
Biochemical Analysis of Urine Samples from Diabetic and Hypertensive Patients without Renal Dysfunction Using Spectrophotometry and Raman Spectroscopy Techniques Aiming Classification and Diagnosis

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Urine Sample Collection and Biochemical Chemometric Assay
2.2. Raman Spectroscopy
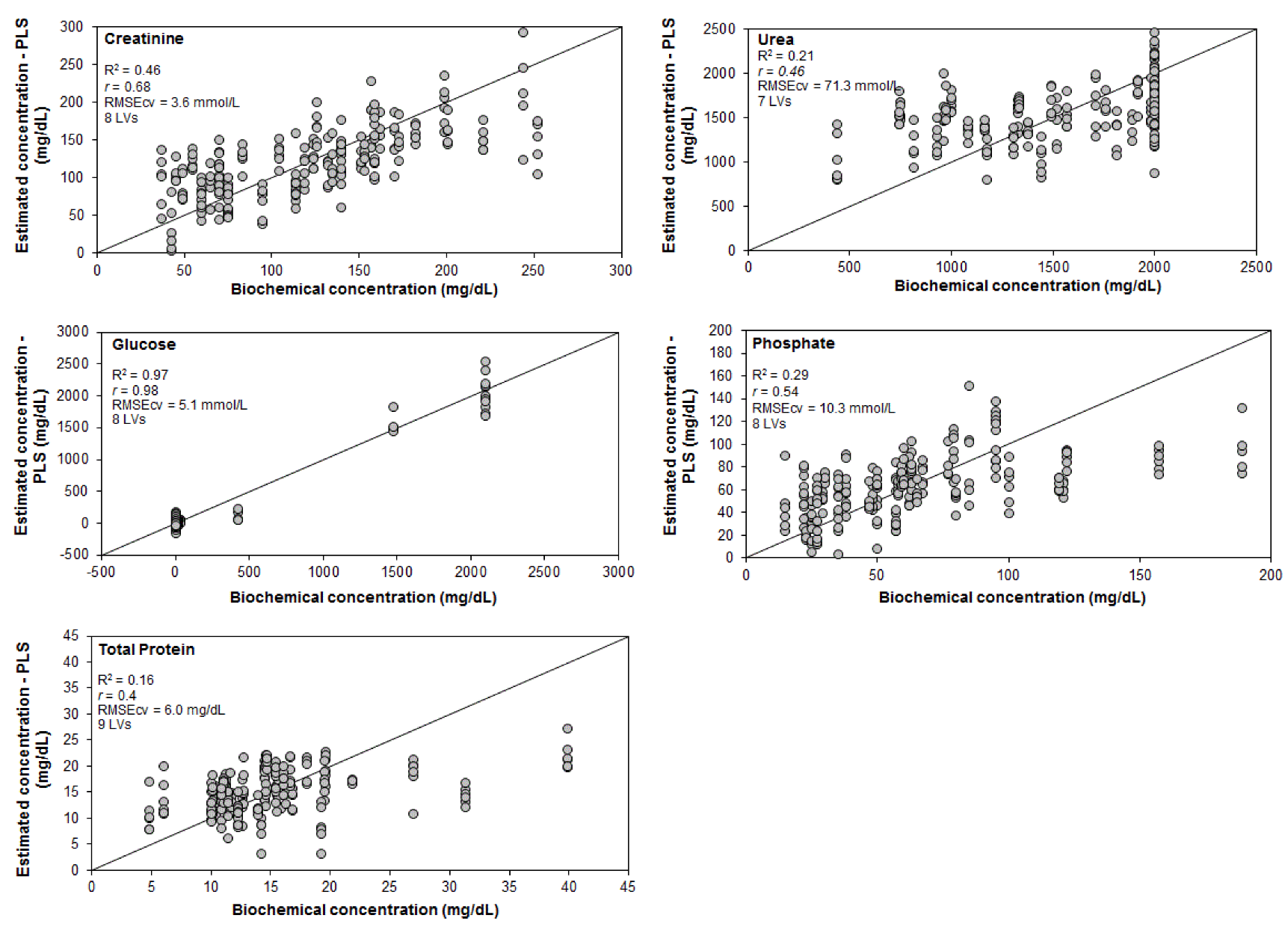
2.3. Data Processing and Analysis—Exploratory Analysis and Linear Regression Models for Quantification and Discrimination
3. Results and Discussion
3.1. Raman Spectra

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Urinary Biomarker | Reference Values | CT Mean Concentration ± SD | CT Total Amount of Samples/No. of Samples Above RVs | DM&HBP Mean Concentration ± SD | DM&HBP Total Amount of Samples/No. of Samples Above RVs |
|---|---|---|---|---|---|
| Urea | 51.6–549 mmol/L (M) 46.9–580 mmol/L (W) | 271 ± 89 mmol/L | 20/0 | 249 ± 68 mmol/L | 20/0 |
| Creatinine | 2.12–34.6 mmol/L (M) 1.4–28.9 mmol/L (W) | 12.5 ± 5.5 mmol/L | 20/0 | 9.3 ± 4.0 mmol/L | 20/0 |
| Glucose | <0.83 mmol/L | 0.23 ± 0.04 mmol/L | 20/0 | 17.3 ± 38.7 mmol/L | 20/5 |
| Phosphate | 1.6–61 mmol/L (M) 2.3–48 mmol/L (W) | 23.4 ± 14.1 | 20/0 | 17.2 ± 9.9 | 20/0 |
| Total protein | 1–15 mg/dL | 14.7 ± 5.5 mg/dL | 20/9 | 15.6 ± 7.2 mg/dL | 20/7 |
3.2. Exploratory Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ridley, J. Fundamentals of the study of urine and body fluids. In Introduction to the Study of Body Fluids; Ridley, J.W., Ed.; Springer: Cham, Switzerland, 2018; pp. 1–7. [Google Scholar]
- Chirizzi, D.; Malitesta, C. Potentiometric urea biosensor based on urease immobilized by an electrosynthesizedpoly(o-phenylenediamine) film with buffering capability. Sens. Actuators B Chem. 2011, 157, 211–215. [Google Scholar] [CrossRef]
- Wang, H.; Malvadkar, N.; Koytek, S.; Bylander, J.; Reeves, W.B.; Demirel, M.C. Quantitative analysis of creatinine in urine by metalized nanostructured parylene. J. Biomed. Opt. 2010, 15, 027004. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.A.; Eyff, T.F.; Campani, R.B.; Ritter, L.; Camargo, J.L.; Silveiro, S.P. Glomerular filtration rate measurement and prediction equations. Clin. Chem. Lab. Med. 2009, 47, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Montero, R.M.; Covic, A.; Gnudi, L.; Goldsmith, D. Diabetic nephropathy: What does the future hold? Int. Urol. Nephrol. 2016, 48, 99–113. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Chronic Kidney Disease Surveillance System Website. Available online: https://nccd.cdc.gov/CKD (accessed on 30 June 2022).
- Bruen, D.; Delaney, C.; Floresa, L.; Diamond, D. Glucose sensing for diabetes monitoring: Recent developments. Sensors 2017, 17, 1866. [Google Scholar] [CrossRef] [PubMed]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, hypertension, and cardiovascular disease: Clinical insights and vascular mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef]
- Oparil, S.; Acelajado, M.C.; Bakris, G.L.; Berlowitz, D.R.; Cífková, R.; Dominiczak, A.F.; Grassi, G.; Jordan, J.; Poulter, N.R.; Rodgers, A.; et al. Hypertension. Nat. Rev. Dis. Primers 2018, 4, 18014. [Google Scholar] [CrossRef]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Li, J.; Zhang, Y.; Ma, W.; Fan, F.; Wang, B.; Xing, H.; Tang, G.; Wang, X.; Xu, X.; et al. Prevalence and associated factors of diabetes and impaired fasting glucose in Chinese hypertensive adults aged 45 to 75 years. PLoS ONE 2012, 7, e42538. [Google Scholar] [CrossRef] [PubMed]
- Giansante, S.; Giana, H.E.; Fernandes, A.B.; Silveira, L. Analytical performance of Raman spectroscopy in assaying biochemical components in human serum. Lasers Med. Sci. 2022, 37, 287–298. [Google Scholar] [CrossRef]
- Eberhardt, K.; Stiebing, C.; Matthäus, C.; Schmitt, M.; Popp, J. Advantages and limitations of Raman spectroscopy for molecular diagnostics: An update. Expert Rev. Mol. Diagn. 2015, 15, 773–787. [Google Scholar] [CrossRef]
- Guleken, Z.; Bulut, H.; Bulut, B.; Paja, W.; Parlinska-Wojtan, M.; Depciuch, J. Correlation between endometriomas volume and Raman spectra. Attempting to use Raman spectroscopy in the diagnosis of endometrioma. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2022, 274, 121119. [Google Scholar] [CrossRef] [PubMed]
- Huefner, A.; Kuan, W.; Mason, S.L.; Mahajan, S.; Barker, R.A. Serum Raman spectroscopy as a diagnostic tool in patients with Huntington’s disease. Chem. Sci. 2020, 11, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Goulart, A.C.C.; Silveira, L., Jr.; Carvalho, H.C.; Dorta, C.B.; Pacheco, M.T.T.; Zângaro, R.A. Diagnosing COVID-19 in human serum using Raman spectroscopy. Lasers Med. Sci. 2022, 37, 2217–2226. [Google Scholar] [CrossRef] [PubMed]
- Staritzbichler, R.; Hunold, P.; Estrela-Lopis, I.; Hildebrand, P.W.; Isermann, B.; Kaiser, T. Raman spectroscopy on blood serum samples of patients with end-stage liver disease. PLoS ONE 2021, 16, e0256045. [Google Scholar] [CrossRef] [PubMed]
- De Souza Vieira, E.E.; Bispo, J.A.M.; Silveira, L.; Fernandes, A.B. Discrimination model applied to urinalysis of patients with diabetes and hypertension aiming at diagnosis of chronic kidney disease by Raman spectroscopy. Lasers Med. Sci. 2017, 32, 1605–1613. [Google Scholar] [CrossRef]
- Bispo, J.A.M.; Vieira, E.E.S.; Silveira, L.; Fernandes, A.B. Correlating the amount of urea, creatinine, and glucose in urine from patients with diabetes mellitus and hypertension with the risk of developing renal lesions by means of Raman spectroscopy and principal component analysis. J. Biomed. Opt. 2013, 18, 087004. [Google Scholar] [CrossRef] [PubMed]
- McMurdy, J.W.; Berger, A.J. Raman spectroscopy-based creatinine measurement in urine samples from a multipatient population. Appl. Spectrosc. 2003, 57, 522–525. [Google Scholar] [CrossRef]
- Saatkamp, C.J.; De Almeida, M.L.; Bispo, J.A.M.; Pinheiro, A.L.B.; Fernandes, A.B.; Silveira, L., Jr. Quantifying creatinine and urea in human urine through Raman spectroscopy aiming at diagnosis of kidney disease. J. Biomed. Opt. 2016, 21, 037001. [Google Scholar] [CrossRef] [PubMed]
- Moreira, L.P.; Rocco, D.D.F.M.; da Silva, A.G.; Pacheco, M.T.T.; Silveira, L. Detecting creatine excreted in the urine of swimming athletes by means of Raman spectroscopy. Lasers Med. Sci. 2020, 35, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Žukovskaja, O.; Ryabchykov, O.; Straßburger, M.; Heinekamp, T.; Brakhage, A.A.; Hennings, C.J.; Hübner, C.A.; Wegmann, M.; Cialla-May, D.; Bocklitz, T.W.; et al. Towards Raman spectroscopy of urine as screening tool. J. Biophotonics 2020, 13, e201900143. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Xu, X.; Zhao, Z.; Li, C.; Tian, Y.; Liu, Q.; Shao, B.; Chen, S.; Zhao, Y.; Li, L.; et al. Detecting urine metabolites of bladder cancer by surface-enhanced Raman spectroscopy. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 247, 119108. [Google Scholar] [CrossRef]
- Peppers, M.P.; Geheb, M.; Desai, T. Hypophosphatemia and hyperphosphatemia. Crit. Care Clin. 1991, 7, 201–214. [Google Scholar] [CrossRef]
- Foley, R.N. Phosphate levels and cardiovascular disease in the general population. Clin. J. Am. Soc. Nephrol. 2009, 4, 1136–1139. [Google Scholar] [CrossRef]
- CLSI. Interference Testing in Clinical Chemistry, 2nd ed.; Approved Guideline; 25. CLSI Document; EP07-A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2005. [Google Scholar]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Beattie, J.R.; Esmonde-White, F.W.L. Exploration of principal component analysis: Deriving principal component analysis visually using spectra. Appl. Spectrosc. 2021, 75, 361–375. [Google Scholar] [CrossRef]
- Baratloo, A.; Hosseini, M.; Negida, A.; El Ashal, G. Part 1: Simple definition and calculation of accuracy, sensitivity and specificity. Emergency 2015, 3, 48–49. [Google Scholar]
- Nunes, C.A.; Freitas, M.P.; Pinheiro, A.C.M.; Bastos, S.C. Chemoface: A novel free user-friendly interface for chemometrics. J. Braz. Chem. Soc. 2012, 23, 2003–2010. [Google Scholar] [CrossRef]
- Flores-Guerrero, J.L.; Muñoz-Morales, A.; Narea-Jimenez, F.; Perez-Fuentes, R.; Torres-Rasgado, E.; Ruiz-Vivanco, G.; Gonzalez-Viveros, N.; Castro-Ramos, J. Novel assessment of urinary albumin excretion in type 2 diabetes patients by Raman spectroscopy. Diagnostics 2020, 10, 141. [Google Scholar] [CrossRef]
- Aitekenov, S.; Gaipov, A.; Bukasov, R. Review: Detection and quantification of proteins in human urine. Talanta 2021, 223 Pt 1, 121718. [Google Scholar] [CrossRef]
- Wu, A.H.B. Tietz Clinical Guide to Laboratory Tests; Elsevier: San Francisco, CA, USA, 2006. [Google Scholar]
- Söderholm, S.; Roos, Y.H.; Meinander, N.; Hotokka, M. Raman spectra of fructose and glucose in the amorphous and crystalline states. J. Raman Spectrosc. 1999, 30, 1009–1018. [Google Scholar] [CrossRef]
- Frost, R.L.; Kristof, J.; Rintoul, L.; Kloprogge, J.T. Raman spectroscopy of urea and urea-intercalated kaolinites at 77 K. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2000, 56, 1681–1691. [Google Scholar] [CrossRef]
- Li, M.; Du, Y.; Zhao, F.; Zeng, J.; Mohan, C.; Shih, W.C. Reagent- and separation-free measurements of urine creatinine concentration using stamping surface enhanced Raman scattering (S-SERS). Biomed. Opt. Express 2015, 6, 849–858. [Google Scholar] [CrossRef]
- Senger, R.S.; Kavuru, V.; Sullivan, M.; Gouldin, A.; Lundgren, S.; Merrifield, K.; Steen, C.; Baker, E.; Vu, T.; Agnor, B.; et al. Spectral characteristics of urine specimens from healthy human volunteers analyzed using Raman chemometric urinalysis (Rametrix). PLoS ONE 2019, 14, e0222115. [Google Scholar] [CrossRef]
- Zhu, W.; Wen, B.; Jie, L.; Tian, X.D.; Yang, Z.L.; Radjenovic, P.M.; Luo, S.Y.; Tian, Z.Q.; Li, J.F. Rapid and low-cost quantitative detection of creatinine in human urine with a portable Raman spectrometer. Biosens. Bioelectron. 2020, 154, 112067. [Google Scholar] [CrossRef]
- Herman, W.H.; Ye, W.; Griffin, S.J.; Simmons, R.K.; Davies, M.J.; Khunti, K.; Rutten, G.E.; Sandbaek, A.; Lauritzen, T.; Borch-Johnsen, K.; et al. Early detection and treatment of type 2 diabetes reduce cardiovascular morbidity and mortality: A simulation of the results of the Anglo-Danish-Dutch study of intensive treatment in people with screen-detected diabetes in primary care (ADDITION-Europe). Diabetes Care 2015, 38, 1449–1455. [Google Scholar] [CrossRef]
- Carswell, W.; Robertson, J.L.; Senger, R.S. Raman spectroscopic detection and quantification of macro- and microhematuria in human urine. Appl. Spectrosc. 2022, 76, 273–283. [Google Scholar] [CrossRef]




| Classification According to the Clinical Criteria | Classification Using Spectrophotometric Analysis | |
|---|---|---|
| Control | DM&HBP | |
| Control (n = 20) | 13 | 7 |
| DM&HBP (n = 20) | 9 | 11 |
| Sensitivity | 55.0% | |
| Specificity | 65.0% | |
| Accuracy | 60.0% | |
| Classification According to the Clinical Criteria | Classification Using the Concentration Values Predicted by PLS | |
| Control | DM&HBP | |
| Control (n = 113) | 85 | 28 |
| DM&HBP (n = 119) | 42 | 77 |
| Sensitivity | 64.7% | |
| Specificity | 75.2% | |
| Accuracy | 69.8% | |
| Classification According to the Clinical Criteria | Classification Using Raman Spectra by PLS (7 LVs) | |
| Control | DM&HBP | |
| Control (n = 113) | 92 | 21 |
| DM&HBP (n = 119) | 22 | 97 |
| Sensitivity | 81.5% | |
| Specificity | 81.4% | |
| Accuracy | 81.5% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Sousa Vieira, E.E.; Silveira, L., Jr.; Carvalho, H.C.; Bispo, J.A.M.; Fernandes, F.B.; Fernandes, A.B. Biochemical Analysis of Urine Samples from Diabetic and Hypertensive Patients without Renal Dysfunction Using Spectrophotometry and Raman Spectroscopy Techniques Aiming Classification and Diagnosis. Bioengineering 2022, 9, 500. https://doi.org/10.3390/bioengineering9100500
de Sousa Vieira EE, Silveira L Jr., Carvalho HC, Bispo JAM, Fernandes FB, Fernandes AB. Biochemical Analysis of Urine Samples from Diabetic and Hypertensive Patients without Renal Dysfunction Using Spectrophotometry and Raman Spectroscopy Techniques Aiming Classification and Diagnosis. Bioengineering. 2022; 9(10):500. https://doi.org/10.3390/bioengineering9100500
Chicago/Turabian Stylede Sousa Vieira, Elzo Everton, Landulfo Silveira, Jr., Henrique Cunha Carvalho, Jeyse Aliana Martins Bispo, Fernanda Barrinha Fernandes, and Adriana Barrinha Fernandes. 2022. "Biochemical Analysis of Urine Samples from Diabetic and Hypertensive Patients without Renal Dysfunction Using Spectrophotometry and Raman Spectroscopy Techniques Aiming Classification and Diagnosis" Bioengineering 9, no. 10: 500. https://doi.org/10.3390/bioengineering9100500
APA Stylede Sousa Vieira, E. E., Silveira, L., Jr., Carvalho, H. C., Bispo, J. A. M., Fernandes, F. B., & Fernandes, A. B. (2022). Biochemical Analysis of Urine Samples from Diabetic and Hypertensive Patients without Renal Dysfunction Using Spectrophotometry and Raman Spectroscopy Techniques Aiming Classification and Diagnosis. Bioengineering, 9(10), 500. https://doi.org/10.3390/bioengineering9100500