 | | | | | |
| 4_2 | 28.77 | 5.56 | 11.14 | 0.08 | 0.40 | 0.00 | 0.17 | 1.09 |
| 5_1 | 29.39 | 5.84 | 11.71 | | | | | |
| 5_2 | 29.31 | 5.80 | 11.63 | 0.08 | 0.43 | −0.02 | 0.17 | 1.14 |
| 6_1 | 29.02 | 5.70 | 11.42 | | | | | |
| 6_2 | 28.91 | 5.66 | 11.34 | 0.11 | 0.42 | 0.02 | 0.20 | 1.12 |
| 7_1 | 28.00 | 5.23 | 10.50 | | | | | |
| 7_2 | 28.10 | 5.28 | 10.58 | −0.10 | 0.69 | −0.25 | 0.04 | 1.57 |
| Mean | 28.84 | 5.57 | 11.17 | 0.04 | 0.48 | −0.06 | 0.14 | 1.21 |
Table 5.
The average temperature of each region of interest in the dorsal hand region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 31.25 | 5.51 | 11.05 | | | | | |
| 1_2 | 31.11 | 5.53 | 11.08 | 0.13 | 0.44 | 0.04 | 0.22 | 1.15 |
| 2_1 | 31.27 | 5.53 | 11.08 | | | | | |
| 2_2 | 31.01 | 5.49 | 11.00 | 0.26 | 0.49 | 0.15 | 0.36 | 1.22 |
| 3_1 | 30.85 | 5.38 | 10.79 | | | | | |
| 3_2 | 30.73 | 5.37 | 10.76 | 0.11 | 0.59 | −0.01 | 0.23 | 1.41 |
| 4_1 | 30.56 | 5.29 | 10.60 | | | | | |
| 4_2 | 30.60 | 5.31 | 10.65 | −0.04 | 0.48 | −0.14 | 0.06 | 1.21 |
| 5_1 | 30.76 | 5.32 | 10.67 | | | | | |
| 5_2 | 30.65 | 5.33 | 10.68 | 0.11 | 0.48 | 0.01 | 0.21 | 1.22 |
| 6_1 | 30.54 | 5.25 | 10.52 | | | | | |
| 6_2 | 30.36 | 5.21 | 10.46 | 0.18 | 0.52 | 0.07 | 0.29 | 1.28 |
| 7_1 | 29.93 | 5.06 | 10.15 | | | | | |
| 7_2 | 30.04 | 5.13 | 10.29 | −0.11 | 0.45 | −0.20 | −0.01 | 1.17 |
| 8_1 | 30.34 | 5.13 | 10.29 | | | | | |
| 8_2 | 30.29 | 5.13 | 10.29 | 0.06 | 0.44 | −0.03 | 0.15 | 1.16 |
| 9_1 | 30.37 | 5.14 | 10.32 | | | | | |
| 9_2 | 30.14 | 5.11 | 10.24 | 0.23 | 0.48 | 0.13 | 0.33 | 1.21 |
| 10_1 | 30.27 | 5.16 | 10.35 | | | | | |
| 10_2 | 30.31 | 5.22 | 10.46 | −0.04 | 0.53 | −0.15 | 0.07 | 1.29 |
| 11_1 | 30.47 | 5.08 | 10.20 | | | | | |
| 11_2 | 30.62 | 5.13 | 10.29 | −0.16 | 0.50 | −0.26 | −0.05 | 1.25 |
| 12_1 | 30.64 | 5.52 | 11.07 | | | | | |
| 12_2 | 30.57 | 5.50 | 11.03 | 0.07 | 0.72 | −0.07 | 0.22 | 1.62 |
| 13_1 | 30.05 | 5.13 | 10.29 | | | | | |
| 13_2 | 29.84 | 5.10 | 10.23 | 0.21 | 0.71 | 0.06 | 0.36 | 1.61 |
| 14_1 | 29.76 | 4.96 | 9.95 | | | | | |
| 14_2 | 29.69 | 4.97 | 9.98 | 0.06 | 0.64 | −0.07 | 0.20 | 1.49 |
| 15_1 | 28.73 | 5.19 | 10.40 | | | | | |
| 15_2 | 28.77 | 5.23 | 10.48 | −0.04 | 0.66 | −0.18 | 0.10 | 1.51 |
| 16_1 | 28.33 | 5.05 | 10.13 | | | | | |
| 16_2 | 28.27 | 5.07 | 10.16 | 0.06 | 0.63 | −0.07 | 0.19 | 1.47 |
| 17_1 | 28.15 | 4.91 | 9.84 | | | | | |
| 17_2 | 28.08 | 4.89 | 9.82 | 0.07 | 0.75 | −0.09 | 0.23 | 1.67 |
| 18_1 | 29.26 | 4.96 | 9.94 | | | | | |
| 18_2 | 29.43 | 4.95 | 9.92 | −0.17 | 0.57 | −0.29 | −0.06 | 1.36 |
| 19_1 | 28.89 | 4.96 | 9.95 | | | | | |
| 19_2 | 28.88 | 4.97 | 9.96 | 0.01 | 0.61 | −0.11 | 0.14 | 1.43 |
| 20_1 | 28.77 | 5.13 | 10.29 | | | | | |
| 20_2 | 28.74 | 5.15 | 10.32 | 0.02 | 0.80 | −0.14 | 0.18 | 1.76 |
| 21_1 | 29.28 | 4.96 | 9.95 | | | | | |
| 21_2 | 29.25 | 4.90 | 9.83 | 0.03 | 0.52 | −0.08 | 0.14 | 1.28 |
| 22_1 | 28.99 | 5.07 | 10.17 | | | | | |
| 22_2 | 28.98 | 4.90 | 9.84 | 0.00 | 0.69 | −0.14 | 0.14 | 1.56 |
| 23_1 | 29.11 | 5.12 | 10.28 | | | | | |
| 23_2 | 28.97 | 5.03 | 10.10 | 0.14 | 0.74 | −0.02 | 0.29 | 1.65 |
| 24_1 | 29.29 | 4.87 | 9.77 | | | | | |
| 24_2 | 29.11 | 4.82 | 9.67 | 0.17 | 0.55 | 0.06 | 0.29 | 1.32 |
| 25_1 | 29.10 | 4.95 | 9.94 | | | | | |
| 25_2 | 29.02 | 4.86 | 9.74 | 0.08 | 0.64 | −0.05 | 0.22 | 1.48 |
| 26_1 | 29.10 | 5.14 | 10.32 | | | | | |
| 26_2 | 28.88 | 5.05 | 10.13 | 0.21 | 0.79 | 0.05 | 0.38 | 1.75 |
| Mean | 29.74 | 5.14 | 10.30 | 0.06 | 0.59 | −0.06 | 0.19 | 1.40 |
Table 6.
The average temperature of each region of interest in the ventral hand region.
| ROI | Mean (°C) | SD | Extended Uncertainty | Difference (ΔT, Right Side–Left Side) |
|---|
| Mean (°C) | SD | 95% CI Lower | 95% CI Upper | Extended Uncertainty |
|---|
| 1_1 | 29.10 | 5.66 | 11.34 | | | | | |
| 1_2 | 29.09 | 5.67 | 11.36 | 0.01 | 0.40 | −0.07 | 0.10 | 1.09 |
| 2_1 | 29.63 | 5.73 | 11.47 | | | | | |
| 2_2 | 29.71 | 5.77 | 11.57 | −0.08 | 0.41 | −0.17 | 0.00 | 1.11 |
| 3_1 | 29.73 | 5.80 | 11.62 | | | | | |
| 3_2 | 29.57 | 5.76 | 11.54 | 0.17 | 0.38 | 0.08 | 0.25 | 1.06 |
| 4_1 | 29.01 | 5.53 | 11.08 | | | | | |
| 4_2 | 29.13 | 5.59 | 11.20 | −0.11 | 0.51 | −0.22 | −0.01 | 1.27 |
| 5_1 | 29.82 | 5.74 | 11.49 | | | | | |
| 5_2 | 29.85 | 5.76 | 11.55 | −0.03 | 0.44 | −0.13 | 0.06 | 1.16 |
| 6_1 | 29.53 | 5.70 | 11.43 | | | | | |
| 6_2 | 29.38 | 5.65 | 11.32 | 0.16 | 0.45 | 0.07 | 0.25 | 1.17 |
| 7_1 | 29.19 | 5.52 | 11.06 | | | | | |
| 7_2 | 29.33 | 5.60 | 11.23 | −0.15 | 0.57 | −0.26 | −0.03 | 1.37 |
| 8_1 | 29.69 | 5.60 | 11.22 | | | | | |
| 8_2 | 29.62 | 5.59 | 11.21 | 0.07 | 0.57 | −0.05 | 0.18 | 1.38 |
| 9_1 | 29.31 | 5.52 | 11.06 | | | | | |
| 9_2 | 29.12 | 5.50 | 11.02 | 0.19 | 0.68 | 0.05 | 0.33 | 1.55 |
| 10_1 | 28.16 | 5.13 | 10.29 | | | | | |
| 10_2 | 28.17 | 5.14 | 10.30 | 0.00 | 0.63 | −0.14 | 0.13 | 1.47 |
| 11_1 | 28.70 | 5.33 | 10.68 | | | | | |
| 11_2 | 28.80 | 5.36 | 10.74 | −0.10 | 0.83 | −0.27 | 0.08 | 1.81 |
| 12_1 | 29.32 | 5.51 | 11.05 | | | | | |
| 12_2 | 29.30 | 5.57 | 11.16 | 0.02 | 0.73 | −0.13 | 0.17 | 1.64 |
| 13_1 | 29.98 | 5.60 | 11.22 | | | | | |
| 13_2 | 29.88 | 5.60 | 11.22 | 0.10 | 0.63 | −0.03 | 0.23 | 1.48 |
| 14_1 | 29.15 | 5.51 | 11.03 | | | | | |
| 14_2 | 29.09 | 5.47 | 10.96 | 0.06 | 0.86 | −0.12 | 0.24 | 1.88 |
| 15_1 | 27.55 | 5.26 | 10.55 | | | | | |
| 15_2 | 27.49 | 5.32 | 10.67 | 0.06 | 0.87 | −0.12 | 0.24 | 1.89 |
| 16_1 | 28.16 | 5.23 | 10.48 | | | | | |
| 16_2 | 28.05 | 5.31 | 10.65 | 0.11 | 0.84 | −0.06 | 0.29 | 1.84 |
| 17_1 | 28.41 | 5.25 | 10.52 | | | | | |
| 17_2 | 28.37 | 5.27 | 10.57 | 0.04 | 0.69 | −0.10 | 0.18 | 1.56 |
| 18_1 | 27.71 | 5.25 | 10.52 | | | | | |
| 18_2 | 27.52 | 5.21 | 10.44 | 0.19 | 0.82 | 0.02 | 0.36 | 1.80 |
| 19_1 | 28.16 | 5.31 | 10.64 | | | | | |
| 19_2 | 27.97 | 5.34 | 10.70 | 0.20 | 0.88 | 0.02 | 0.38 | 1.91 |
| 20_1 | 28.41 | 5.35 | 10.72 | | | | | |
| 20_2 | 28.30 | 5.36 | 10.74 | 0.11 | 0.74 | −0.04 | 0.26 | 1.66 |
| 21_1 | 27.35 | 5.29 | 10.61 | | | | | |
| 21_2 | 27.26 | 5.23 | 10.49 | 0.09 | 0.84 | −0.09 | 0.26 | 1.85 |
| 22_1 | 28.00 | 5.36 | 10.75 | | | | | |
| 22_2 | 27.88 | 5.25 | 10.54 | 0.12 | 0.85 | −0.06 | 0.29 | 1.86 |
| 23_1 | 28.40 | 5.36 | 10.75 | | | | | |
| 23_2 | 28.20 | 5.30 | 10.63 | 0.20 | 0.76 | 0.04 | 0.36 | 1.70 |
| 24_1 | 27.25 | 5.16 | 10.35 | | | | | |
| 24_2 | 27.08 | 5.14 | 10.31 | 0.17 | 0.77 | 0.01 | 0.33 | 1.71 |
| 25_1 | 27.59 | 5.34 | 10.71 | | | | | |
| 25_2 | 27.41 | 5.33 | 10.69 | 0.19 | 0.79 | 0.02 | 0.35 | 1.75 |
| 26_1 | 27.84 | 5.48 | 10.98 | | | | | |
| 26_2 | 27.65 | 5.48 | 10.98 | 0.19 | 0.93 | −0.01 | 0.38 | 2.01 |
| Mean | 28.62 | 5.44 | 10.91 | 0.07 | 0.69 | −0.07 | 0.22 | 1.58 |
Table 7.
Comparison of the average temperature in the same region of interest according to sex and age group.
| Characteristics | Male (°C) | Female (°C) | Mean (°C) | Difference between Sexes (°C) | p Value |
|---|
| Dorsal arm region | | | | | <0.001 a |
| 20s (n = 183) | 29.82 ± 5.37 | 28.99 ± 6.05 | 29.43 ± 5.69 | 0.83 (95% CI, 0.57–1.09) | <0.001 b |
| 30s (n = 213) | 29.45 ± 5.83 | 26.06 ± 5.85 | 27.79 ± 5.84 | 3.39 (95% CI, 3.19–3.59) | <0.001 b |
| 40s (n = 228) | 30.44 ± 5.55 | 28.58 ± 6.41 | 29.47 ± 6.00 | 1.86 (95% CI, 1.61–2.12) | <0.001 b |
| 50s (n = 177) | 31.15 ± 5.04 | 28.82 ± 5.53 | 29.68 ± 5.35 | 2.33 (95% CI, 2.12–2.54) | <0.001 b |
| 60s (n = 104) | 32.51 ± 4.59 | 29.59 ± 5.82 | 30.49 ± 5.44 | 2.92 (95% CI, 2.65–3.18) | <0.001 b |
| Sum | 30.31 ± 5.43 | 28.32 ± 5.94 | 29.22 ± 5.71 | 1.99 (95% CI, 1.76–2.22 | <0.001 b |
| Ventral arm region | | | | | <0.001 a |
| 20s (n = 183) | 30.18 ± 5.41 | 29.40 ± 6.12 | 29.81 ± 5.74 | 0.78 (95% CI, 0.60–0.96) | <0.001 b |
| 30s (n = 213) | 29.95 ± 5.93 | 26.51 ± 5.92 | 28.25 ± 5.93 | 3.44 (95% CI, 3.31–3.58) | <0.001 b |
| 40s (n = 228) | 30.82 ± 5.59 | 28.90 ± 6.35 | 29.82 ± 5.99 | 1.92 (95% CI, 1.73–2.10) | <0.001 b |
| 50s (n = 177) | 31.59 ± 5.05 | 29.25 ± 5.56 | 30.11 ± 5.37 | 2.34 (95% CI, 2.19–2.49) | <0.001 b |
| 60s (n = 104) | 32.89 ± 4.55 | 30.05 ± 5.86 | 30.92 ± 5.46 | 2.84 (95% CI, 2.64–3.05) | <0.001 b |
| Sum | 30.72 ± 5.47 | 28.73 ± 5.97 | 29.63 ± 5.74 | 2.00 (95% CI, 1.84–2.16) | <0.001 b |
| Lateral arm region | | | | | <0.001 a |
| 20s (n = 183) | 29.18 ± 5.40 | 28.29 ± 6.16 | 28.76 ± 5.76 | 0.90 (95% CI, 0.66–1.14) | <0.001 b |
| 30s (n = 213) | 28.76 ± 5.89 | 25.13 ± 5.85 | 26.97 ± 5.87 | 3.63 (95% CI, 3.43–3.83) | <0.001 b |
| 40s (n = 228) | 29.85 ± 5.52 | 27.62 ± 6.31 | 28.69 ± 5.93 | 2.23 (95% CI, 1.99–2.48) | <0.001 b |
| 50s (n = 177) | 30.57 ± 5.07 | 27.88 ± 5.52 | 28.87 ± 5.35 | 2.69 (95% CI, 2.48–2.90) | <0.001 b |
| 60s (n = 104) | 31.67 ± 4.60 | 28.81 ± 5.73 | 29.69 ± 5.38 | 2.85 (95% CI, 2.58–3.13) | <0.001 b |
| Sum | 29.66 ± 5.45 | 27.44 ± 5.92 | 28.62 ± 5.67 | 2.22 (95% CI, 2.00–2.45) | <0.001 b |
| Medial arm region | | | | | <0.001 a |
| 20s (n = 183) | 29.25 ± 5.25 | 28.62 ± 5.97 | 28.94 ± 5.60 | 0.63 (95% CI, 0.24–1.01) | 0.003 b |
| 30s (n = 213) | 29.11 ± 5.72 | 25.80 ± 5.64 | 27.38 ± 5.68 | 3.15 (95% CI, 2.90–3.40) | <0.001 b |
| 40s (n = 228) | 29.96 ± 5.44 | 28.21 ± 6.18 | 28.85 ± 5.91 | 1.74 (95% CI, 1.29–2.20) | <0.001 b |
| 50s (n = 177) | 30.77 ± 4.98 | 28.50 ± 5.37 | 29.20 ± 5.25 | 2.27 (95% CI, 1.96–2.58) | <0.001 b |
| 60s (n = 104) | 31.84 ± 4.56 | 29.34 ± 5.72 | 30.48 ± 5.19 | 2.51 (95% CI, 2.06–2.95) | <0.001 b |
| Sum | 29.84 ± 5.33 | 28.00 ± 5.78 | 28.84 ± 5.57 | 1.84 (95% CI, 1.49–2.20) | <0.001 b |
| Dorsal hand region | | | | | <0.001 a |
| 20s (n = 183) | 29.86 ± 5.31 | 29.04 ± 5.81 | 29.46 ± 5.56 | 0.82 (95% CI, 0.45–1.18) | <0.001 b |
| 30s (n = 213) | 32.38 ± 3.83 | 29.38 ± 5.25 | 30.81 ± 4.57 | 3.00 (95% CI, 2.63–3.38) | <0.001 b |
| 40s (n = 228) | 30.70 ± 4.92 | 28.93 ± 5.36 | 29.87 ± 5.13 | 1.77 (95% CI, 1.44–2.11) | <0.001 b |
| 50s (n = 177) | 29.67 ± 5.33 | 27.34 ± 5.21 | 28.52 ± 5.27 | 2.33 (95% CI, 2.01–2.66) | <0.001 b |
| 60s (n = 104) | 29.58 ± 5.51 | 28.76 ± 4.98 | 29.15 ± 5.23 | 0.83 (95% CI, 0.51–1.14) | <0.001 b |
| Sum | 30.51 ± 4.93 | 28.81 ± 5.38 | 29.74 ± 5.14 | 1.70 (95% CI, 1.36–2.05) | <0.001 b |
| Ventral hand region | | | | | <0.001 a |
| 20s (n = 183) | 29.12 ± 5.14 | 28.07 ± 5.79 | 28.39 ± 5.59 | 1.05 (95% CI, 0.70–1.40) | <0.001 b |
| 30s (n = 213) | 29.28 ± 5.78 | 25.48 ± 5.43 | 27.21 ± 5.59 | 3.80 (95% CI, 3.49–4.10) | <0.001 b |
| 40s (n = 228) | 29.52 ± 5.21 | 27.88 ± 5.80 | 28.75 ± 5.49 | 1.64 (95% CI, 1.27–2.02) | <0.001 b |
| 50s (n = 177) | 30.86 ± 4.75 | 28.45 ± 5.49 | 29.67 ± 5.11 | 2.41 (95% CI, 2.12–2.70) | <0.001 b |
| 60s (n = 104) | 31.30 ± 4.55 | 29.14 ± 5.67 | 30.17 ± 5.13 | 2.16 (95% CI, 1.74–2.59) | <0.001 b |
| Sum | 29.71 ± 5.22 | 27.72 ± 5.63 | 28.62 ± 5.44 | 2.00 (95% CI, 1.67–2.33) | <0.001 b |












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}