
Inguinal Hernia in Nonhuman Primates: From Asymptomatic to Life-Threatening Events



Abstract
:1. Introduction
2. Epidemiology and Anamnesis
- Trauma [12]. Although the exact role of trauma in the occurrence and progress of inguinal hernia remains unclear, accidents such as a fall from height while hopping from one tree to another may play a role;
- Congenital weakness of muscles of the groin region or other congenital anomalies from the time of birth [12];
- In utero lead exposure [26].
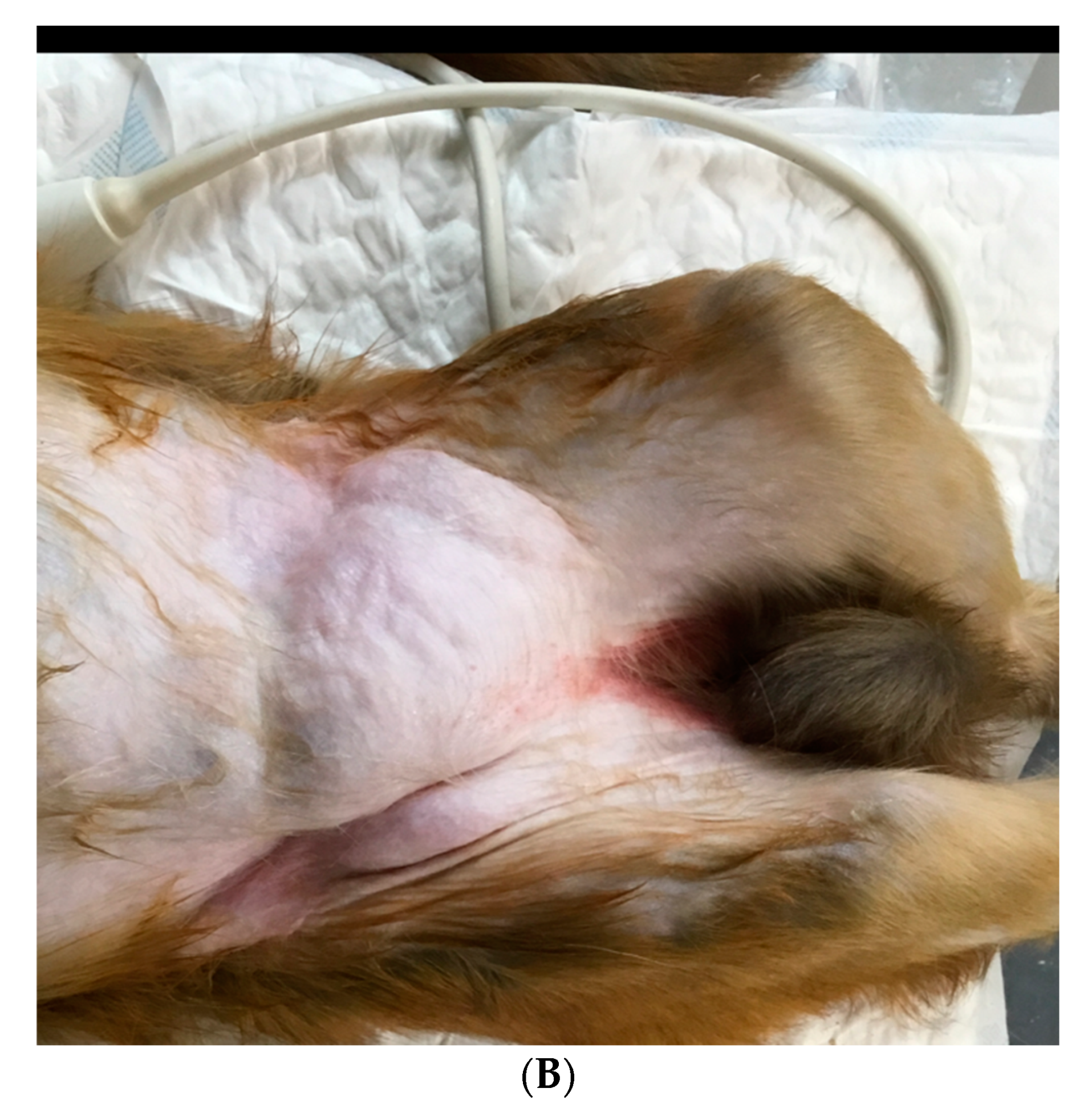
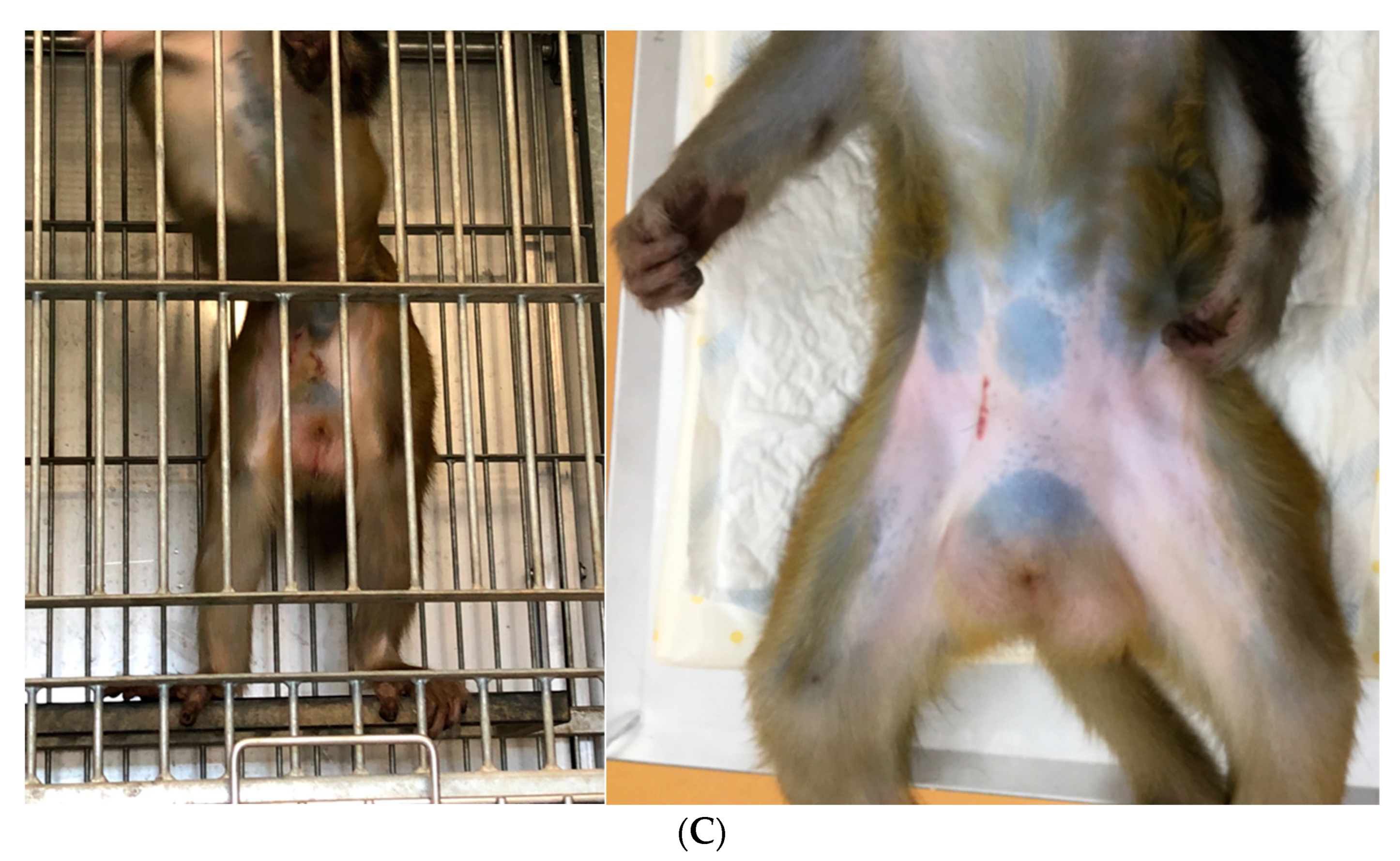
3. Clinical Signs
4. Diagnostics
5. Differential Diagnosis
6. Medical Management
7. Prognosis
8. Complications
9. Reproductive Potential
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shakil, A.; Aparicio, K.; Barta, E.; Munez, K. Inguinal Hernias: Diagnosis and Management. Am. Fam. Physician 2020, 102, 487–492. [Google Scholar]
- Pastorino, A.; Alshuqayfi, A.A. Strangulated Hernia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555972/ (accessed on 28 December 2021).
- Holzheimer, R.G. Inguinal Hernia: Classification, diagnosis and treatment--classic, traumatic and Sportsman’s hernia. Eur. J. Med. Res. 2005, 10, 121–134. [Google Scholar]
- Gilbert, A.I. An anatomic and functional classification for the diagnosis and treatment of inguinal hernia. Am. J. Surg. 1989, 157, 331–333. [Google Scholar] [CrossRef]
- Jenkins, J.T.; O’Dwyer, P.J. Inguinal hernias. Br. Med. J. 2008, 336, 269–272. [Google Scholar] [CrossRef]
- Kulacoglu, H. Current options in inguinal hernia repair in adult patients. Hippokratia 2011, 15, 223–231. [Google Scholar]
- Cline, M.J.; Brignolo, L.; Ford, E.W. Chapter 10: Urogenital System. In Nonhuman Primates in Biomedical Research, Volume II: Diseases, 2nd ed.; Abee, C.R., Mansfield, K., Tardif, S., Morris, T., Eds.; Academic Press: San Diego, CA, USA, 2012. [Google Scholar]
- Valverde, C.R.; Christe, K.L. Chapter 22: Radiographic imaging of nonhuman primates. In The Laboratory Primate; Wolfe-Coote, S., Ed.; Elsevier Academic Press: San Diego, CA, USA, 2005. [Google Scholar]
- Butler, T.M.; Brown, B.G.; Dysko, R.C.; Ford, E.W.; Hoskins, D.E.; Klein, H.J.; Levin, J.L.; Murray, K.A.; Rosenberg, D.P.; Southers, J.L.; et al. Chapter 13: Medical management. In Nonhuman Primates in Biomedical Research: Biology and Management; Bennett, T.B., Abee, C.R., Henrickson, R., Eds.; Academic Press: San Diego, CA, USA, 1995. [Google Scholar]
- Kavoussi, P.K.; Wilkerson, G.; Gray, S.B. Vasocutaneous fistula formation and repair following inguinal hernia repair in a rhesus monkey (Macaca mulatta). J. Med. Primatol. 2022, 51, 183–186. [Google Scholar] [CrossRef]
- Berg, M.R.; MacAllister, R.P.; Martin, L.D. Nonreducible Inguinal Hernia Containing the Uterus and Bilateral Adnexa in a Rhesus Macaque (Macaca mulatta). Comp. Med. 2017, 67, 537–540. [Google Scholar]
- Kumar, V.; Raj, A. Surgical management of unilateral inguinoscrotal hernia in a male rhesus macaque. J. Vet. Sci. Technol. 2012, 1, 1–4. [Google Scholar]
- Jaax, G.P.; McNamee, G.A.; Donovan, J.C., Jr.; Stokes, W.S.; Montrey, R.D.; Rozmiarek, H. An Incarcerated Inguinal Hernia Involving the Urinary Bladder in a Cynomolgus Monkey (Macaca Fascicularis); Defense Technical Information Center: Fort Detrick, MD, USA, 1982. [Google Scholar]
- Carpenter, R.H.; Riddle, K.E. Direct inguinal hernia in the cynomolgus monkey (Macaca fascicularis). J. Med. Primatol. 1980, 9, 194–199. [Google Scholar] [CrossRef]
- Sadoughi, B.; Dirheimer, M.; Regnard, P.; Wanert, F. Surgical management of a strangulated inguinal hernia in a Cynomolgus Monkey (Macaca fascicularis): A case report with discussion of diagnosis, and review of literature. Rev. De Primatol. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Ambar, N.; Fahie, M.; Levi, O.; Lee, L.; Martin, H.; Eshar, D. Surgical Management of an Inguinal Hernia in an Infant Captive Eastern Hoolock Gibbon (Hoolock leuconedys). Isr. J. Vet. Med. 2020, 75, 22–27. [Google Scholar]
- Taylor, A.F.; Smith, M.; Eichberg, J.W. Inguinal hernial surgery in an infant chimpanzee. J. Med. Primatol. 1989, 18, 415–417. [Google Scholar] [CrossRef]
- Starzynski, W. Surgery for abdominal hernia in a pig-tailed macaque Macaca nemestrina. Int. Zoo Yearb. 1965, 5, 184–185. [Google Scholar] [CrossRef]
- Öberg, S.; Andresen, K.; Rosenberg, J. Etiology of Inguinal Hernias: A Comprehensive Review. Front. Surg. 2017, 4, 52. [Google Scholar] [CrossRef] [Green Version]
- Köckerling, F.; Simons, M.P. Current Concepts of Inguinal Hernia Repair. Visc. Med. 2018, 34, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Primatesta, P.; Goldacre, M.J. Inguinal hernia repair: Incidence of elective and emergency surgery, readmission and mortality. Int. J. Epidemiol. 1996, 25, 835–839. [Google Scholar] [CrossRef] [Green Version]
- Burcharth, J.; Pommergaard, H.C.; Rosenberg, J. The inheritance of groin hernia: A systematic review. Hernia 2013, 17, 183–189. [Google Scholar] [CrossRef]
- Zoller, B.; Ji, J.; Sundquist, J.; Sundquist, K. Shared and nonshared familial susceptibility to surgically treated inguinal hernia, femoral hernia, incisional hernia, epigastric hernia, and umbilical hernia. J. Am. Coll. Surg. 2013, 217, 289–299. [Google Scholar] [CrossRef]
- Andrews, E.; Bissell, A. Comparative Studies of Hernia in Man and Animals. J. Urol. 1934, 31, 839–866. [Google Scholar] [CrossRef]
- Fowler, M.E. Chapter 37: New world and old world monkeys, In Fowler’s Zoo and Wild Animal Medicine; Miller, R.E., Fowler, M.E., Eds.; Saunders: St. Louis, Mo, USA, 2014; Volume 8, p. 307. [Google Scholar]
- Krugner-Higby, L.; Rosenstein, A.; Handschke, L.; Luck, M.; Laughlin, N.K.; Mahvi, D.; Gendron, A. Inguinal hernias, endometriosis, and other adverse outcomes in rhesus monkeys following lead exposure. Neurotoxicol. Teratol. 2003, 25, 561–570. [Google Scholar] [CrossRef]
- Bush, M.; Heller, R.; Gray, C.W.; Oh, K.S.; James, A.E. Peritoneography and Herniography in Non-Human Primates. Vet. Radiol. 1975, 15, 77–82. [Google Scholar] [CrossRef]
- Grosfeld, J.L. Current concepts in inguinal hernia in infants and children. World J. Surg. 1989, 13, 506–515. [Google Scholar] [CrossRef]
- Liem, M.S.; van der Graaf, Y.; Zwart, R.C.; Geurts, I.; van Vroonhoven, T.J. Risk factors for inguinal hernia in women: A case control study. Am. J. Epidemiol. 1997, 146, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.; Cho, J.; Michael, M.J.; Saouaf, R.; Towfigh, S. Role of imaging in the diagnosis of occult hernias. JAMA Surg. 2014, 149, 1077–1080. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.; Light, D.; Kasim, A.; Nice, C. A systematic review and meta-analysis of the role of radiology in the diagnosis of occult inguinal hernia. Surg. Endosc. 2013, 27, 11–18. [Google Scholar] [CrossRef]
- James, A.E., Jr.; Heller, R.M., Jr.; Bush, M.; Gray, C.W.; Oh, K.S. Positive contrast peritoneography and herniography in primate animals. With special reference to indirect inguinal hernias. J. Med. Primatol. 1975, 4, 114–119. [Google Scholar] [CrossRef]
- Kingsnorth, A.; LeBlanc, K. Hernias: Inguinal and incisional. Lancet 2003, 362, 1561–1571. [Google Scholar] [CrossRef]
- Montgomery, J.; Dimick, J.B.; Telem, D.A. Management of Groin Hernias in Adults-2018. JAMA 2018, 320, 1029–1030. [Google Scholar] [CrossRef]
- Srisajjakul, S.; Prapaisilp, P.; Bangchokdee, S. Comprehensive review of acute small bowel ischemia: CT imaging findings, pearls, and pitfalls. Emerg. Radiol. 2022, 29, 531–544. [Google Scholar] [CrossRef]
- Gandhi, J.; Zaidi, S.; Suh, Y.; Joshi, G.; Smith, N.L.; Ali Khan, S. An index of inguinal and inguinofemoral masses in women: Critical considerations for diagnosis. Transl. Res. Anat. 2018, 12, 1–10. [Google Scholar] [CrossRef]
- LeBlanc, K.E.; LeBlanc, L.L.; LeBlanc, K.A. Inguinal hernias: Diagnosis and management. Am. Fam. Physician 2013, 87, 844–848. [Google Scholar] [PubMed]
- Kouhia, S. Complication and Cost Analysis of Inguinal Hernia Surgery: Comparison of Open and Laparoscopic Techniques. Ph.D. Thesis, Faculty of Health Sciences Publications of the University of Eastern Finland, University of Eastern Finland, Joensuu, Finland, 2016. [Google Scholar]
- HerniaSurge Group. International guidelines for groin hernia management. Hernia 2018, 22, 1–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammoud, M.; Gerken, J. Inguinal Hernia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513332/ (accessed on 22 August 2021).
- van den Heuvel, B.; Dwars, B.J.; Klassen, D.R.; Bonjer, H.J. Is surgical repair of an asymptomatic groin hernia appropriate? A review. Hernia 2011, 15, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgibbons, R.J., Jr.; Giobbie-Hurder, A.; Gibbs, J.O.; Dunlop, D.D.; Reda, D.J.; McCarthy, M., Jr.; Neumayer, L.A.; Barkun, J.S.; Hoehn, J.L.; Murphy, J.T.; et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: A randomized clinical trial. JAMA 2006, 295, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Gallegos, N.C.; Dawson, J.; Jarvis, M.; Hobsley, M. Risk of strangulation in groin hernias. Br. J. Surg. 1991, 178, 1171–1173. [Google Scholar] [CrossRef] [PubMed]
- McFadyen, B.V.; Mathis, C.R. Inguinal herniorraphy: Complications and recurrences. Semin. Laparosc. Surg. 1994, 1, 128–140. [Google Scholar]
- Bali, C.; Tsironis, A.; Zikos, N.; Mouselimi, M.; Katsamakis, N. An unusual case of a strangulated right inguinal hernia containing the sigmoid colon. Int. J. Surg. Case. Rep. 2011, 2, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Bax, T.; Sheppard, B.C.; Crass, R.A. Surgical options in the management of groin hernias. Am, Fam, Physician 1999, 59, 893–906. [Google Scholar]
- Itani, K.M.F.; Fitzgibbons, R. Approach to Groin Hernias. JAMA Surg. 2019, 154, 551–552. [Google Scholar] [CrossRef]
- Kokotovic, D.; Bisgaard, T.; Helgstrand, F. Long-term Recurrence and Complications Associated With Elective Incisional Hernia Repair. JAMA 2016, 316, 1575–1582. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.N.; Finch, J.G. Which mesh for hernia repair? Ann. R Coll. Surg. Engl. 2010, 92, 272–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempton, S.J.; Israel, J.S.; Capuano, S., III; Poore, S.O. Repair of a Large Ventral Hernia in a Rhesus Macaque (Macaca mulatta) by Using an Abdominal Component Separation Technique. Comp. Med. 2018, 68, 177–181. [Google Scholar] [PubMed]
- Gudigopuram, S.V.R.; Raguthu, C.C.; Gajjela, H.; Kela, I.; Kakarala, C.L.; Hassan, M.; Belavadi, R.; Sange, I. Inguinal Hernia Mesh Repair: The Factors to Consider When Deciding Between Open Versus Laparoscopic Repair. Cureus 2021, 13, e19628. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.L.; Phillips, E.H. Laparoscopic repair and groin hernia surgery. Surg. Clin. North Am. 1998, 78, 1047–1062. [Google Scholar] [CrossRef]
- Tamme, C.; Scheidbach, H.; Hampe, C.; Schneider, C.; Köckerling, F. Totally extraperitoneal endoscopic inguinal hernia repair (TEP). Surg. Endosc. 2003, 17, 190–195. [Google Scholar] [CrossRef]
- Fossum, T.W. Chapter 6: Preparation of the operative site. In Small Animal Surgery, 2nd ed.; Fossum, T.W., Hedlund, C.S., Hulse, D.A., Johnson, A.L., Seim, H.B., Willard, M.D., Carroll, G.L., Eds.; Mosby Inc.: St. Louis, Mo, USA, 2002. [Google Scholar]
- Fossum, T.W. Chapter 20 Surgery of the abdominal cavity. In Small Animal Surgery, 2nd ed.; Fossum, T.W., Hedlund, C.S., Hulse, D.A., Johnson, A.L., Seim, H.B., Willard, M.D., Carroll, G.L., Eds.; Mosby Inc.: St. Louis, Mo, USA, 2002. [Google Scholar]
- Popilskis, S.J.; Kohn, D.F. Chapter 11: Anesthesia and Analgesia in Nonhuman Primates. In Anesthesia and Analgesia in Laboratory Animals; Academic Press: San Diego, CA, USA, 1997; pp. 233–255. [Google Scholar]
- Pizarro, A.I.; Amarasekaran, B.; Brown, D.; Pizzi, R. Laparoscopic repair of an umbilical hernia in a Western chimpanzee (Pan troglodytes verus) rescued in Sierra Leone. J. Med. Primatol. 2019, 48, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Mallick, I.H.; Yang, W.; Winslet, M.C.; Seifalian, A.M. Ischemia-reperfusion injury of the intestine and protective strategies against injury. Dig. Dis. Sci. 2004, 49, 1359–1377. [Google Scholar] [CrossRef]
- Khalil, A.A.; Aziz, F.A.; Hall, J.C. Reperfusion Injury. Plast. Reconstr. Surg. 2006, 117, 1024–1033. [Google Scholar] [CrossRef]
- Smeak, D.D.; Monnet, E. Chapter 25: Enterectomy. In Gastrointestinal Surgical Techniques in Small Animals; Monnet, E., Smeak, D.D., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2020; pp. 187–202. [Google Scholar]
- Bala, M.; Kashuk, J.; Moore, E.E.; Kluger, Y.; Biffl, W.; Augusto Gomes, C.; Ben-Ishay, O.; Rubinstein, C.; Balogh, J.Z.; Civil, I.; et al. Acute mesenteric ischemia: Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2017, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Woods, R.K.; Dellinger, E.P. Current guidelines for antibiotic prophylaxis of surgical wounds. Am. Fam. Physician 1998, 57, 2731–2740. [Google Scholar]
- European Medicines Agency, Committee for Veterinary Medicinal Products (CVMP). Advice on the Designation of Antimicrobials or Groups of Antimicrobials Reserved for Treatment of Certain Infections in Humans—In Relation to Implementing Measures under Article 37(5) of Regulation (EU) 2019/6 on Veterinary Medicinal Products, EMA/CVMP/678496/2021; European Medicines Agency: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Wong, P.F.; Gilliam, A.D.; Kumar, S.; Shenfine, J.; O’Dair, G.N.; Leaper, D.J. Antibiotic regimens for secondary peritonitis of gastrointestinal origin in adults. Cochrane Database Syst Rev. 2005, 18, CD004539. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.P.; Rao, R.; Nanda, S. Amoxicillin: A broad spectrum antibiotic. Int. J. Pharm. Pharm. Sci. 2011, 3, 30–37. [Google Scholar]
- Ory, E.M.; Yow, E.M. The Use and Abuse of the Broad Spectrum Antibiotics. JAMA 1963, 185, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Burcharth, J. The epidemiology and risk factors for recurrence after inguinal hernia surgery. Dan. Med. J. 2014, 61, B4846. [Google Scholar]
- Siddaiah-Subramanya, M.; Ashrafi, D.; Memon, B.; Memon, M.A. Causes of recurrence in laparoscopic inguinal hernia repair. Hernia 2018, 22, 975–986. [Google Scholar] [CrossRef] [Green Version]
- Ashrafi, D.; Siddaiah-Subramanya, M.; Memon, B.; Memon, M.A. Causes of recurrences after open inguinal herniorrhaphy. Hernia 2019, 23, 637–645. [Google Scholar] [CrossRef]
- Andrews, N.J. Presentation and outcome of strangulated external hernia in a district general hospital. Br. J. Surg. 1981, 68, 329–332. [Google Scholar] [CrossRef]
- Buch, K.E.; Tabrizian, P.; Divino, C.M. Management of Hernias in Pregnancy. J. Am. Coll. Surg. 2008, 207, 539–542. [Google Scholar] [CrossRef]
- Staelens, A.S.; Van Cauwelaert, S.; Tomsin, K.; Mesens, T.; Malbrain, M.L.; Gyselaers, W. Intra-abdominal pressure measurements in term pregnancy and postpartum: An observational study. PLoS ONE 2014, 9, e104782. [Google Scholar] [CrossRef] [Green Version]
- Lechner, M.; Fortelny, R.; Ofner, D.; Mayer, F. Suspected inguinal hernias in pregnancy—Handle with care! Hernia 2014, 18, 375–379. [Google Scholar] [CrossRef]
- Oma, E.; Henriksen, N.A.; Jensen, K.K. Ventral hernia and pregnancy: A systematic review. Am. J. Surg. 2019, 217, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Dent, B.; Al Samaraee, A.; Coyne, P.; Nice, C.; Katory, M. Varices of the round ligament mimicking an inguinal hernia—an important differential diagnosis during pregnancy. Ann. R. Coll. Surg. Engl. 2010, 92, e10–e11. [Google Scholar] [CrossRef] [PubMed]
- Yonggang, H.; Jing, Y.; Ping, W.; Guodong, G.; Chenxia, M.; Xiaojing, X.; Fangjie, Z.; Hao, W. Forty-one cases of round ligament varicosities that are easily misdiagnosed as inguinal hernias. Hernia 2017, 21, 901–904. [Google Scholar] [CrossRef]
- IJpma, F.F.; Boddeus, K.M.; de Haan, H.H.; van Geldere, D. Bilateral round ligament varicosities mimicking inguinal hernia during pregnancy. Hernia 2009, 13, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Bittner, R.; Borhanian, K.; Mitterwallner, S.; Emmanuel, K.; Mayer, F. Is round ligament varicosity in pregnancy a common precursor for the later development of inguinal hernias? The prospective analysis of 28 patients over 9 years. Hernia 2020, 24, 633–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IJpma, F.F.A.; Boddeus, K.M.; de Haan, H.H.; van Geldere, D. Management of Hernias in Pregnancy. J. Am. Coll. Surg. 2009, 208, 320. [Google Scholar] [CrossRef] [PubMed]
- Getman, L.M. Post castration evisceration. Equine Vet. Educ. 2013, 25, 563–564. [Google Scholar] [CrossRef]
- Weaver, A.D. Acquired incarcerated inguinal hernia: A review of 13 horses. Can. Vet. J. 1987, 28, 195–199. [Google Scholar]
- Wilson, A.P.; Vessey, S.H. Behavior of free-ranging castrated rhesus monkeys. Folia Primatol. 1968, 9, 1–14. [Google Scholar] [CrossRef]
- Zitzmann, M.; Nieschlag, E. Testosterone levels in healthy men and the relation to behavioural and physical characteristics: Facts and constructs. Eur. J. Endocrinol. 2001, 144, 183–197. [Google Scholar] [CrossRef] [Green Version]
- AVMA. Literature Review on the Welfare Implications of Castration of Cattle. American Veterinary Medical Association. 2014. Available online: https://www.avma.org/KB/Resources/LiteratureReviews/Documents/castration-cattle-bgnd.pdf (accessed on 15 July 2014).
- Kessler, M.J.; Wang, Q.; Cerronim, A.M.; Kessler, M.J.; Wang, Q.; Cerroni, A.M.; Grynpas, M.D.; Gonzalez Velez, O.D.; Rawlins, R.G.; Ethun, K.F.; et al. Long-term effects of castration on the skeleton of male rhesus monkeys (Macaca mulatta). Am. J. Primatol. 2016, 78, 152–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, A.C. The influence of steroid sex hormones on the cognitive and emotional processing of visual stimuli in humans. Front. Neuroendocrinol. 2013, 34, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Hart, B.L. Effect of gonadectomy on subsquent development of age-related cognitive impairment in dogs. J. Am. Vet. Med. Association. 2001, 219, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, N.; Hanaoka, R.; Horiuchi, H.; Kitakaze, T.; Mitani, T.; Inui, H.; Yamaji, R. Castration influences intestinal microflora and induces abdominal obesity in high-fat diet-fed mice. Sci. Rep. 2016, 10, 23001. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Zakikhani, M.; David, S.; Algire, C.; Blouin, M.J.; Pollak, M. Effects of castration on insulin levels and glucose tolerance in the mouse differ from those in man. Prostate 2010, 70, 1628–1635. [Google Scholar] [CrossRef] [PubMed]
- Krotkiewski, M.; Kral, J.G.; Karlsson, J. Effects of castration and testosterone substitution on body composition and muscle metabolism in rats. Acta. Physiol. Scand. 1980, 109, 233–237. [Google Scholar] [CrossRef]
- Wilson, J.D.; Roehrborn, C. Long-term consequences of castration in men: Lessons from the Skoptzy and the eunuchs of the Chinese and Ottoman courts. J. Clin. Endocrinol. Metab. 1999, 84, 4324–4331. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Common Name | Latin Name | Reference | Number of Cases | Age | Sex |
|---|---|---|---|---|---|
| Rhesus macaque | Macaca mulatta | [10] | 1 | 6 years | Male |
| [11] | 1 | 3 years | Female | ||
| [12] | 1 | 12 years | Male | ||
| Cynomolgus macaque | Macaca fascicularis | [13] | 1 | Adult * | Male |
| [14] | 1 | Adult * | Male | ||
| [15] | 1 | 14 years | Male | ||
| Eastern Hoolock gibbon | Hoolock leuconedys | [16] | 1 | 3 weeks | Male |
| Chimpanzee | Pan troglodytes | [17] | 1 | 5 weeks | Male |
| Pig tailed macaque | Macaca nemestrina | [18] | 1 | Adult * | Female |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Garza, M.A.; Hegge, S.R.; Bakker, J. Inguinal Hernia in Nonhuman Primates: From Asymptomatic to Life-Threatening Events. Vet. Sci. 2022, 9, 280. https://doi.org/10.3390/vetsci9060280
de la Garza MA, Hegge SR, Bakker J. Inguinal Hernia in Nonhuman Primates: From Asymptomatic to Life-Threatening Events. Veterinary Sciences. 2022; 9(6):280. https://doi.org/10.3390/vetsci9060280
Chicago/Turabian Stylede la Garza, Melissa A., Sara R. Hegge, and Jaco Bakker. 2022. "Inguinal Hernia in Nonhuman Primates: From Asymptomatic to Life-Threatening Events" Veterinary Sciences 9, no. 6: 280. https://doi.org/10.3390/vetsci9060280
APA Stylede la Garza, M. A., Hegge, S. R., & Bakker, J. (2022). Inguinal Hernia in Nonhuman Primates: From Asymptomatic to Life-Threatening Events. Veterinary Sciences, 9(6), 280. https://doi.org/10.3390/vetsci9060280