
Automatic Identification of Failure in Hip Replacement: An Artificial Intelligence Approach

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Model Development
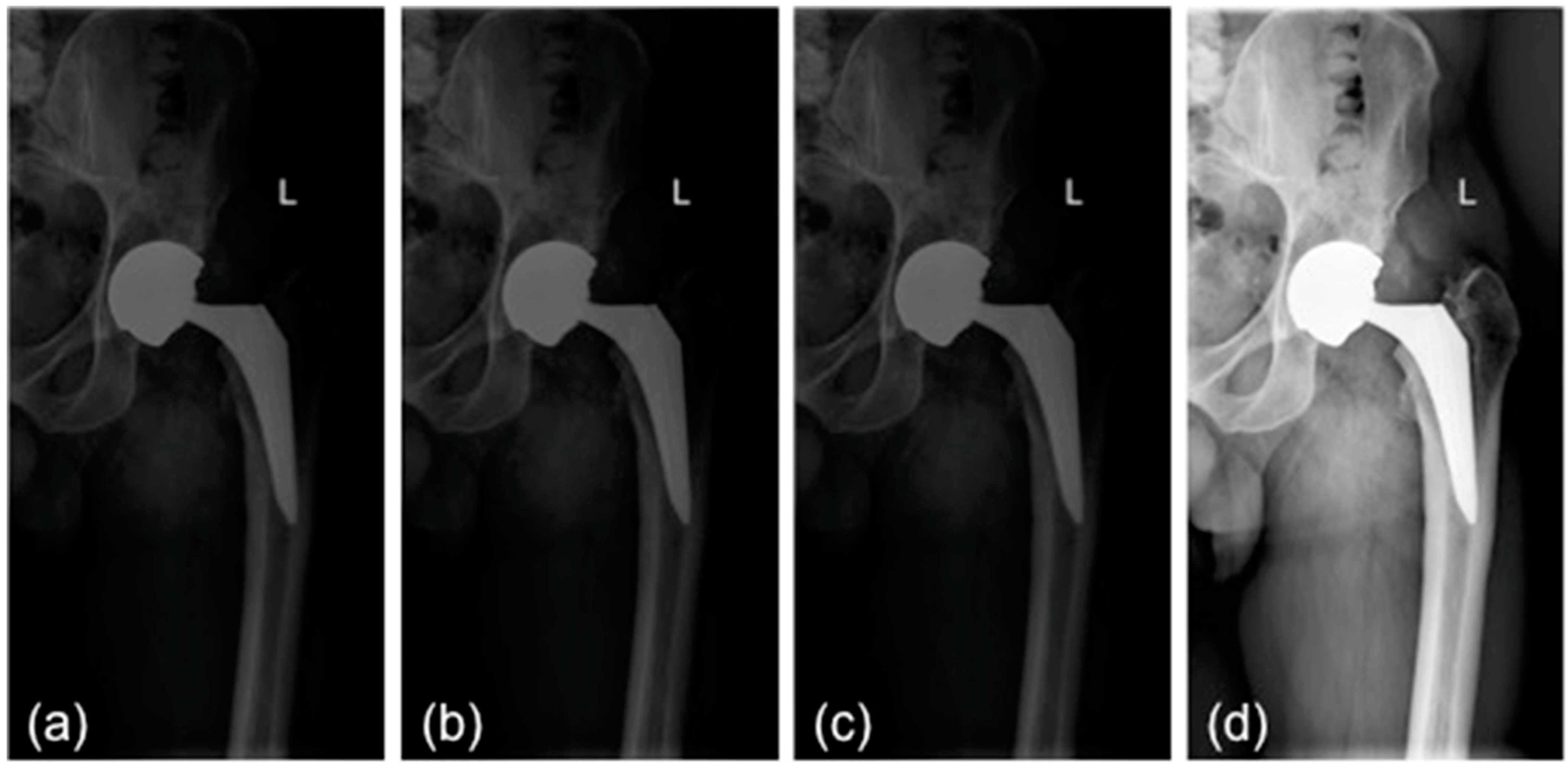
2.2.1. Preprocessing
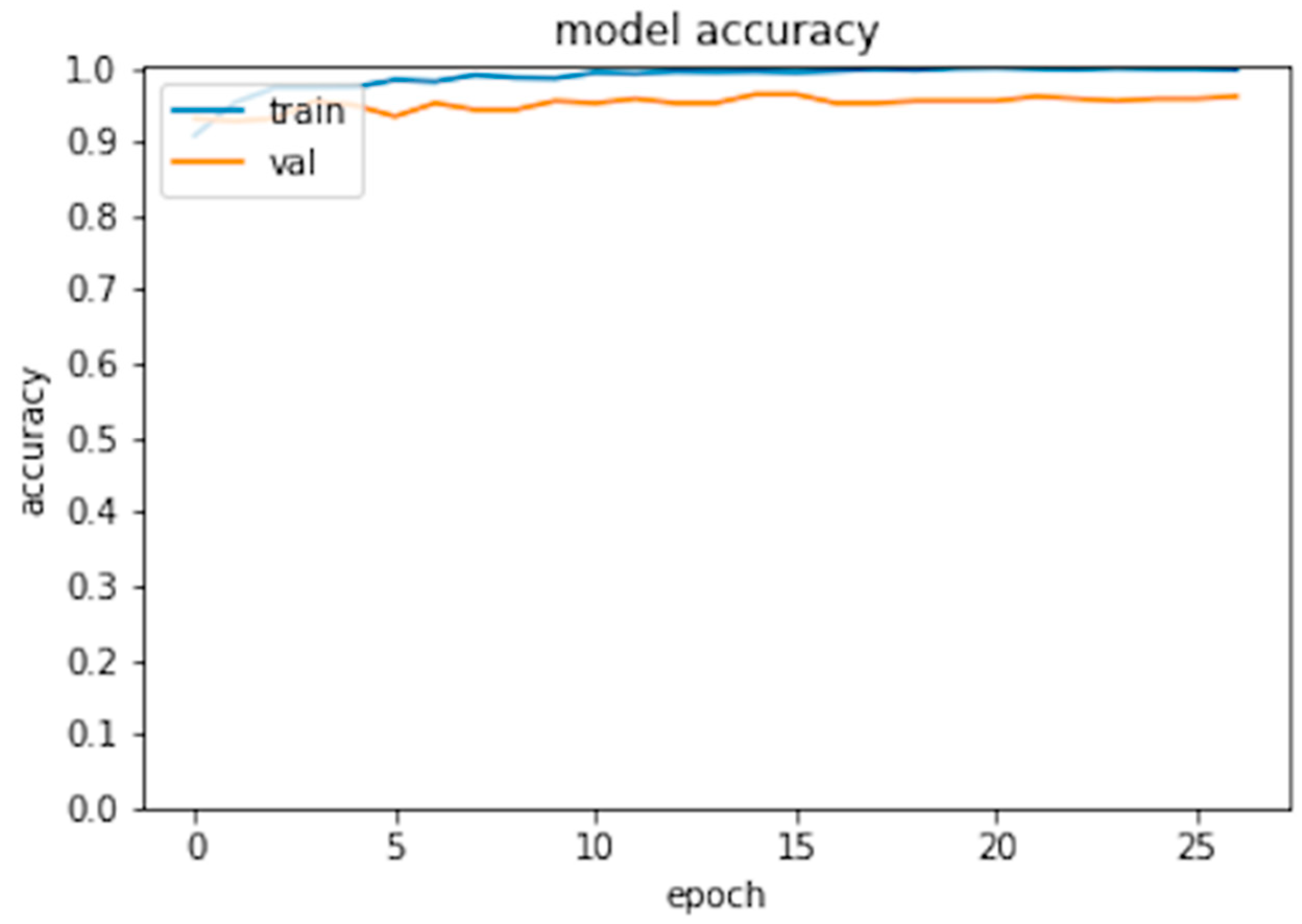
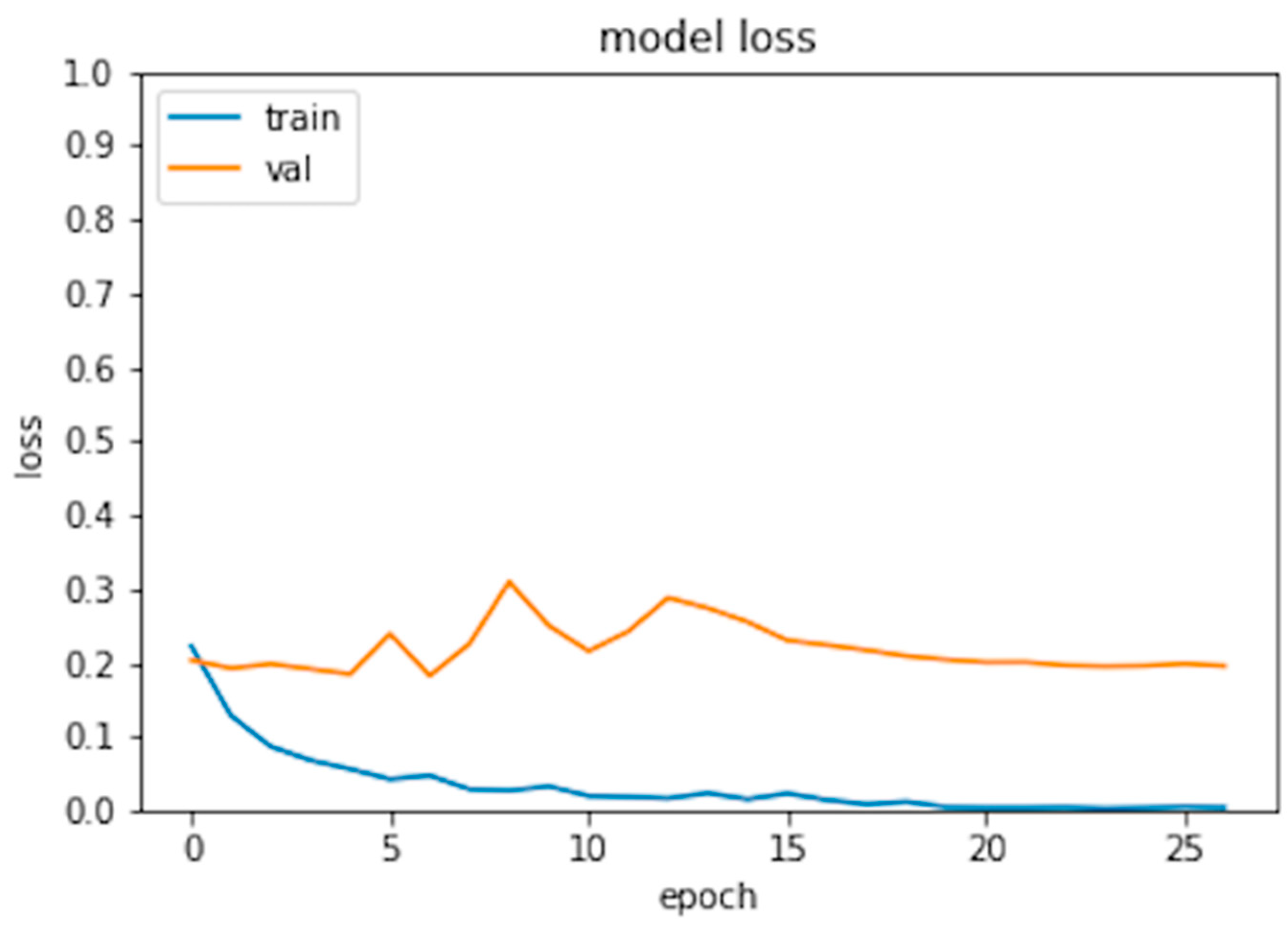
2.2.2. CNN Training
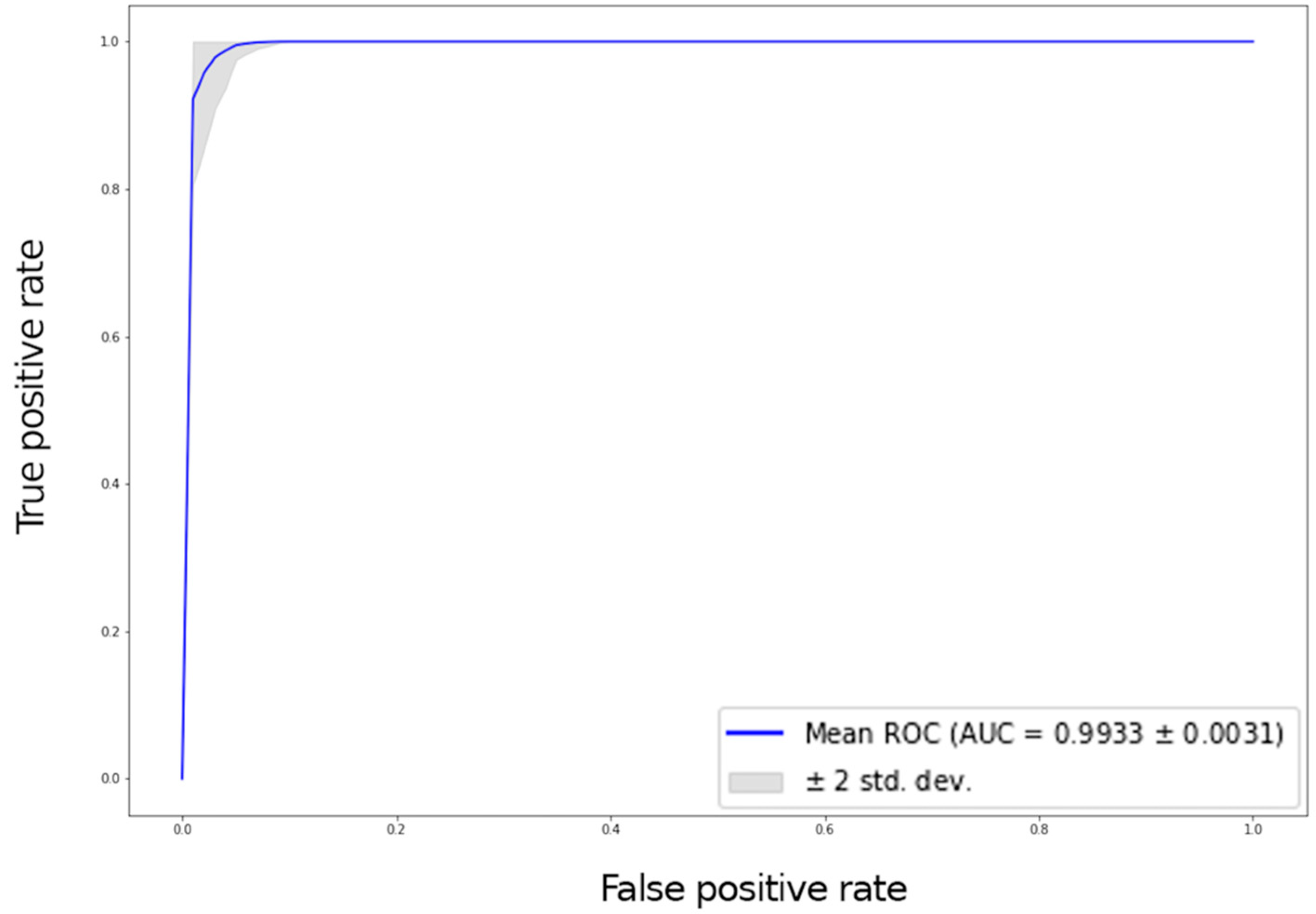
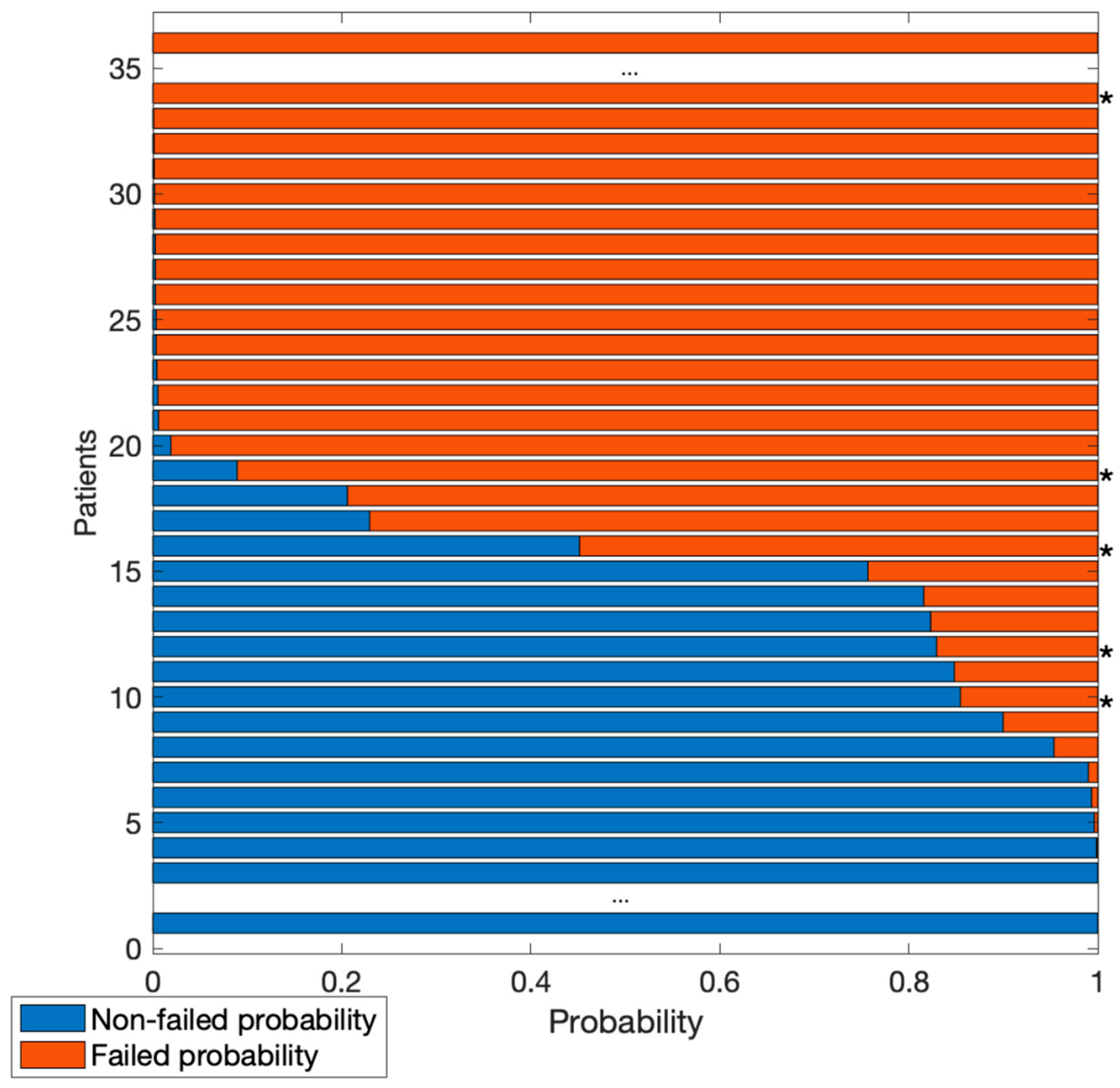
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Registro Italiano ArtroProtesi. Report Annuale 2018; Registro Italiano ArtroProtesi: Rome, Italy, 2018. [Google Scholar]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The Epidemiology of Revision Total Hip Arthroplasty in the United States. J. Bone Jt. Surg. Am. 2009, 91, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Oh, S.-H.; Kim, J.-S. Primary Total Hip Arthroplasty with a Second-Generation Cementless Total Hip Prosthesis in Patients Younger than Fifty Years of Age. J. Bone Jt. Surg. Am. 2003, 85, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.A.; Kidziński, Ł.; Halilaj, E.; Fleming, S.L.; Venkataraman, G.R.; Oei, E.H.G.; Gold, G.E.; Delp, S.L. Automated Classification of Radiographic Knee Osteoarthritis Severity Using Deep Neural Networks. Radiol. Artif. Intell. 2020, 2, e190065. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLOS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.-L.; Lin, T.; Liu, A.; Shi, M.-M.; Hu, B.; Shi, Z.; Yan, S.-G. Does Hydroxyapatite Coating Have No Advantage over Porous Coating in Primary Total Hip Arthroplasty? A Meta-Analysis. J. Orthop. Surg. Res. 2015, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigdorchik, J.M.; Sharma, A.K.; Madurawe, C.S.; Elbuluk, A.M.; Baré, J.V.; Pierrepont, J.W. Does Prosthetic or Bony Impingement Occur More Often in Total Hip Arthroplasty: A Dynamic Preoperative Analysis. J. Arthroplast. 2020, 35, 2501–2506. [Google Scholar] [CrossRef]
- Reito, A.; Lainiala, O.; Elo, P.; Eskelinen, A. Prevalence of Failure Due to Adverse Reaction to Metal Debris in Modern, Medium and Large Diameter Metal-on-Metal Hip Replacements—The Effect of Novel Screening Methods: Systematic Review and Metaregression Analysis. PLoS ONE 2016, 11, e0147872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.; Zhu, Q.; Yu, S.; Li, Q.; Xie, Y. Multiscale X-Ray Image Contrast Enhancement Based on Limited Adaptive Histogram Equalization. In Proceedings of the Fifth International Conference on Internet Multimedia Computing and Service, Huangshan, China, 17–18 August 2013; Association for Computing Machinery: New York, NY, USA, 2013; pp. 231–236. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. arXiv 2015, arXiv:1409.0575. [Google Scholar] [CrossRef] [Green Version]
- Marcelino, P. Transfer Learning from Pre-Trained Models. Available online: https://towardsdatascience.com/transfer-learning-from-pre-trained-models-f2393f124751 (accessed on 8 April 2022).
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef] [Green Version]
- Kärrholm, J. Roentgen Stereophotogrammetry. Review of Orthopedic Applications. Acta Orthop. Scand. 1989, 60, 491–503. [Google Scholar] [CrossRef]
- Selvik, G. Roentgen Stereophotogrammetry. A Method for the Study of the Kinematics of the Skeletal System. Acta Orthop. Scand. 1989, 60 (Suppl. S232), 1–51. [Google Scholar] [CrossRef]
- Syu, C.-B.; Lai, J.-Y.; Chang, R.-Y.; Shih, K.-S.; Chen, K.-J.; Lin, S.-C. Automatic Model-Based Roentgen Stereophotogrammetric Analysis (RSA) of Total Knee Prostheses. J. Biomech. 2012, 45, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Krismer, M.; Bauer, R.; Tschupik, J.; Mayrhofer, P. EBRA: A Method to Measure Migration of Acetabular Components. J. Biomech. 1995, 28, 1225–1236. [Google Scholar] [CrossRef]
- Shah, R.F.; Bini, S.A.; Martinez, A.M.; Pedoia, V.; Vail, T.P. Incremental Inputs Improve the Automated Detection of Implant Loosening Using Machine-Learning Algorithms. Bone Jt. J. 2020, 102-B, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Kingsbury, S.R.; Dube, B.; Thomas, C.M.; Conaghan, P.G.; Stone, M.H. Is a Questionnaire and Radiograph-Based Follow-up Model for Patients with Primary Hip and Knee Arthroplasty a Viable Alternative to Traditional Regular Outpatient Follow-up Clinic? Bone Jt. J. 2016, 98-B, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkes, R.J.; Palmer, J.; Wingham, J.; Williams, D.H. Is Virtual Clinic Follow-up of Hip and Knee Joint Replacement Acceptable to Patients and Clinicians? A Sequential Mixed Methods Evaluation. BMJ Open Qual. 2019, 8, e000502. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set | Metrics | |
|---|---|---|
| Training | Accuracy | 0.99 |
| Validation | Accuracy | 0.975 |
| Test | Accuracy | 0.9677 |
| Sensitivity | 0.9677 | |
| Specificity | 0.9677 | |
| AUC | 0.9933 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loppini, M.; Gambaro, F.M.; Chiappetta, K.; Grappiolo, G.; Bianchi, A.M.; Corino, V.D.A. Automatic Identification of Failure in Hip Replacement: An Artificial Intelligence Approach. Bioengineering 2022, 9, 288. https://doi.org/10.3390/bioengineering9070288
Loppini M, Gambaro FM, Chiappetta K, Grappiolo G, Bianchi AM, Corino VDA. Automatic Identification of Failure in Hip Replacement: An Artificial Intelligence Approach. Bioengineering. 2022; 9(7):288. https://doi.org/10.3390/bioengineering9070288
Chicago/Turabian StyleLoppini, Mattia, Francesco Manlio Gambaro, Katia Chiappetta, Guido Grappiolo, Anna Maria Bianchi, and Valentina D. A. Corino. 2022. "Automatic Identification of Failure in Hip Replacement: An Artificial Intelligence Approach" Bioengineering 9, no. 7: 288. https://doi.org/10.3390/bioengineering9070288
APA StyleLoppini, M., Gambaro, F. M., Chiappetta, K., Grappiolo, G., Bianchi, A. M., & Corino, V. D. A. (2022). Automatic Identification of Failure in Hip Replacement: An Artificial Intelligence Approach. Bioengineering, 9(7), 288. https://doi.org/10.3390/bioengineering9070288