Improving Care Transitions for Hospitalized Veterans Discharged to Skilled Nursing Facilities: A Focus on Polypharmacy and Geriatric Syndromes


Abstract
:1. Introduction
1.1. Problem Description
1.2. Available Knowledge
1.3. Rationale and Aims
2. Materials and Methods
2.1. Study Setting, Design, and Context
2.2. Participants
2.3. Data Collection
2.4. Intervention
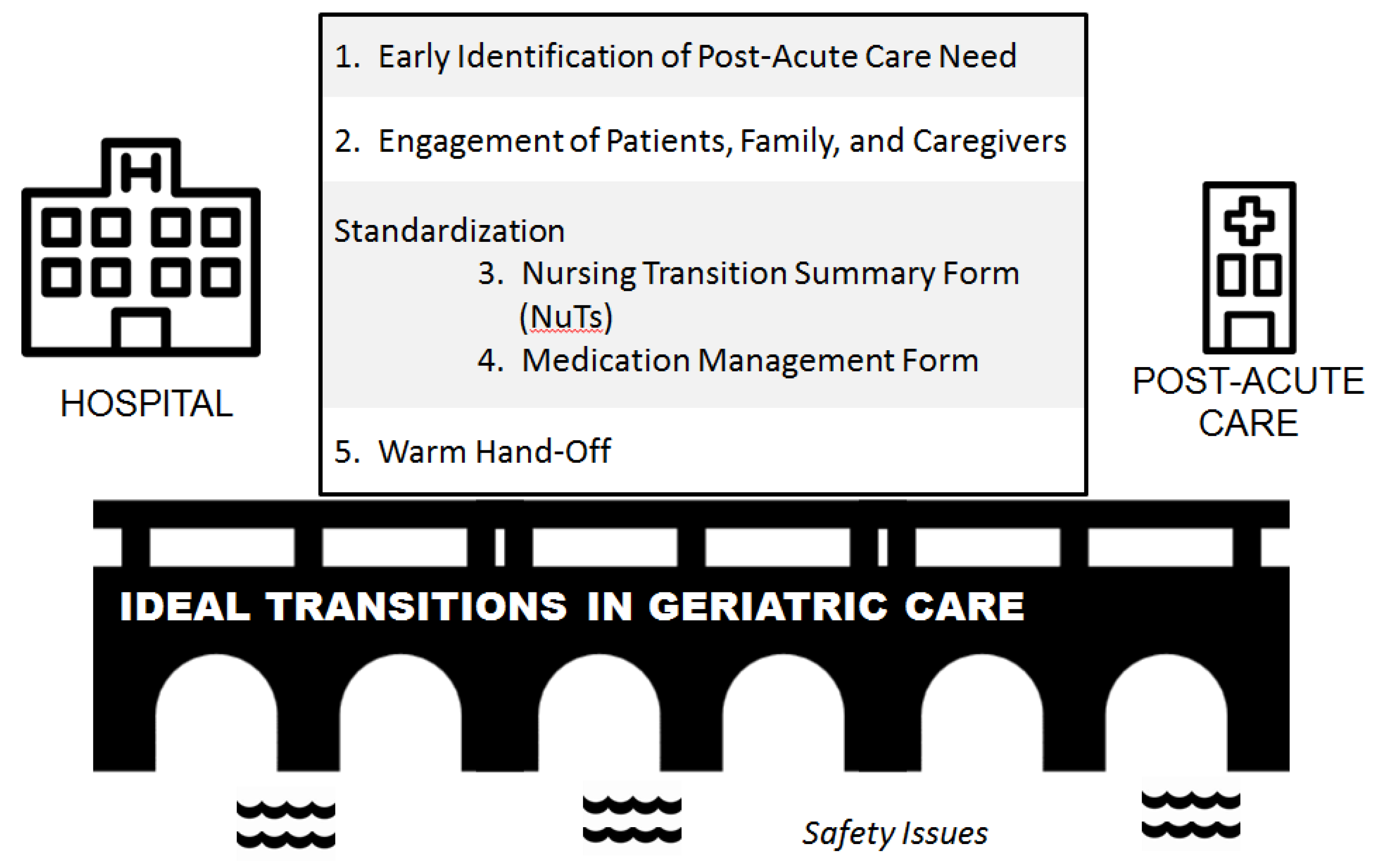
2.4.1. The Care Transitions Communication Tools
2.4.2. Warm Handover
2.5. Measures
2.6. Analysis
3. Results
3.1. Patient Characteristics
3.2. Geriatric Syndromes
3.3. Polypharmacy
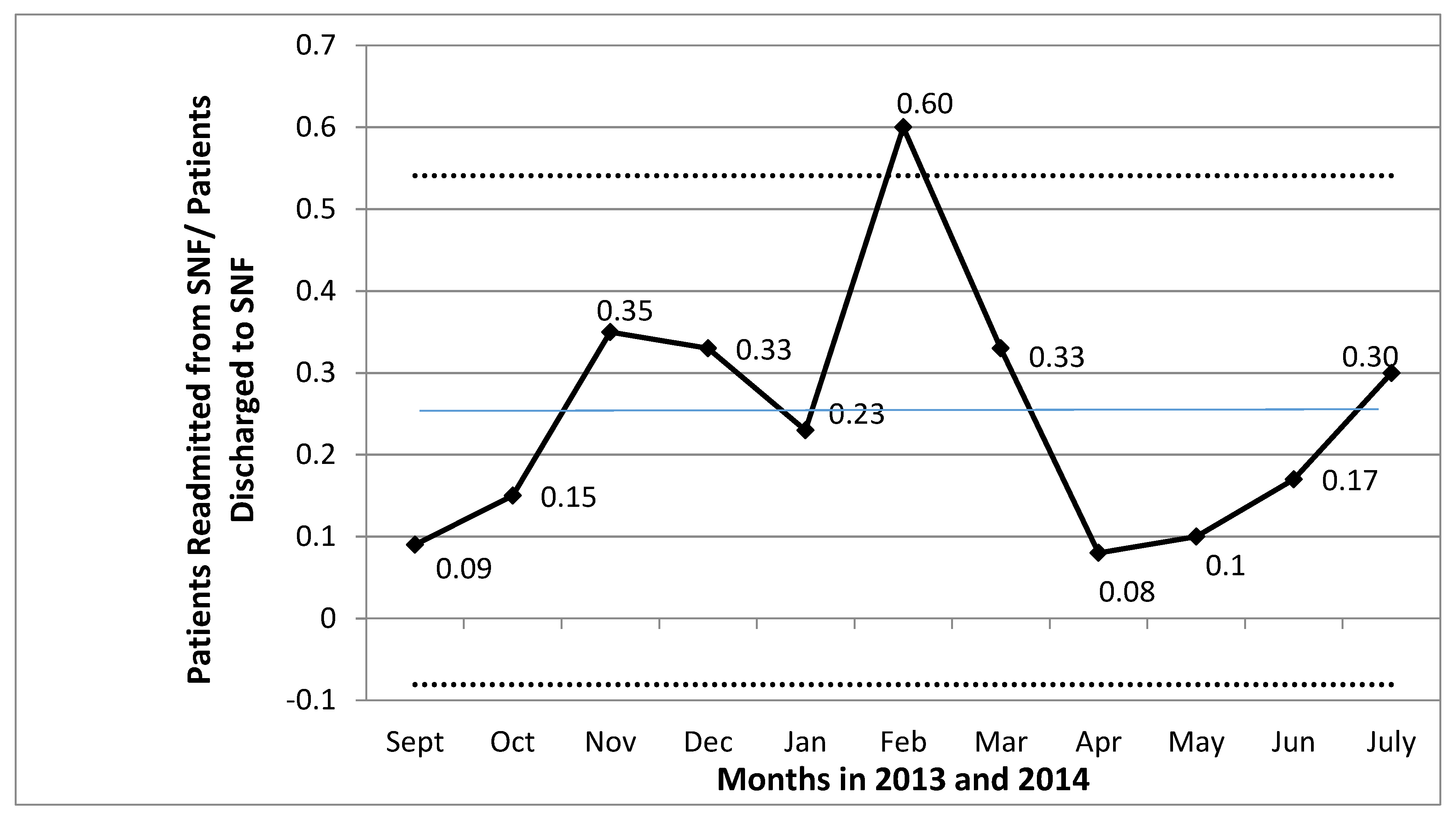
3.4. Readmission Rate
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dobrzanska, L.; Newell, R. Readmissions: A primary care examination of reasons for readmission of older people and possible readmission risk factors. J. Clin. Nurs. 2006, 15, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Jencks, S.F.; Williams, M.V.; Coleman, E.A. Rehospitalizations among Patients in the Medicare Fee-for-Service Program. N. Engl. J. Med. 2009, 360, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Boyd, C.M.; Landefeld, C.S.; Counsell, S.R.; Palmer, R.M.; Fortinsky, R.H.; Kresevic, D.; Burant, C.; Covinsky, K.E. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J. Am. Geriatr. Soc. 2008, 56, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Hsu, J.; McWilliams, J.M. Patient Characteristics and Differences in Hospital Readmission Rates. J. AMA Intern. Med. 2015, 175, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Hess, E.; Baron, A.E.; Levy, C.; Donze, J.D. Predicting Potential Adverse Events During a Skilled Nursing Facility Stay: A Skilled Nursing Facility Prognosis Score. J. Am. Geriatr. Soc. 2018, 66, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Intrator, O.; Feng, Z.; Grabowski, D.C. The revolving door of rehospitalization from skilled nursing facilities. Health Aff. (Millwood) 2010, 29, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Branch, L.G.; Bulat, T.; Vyas, B.B.; Roever, C.P. Influence of a Transitional Care Clinic on Subsequent 30-Day Hospitalizations and Emergency Department Visits in Individuals Discharged from a Skilled Nursing Facility. J. Am. Geriatr. Soc. 2013, 61, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Prescott, H.C. Variation in Postsepsis Readmission Patterns: A Cohort Study of Veterans Affairs Beneficiaries. Annals Amer. Thoracic Soc. 2017, 14, 230–237. [Google Scholar]
- Fabbietti, P.; Di Stefano, G.; Moresi, R.; Cassetta, L.; Di Rosa, M.; Fimognari, F.; Bambara, V.; Ruotolo, G.; Castagna, A.; Ruberto, C.; et al. Impact of potentially inappropriate medications and polypharmacy on 3-month readmission among older patients discharged from acute care hospital: A prospective study. Aging Clin. Exp. Res. 2018, 30, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Rosted, E.; Schultz, M.; Sanders, S. Frailty and polypharmacy in elderly patients are associated with a high readmission risk. Danish Med. J. 2016, 63, A5274. [Google Scholar]
- Sganga, F.; Landi, F.; Ruggiero, C.; Corsonello, A.; Vetrano, D.L.; Lattanzio, F.; Cherubini, A.; Bernabei, R.; Onder, G. Polypharmacy and health outcomes among older adults discharged from hospital: Results from the CRIME study. Geriatr. Gerontol. Int. 2015, 15, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Morandi, A.; Bellelli, G.; Vasilevskis, E.E.; Turco, R.; Guerini, F.; Torpilliesi, T.; Speciale, S.; Emiliani, V.; Gentile, S.; Schnelle, J.; et al. Predictors of rehospitalization among elderly patients admitted to a rehabilitation hospital: The role of polypharmacy, functional status, and length of stay. J. Am. Med. Dir. Assoc. 2013, 14, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Valencia, M.; Izquierdo, M.; Malafarina, V.; Alonso-Renedo, J.; Gonzalez-Glaria, B.; Larrayoz-Sola, B.; Monforte-Gasque, M.P.; Latasa-Zamalloa, P.; Martinez-Velilla, N. Impact of hospitalization in an acute geriatric unit on polypharmacy and potentially inappropriate prescriptions: A retrospective study. Geriatr. Gerontol Int. 2017, 17, 2354–2360. [Google Scholar] [CrossRef] [PubMed]
- Poudel, A.; Peel, N.M.; Nissen, L.M.; Mitchell, C.A.; Gray, L.C.; Hubbard, R.E. Adverse Outcomes in Relation to Polypharmacy in Robust and Frail Older Hospital Patients. J. Am. Med. Dir. Assoc. 2016, 17, e9–e767. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.P.; Hirdes, J.P.; Heckman, G.A.; Dey, A.B.; Jonsson, P.V.; Lakhan, P.; Ljunggren, G.; Singler, K.; Sjostrand, F.; Swoboda, W.; et al. Geriatric syndromes predict postdischarge outcomes among older emergency department patients: Findings from the interRAI Multinational Emergency Department Study. Acad. Emerg. Med. 2014, 21, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric syndromes: Clinical, research and policy implications of a core geriatric concept. J. Am. Geriatr. Soc. 2007, 55, 780. [Google Scholar] [CrossRef] [PubMed]
- Lakhan, P.; Jones, M.; Wilson, A.; Courtney, M.; Hirdes, J.; Gray, L.C. A prospective cohort study of geriatric syndromes among older medical patients admitted to acute care hospitals. J. Am. Geriatr. Soc. 2011, 59, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.P.; Vasilevskis, E.E.; Saraf, A.A.; Jacobsen, J.M.; Kripalani, S.; Mixon, A.S.; Schnelle, J.F.; Simmons, S.F. Geriatric Syndromes in Hospitalized Older Adults Discharged to Skilled Nursing Facilities. J. Am. Geriatr. Soc. 2016, 64, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Graham, J.E.; Lin, Y.-L.; Goodwin, J.S.; Bettger, J.P.; Deutsch, A.; Ottenbacher, K.J. Motor and cognitive functional status are associated with 30-day unplanned rehospitalization following post-acute care in Medicare fee-for-service beneficiaries. J. Gen. Intern. Med. 2016, 31, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Ayatollahi, Y.; Liu, X.; Namazi, A.; Jaradat, M.; Yamashita, T.; Shen, J.J.; Lee, Y.J.; Upadhyay, S.; Kim, S.J.; Yoo, J.W. Early Readmission Risk Identification for Hospitalized Older Adults with Decompensated Heart Failure. Res. Gerontol. Nursing 2018, 11, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Forsyth, D.R.; Wilson, K.J.; Cameron, E.; Wallis, S.; Biram, R.; Keevil, V. The Association of Geriatric Syndromes with Hospital Outcomes. J. Hosp. Med. 2017, 12, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, E.R.; Cafiero, A.C.; Hanlon, J.T. Polypharmacy in elderly patients. Am. J. Geriatr. Pharmacother. 2007, 5, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Fulton, M.M.; Allen, E.R. Polypharmacy in the elderly: A literature review. J. Amer. Acad. Nurse Practitioners 2005, 17, 123–132. [Google Scholar] [CrossRef]
- Hanlon, J.T.; Pieper, C.F.; Hajjar, E.R.; Sloane, R.J.; Lindblad, C.I.; Ruby, C.M.; Schmader, K.E. Incidence and predictors of all and preventable adverse drug reactions in frail elderly persons after hospital stay. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Col, N.; Fanale, J.E.; Kronholm, P. The role of medication noncompliance and adverse drug reactions in hospitalizations of the elderly. Arch. Intern. Med. 1990, 150, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Steinman, M.A.; Lund, B.C.; Miao, Y.; Boscardin, W.J.; Kaboli, P.J. Geriatric conditions, medication use, and risk of adverse drug events in a predominantly male, older veteran population. J. Am. Geriatr. Soc. 2011, 59, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Kripalani, S.; Jackson, A.T.; Schnipper, J.L.; Coleman, E.A. Promoting effective transitions of care at hospital discharge: A review of key issues for hospitalists. J. Hosp. Med. 2007, 2, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Raval, A.D.; Zhou, S.; Wei, W.; Bhattacharjee, S.; Miao, R.; Sambamoorthi, U. 30-Day Readmission Among Elderly Medicare Beneficiaries with Type 2 Diabetes. Pop. Health Manag. 2015, 18, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Saraf, A.A.; Petersen, A.W.; Simmons, S.F.; Schnelle, J.F.; Bell, S.P.; Kripalani, S.; Myers, A.P.; Mixon, A.S.; Long, E.A.; Jacobsen, J.M.; et al. Medications associated with geriatric syndromes and their prevalence in older hospitalized adults discharged to skilled nursing facilities. J. Hosp. Med. 2016, 11, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Qual. Saf. 2016, 25, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Vasilevskis, E.E.; Ouslander, J.G.; Mixon, A.S.; Bell, S.P.; Jacobsen, J.M.; Saraf, A.A.; Markley, D.; Sponsler, K.C.; Shutes, J.; Long, E.A.; et al. Potentially Avoidable Readmissions of Patients Discharged to Post-Acute Care: Perspectives of Hospital and Skilled Nursing Facility Staff. J. Am. Geriatr. Soc. 2017, 65, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare & Medicaid Services MDS 3.0 RAI Manual. Available online: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/MDS30RAIManual.html (accessed on 28 May 2018).
- Saliba, D.; Buchanan, J.; Edelen, M.O.; Streim, J.; Ouslander, J.; Berlowitz, D.; Chodosh, J. MDS 3.0: Brief interview for mental status. J. Am. Med. Dir. Assoc. 2012, 13, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Chodosh, J.; Edelen, M.O.; Buchanan, J.L.; Yosef, J.A.; Ouslander, J.G.; Berlowitz, D.R.; Streim, J.E.; Saliba, D. Nursing home assessment of cognitive impairment: Development and testing of a brief instrument of mental status. J. Am. Geriatr. Soc. 2008, 56, 2069–2075. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Wilson, A.; Vasilevskis, E.E.; Shintani, A.; Schnelle, J.F.; Dittus, R.S.; Graves, A.J.; Storrow, A.B.; Shuster, J.; Ely, E.W. Diagnosing delirium in older emergency department patients: Validity and reliability of the delirium triage screen and the brief confusion assessment method. Ann. Emerg. Med. 2013, 62, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Kripalani, S.; Vasilevskis, E.E.; Schnipper, J.L. Moving beyond readmission penalties: Creating an ideal process to improve transitional care. J. Hosp. Med. 2013, 8, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.G. Control charts 101: A guide to health care applications. Qual. Manag. Health Care 2001, 9, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Cumming, R.G.; Handelsman, D.J.; McLachlan, A.J.; Abernethy, D.R.; Banks, E.; Le Couteur, D.G. High-risk prescribing and incidence of frailty among older community-dwelling men. Clin. Pharmacol. Ther. 2012, 91, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Simmons, S.F.; Bell, S.; Saraf, A.A.; Coelho, C.S.; Long, E.A.; Jacobsen, J.M.; Schnelle, J.F.; Vasilevskis, E.E. Stability of Geriatric Syndromes in Hospitalized Medicare Beneficiaries Discharged to Skilled Nursing Facilities. J. Am. Geriatr. Soc. 2016, 64, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Society of Hospital Medicine. Better Outcomes for Older Adults through Safe Transitions (BOOST). Available online: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/html_CC/project_boost_background.cfm (accessed on 2 April 2009).



{kind=link}
{kind=link}
| Demographics | N = 134 |
|---|---|
| Age, Mean ± SD | 73.9 ± 10.2 |
| Sex (Male) | 96.3% |
| Race | |
| White | 85.7% |
| Black | 14.3% |
| Hospital length of stay in days | |
| Mean ± SD | 14.6 ± 10.3 |
| Median | 11 |
| Total number of medications at hospital discharge *, Mean ± SD | 14.7 ± 5.3 |
| Geriatric Syndromes | Prevalence N = 134 1 | Medications Associated with Geriatric Syndromes (MAGS) 2 N = 25 | |
|---|---|---|---|
| Mean Number of MAGS ± SD | Proportion with ≥1 MAGS | ||
| Cognitive Impairment (Brief Interview for Mental Status, BIMS ≤ 12) | 38.5% (45/117) | 1.76 ± 1.13 | 88% |
| Delirium (Positive Brief Confusion Assessment Method, BCAM) | 10.1% (13/129) | 1.35 ± 1.11 | 84% |
| Probable Depression (Geriatric Depression Scale five-Item, GDS ≥ 2) | 41.1% (44/107) | 1.72 ± 1.34 | 80% |
| Incontinence (bowel and/or bladder) | 39.6% (44/111) | 1.57 ± 1.00 | 86% |
| Unintentional Weight Loss (in last 1 month or during hospitalization) | 40.6% (28/69) | 0.36 ± 0.64 | 28% |
| Moderate to Severe Pain (≥4 on a 0–10 rating scale) | 23.7% (23/97) | N/A | N/A |
| History of Falls (in last 3 months) | 61.7% (82/133) | 5.08 ± 2.34 | 100% |
| Pressure Ulcers (at any point during hospitalization) | 32.3% (43/133) | N/A | N/A |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mixon, A.S.; Yeh, V.M.; Simmons, S.; Powers, J.; Ely, E.W.; Schnelle, J.; Vasilevskis, E.E. Improving Care Transitions for Hospitalized Veterans Discharged to Skilled Nursing Facilities: A Focus on Polypharmacy and Geriatric Syndromes. Geriatrics 2019, 4, 19. https://doi.org/10.3390/geriatrics4010019
Mixon AS, Yeh VM, Simmons S, Powers J, Ely EW, Schnelle J, Vasilevskis EE. Improving Care Transitions for Hospitalized Veterans Discharged to Skilled Nursing Facilities: A Focus on Polypharmacy and Geriatric Syndromes. Geriatrics. 2019; 4(1):19. https://doi.org/10.3390/geriatrics4010019
Chicago/Turabian StyleMixon, Amanda S., Vivian M. Yeh, Sandra Simmons, James Powers, Eugene Wesley Ely, John Schnelle, and Eduard E. Vasilevskis. 2019. "Improving Care Transitions for Hospitalized Veterans Discharged to Skilled Nursing Facilities: A Focus on Polypharmacy and Geriatric Syndromes" Geriatrics 4, no. 1: 19. https://doi.org/10.3390/geriatrics4010019
APA StyleMixon, A. S., Yeh, V. M., Simmons, S., Powers, J., Ely, E. W., Schnelle, J., & Vasilevskis, E. E. (2019). Improving Care Transitions for Hospitalized Veterans Discharged to Skilled Nursing Facilities: A Focus on Polypharmacy and Geriatric Syndromes. Geriatrics, 4(1), 19. https://doi.org/10.3390/geriatrics4010019