


Spinal Cord Epidural Stimulation Improves Lower Spine Sitting Posture Following Severe Cervical Spinal Cord Injury

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocol
2.2. Data Analysis
2.3. Statistical Comparisons
3. Results
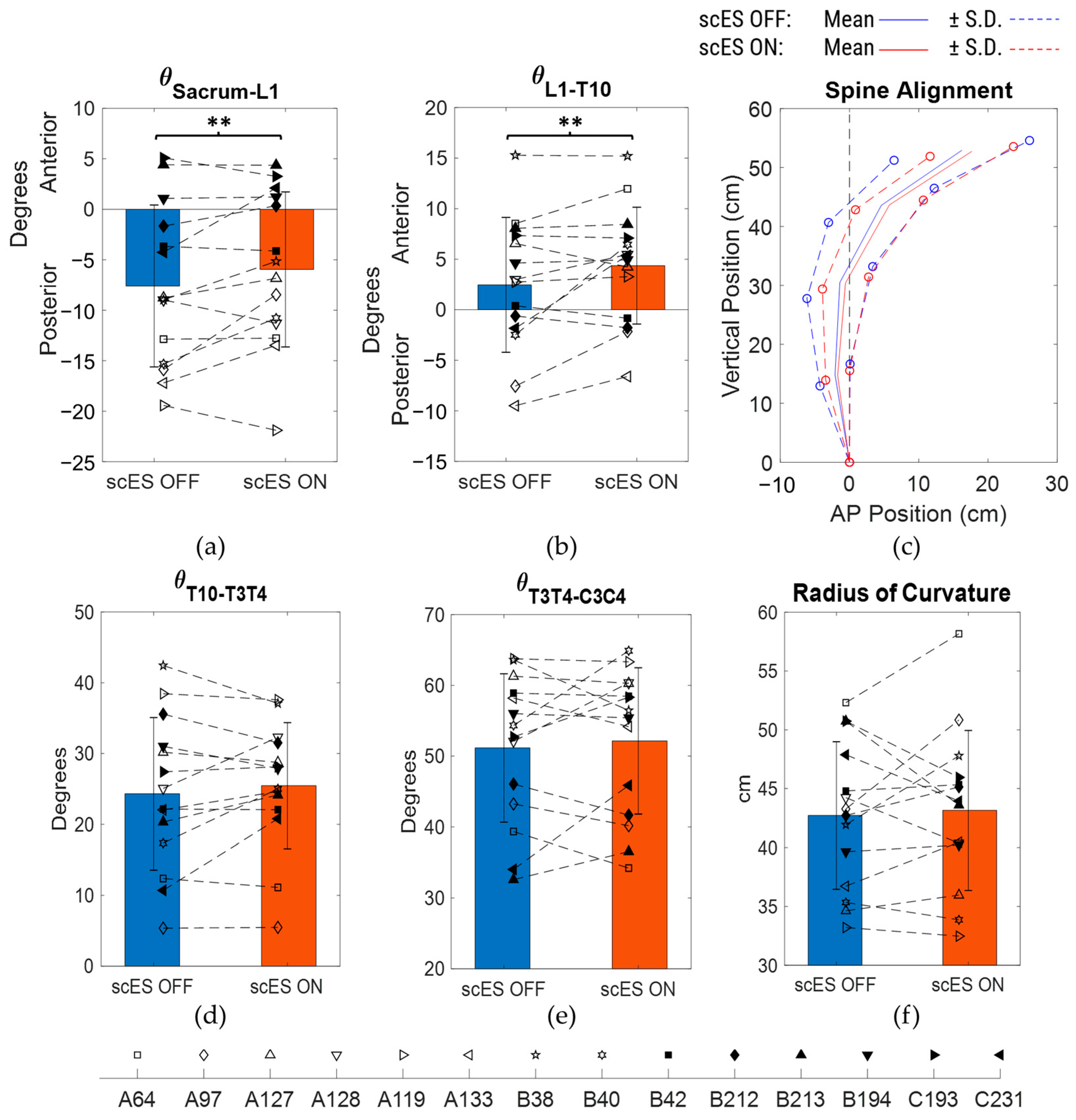
3.1. Posture Outcomes
3.2. Level of Independence
3.3. Subset Analysis
4. Discussion
4.1. Posture and Independence with scES
4.2. Physiological Response to scES
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Additional Demographics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PID | Spine Characteristics | Trunk-Specific Intervention? |
|---|---|---|
| A64 |
| No |
| A97 |
| No |
| A127 |
| Yes–80 sessions |
| A128 |
| No |
| A119 |
| No |
| A133 |
| No |
| B38 |
| Yes–160 sessions |
| B40 |
| No |
| B42 |
| No |
| B212 |
| Yes–80 sessions |
| B213 |
| Yes–80 sessions |
| B194 |
| Yes–80 sessions |
| C193 |
| No |
| C231 |
| No |
Appendix B. scES Electrode Configurations for Trunk Stability
| PID | Configuration | Frequency | Pulse Width | Amplitude |
|---|---|---|---|---|
| A64 | C1: (0-/5-/11-//1+/2+/7+/8+/12+/13+) | 21.67 Hz | 800 µs | 11.2 mA |
| C2: (0-/5-/11-//2+/3+/8+/9+/13+/14+) | 21.67 Hz | 800 µs | 13.5 mA | |
| A97 | C1: (0-/5-//2+/7+) | 20 Hz | 650 µs | 6.9 mA |
| C2: (6-//0+/1+/2+/3+/4+/5+/7+/8+/9+/10+/11+/12+/13+/14+/15+) | 100 Hz | 500 µs | 5.5 mA | |
| A127 | C1: (5-/11-//0+/1+/6+/7+/12+) | 35 Hz | 650 µs | 18.8 mA |
| A128 | C1: (5-//0+/11+) | 16.67 Hz | 1000 µs | 25.5 mA |
| C2: (8-//0+/1+/2+/3+/4+/5+/6+/7+/9+/10+/11+/12+/13+/14+/15+) | 100 Hz | 500 µs | 10 mA | |
| A119 | C1: (0-/5-/11-//2+/7+/8+/13+) | 37.5 Hz | 600 µs | 12.1 mA |
| C2: (3-/8-/14-//1+/2+/4+/7+/9+/10+/12+/13+/15+) | 150 Hz | 300 µs | 10 mA | |
| A133 | C1: (0-/1-/5-/11-/12-//2+/3+/8+/13+/14+) | 25 Hz | 600 µs | 12. 9 mA |
| C2: (0-/11-//7+/8+/9+/10+) | 16.67 Hz | 600 µs | 5 mA | |
| B38 | C1: (0-/5-/11-//2+/3+/7+/8+/13+/14+) | 30 Hz | 950 µs | 15.3 mA |
| B40 | C1: (5-//0+/11+) | 30 Hz | 850 µs | 3.5 mA |
| C2:(7-//0+/1+/2+/3+/4+/6+/8+/9+/10+/11+/12+/13+/14+/15+) | 90 Hz | 450 µs | 8 mA | |
| C3: (0-//6+/12+) | 22.5 Hz | 700 µs | 4.4 mA | |
| B42 | C1: (1-/6-/12-//2+/3+/7+/8+/13+/14+) | 32 Hz | 650 µs | 12.9 mA |
| B212 | C1: (5-/11-//0+/6+/12+) | 21.67 Hz | 900 µs | 8.2 mA |
| C2: (1-/7-/12-//0+/2+/3+/4+/6+/8+/9+/10+/11+/13+/14+/15+) | 130 Hz | 300 µs | 6.2 mA | |
| B213 | C1: (0-/5-/11-//1+/6+/12+) | 16.67 Hz | 1000 µs | 17 mA |
| B194 | C1: (0-/5-/6-/11-/12-//1+/2+/7+/13+) | 28 Hz | 700 µs | 7.8 mA |
| C2: (0-/1-/2-//5+/6+/7+) | 140 Hz | 300 µs | 2 mA | |
| C193 | C1: (0-/5-/11-//1+/2+/6+/7+/12+/13+) | 25 Hz | 800 µs | 10.1 mA |
| C2: (0-/1-/5-/6-/11-/12-//2+/3+/13+/14+) | 25 Hz | 700 µs | 11.5 mA | |
| C231 | C1: (0-/5-/11-//2+/7+/8+/9+/13+) | 19.17 Hz | 700 µs | 6.1 mA |
| C3: (10-//2+/3+/4+/7+/8+/9+/13+/14+/15+) | 9.58 Hz | 300 µs | 3.1 mA |

References
- Murphy, J.O.; Audu, M.L.; Lombardo, L.M.; Foglyano, K.M.; Triolo, R.J. Feasibility of closed-loop controller for righting seated posture after spinal cord injury. J. Rehabil. Res. Dev. 2014, 51, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Hagen, E.; Eide, G.E.; Rekand, T.; Gilhus, N.; Gronning, M. A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010, 48, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Lanzetta, D.; Cattaneo, D.; Pellegatta, D.; Cardini, R. Trunk control in unstable sitting posture during functional activities in healthy subjects and patients with multiple sclerosis. Arch. Phys. Med. Rehabil. 2004, 85, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.; Wilson, S. Trunk posture and spinal stability. Clin. Biomech. 2001, 16, 650–659. [Google Scholar] [CrossRef]
- Lissy, D.; Kukke, S. Preliminary performance of a surgically implanted neuroprosthesis for standing and transfers—Where do we stand? Development 2001, 38, 609–617. [Google Scholar]
- Minkel, J.L. Seating and mobility considerations for people with spinal cord injury. Phys. Ther. 2000, 80, 701–709. [Google Scholar] [CrossRef]
- Seelen, H.A.M.; Potten, Y.J.M.; Huson, A.; Spaans, F.; Reulen, J.P.H. Impaired balance control in paraplegic subjects. J. Electromyogr. Kinesiol. 1997, 7, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Hobson, D.A.; Tooms, R.E. Seated lumbar/pelvic alignment: A comparison between spinal cord-injured and noninjured groups. Spine 1992, 17, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.D. Targeting recovery: Priorities of the spinal cord-injured population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef]
- Triolo, R.J.; Bailey, S.N.; Miller, M.E.; Lombardo, L.M.; Audu, M.L. Effects of stimulating hip and trunk muscles on seated stability, posture, and reach after spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.; Zahharova, A.; Reinvee, M.; Asser, T.; Gapeyeva, H.; Vahtrik, D. The effect of functional electrical stimulation and therapeutic exercises on trunk muscle tone and dynamic sitting balance in persons with chronic spinal cord injury: A crossover trial. Medicina 2019, 55, 619. [Google Scholar] [CrossRef]
- Wu, G.A.; Lombardo, L.; Triolo, R.J.; Bogie, K.M. The effects of combined trunk and gluteal neuromuscular electrical stimulation on posture and tissue health in spinal cord injury. PM&R 2013, 5, 688–696. [Google Scholar]
- Rath, M.; Vette, A.H.; Ramasubramaniam, S.; Li, K.; Burdick, J.; Edgerton, V.R.; Gerasimenko, Y.P.; Sayenko, D.G. Trunk stability enabled by noninvasive spinal electrical stimulation after spinal cord injury. J. Neurotrauma 2018, 35, 2540–2553. [Google Scholar] [CrossRef]
- Gerasimenko, Y.; Gorodnichev, R.; Moshonkina, T.; Sayenko, D.; Gad, P.; Edgerton, V.R. Transcutaneous electrical spinal-cord stimulation in humans. Ann. Phys. Rehabil. Med. 2015, 58, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Singh, G.; Sommerfeld, J.H.; King, M.; Parikh, P.; Ugiliweneza, B.; D’Amico, J.; Gerasimenko, Y.; Behrman, A.L. Noninvasive spinal stimulation safely enables upright posture in children with spinal cord injury. Nat. Commun. 2021, 12, 5850. [Google Scholar] [CrossRef] [PubMed]
- Audu, M.L.; Lombardo, L.M.; Schnellenberger, J.R.; Foglyano, K.M.; Miller, M.E.; Triolo, R.J. A neuroprosthesis for control of seated balance after spinal cord injury. J. Neuroeng. Rehabil. 2015, 12, 8. [Google Scholar] [CrossRef]
- Friederich, A.R.; Bao, X.; Triolo, R.J.; Audu, M.L. Feedback control of upright seating with functional neuromuscular stimulation during a reaching task after spinal cord injury: A feasibility study. J. Neuroeng. Rehabil. 2022, 19, 139. [Google Scholar] [CrossRef]
- Rahimi, M.; Torkaman, G.; Ghabaee, M.; Ghasem-Zadeh, A. Advanced weight-bearing mat exercises combined with functional electrical stimulation to improve the ability of wheelchair-dependent people with spinal cord injury to transfer and attain independence in activities of daily living: A randomized controlled trial. Spinal Cord 2020, 58, 78–85. [Google Scholar] [PubMed]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; McKay, W.B.; Binder, H.; Hofstoetter, U.S. Targeting Lumbar Spinal Neural Circuitry by Epidural Stimulation to Restore Motor Function After Spinal Cord Injury. Neurotherapeutics 2016, 13, 284–294. [Google Scholar] [CrossRef]
- Dimitrijevic, M.R.; Gerasimenko, Y.; Pinter, M.M. Evidence for a spinal central pattern generator in humans. Ann. N. Y. Acad. Sci. 1998, 860, 360–376. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.; Harkema, S. Effects of lumbosacral spinal cord epidural stimulation for standing after chronic complete paralysis in humans. PLoS ONE 2015, 10, e0133998. [Google Scholar] [CrossRef] [PubMed]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of over-ground walking after chronic motor complete spinal cord injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Gill, M.; Linde, M.; Fautsch, K.; Hale, R.; Lopez, C.; Veith, D.; Calvert, J.; Beck, L.; Garlanger, K.; Edgerton, R. Epidural electrical stimulation of the lumbosacral spinal cord improves trunk stability during seated reaching in two humans with severe thoracic spinal cord injury. Front. Syst. Neurosci. 2020, 14, 79. [Google Scholar] [CrossRef]
- Rowald, A.; Komi, S.; Demesmaeker, R.; Baaklini, E.; Hernandez-Charpak, S.D.; Paoles, E.; Montanaro, H.; Cassara, A.; Becce, F.; Lloyd, B. Activity-dependent spinal cord neuromodulation rapidly restores trunk and leg motor functions after complete paralysis. Nat. Med. 2022, 28, 260–271. [Google Scholar] [CrossRef]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain 2014, 137, 1394–1409. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F., Jr.; Black William, C.; Babin Barry, J.; Anderson Rolph, E. Multivariate data analysis. In Upper Saddle River, 7th ed.; Prentice Hall: Hoboken, NJ, USA, 2009. [Google Scholar]
- Cohen, J. The effect size. In Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; pp. 77–83. [Google Scholar]
- Farivar, S.S.; Liu, H.; Hays, R.D. Half standard deviation estimate of the minimally important difference in HRQOL scores? Expert Rev. Pharmacoecon. Outcomes Res. 2004, 4, 515–523. [Google Scholar] [CrossRef]
- Hansen, T.; Slagsvold, B. The age and subjective well-being paradox revisited: A multidimensional perspective. Nor. Epidemiol. 2012, 22, 187–195. [Google Scholar]
- Boswell-Ruys, C.L.; Harvey, L.A.; Barker, J.J.; Ben, M.; Middleton, J.W.; Lord, S.R. Training unsupported sitting in people with chronic spinal cord injuries: A randomized controlled trial. Spinal Cord 2010, 48, 138–143. [Google Scholar] [CrossRef]
- Carini, F.; Mazzola, M.; Fici, C.; Palmeri, S.; Messina, M.; Damiani, P.; Tomasello, G. Posture and posturology, anatomical and physiological profiles: Overview and current state of art. Acta Biomed. 2017, 88, 11–16. [Google Scholar] [CrossRef]






| ID | Gender | Age | Time Since Injury | Neuro Level | AIS | BMI | Mobility | Lifestyle | Caregiver | Transfers |
|---|---|---|---|---|---|---|---|---|---|---|
| A64 | M | 55.7 | 38.6 | C4 | A | 21.6 | Power wheelchair | Sedentary | 24 h | Two-person |
| A97 | M | 38.6 | 15.4 | C4 | A | 16.7 | Power wheelchair | Sedentary | 24 h | Two-person |
| A127 | F | 40.6 | 13.1 | C4 | A | 23.9 | Manual wheelchair | Sedentary | Periodic | One person Transfer board |
| A128 | M | 38.6 | 8.7 | C4 | A | 23.7 | Manual wheelchair | Sedentary | Periodic | One person Transfer board |
| A119 | F | 26.4 | 11.5 | C5 | A | 17.6 | Power wheelchair | Sedentary | Periodic | Two-person |
| A133 | M | 34.6 | 13.1 | C5 | A | 27.9 | Power wheelchair | Sedentary | Periodic | One person Transfer board |
| B38 | M | 21.9 | 3.3 | C4 | B | 26.8 | Power wheelchair | Sedentary | Periodic | Two-person |
| B40 | M | 36.0 | 4.7 | C4 | B | 20.3 | Power wheelchair | Sedentary | 24 h | Two-person |
| B42 | M | 58.7 | 7.5 | C4 | B | 26.8 | Power wheelchair | Sedentary | 24 h | Two-person |
| B212 | F | 47.9 | 29.7 | C4 | B | 24.8 | Manual wheelchair | Sedentary | Periodic | One person Transfer board |
| B213 | F | 25.1 | 5.4 | C4 | B | 19.5 | Power wheelchair | Sedentary | 24 h | One person Transfer board |
| B194 | F | 37.8 | 18.2 | C5 | B | 17.9 | Manual wheelchair + SmartDrive | Sedentary | Independent | Independent Transfer board |
| C193 | F | 41.1 | 8.9 | C4 | C | 24.4 | Manual wheelchair + SmartDrive | Sedentary | Periodic | One person Transfer board |
| C231 | F | 26.8 | 5.7 | C6 | C | 23.5 | Manual wheelchair | Sedentary | 24 h | One person Transfer board |
| Parameter | scES OFF | scES ON | Change | p-Value | Effect Size | Classification |
|---|---|---|---|---|---|---|
| θS-L1 (°) | −7.6 ± 8.02 | −5.96 ± 7.68 | 1.64 ± 3.16 | 0.07 | 0.52 ** | Medium |
| θL1-T10 (°) | 2.46 ± 6.67 | 4.36 ± 5.78 | 1.9 ± 3.35 | 0.054 | 0.57 ** | Medium |
| θT10-T3T4 (°) | 24.32 ± 10.76 | 25.46 ± 8.9 | 1.14 ± 4.6 | 0.37 | 0.25 | Small |
| θT3T4-C3C4 (°) | 51.16 ± 10.48 | 52.15 ± 10.34 | 1 ± 6.06 | 0.55 | 0.16 | Very small |
| rcurvature (cm) | 42.72 ± 6.26 | 43.15 ± 6.79 | 0.42 ± 4.41 | 0.72 | 0.1 | Very small |
| % Independent | 98.5 [22.81, 100] | 100 [71.74, 100] | 0.12 [0, 12.65] | 0.18 | 0.12 | Small |
| % Assisted | 1.5 [0, 77.19] | 0 [0, 28.26] | −0.12 [−12.65, 0] | 0.18 | 0.12 | Small |
| No. of Independence Changes | 13.29 ± 22.1 | 3.43 ± 8.46 | −9.86 ± 16.8 | 0.047 * | 0.59 ** | Medium |
| Independence Score | 0.93 [0, 2.33] | 0 [0, 2] | −0.17 [−0.67, 0] | 0.34 | 0.43 | Small |
| Parameter | scES OFF | scES ON | Change | p-Value | Effect Size | Classification |
|---|---|---|---|---|---|---|
| θS-L1 (°) | −9.97 ± 8.84 | −7.73 ± 6.36 | 2.25 ± 3.54 | 0.18 | 0.63 ** | Medium |
| θL1-T10 (°) | −0.55 ± 7.46 | 2.65 ± 6.95 | 3.2 ± 3.72 | 0.09 | 0.86 ** | Large |
| θT10-T3T4 (°) | 17.78 ± 7.92 | 19.4 ± 8.99 | 1.62 ± 3.21 | 0.27 | 0.5 ** | Medium |
| θT3T4-C3C4 (°) | 51.13 ± 8.05 | 51.7 ± 11.9 | 0.58 ± 6.21 | 0.83 | 0.09 | Very small |
| rcurvature (cm) | 43.86 ± 6.97 | 45.77 ± 8.36 | 1.9 ± 4.67 | 0.37 | 0.41 | Small |
| % Independent | 11.88 [0, 40.23] | 53.87 [0, 100] | 12.91 [0, 31.52] | 0.38 | 0.96 ** | Large |
| % Assisted | 88.12 [59.77, 100] | 46.13 [0, 100] | −12.91 [−31.52, 0] | 0.38 | 0.96 ** | Large |
| % Assisted (1 Hand Only) | 0 [0, 15.6] | 0 [0, 0] | 0 [−15.6, 0] | 0.5 | 0.63 ** | Medium |
| % Assisted (2 Hands) | 5.94 [0, 17.44] | 0 [0, 5.97] | 0 [−11.47, 0] | 1 | 0.23 | Small |
| % Assisted (Trunk Only) | 22.89 [1.33, 53.59] | 1.18 [0, 20.58] | −1.21 [−21.75, 0] | 0.38 | 0.19 | Very Small |
| % Assisted (Trunk + 1 Hand) | 4 [0, 14.73] | 0 [0, 0] | −4 [−8.87, 0] | 0.25 | 1 ** | Large |
| % Assisted (Trunk + 2 Hands) | 8.87 [0, 31.4] | 0.61 [0, 1.7] | −0.38 [−15.75, 1.7] | 1 | 0.06 | Very Small |
| No. of Independence Changes | 29.67 ± 26.52 | 7.67 ± 12.16 | −22 ± 20.48 | 0.047 * | 1.07 ** | Large |
| Independence Score | 3.14 [1.64, 4.92] | 2.09 [0, 3.5] | −0.39 [−1.27, 0.08] | 0.69 | 0.57 ** | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joshi, K.; Rejc, E.; Ugiliweneza, B.; Harkema, S.J.; Angeli, C.A. Spinal Cord Epidural Stimulation Improves Lower Spine Sitting Posture Following Severe Cervical Spinal Cord Injury. Bioengineering 2023, 10, 1065. https://doi.org/10.3390/bioengineering10091065
Joshi K, Rejc E, Ugiliweneza B, Harkema SJ, Angeli CA. Spinal Cord Epidural Stimulation Improves Lower Spine Sitting Posture Following Severe Cervical Spinal Cord Injury. Bioengineering. 2023; 10(9):1065. https://doi.org/10.3390/bioengineering10091065
Chicago/Turabian StyleJoshi, Kundan, Enrico Rejc, Beatrice Ugiliweneza, Susan J. Harkema, and Claudia A. Angeli. 2023. "Spinal Cord Epidural Stimulation Improves Lower Spine Sitting Posture Following Severe Cervical Spinal Cord Injury" Bioengineering 10, no. 9: 1065. https://doi.org/10.3390/bioengineering10091065
APA StyleJoshi, K., Rejc, E., Ugiliweneza, B., Harkema, S. J., & Angeli, C. A. (2023). Spinal Cord Epidural Stimulation Improves Lower Spine Sitting Posture Following Severe Cervical Spinal Cord Injury. Bioengineering, 10(9), 1065. https://doi.org/10.3390/bioengineering10091065