
Retention, Bacterial Adhesion, and Biofilm Formation between Anionic and Zwitterionic Bandage Contact Lenses in Healthy Dogs: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Contact Lenses
2.3. Bacterial Strains
2.4. Bacterial Isolation
2.5. Selecting the Size of BCL
2.6. Retention
2.7. In Vitro Bacterial Adhesion
2.8. In Vitro Biofilm Formation
2.9. In Vivo Bacterial Adhesion
2.10. Statistical Analysis
3. Results
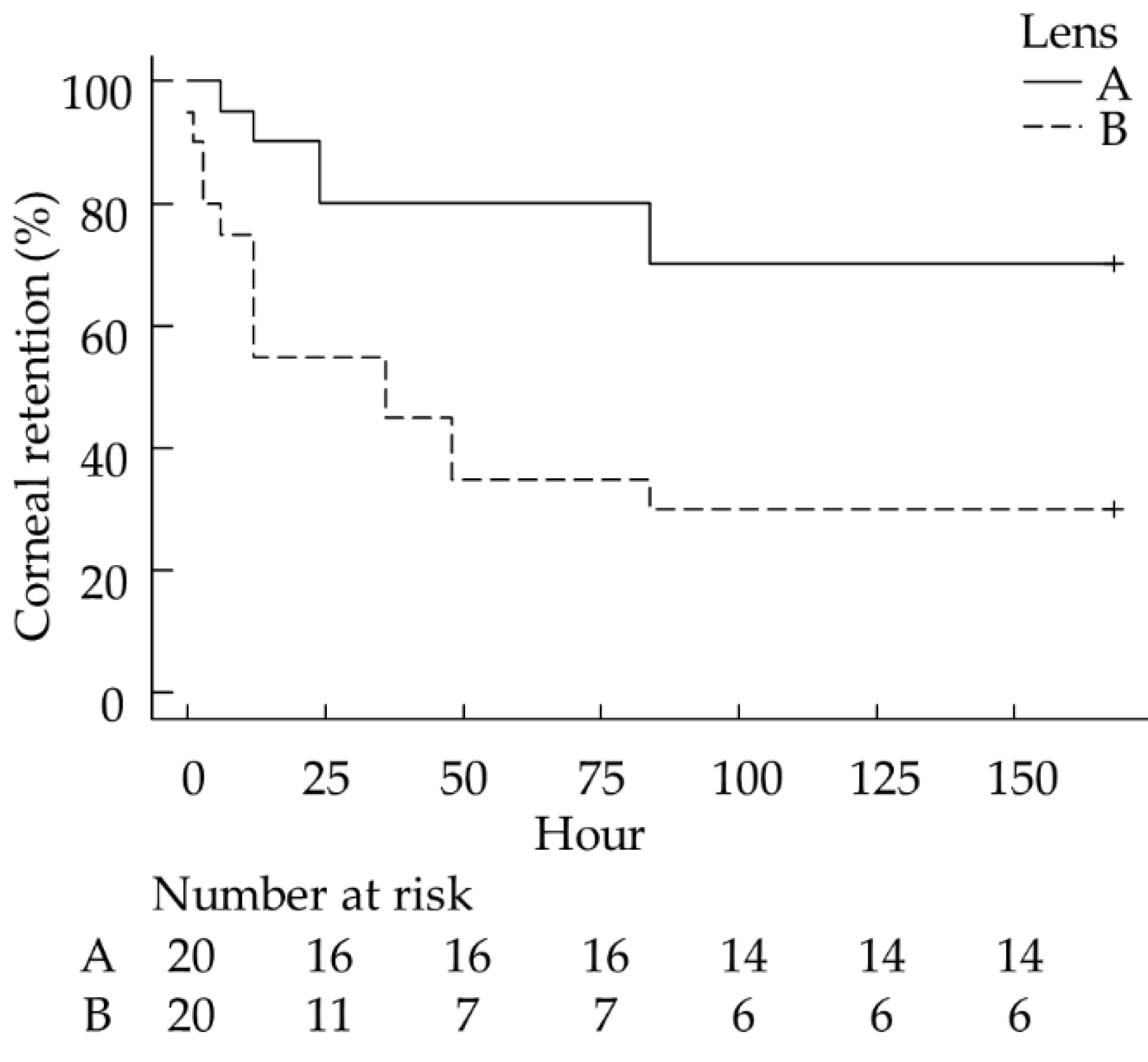
3.1. Retention
3.2. Bacterial Isolation
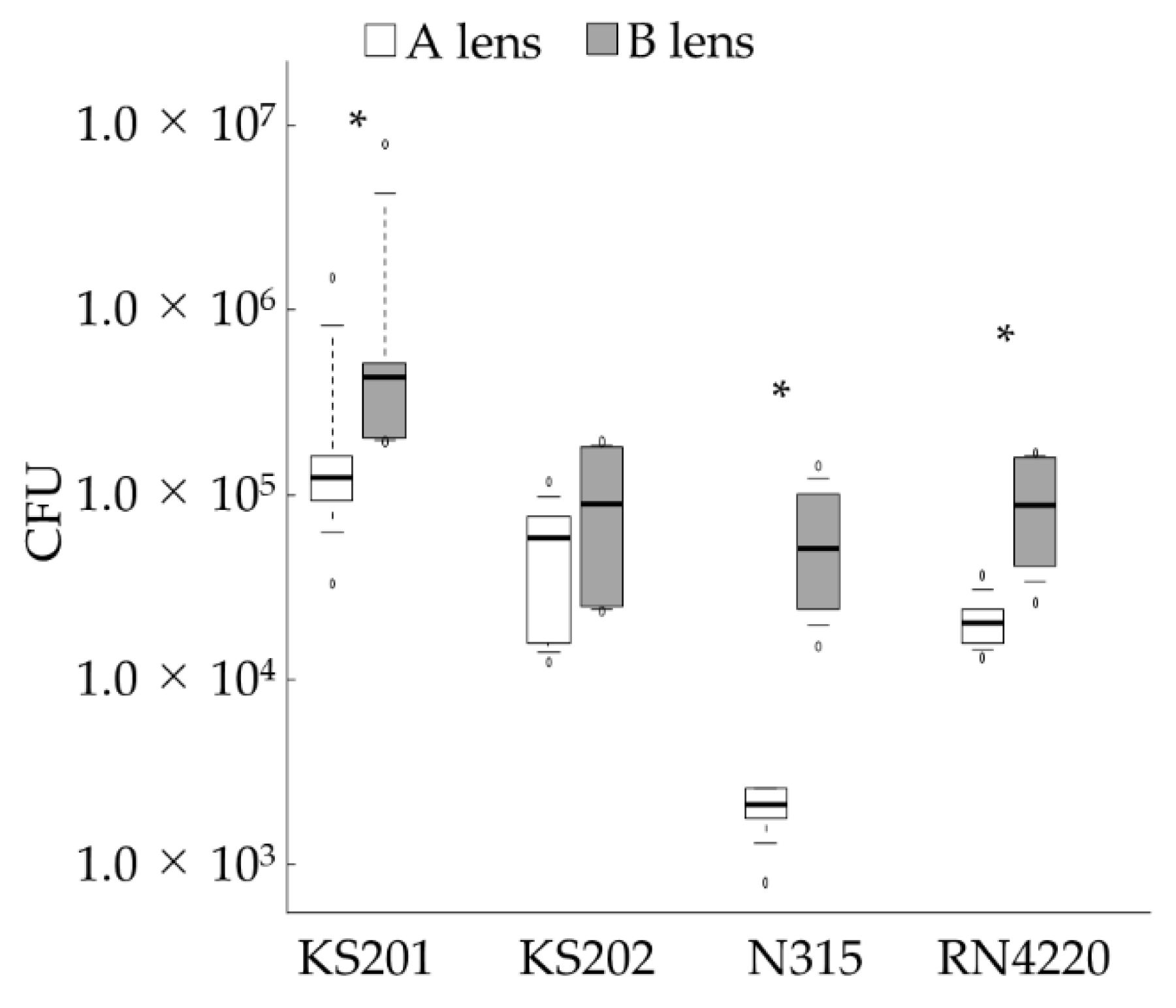
3.3. In Vitro Bacterial Adhesion
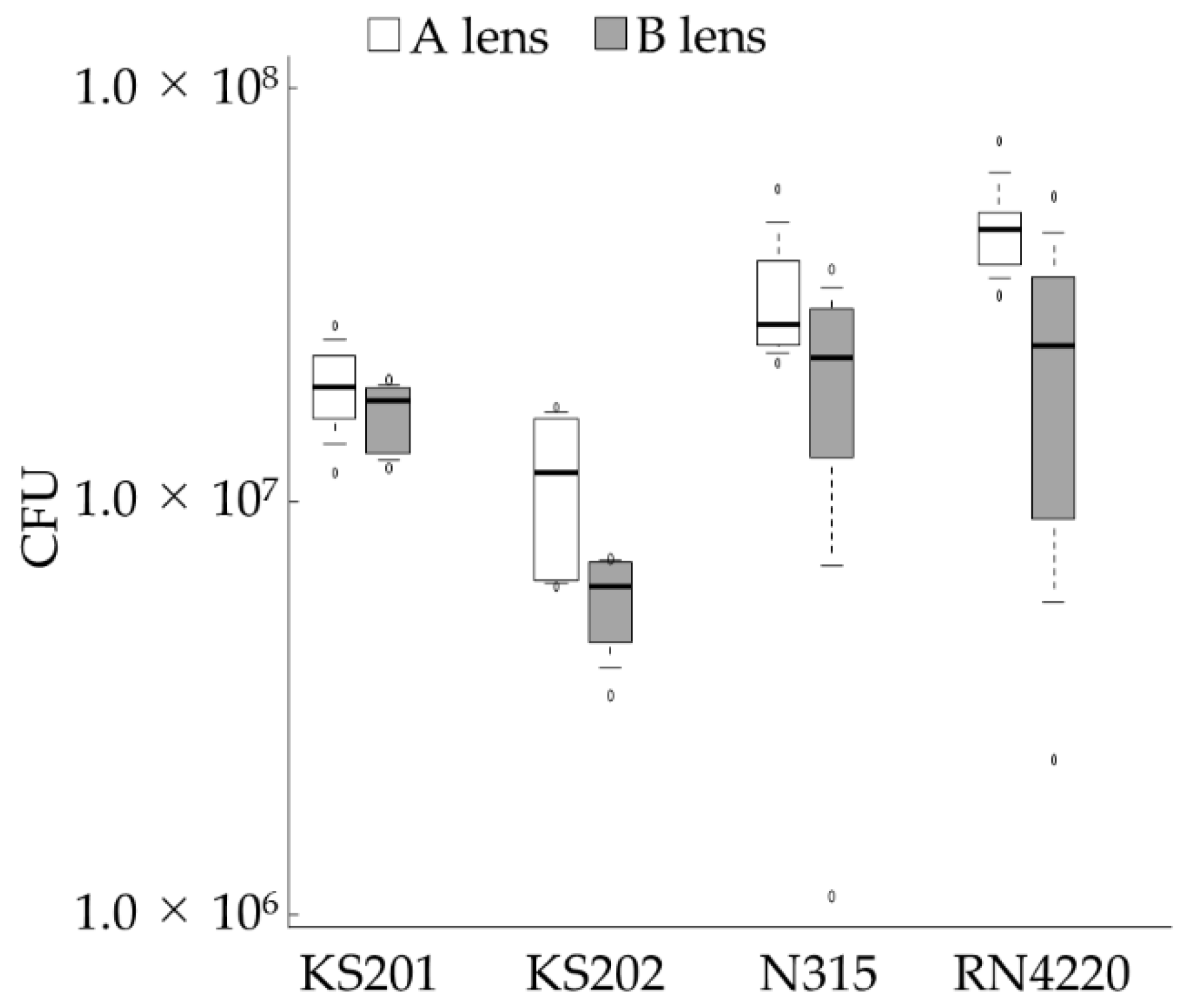
3.4. In Vitro Biofilm Formation
3.5. In Vivo Bacterial Adhesion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dees, D.D.; Fritz, K.J.; Wagner, L.; Paglia, D.; Knollinger, A.M.; Madsen, R. Effect of bandage contact lens wear and postoperative medical therapies on corneal healing rate after diamond burr debridement in dogs. Vet. Ophthalmol. 2017, 20, 382–389. [Google Scholar] [CrossRef]
- Gosling, A.A.; Labelle, A.L.; Breaux, C.B. Management of spontaneous chronic corneal epithelial defects (SCCEDs) in dogs with diamond burr debridement and placement of a bandage contact lens. Vet. Ophthalmol. 2013, 16, 83–88. [Google Scholar] [CrossRef]
- Grinninger, P.; Verbruggen, A.M.J.; Kraijer-Huver, I.M.G.; Djajadiningrat-Laanen, S.C.; Teske, E.; Boevé, M.H. Use of bandage contact lenses for treatment of spontaneous chronic corneal epithelial defects in dogs. J. Small Anim. Pract. 2015, 56, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Wooff, P.J.; Norman, J.C. Effect of corneal contact lens wear on healing time and comfort post LGK for treatment of SCCEDs in boxers. Vet. Ophthalmol. 2015, 18, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Mashige, K.P. A review of corneal diameter, curvature and thickness values and influencing factors. Afr. Vis. Eye Health 2013, 72, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Punjabi, S.; Bedi, N. A clinical study to evaluate therapeutic efficacy of soft contact lenses in corneal diseases. Int. J. Res. Med. Sci. 2016, 4, 4632–4636. [Google Scholar] [CrossRef]
- Ramakrishnan, R.; Naik, A. Comparison of manual keratometer with autokeratometer. Biosci. Biotechnol. Res. Asia 2014, 11, 339–341. [Google Scholar] [CrossRef] [Green Version]
- Braus, B.K.; Riedler, D.; Tichy, A.; Spergser, J.; Schwendenwein, I. The effects of two different types of bandage contact lenses on the healthy canine eye. Vet. Ophthalmol. 2018, 21, 477–486. [Google Scholar] [CrossRef]
- Diehl, K.A.; Bowden, A.C.; Knudsen, D. Bandage contact lens retention in dogs—A pilot study. Vet. Ophthalmol. 2019, 22, 584–590. [Google Scholar] [CrossRef]
- Kawasaki, M.; Furujo, T.; Kuroda, K.; Azuma, K.; Okamoto, Y.; Ito, N. Characterising keratometry in different dog breeds using an automatic handheld keratometer. Vet. Rec. 2020, 186, e4. [Google Scholar] [CrossRef] [Green Version]
- Cheng, K.H.; Leung, S.L.; Hoekman, H.W.; Beekhuis, W.H.; Mulder, P.G.H.; Geerards, A.J.M.; Kijlstra, A. Incidence of contact-lens-associated microbial keratitis and its related morbidity. Lancet 1999, 354, 181–185. [Google Scholar] [CrossRef]
- Loh, K.Y.; Agarwal, P. Contact lens related corneal ulcer. Malays. Fam. Physician 2010, 5, 6–8. [Google Scholar] [PubMed]
- Dosler, S.; Hacioglu, M.; Yilmaz, F.N.; Oyardi, O. Biofilm modelling on the contact lenses and comparison of the in vitro activities of multipurpose lens solutions and antibiotics. PeerJ 2020, 8, e9419. [Google Scholar] [CrossRef] [PubMed]
- Efron, N.; Brennan, N.A.; Chalmers, R.L.; Jones, L.; Lau, C.; Morgan, P.B.; Nichols, J.J.; Szczotka-Flynn, L.B.; Willcox, M.D. Thirty years of ‘quiet eye’ with etafilcon A contact lenses. Contact Lens Anterior Eye 2020, 43, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Willcox, M.D.; Holden, B.A. Contact lens related corneal infections. Biosci. Rep. 2001, 21, 445–461. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.J.; Park, J.H.; Kim, M.; Park, C.Y. The antibiofilm efficacy of nitric oxide on soft contact lenses. BMC Ophthalmol. 2017, 17, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prosser, B.L.; Taylor, D.; Dix, B.A.; Cleeland, R. Method of evaluating effects of antibiotics on bacterial biofilm. Antimicrob. Agents Chemother. 1987, 31, 1502–1506. [Google Scholar] [CrossRef] [Green Version]
- Omali, N.B.; Subbaraman, L.N.; Coles-Brennan, C.; Fadli, Z.; Jones, L.W. Biological and clinical implications of lysozyme deposition on soft contact lenses. Optom. Vis. Sci. 2015, 92, 750–757. [Google Scholar] [CrossRef]
- Auten, C.R.; Urbanz, J.L.; Dees, D.D. Comparison of bacterial culture results collected via direct corneal ulcer vs conjunctival fornix sampling in canine eyes with presumed bacterial ulcerative keratitis. Vet. Ophthalmol. 2020, 23, 135–140. [Google Scholar] [CrossRef]
- Beck, G.; Puchelle, E.; Plotkowski, C.; Peslin, R. Effect of growth on surface charge and hydrophobicity of Staphylococcus aureus. Ann. Inst. Pasteur. Microbiol. 1988, 139, 655–664. [Google Scholar] [CrossRef]
- Gottenbos, B.; Grijpma, D.W.; Van Der Mei, H.C.; Feijen, J.; Busscher, H.J. Antimicrobial effects of positively charged surfaces on adhering Gram-positive and Gram-negative bacteria. J. Antimicrob. Chemother. 2001, 48, 7–13. [Google Scholar] [CrossRef]
- LoPinto, A.J.; Mohammed, H.O.; Ledbetter, E.C. Prevalence and risk factors for isolation of methicillin-resistant Staphylococcus in dogs with keratitis. Vet. Ophthalmol. 2015, 18, 297–303. [Google Scholar] [CrossRef]
- Marshall, K.C. Adsorption and adhesion processes in microbial growth at interfaces. Adv. Colloid Interface Sci. 1986, 25, 59–86. [Google Scholar] [CrossRef]
- Prado, M.R.; Rocha, M.F.G.; Brito, É.H.S.; Girão, M.D.; Monteiro, A.J.; Teixeira, M.F.S.; Sidrim, J.J.C. Survey of bacterial microorganisms in the conjunctival sac of clinically normal dogs and dogs with ulcerative keratitis in Fortaleza, Ceará, Brazil. Vet. Ophthalmol. 2005, 8, 33–37. [Google Scholar] [CrossRef]
- Al-Mujaini, A.; Al-Kharusi, N.; Thakral, A.; Wali, U.K. Bacterial keratitis: Perspective on epidemiology, Clinico-Pathogenesis, diagnosis and treatment. Sultan Qaboos Univ. Med. J. 2009, 9, 184–195. [Google Scholar]
- Sasaki, T.; Tsubakishita, S.; Tanaka, Y.; Sakusabe, A.; Ohtsuka, M.; Hirotaki, S.; Kawakami, T.; Fukata, T.; Hiramatsu, K. Multiplex-PCR method for species identification of coagulase-positive staphylococci. J. Clin. Microbiol. 2010, 48, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.L. Immunopathogenesis of keratoconjunctivitis sicca in the dog. Vet. Clin. North Am. Small Anim. Pract. 2008, 38, 251–268. [Google Scholar] [CrossRef]
- Giraldez, M.J.; Resua, C.G.; Lira, M.; Real Oliveira, M.E.C.D.; Magariños, B.; Toranzo, A.E.; Yebra-Pimentel, E. Contact lens hydrophobicity and roughness effects on bacterial adhesion. Optom. Vis. Sci. 2010, 87, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Merritt, J.H.; Kadouri, D.E.; O’Toole, G.A. Growing and analyzing static biofilms. Curr. Protoc. Microbiol. 2005, 22, 1B.1.1–1B.1.18. [Google Scholar] [CrossRef] [Green Version]
- Okajima, Y.; Kobayakawa, S.; Tsuji, A.; Tochikubo, T. Biofilm formation by Staphylococcus epidermidis on intraocular lens material. Invest. Ophthalmol. Vis. Sci. 2006, 47, 2971–2975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.; Siddireddy, J.S.; Wong, K.; Shen, Q.; Vijay, A.K.; Stapleton, F. Factors Affecting Microbial Contamination on the Back Surface of Worn Soft Contact Lenses. Optom. Vis. Sci. 2021, 98, 512–517. [Google Scholar] [CrossRef]
- Jucker, B.A.; Harms, H.; Zehnder, A.J.B. Adhesion of the positively charged bacterium Stenotrophomonas (Xanthomonas) maltophilia 70401 to glass and teflon. J. Bacteriol. 1996, 178, 5472–5479. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.; Bawazir, M.; Dhall, A.; Kim, H.E.; He, L.; Heo, J.; Hwang, G. Implication of surface properties, bacterial motility, and hydrodynamic conditions on bacterial surface sensing and their initial adhesion. Front. Bioeng. Biotechnol. 2021, 9, 82. [Google Scholar] [CrossRef]
- Terada, A.; Okuyama, K.; Nishikawa, M.; Tsuneda, S.; Hosomi, M. The effect of surface charge property on Escherichia coli initial adhesion and subsequent biofilm formation. Biotechnol. Bioeng. 2012, 109, 1745–1754. [Google Scholar] [CrossRef] [PubMed]
- Artini, M.; Cellini, A.; Scoarughi, G.L.; Papa, R.; Tilotta, M.; Palma, S.; Selan, L. Evaluation of contact lens multipurpose solutions on bacterial biofilm development. Eye Contact Lens 2015, 41, 177–182. [Google Scholar] [CrossRef]
- Baillif, S.; Casoli, E.; Marion, K.; Roques, C.; Pellon, G.; Hartmann, D.J.; Freney, J.; Burillon, C.; Kodjikian, L. A novel in vitro model to study staphylococcal biofilm formation on intraocular lenses under hydrodynamic conditions. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3410–3416. [Google Scholar] [CrossRef] [Green Version]
- Bazzaz, B.S.F.; Jalalzadeh, M.; Sanati, M.; Zarei-Ghanavati, S.; Khameneh, B. Biofilm formation by Staphylococcus epidermidis on foldable and rigid intraocular lenses. Jundishapur J. Microbiol. 2014, 7, e10020. [Google Scholar] [CrossRef] [Green Version]
- Christensen, G.D.; Simpson, W.A.; Younger, J.J.; Baddour, L.M.; Barrett, F.F.; Melton, D.M.; Beachey, E.H. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: A quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbiol. 1985, 22, 996–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolffsohn, J.S.; Drew, T.; Dhallu, S.; Sheppard, A.; Hofmann, G.J.; Prince, M. Impact of soft contact lens edge design and midperipheral lens shape on the epithelium and its indentation with lens mobility. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6190–6196. [Google Scholar] [CrossRef] [Green Version]
- Sebbag, L.; Allbaugh, R.A.; Weaver, A.; Seo, Y.J.; Mochel, J.P. Histamine-induced conjunctivitis and breakdown of blood–tear barrier in dogs: A model for ocular pharmacology and therapeutics. Front. Pharmacol. 2019, 10, 752. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A Lens | B Lens | |
|---|---|---|
| Material | Etafilcon A | SIB |
| Ionicity | Anionic | Zwitterionic |
| BC (mm) | 8.9/9.3 | 8.9/9.3 |
| DIA (mm) | 16.0 | 16.0 |
| CT (mm) | 0.25 | 0.25 |
| WC (%) | 58 | 58 |
| Grade | Both Lenses | A Lens | B Lens |
|---|---|---|---|
| 0 | 417 (95.4%) | 262 (95.3%) | 155 (95.7%) |
| 1 | 020 (4.6%) | 013 (4.7%) | 007 (4.3%) |
| 2 | 000 (0%) | 000 (0%) | 000 (0%) |
| 3 | 000 (0%) | 000 (0%) | 000 (0%) |
| Total recordings | 437 | 275 | 162 |
| A Lens | B Lens | |
|---|---|---|
| CFU/lens | 35.9 ± 38.4 | 49.1 ± 91.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kita, M.; Kanai, K.; Ono, H.K.; Otaka, Y.; Okada, D.; Nagai, N.; Kudo, R.; Yamashita, Y.; Hino, S.; Matsunaga, T.; et al. Retention, Bacterial Adhesion, and Biofilm Formation between Anionic and Zwitterionic Bandage Contact Lenses in Healthy Dogs: A Pilot Study. Vet. Sci. 2021, 8, 238. https://doi.org/10.3390/vetsci8100238
Kita M, Kanai K, Ono HK, Otaka Y, Okada D, Nagai N, Kudo R, Yamashita Y, Hino S, Matsunaga T, et al. Retention, Bacterial Adhesion, and Biofilm Formation between Anionic and Zwitterionic Bandage Contact Lenses in Healthy Dogs: A Pilot Study. Veterinary Sciences. 2021; 8(10):238. https://doi.org/10.3390/vetsci8100238
Chicago/Turabian StyleKita, Mizuki, Kazutaka Kanai, Hisaya K. Ono, Yuya Otaka, Daiki Okada, Noriaki Nagai, Rina Kudo, Yohei Yamashita, Shiori Hino, Toru Matsunaga, and et al. 2021. "Retention, Bacterial Adhesion, and Biofilm Formation between Anionic and Zwitterionic Bandage Contact Lenses in Healthy Dogs: A Pilot Study" Veterinary Sciences 8, no. 10: 238. https://doi.org/10.3390/vetsci8100238
APA StyleKita, M., Kanai, K., Ono, H. K., Otaka, Y., Okada, D., Nagai, N., Kudo, R., Yamashita, Y., Hino, S., Matsunaga, T., & Tajima, K. (2021). Retention, Bacterial Adhesion, and Biofilm Formation between Anionic and Zwitterionic Bandage Contact Lenses in Healthy Dogs: A Pilot Study. Veterinary Sciences, 8(10), 238. https://doi.org/10.3390/vetsci8100238