
A Portable, Neurostimulation-Integrated, Force Measurement Platform for the Clinical Assessment of Plantarflexor Central Drive

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
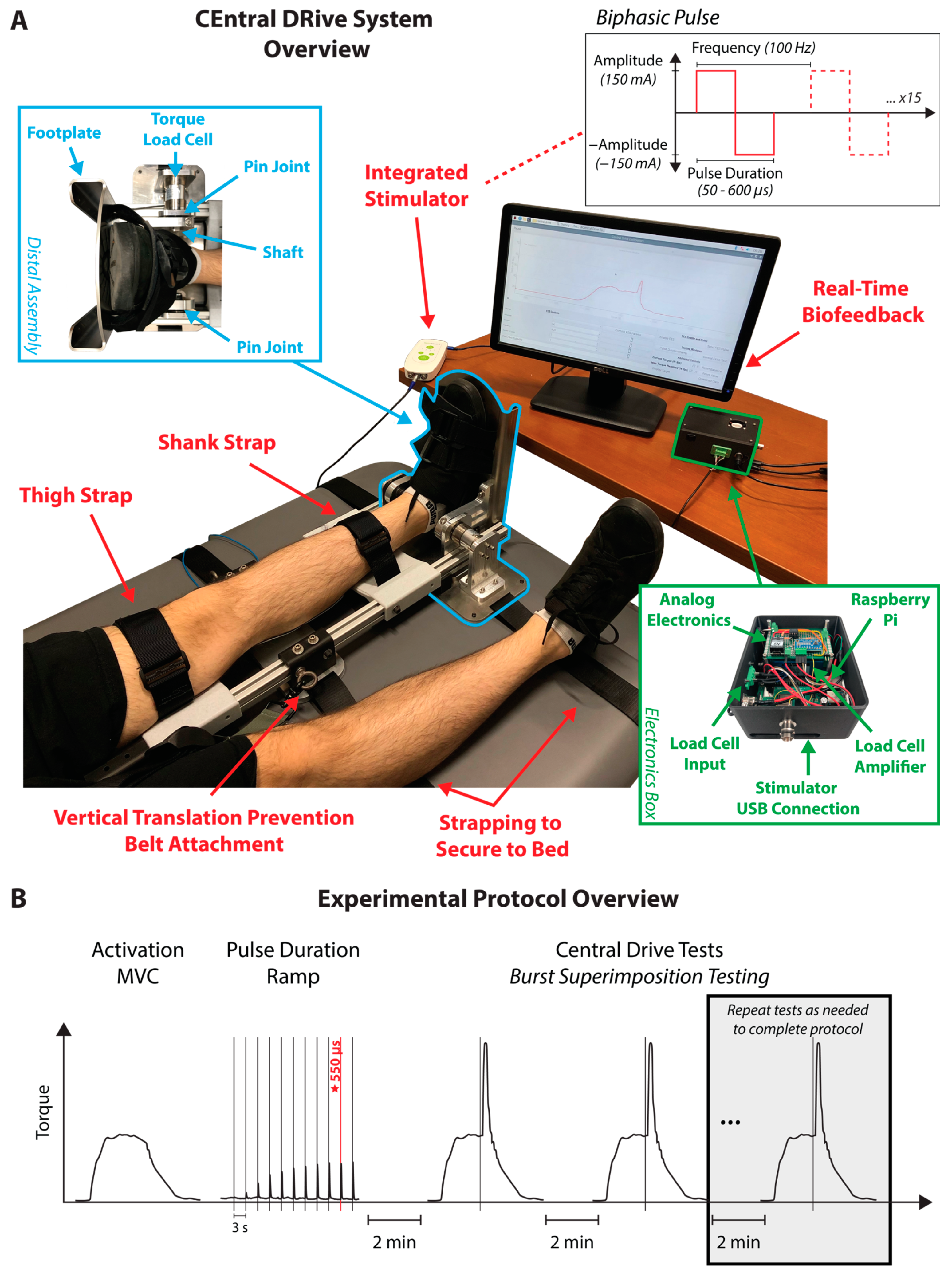
2.1. Device Development
2.1.1. Hardware
2.1.2. Software
2.1.3. Integrated Stimulator
2.2. Experiment #1: Device Accuracy and Adjustment Equation Development
2.2.1. Study Procedures
Participant Setup
Selecting Burst Parameters
Central Drive Testing
2.2.2. Data Processing
2.2.3. Statistical Analyses
2.3. Experiment #2: Post-Stroke Evaluation
2.3.1. Study Procedures
Central Drive Testing
Six-Minute Walk Test Procedures
2.3.2. Data Processing
2.3.3. Statistical Analyses
3. Results
3.1. Experiment #1: Device Accuracy and Adjustment Equation Development
3.1.1. Participants
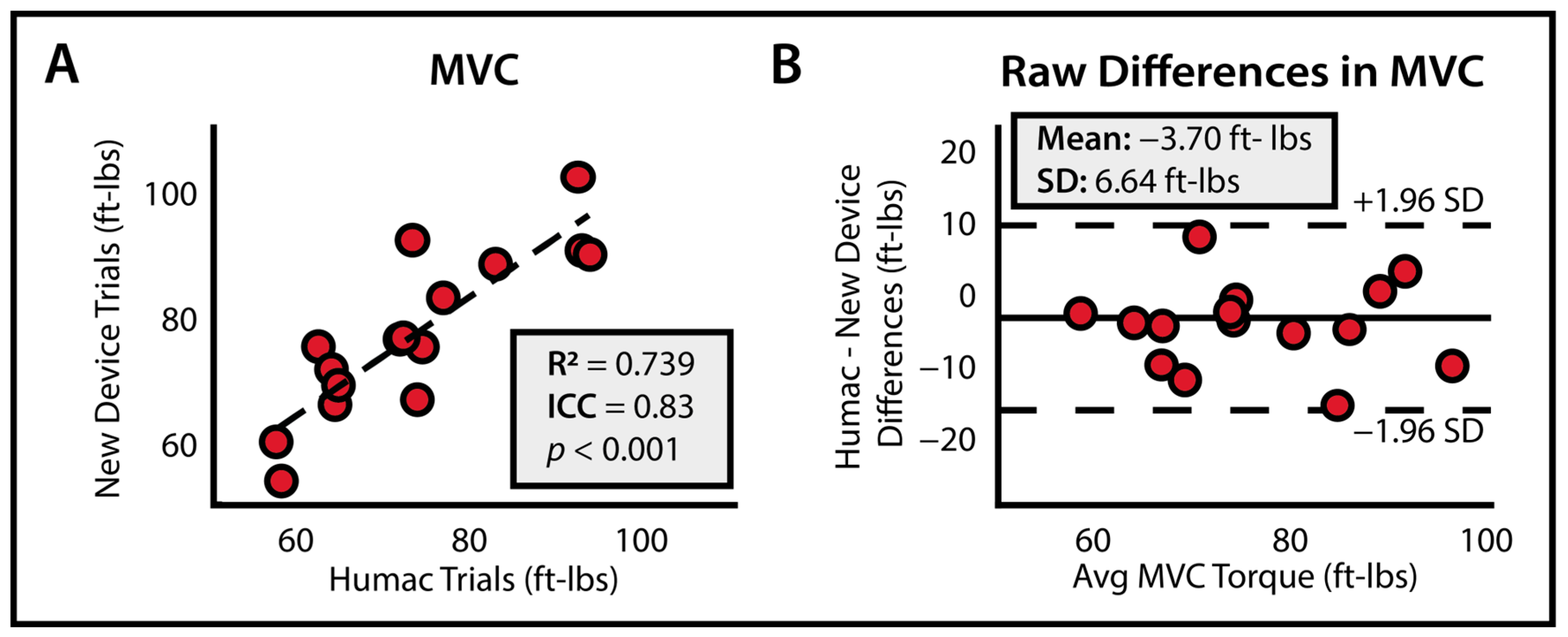
3.1.2. Accuracy of Force Measurement
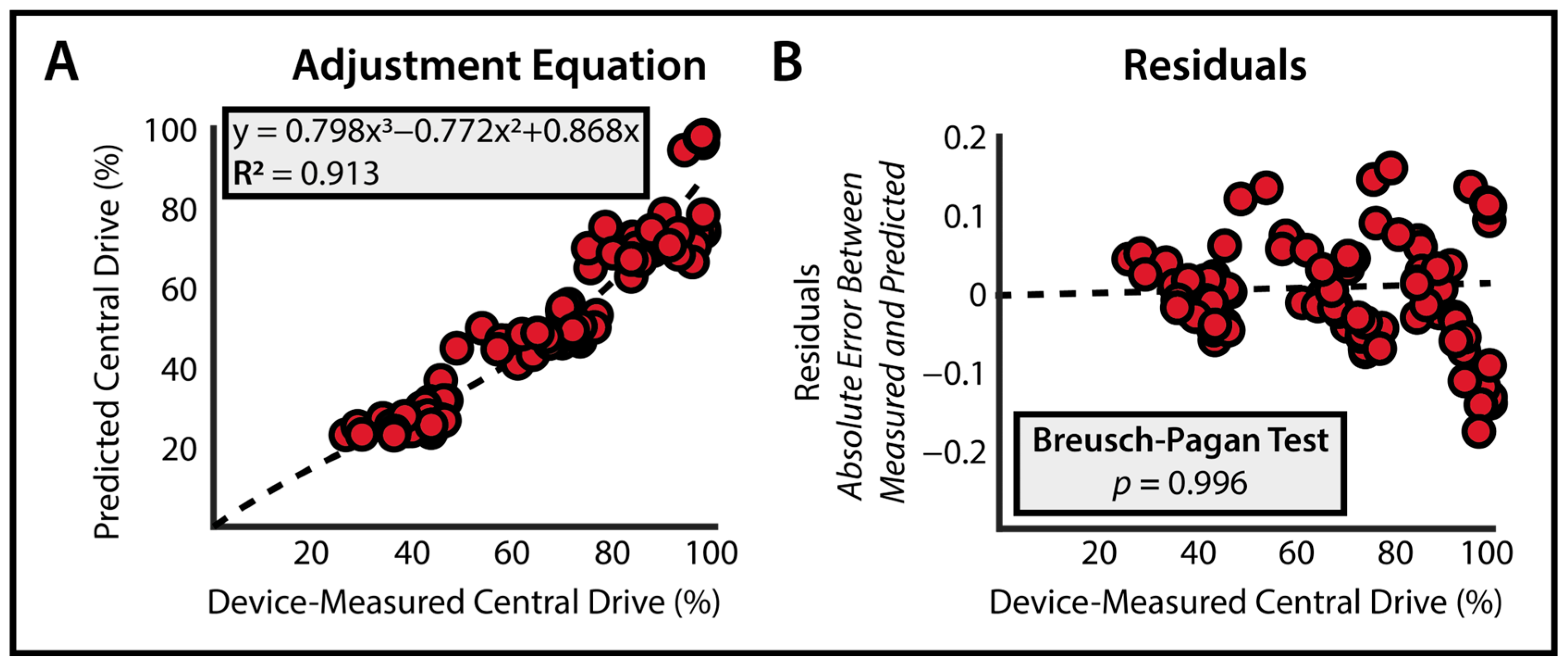
3.1.3. Development and Validation of Adjustment Equation
3.2. Experiment #2: Post-Stroke Evaluation
3.2.1. Participants
3.2.2. Feasibility of Using CEDRS Post-Stroke
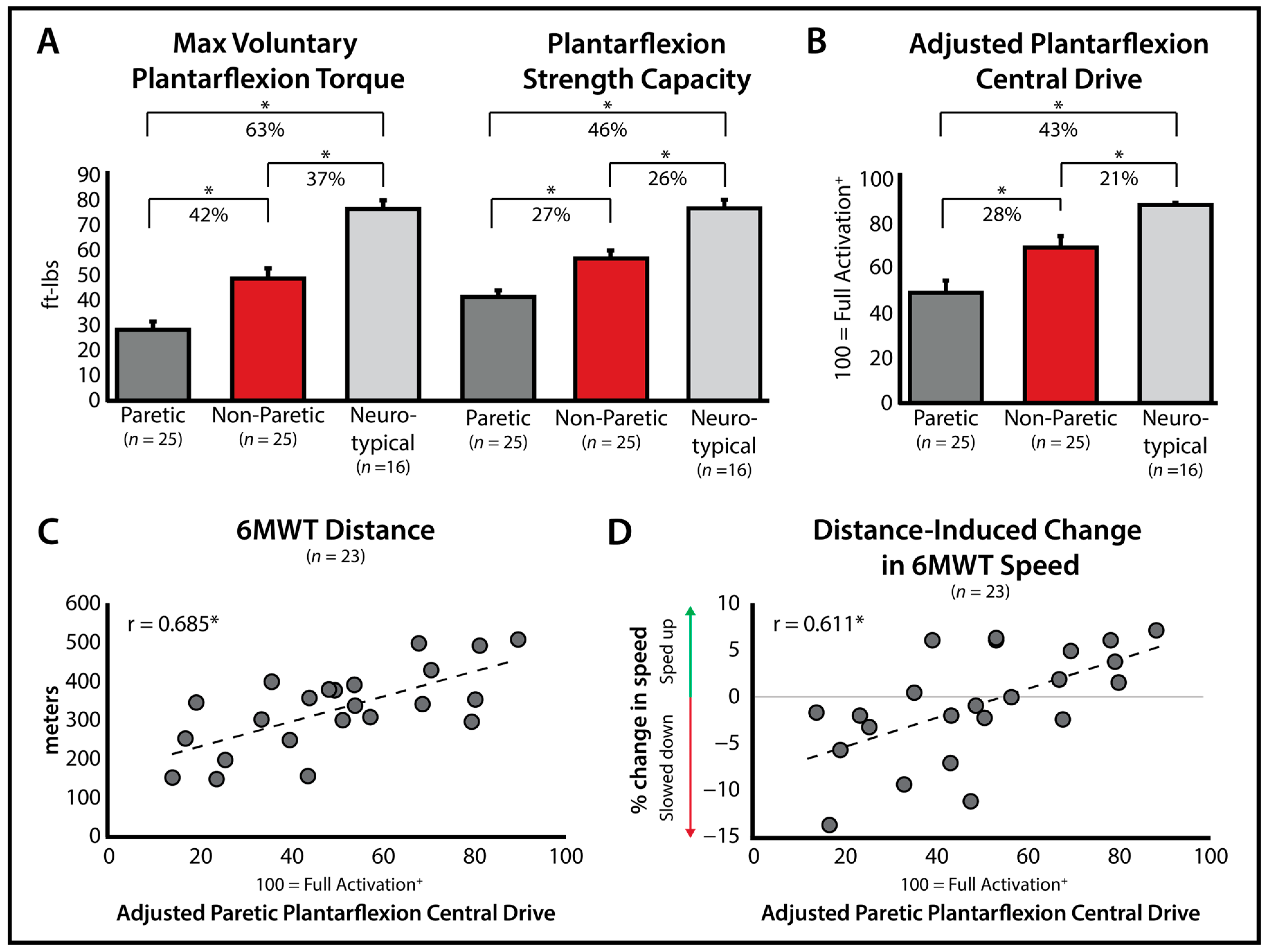
3.2.3. Evaluation of Deficits Post-Stroke
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zarkou, A.; Stackhouse, S.; Binder-Macleod, S.A.; Lee, S.C.K. Comparison of Techniques to Determine Human Skeletal Muscle Voluntary Activation. J. Electromyogr. Kinesiol. 2017, 36, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Shield, A.; Zhou, S. Assessing Voluntary Muscle Activation with the Twitch Interpolation Technique. Sports Med 2004, 34, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Fimland, M.S.; Moen, P.M.R.; Hill, T.; Gjellesvik, T.I.; Tørhaug, T.; Helgerud, J.; Hoff, J. Neuromuscular Performance of Paretic versus Non-Paretic Plantar Flexors after Stroke. Eur. J. Appl. Physiol. 2011, 111, 3041–3049. [Google Scholar] [CrossRef] [PubMed]
- Awad, L.N.; Hsiao, H.Y.; Binder-Macleod, S.A. Central Drive to the Paretic Ankle Plantarflexors Affects the Relationship Between Propulsion and Walking Speed after Stroke. J. Neurol. Phys. Ther. 2020, 44, 42–48. [Google Scholar] [CrossRef]
- Klein, C.S.; Brooks, D.; Richardson, D.; Mcilroy, W.E.; Bayley, M.T. Voluntary Activation Failure Contributes More to Plantar Flexor Weakness than Antagonist Coactivation and Muscle Atrophy in Chronic Stroke Survivors. J. Appl. Physiol. 2010, 109, 1337–1346. [Google Scholar] [CrossRef]
- Lepley, L.K.; Palmieri-Smith, R.M. Quadriceps Strength, Muscle Activation Failure, and Patient-Reported Function at the Time of Return to Activity in Patients Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study. J. Orthop. Sports Phys. Ther. 2015, 45, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, S.J.; Chmielewski, T.L.; Snyder-Mackler, L. Accuracy of Predicting Maximal Quadriceps Force from Submaximal Effort Contractions after Anterior Cruciate Ligament Injury. Muscle Nerve 2005, 32, 500–505. [Google Scholar] [CrossRef]
- Lisee, C.; Lepley, A.S.; Birchmeier, T.; O’Hagan, K.; Kuenze, C. Quadriceps Strength and Volitional Activation after Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. Sports Health 2019, 11, 163–179. [Google Scholar] [CrossRef]
- Rice, D.A.; McNair, P.J. Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives. Semin. Arthritis Rheum. 2010, 40, 250–266. [Google Scholar] [CrossRef]
- Djajadikarta, Z.J.; Dongés, S.C.; Brooks, J.; Kennedy, D.S.; Gandevia, S.C.; Taylor, J.L. Impaired Central Drive to Plantarflexors and Minimal Ankle Proprioceptive Deficit in People with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 46, 102584. [Google Scholar] [CrossRef]
- O’Brien, S.M.; Carroll, T.J.; Barber, L.A.; Lichtwark, G.A. Plantar Flexor Voluntary Activation Capacity, Strength and Function in Cerebral Palsy. Eur. J. Appl. Physiol. 2021, 121, 1733–1741. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich-Zwahlen, A.K.; Casartelli, N.C.; Item-Glatthorn, J.F.; Maffiuletti, N.A. Validity of Resting Myotonometric Assessment of Lower Extremity Muscles in Chronic Stroke Patients with Limited Hypertonia: A Preliminary Study. J. Electromyogr. Kinesiol. 2014, 24, 762–769. [Google Scholar] [CrossRef]
- Knarr, B.A.; Higginson, J.S.; Binder-Macleod, S.A. Validation of an Adjustment Equation for the Burst Superimposition Technique in Subjects Post-Stroke. Muscle Nerve 2012, 46, 267–269. [Google Scholar] [CrossRef]
- Martin, H.J.; Yule, V.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Aihie Sayer, A. Is Hand-Held Dynamometry Useful for the Measurement of Quadriceps Strength in Older People? A Comparison with the Gold Standard Biodex Dynamometry. Gerontology 2006, 52, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-Held Dynamometry Correlation with the Gold Standard Isokinetic Dynamometry: A Systematic Review. PM&R 2011, 3, 472–479. [Google Scholar]
- Marmon, A.R.; Pozzi, F.; Alnahdi, A.H.; Zeni, J.A. The Validity of Plantarflexor Strength Measures Obtained through Hand-Held Dynamometry Measurements of Force. Int. J. Sports Phys. Ther. 2013, 8, 820–827. [Google Scholar]
- Stackhouse, S.K.; Stevens, J.E.; Johnson, C.D.; Snyder-Mackler, L.; Binder-Macleod, S.A. Predictability of Maximum Voluntary Isometric Knee Extension Force from Submaximal Contractions in Older Adults. Muscle Nerve 2003, 27, 40–45. [Google Scholar] [CrossRef]
- Riverbank Computing Limited. PyQt5, Version 5.15.7. Available online: https://www.riverbankcomputing.com/static/Docs/PyQt5 (accessed on 10 January 2023).
- PyQtGraph Developers. PyQtGraph, Version 0.13.1. Available online: https://www.pyqtgraph.org/ (accessed on 10 January 2023).
- Zou, G.Y. Sample Size Formulas for Estimating Intraclass Correlation Coefficients with Precision and Assurance. Stat. Med. 2012, 31, 3972–3981. [Google Scholar] [CrossRef]
- Davis, P.R.; Mckay, M.J.; Baldwin, J.N.; Burns, J.; Pareyson, D.; Rose, K.J. Repeatability, Consistency, and Accuracy of Hand-Held Dynamometry with and without Fixation for Measuring Ankle Plantarflexion Strength in Healthy Adolescents and Adults. Muscle Nerve 2017, 56, 896–900. [Google Scholar] [CrossRef]
- Moraux, A.; Canal, A.; Ollivier, G.; Ledoux, I.; Doppler, V.; Payan, C.; Hogrel, J.Y. Ankle Dorsi- and Plantar-Flexion Torques Measured by Dynamometry in Healthy Subjects from 5 to 80 Years. BMC Musculoskelet. Disord. 2013, 14, 104. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef]
- Trappe, S.; Costill, D.; Gallagher, P.; Creer, A.; Peters, J.R.; Evans, H.; Riley, D.A.; Fitts, R.H. Exercise in Space: Human Skeletal Muscle after 6 Months Aboard the International Space Station. J. Appl. Physiol. 2009, 106, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Hornby, T.G.; Reisman, D.S.; Ward, I.G.; Scheets, P.L.; Miller, A.; Haddad, D.; Fox, E.J.; Fritz, N.E.; Hawkins, K.; Henderson, C.E.; et al. Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury. J. Neurol. Phys. Ther. 2020, 44, 49–100. [Google Scholar] [CrossRef]
- Awad, L.N.; Reisman, D.S.; Binder-Macleod, S.A. Distance-Induced Changes in Walking Speed after Stroke: Relationship to Community Walking Activity. J. Neurol. Phys. Ther. 2019, 43, 220–223. [Google Scholar] [CrossRef]
- Todd, G.; Gorman, R.B.; Gandevia, S.C. Measurement and Reproducibility of Strength and Voluntary Activation of Lower-Limb Muscles. Muscle Nerve 2004, 29, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Rozand, V.; Sundberg, C.W.; Hunter, S.K.; Smith, A.E. Age-Related Deficits in Voluntary Activation: A Systematic Review and Meta-Analysis. Med. Sci. Sports Exerc. 2020, 52, 549–560. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neurotypical | Paretic | Non-Paretic | Significance | |
|---|---|---|---|---|
| Fvol (ft-lbs.) | 76.21 ± 13.84 | 27.99 ± 14.15 | 48.25 ± 18.75 | p < 0.001 *,+,# |
| MFGA (ft-lbs.) | 76.47 ± 13.59 | 41.07 ± 13.41 | 56.54 ± 15.71 | p < 0.001 *,+,# |
| Central Drive | 88.73% ± 1.71% | 50.39% ± 21.44% | 70.12% ± 20.25% | p < 0.001 *,+,# |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collimore, A.N.; Alvarez, J.T.; Sherman, D.A.; Gerez, L.F.; Barrow, N.; Choe, D.K.; Binder-Macleod, S.; Walsh, C.J.; Awad, L.N. A Portable, Neurostimulation-Integrated, Force Measurement Platform for the Clinical Assessment of Plantarflexor Central Drive. Bioengineering 2024, 11, 137. https://doi.org/10.3390/bioengineering11020137
Collimore AN, Alvarez JT, Sherman DA, Gerez LF, Barrow N, Choe DK, Binder-Macleod S, Walsh CJ, Awad LN. A Portable, Neurostimulation-Integrated, Force Measurement Platform for the Clinical Assessment of Plantarflexor Central Drive. Bioengineering. 2024; 11(2):137. https://doi.org/10.3390/bioengineering11020137
Chicago/Turabian StyleCollimore, Ashley N., Jonathan T. Alvarez, David A. Sherman, Lucas F. Gerez, Noah Barrow, Dabin K. Choe, Stuart Binder-Macleod, Conor J. Walsh, and Louis N. Awad. 2024. "A Portable, Neurostimulation-Integrated, Force Measurement Platform for the Clinical Assessment of Plantarflexor Central Drive" Bioengineering 11, no. 2: 137. https://doi.org/10.3390/bioengineering11020137
APA StyleCollimore, A. N., Alvarez, J. T., Sherman, D. A., Gerez, L. F., Barrow, N., Choe, D. K., Binder-Macleod, S., Walsh, C. J., & Awad, L. N. (2024). A Portable, Neurostimulation-Integrated, Force Measurement Platform for the Clinical Assessment of Plantarflexor Central Drive. Bioengineering, 11(2), 137. https://doi.org/10.3390/bioengineering11020137