1. Introduction
The emergency department (ED) setting can be an extremely challenging environment for vulnerable patients, especially those with advanced age, baseline cognitive impairment, functional limitations, or frailty. While the ED is the traditional entry point into the healthcare system providing essential acute emergency medical care, it is often not an ideal care environment for many older, vulnerable patients. Older adults tend to have greater complex medical co-morbidities, higher illness severity, and limited cognitive and functional reserves to overcome the stress of an acute illness and a hospitalization [
1,
2,
3,
4].
While the reasons for presenting to the ED are varied, there is a growing recognition that for older adults an ED visit is a critical opportunity to identify and intervene upon unique care needs in addition to the acute illness [
2,
3,
4,
5].
1.1. Geriatric Emergency Department
The traditional model of ED care prioritizes efficient triage and treatment for an acute illness or trauma [
4]. This model of rapid ED care does not afford time often required to identify and address the complexities of frail and vulnerable older adult patients with multiple chronic conditions complicated by functional, cognitive, and psychosocial challenges [
6]. Patients with these multiple co-morbidities, however, have higher disease and symptom burden which must be addressed to ensure successful care of the acute medical condition. Comprehensive evaluations and disposition plans that account for the functional, cognitive, and psychosocial issues that impact health care-related quality of life are essential to the successful management of the acute medical condition [
6,
7].
Recognizing the need for a better approach to older patients in the emergency room, Mount Sinai Hospital opened a dedicated Geriatric Emergency Department (GED) in 2012, transforming the way emergency care is provided for older adults. Taking advantage of a strong geriatrics presence in the hospital, and enthusiastic buy-in from the Emergency Medicine Department, this innovative GED model included universal and focused assessments on common geriatric syndromes and daily comprehensive interdisciplinary team (IDT) bedside discussions for high-risk patients, essentially replicating an Acute Care for Elderly (ACE) model. The typical ACE model of care emphasizes patient centered care, nurse driven prevention protocols, frequent interdisciplinary team rounds addressing common geriatric syndromes, and early discharge planning, and anticipation of care needs [
8,
9]. At the core of this model is an IDT, working together to improve care for older ED patients and impact care and outcome trajectories [
10,
11].
1.2. Securing Grant Support for Demonstration Project
Subsequent to the opening of the Geriatric ED, Mount Sinai received a Center for Medicare and Medicaid Innovation award as part of a clinical implementation demonstration program called GEDIWISE (Geriatric Emergency Department Innovations in Care through Workforce, Informatics, and Structural Enhancements) in collaboration with St Joseph’s Regional Medical Center in New Jersey and Northwestern Memorial Hospital in Illinois [
12,
13]. The three-year GEDI WISE program focused on implementing and demonstrating a new model of geriatric emergency care by providing a broader and more comprehensive range of services, assessments, and care coordination to address the complex needs of older adults in the ED. The goal of the GEDI WISE program was to provide a patient centered comprehensive approach to care, reduce avoidable inpatient hospital admissions and return visits to the ED. The program was a paradigm shift in the treatment and approach for older adults in EDs who are at risk for admission to the hospital [
12].
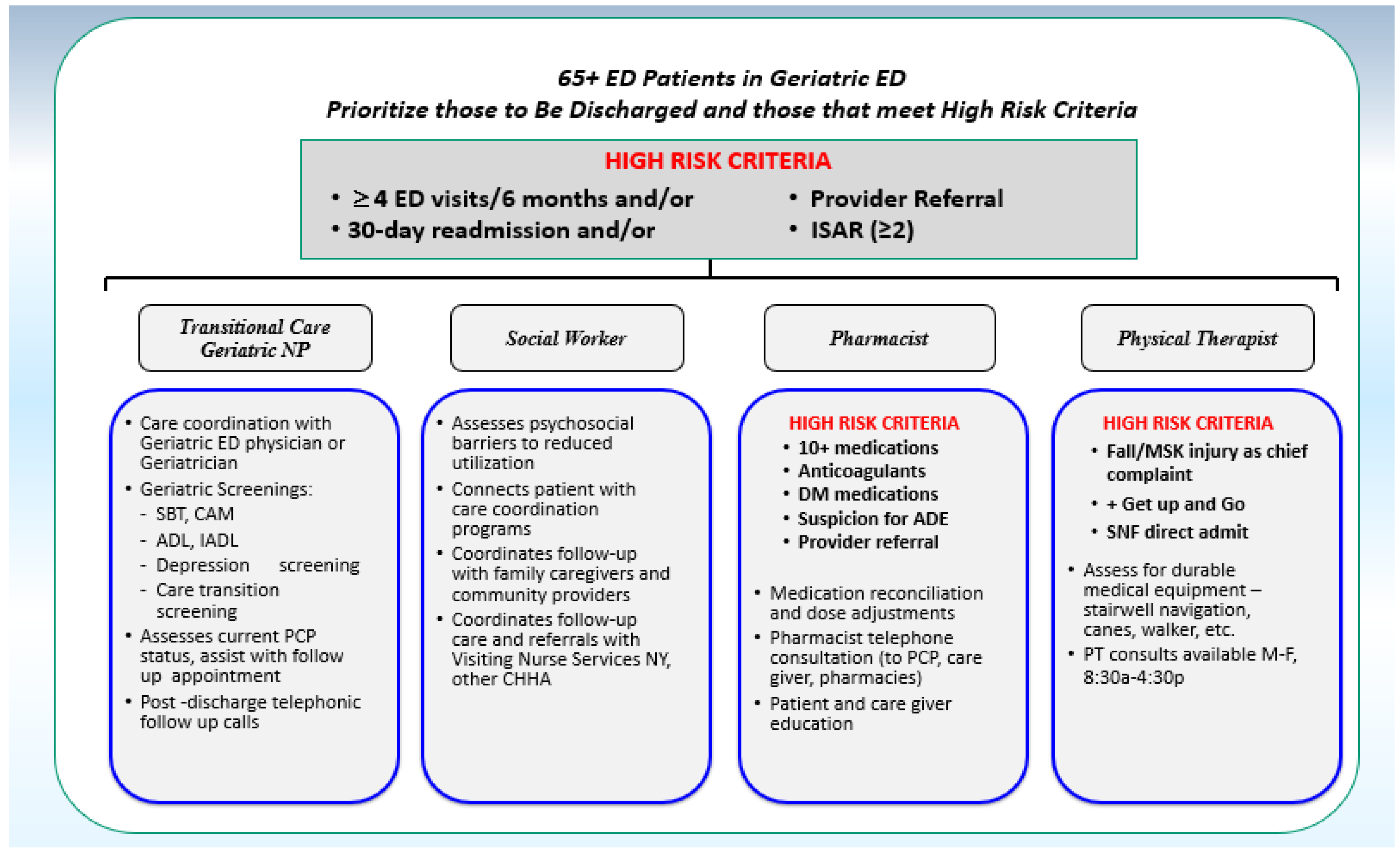
The GEDI WISE program provided additional resources specific to unique needs of older adults, improved staffing, and geriatric training for staff dedicated to enhancing geriatric care in the ED. The program supported and expanded the workforce to provide comprehensive evaluations to older patients in the ED facilitating critical decisions regarding hospital admission or ED discharge for complex cases. The geriatric IDT, including a transitional care nurse, social workers, pharmacists, and physical therapists, as shown in
Figure 1, utilized algorithms of patient care and clinical care protocols tailored to treating older patients in the ED. An intervention design was created that could be used to explore ‘proof of concept’ of this model.
In this paper we will describe the creation of an ACE model in a Geriatric Emergency Department (including expanded IDT roles, focused geriatric assessments, clinical work flow) and how this model was implemented as part of the GEDI WISE intervention at The Mount Sinai Hospital. Preliminary program outcomes will be described. Previous patient outcome data has been published on the transitional care nursing role and social work intervention.
2. Methods
2.1. Setting
Mount Sinai Hospital is a 1171 bed tertiary- and quaternary-care facility in New York City. The Mount Sinai Hospital Department of Emergency Medicine has an annual visit volume of 100,000 patients a year; those 65 years or older account for more than 15% of ED visits. Mount Sinai Hospital is also home to the Brookdale Department of Geriatrics and Palliative Medicine, one of the first freestanding academic geriatric departments in the country.
2.2. Study Population
To assess impact of this Geriatric ED IDT intervention on programmatic as well as patient care outcomes, we conducted a retrospective chart review of patients 65 years and older who presented to the Mount Sinai Hospital Emergency Department (Mount Sinai ED) in New York City, New York between 1 January 2013 and 31 December 2015. During the study period there were 48,268 patient encounters (23,381 unique patients, 65 years and older) in the Mount Sinai ED. Of this cohort, 22,315 (12,328 unique patients, 65 years and older) met high-risk criteria as defined by Identification of Seniors at Risk (ISAR) ≥ 2. The study population consisted of the 6050 patients that received the intervention during the hours of the IDT staffing in the Mount Sinai ED. As seen in
Table 1, 64.74% were female; 64.41% were 75 years of age or older; 91.04% had an Emergency Severity Index (ESI) score of 2 or 3 and 50.31% had an ISAR score ≥ 2.
2.3. Program Description
Mount Sinai’s GEDI WISE program essentially replicated a Geriatric ED ACE model with the goal of reframing the way care is provided for elders in the ED. GEDI WISE expanded an integrated and collaborative IDT workforce, and provided enhanced informatics to support focused geriatric assessments that improved clinical decision-making. There are four basic components introduced in this ACE model for the ED:
2.4. Dedicated Geriatric IDT Members and Roles
The Geriatric ED was staffed with an inter-professional team which included an emergency physician, emergency medicine residents, physician assistants, ED nurses, a transitional care geriatric nurse (TCN) and/or geriatric nurse practitioner (NP), social worker (SW), pharmacist (RX), physical therapist (PT), a consulting geriatrician and ED palliative care consultant, as shown in
Table 2 and
Table 3. The full staffing model and full time equivalent (FTE) support essentially included reframing and expanding the roles of the existing IDT members to optimize the care of older adults in the ED and the addition of a new clinical role for a transitional care nurse. All providers received additional training by the geriatrician in core geriatric education principles to meet the needs of this population. The role of the TCN/NP was to provide more focused geriatric assessments in the ED and facilitate the coordination required for complex transitional care planning of older adults being discharged from the ED. The role of PT was new to the ED, but therapists were able to incorporate standard assessments used in the inpatient hospital setting for evaluations in the ED.
2.5. Geriatric Triage Assessments
Optimal geriatric care frequently requires a Comprehensive Geriatric Assessment (CGA) to address the medical, psychosocial, and functional complexities of this vulnerable patient population [
6]. While CGAs can be time consuming, they are a critically important aspect of a coordinated care plan that aims to maximize overall health and improve patient outcomes. Assessments of older adults for geriatric specific syndromes were integrated into the clinical work flow of ED nurses at the point of triage and also during the primary nursing assessment. Enhanced electronic health record (EHR) support with discipline specific documentation templates for TCN, SW, RX, and PT helped capture these comprehensive assessments related to geriatric syndromes, cognitive and functional assessments, psycho social needs, and medication management. Patients over the age of 65 were screened with the Identification for Seniors at Risk (ISAR) score [
15,
16], Timed Get up and Go Fall risk assessment [
17], and the brief Confusion Assessment Method (bCAM) for delirium [
18]. Patients with ISAR score >2, fall risk, multiple prior ED visits, hospital admissions were considered to have met high-risk criteria.
2.6. Discipline Specific Geriatric Assessments for the ED
Patients who met high-risk criteria would subsequently receive IDT consultation through a collaborative identification process involving various disciplines (SW, PT, pharmacy, and nursing) and Geriatric Emergency Medicine providers. Additional criteria guided the specific IDT consults to assure focus on the highest risk patients, and to maximize impact and improve patient outcomes, as shown in
Figure 1 and
Table 3. Geriatric TCN/NP and social work assessments, for example, were frequently performed on high-risk patients prior to either hospital admission or discharge designation, and integrated recommendations from the ED provider’s clinical workup into the admission or discharge plans. The transitional care nurses (TCN) perform focused assessments including cognitive and functional screens to assist in the evaluation of the complex, older adults presenting with change in mental status, falls, functional decline, or delirium in the setting of the acute illness. They are equipped to make recommendations to focus further workup in ED, transitions of care, and evaluations during hospitalization if admitted. For patients who were discharged, the TCN helps to improve communication and facilitate care coordination across practice sites, ensure appropriate outpatient services to reduce unnecessary utilization, and assist with safe discharge and transition planning.
Similarly, the role of the SW in the ED setting is versatile and encompasses a multitude of complex psychosocial needs of this population. The social worker can help elderly individuals with psychosocial, medical, and/or financial challenges they may experience. As part of the care team, they are available to assist with assessments, offer counseling services which often deal with end-of-life issues, bereavement, elder abuse, and other concerns common in older adults. They are helpful identifying community resources for meals, transportation, and applying for medical benefits and other resources available to elders.
Pharmacy (RX) and physical therapy (PT) consults, on the other hand, had narrower criteria that focused their assessment primarily on high-risk patients who were to be discharged to home. For example, a pharmacy consult was triggered in patients taking 10 or more medications, or if their clinical presentation was associated with an adverse drug event (ADE). However, a pharmacy consult could also be triggered to guide real time treatment decisions after discussion during IDT rounds.
PT consults were triggered by a new fall, or musculoskeletal injury due to a fall, or to assess for a transition to a sub-acute rehabilitation facility. However, PT were also available to assess patients at the request of the ED team to ensure an evaluation for a safe discharge to home if needed. Geriatrician and palliative care providers were also consulted by the IDT clinical team for highest risk and complex cases when necessary. While the interdisciplinary team members created established criteria to guide assessments, consults could also be triggered simply by a recognized need that the patient could benefit from a more comprehensive evaluation. It was rare for assessments to be completed on patients who did not meet the need for an evaluation.
2.7. Incorporating the ACE Model into a Geriatric ED Clinical Work Flow
Clinical work flow is a crucial aspect of ED care. In an ED environment where efficiency and expedited workup is imperative, the IDT worked in parallel with the ED treatment team to identify complex clinical and psychosocial needs while assisting in the coordination of clinical evaluations and safe transitions for patients upon discharge from the ED. Patients received individual IDT consultations throughout the workday (8:00–20:00 Monday–Friday), and results were discussed with the entire team during designated IDT midday discussions. These IDT rounds were led by the emergency physician or geriatrician with the opportunity for all IDT members to present updates on cases and identify patients with specific issues requiring targeted consultations by the team. This dedicated time for daily rounds allowed the team members to collaborate and discuss high-risk cases, troubleshoot complex clinical and psychosocial issues, make use of inter-professional team members’ unique skill sets, develop comprehensive disposition plans with the goal of improving health care outcomes, intervene with community resources, and prevent avoidable admission. These discussions also provided a forum for inter-professional education, information exchange, and guidance on how to address common issues for future patients. The geriatric emergency provider was the point person for clinical issues or updates that came up after the IDT daily rounds and throughout the shift. Patients identified after the IDT rounds were discussed with individual consultants on an as-needed basis. Staff were encouraged to work collaboratively even after IDT rounds. All disciplines were available for consultations throughout the day.
2.8. Data Sources
Data on all ED visits at Mount Sinai Hospital between 1 January 2013 through 31 December 2015 were abstracted from the EPIC Electronic Medical Record and Mount Sinai Data Warehouse and included administrative and clinical data for all inpatient and ED visit encounters for patients 65 years and older.
2.9. IDT Consultation
Each encounter level consultation note entered by an interdisciplinary team member (i.e., TCN, SW, PT, pharmacist) was considered an indication of an assessment/intervention by the IDT during the ED visit encounter.
3. Results
There were 48,268 ED visit encounters during the study period made by 23,381 unique patients 65 years and older. Of the 22,315 who met high-risk criteria as defined by ISAR ≥ 2, 3321 (14.8%) of these received a GEDI WISE IDT consultation, representing 2606 unique patients. Of these, 1360 (40.90%) involved a geriatric RN/NP consultation, 2389 (71.9%) involved a social work consultation, 826 (24.8%) involved a pharmacy consultation, 616 (18.5%) involved a physical therapy consultation, and 82 (2.46%) involved consultations from all four disciplines (geriatric RN/NP, social work, pharmacy, and physical therapy), as shown in
Table 4. Official consultations from Geriatrics and Palliative Care were requested as needed.
3.1. Assessments by Transitional Care RN/NP
Previous studies have demonstrated that individual geriatric assessments completed by the transitional care NP were associated with lower risk of admission, but greater risk of a 72 h ED revisit. Risk of any admission within 30 days of the index ED visit also remained lower for TCN patients thus indicating these patients were safely discharged during the index ED visit [
19]. For patients being discharged from the ED, the transitional care RN or NP completed post-discharge phone calls to ensure proper follow up with outpatient providers, consultants, and ensure seamless care coordination after an ED visit.
3.2. Assessments by Social Work
The most commonly requested assessment for older adults in the ED was an evaluation by the social worker. Seventy percent of the study population had contact with a SW, however the interventions varied in intensity. The majority of interventions facilitated safe transitions to home for patients who were unlikely to be admitted (i.e., home safety assessment, transportation assistance, or access to visiting nurses and community resources) [
20]. The SW assessment was also crucial in exploring the patient’s psychosocial needs and connecting patients with the proper community resources so patients could safely return home and avoid unnecessary admissions.
3.3. Assessments by Pharmacy
Older adults with multiple co-morbidities, are more likely to be prescribed a greater number of medications and hence at greater risk for adverse drug interactions. Pharmacy consults in the study were initiated in two ways: (1) to help facilitate a safe discharge especially in patients with polypharmacy or taking a high-risk medication; or (2) pharmacists also assessed admitted patients who were boarding in the ED. As a result, there were a disproportionate number of consults by pharmacy associated with admissions, as they frequently completed medication reconciliation for the admitted patients.
3.4. Assessments by Physical Therapy
Patients who met criteria for PT evaluation were screened for home safety, the need for assistive devices, or assistance in safe transition planning. In addition, PT evaluation facilitated transitions to Skilled Nursing Facilities (SNF) or sub-acute rehabilitation (SAR) from the ED for eligible patients. Evaluations by PT helped ensure safe disposition plans for patients with functional limitations. Despite PT evaluation in the ED, however, many SNF or SAR eligible patients were admitted if they required a 72 h hospitalization to satisfy the Centers for Medicare and Medicaid Services (CMS) requirements.
3.5. Assessments by More Than One Discipline
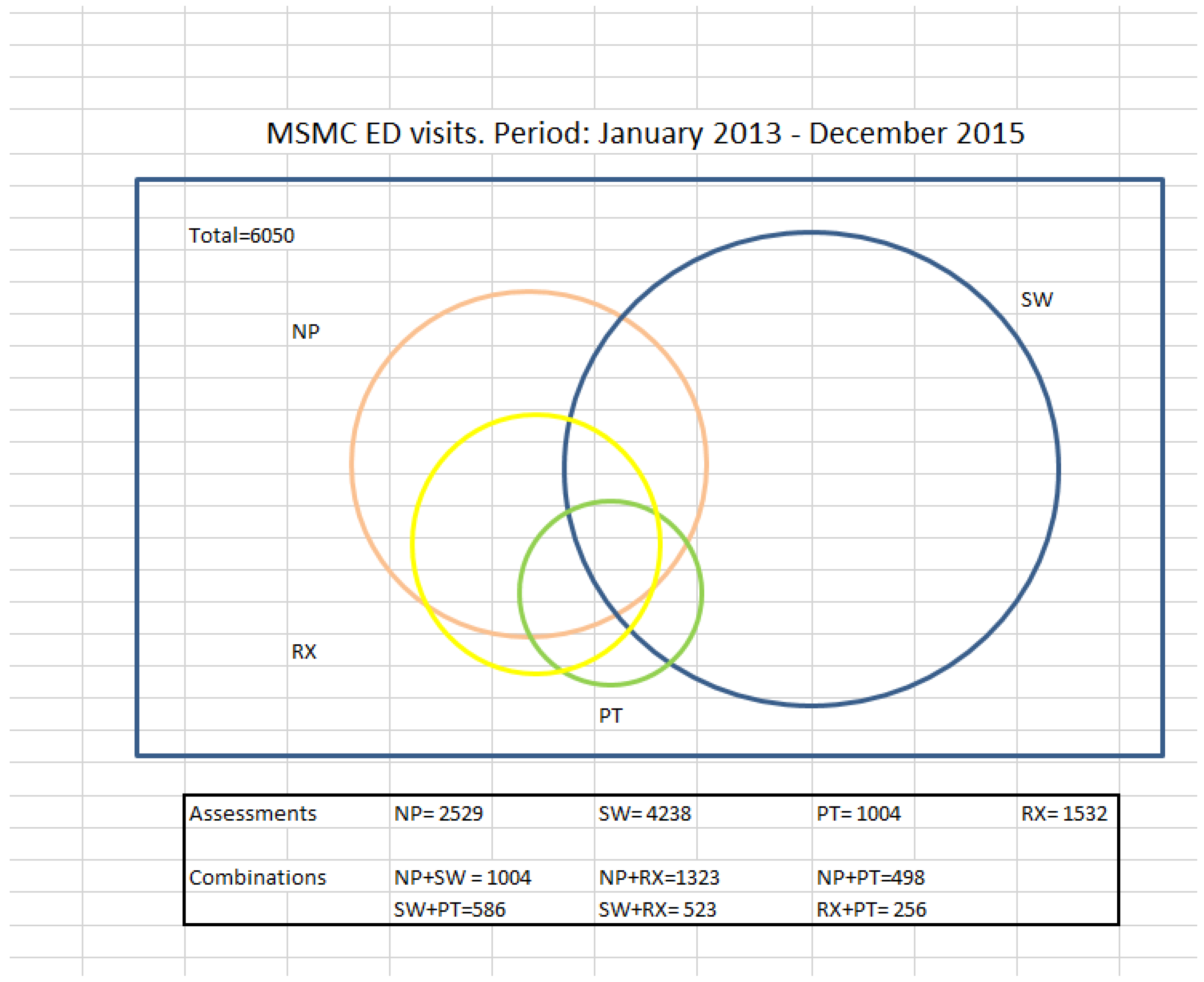
Many individuals had multiple consultations during the same ED visit. The most common combinations of shared assessment included NP and pharmacist or NP and SW, as shown in
Figure 2. Team members could decide to see patients together, or individually, and then make final recommendations once information was gathered by the various disciplines. Furthermore, clinical decision-making and care planning were enhanced by the multiple sources of evaluation.
Figure 2 highlights the overlap in collaborative assessments per discipline.
3.6. Additional Criteria Guided the IDT Consults
In order to focus interventions on the highest risk patients to maximize impact and improve patient outcomes, specific criteria were created to trigger consults. As described above, geriatric RN/NP and social work assessments were broader in focus and performed primarily on high-risk patients prior to admission or discharge designation. Pharmacy and physical therapy consults, on the other hand, had a narrower and specific focus, assessing only high-risk patients that were confirmed for discharge to home, as shown in
Figure 1,
Table 2 and
Table 3. While established criteria were created to guide the assessments by the interdisciplinary team members, consultations could be requested by a clinical provider simply by a recognized need that the patient could benefit from a more comprehensive evaluation. As seen in
Table 4, approximately 6–30% of IDT assessments were completed on patients who did not necessarily meet sole criteria of ISAR ≥ 2, but met criteria for a discipline-specific intervention.
3.7. Variation in Staffing and Community Resources
Staffing resources varied throughout the study period. The full staffing model could not be fully matched to patient arrivals at the Mount Sinai ED which receives patients 24 h a day, 7 days a week, 365 days per year. The IDT staffing hours were designed to match ED arrival patterns of patients >65 years old as well as the availability of community resources (i.e., Skilled Nursing Facilities, visiting nurse, and other community resources) for coordination and admission, typically Monday through Friday 9:00–16:00. The staffing and hours in this model included: geriatric RN/NP 8:00–20:00, SW 8:00–20:00 onsite full coverage, 20:00–8:00 offsite SW limited coverage for transportation and elder abuse cases. Physical therapy provided 8:00–16:00 coverage and a pharmacist available for 8:00–20:00 coverage. Geriatric medicine and palliative consults were available throughout the day as needed, for patients who were not in ED during the time of daily IDT rounds.
4. Discussion
For older adults, a visit to the ED and a subsequent hospitalization is considered a sentinel event, often associated with a decline in the patient’s health status and quality of life. An admission to the hospital should therefore be prevented whenever possible for this population to avoid the greater risk for adverse outcomes, such as delirium, iatrogenic infections, medication errors, adverse drug events, and functional decline, which in turn lead to more complex transitions to post-acute care, rehabilitation, or nursing home placement [
6,
21].
Older adults who present to an emergency department (ED) generally have more complex medical conditions with complicated care needs and are at high risk for preventable adverse outcomes during their ED visit. The ED is uniquely positioned to alter care trajectories and prevent complications that significantly affect the patients’ outcomes. The addition of an interdisciplinary team and enhanced geriatric assessments in the ED can guide clinical decisions and prevent avoidable hospital admissions and impact care outcomes for this vulnerable population.
The ACE model that we describe here addresses a growing need for older adults in the ED. Our project demonstrated the feasibility of implementing principles of an ACE practice in an emergency department setting. Integrating geriatric assessments into the ED clinical work flow to identify specific geriatric syndromes, such as dementia, delirium, functional status, frailty, or polypharmacy, allows all providers to address significant patient care needs and make better clinical decisions. Incorporating an interdisciplinary team model into the Geriatric Emergency Department also allows providers to better address the potential gaps in the care of older patients, specifically in cognitive assessment, medication management, and safe transitional care planning [
22].
In this care model, the focus is on identifying patients who have the highest needs, reducing avoidable admissions, and decreasing ED revisits by developing safe, realistic, and seamlessly coordinated discharge plans. In order to implement this model in a busy ED setting, IDT assessments and consultations were prioritized for patients who met specific criteria and could potentially be discharged from the ED. Social work evaluations were the most commonly requested interventions, followed by NP, pharmacist, and then PT. This was most likely due to the fact the SW and NP assessments covered a broader scope of issues, compared to the more limited criteria for pharmacy and PT consultation evaluations.
The key aspect of programmatic implementation included securing support from hospital leadership. Additional staffing underwritten by a unique grant funding opportunity was critically important and allowed the ED to leverage and enhance existing resources with augmentation in staffing, building of care protocols, assessment templates, and criteria to identify at risk patients, and geriatric-focused training and education. This model illustrates how the realignment and addition of dedicated resources with an interdisciplinary team can enhance the care for older adults in the ED.
The collaboration by IDT disciplines allows for more comprehensive evaluation to guide informed clinical decision-making and better align with quality of care, patient safety, and health system priorities. By focusing on the patients who have the highest need these programs are able to develop safer, feasible, and seamlessly coordinated care plans for patients that could be discharged and reduce their risk for hospital admission.
5. Conclusions
This innovative model of geriatric emergency care we describe reframes the traditional model of ED care to address these unique care needs of older adults in the ED. In this model we were able to able to create clinical protocols to identify high risk older adults, incorporate IDT assessments to better guide clinical decision making, and facilitate transitional care after an ED visit.
Further publications from the GEDI-WISE team will review the impact of all aspects of this model on patient outcomes such as discharge dispositions, readmission rates, hospital LOS for those admitted, final post-acute care destination and cost savings. Analysis of these outcomes will identify which combinations of IDT interventions are most effective in improving emergency care for older adults.
The importance of this new approach to geriatric emergency care is already widely recognized. In 2014, the American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association and the Society for Academic Emergency Medicine created the Geriatric Emergency Department Guidelines with descriptions of requirements for structure, screening protocols, staff education and community resources to meet the criteria to qualify as a Geriatric Emergency Department [
22]. Subsequently, in January 2018, the American College of Emergency Physicians, with support from the Gary and Mary West Health Institute and the John A. Hartford Foundation, launched an accreditation program for geriatric emergency departments that have met certain quality standards [
23,
24,
25,
26]. In May 2018, The Mount Sinai Hospital received ACEP Geriatric Emergency Department accreditation, one of the first Level 1 GEDs in the United States.
Author Contributions
M.S., U.H., G.A., L.D.R., and the GEDI WISE Investigators conceived and designed the clinical care model U.H., and L.D.R. analyzed and interpreted the data; M.S., S.G., G.A., and U.H. wrote and edited the paper.
Funding
The GEDI WISE project described in the following presentation is supported by Grant 1C1CMS331055-01-00, Department of Health and Human Services, Centers for Medicare and Medicaid Services. Its contents are solely the responsibility of the author and have not been approved by DHHS or CMS.
Acknowledgments
The GEDI WISE Investigators include (in addition to the named authors) the following for their contributions to the implementation and clinical care of the GEDI WISE program: Cindy Amoko, Kevin Baumlin, Nicholas Genes, Corita R. Grudzen, Christine Hamilton, George Loo, Barbara Morano, Denise Nassisi, Gloria Nimo, Joanna M. Ortiz, Laura Rivera-Reyes, Jason Shapiro, Jeremy Sze, Carmen Vargas-Torres and Gary Winkel.
Conflicts of Interest
The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the result.
References
- Adams, J.G.; Gerson, L.W. A new model for Emergency care of Geriatric patients. Acad. Emerg. Med. 2003, 10, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Aminzadeh, F.; Dalziel, W.B. Older adults in the Emergency Department: A systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann. Emerg. Med. 2002, 39, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.; Morrison, R.S. The Geriatric Emergency Department. J. Am. Geriatr. Soc. 2007, 55, 1873–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaras, N.; Chevalley, T.; Samaras, D.; Gold, G. Older patients in the emergency department: A review. Ann. Emerg Med. 2010, 56, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.; McCaig, L.F.; Ashman, J.J. NCHS Emergency department visits by persons aged 65 and over: United States, 2009–2010. NCHS Data Brief. 2013, 130, 1–2018. [Google Scholar]
- Ellis, G.; Marshall, T.; Ritchie, C. Comprehensive geriatric assessment in the emergency department. Clin. Interv. Aging 2014, 9, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- McCabe, J.J.; Kennelly, S.P. Acute care of older patients in the emergency department: Strategies to improve patient outcomes. Open Access Emerg. Med. 2015, 7, 45–54. [Google Scholar] [PubMed]
- Flood, K.L.; MacLennan, P.A.; McGrew, D.; Green, D.; Dodd, C.; Brown, C.J. Effects of an Acute Care for Elders Unit on Costs and 30-Day Readmissions. JAMA Intern. Med. 2013, 173, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Steele, J. Current Evidence Regarding Models of Acute Hospitalized Geriatric Patients. Geriatr. Nurs. 2010, 31, 5331–5341. [Google Scholar] [CrossRef] [PubMed]
- Reeves, S.; Zwarenstein, M.; Goldman, J.; Barr, H.; Freeth, D.; Hammick, M.; Koppel, I. Interprofessional education: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Barnes, D.E.; Palmer, R.M.; Kresevic, D.M.; Fortinsky, R.H.; Kowal, J.; Chren, M.M.; Landefeld, C.S. Acute Care for Elders Units Produced Shorter Hospital Stays at Lower Cost While Maintaining Patients’ Functional Status. Health Aff. 2012. [Google Scholar] [CrossRef]
- Hwang, U.; Rosenberg, M.S.; Dresden, S.M. Geriatrics Emergency Department—The GEDI WISE Program. In Geriatrics Models of Care: Bringing “Best Practice” to an Aging America; Malone, M., Capezuti, E., Palmer, R.M., Eds.; Springer: New York, NY, USA, 2015. [Google Scholar]
- Centers for Medicare and Medicaid Innovation. Health Care Innovation Award Project Profiles. 2012. Available online: http://innovation.cms.gov/Files/x/HCIA-Project-Profiles.pdf (accessed on 18 August 2014).
- Emergency Severity Index (ESI): A Triage Tool for Emergency Departments. Available online: https://www.ahrq.gov/professionals/systems/hospital/esi/index.html (accessed on 12 July 2018).
- McCusker, J.; Bellavance, F.; Cardin, S.; Trepanier, S.; Verdon, J.; Ardman, O. Detection of older people at increased risk of adverse health outcomes after an emergency visit: The ISAR screening tool. J. Am. Geriatr. Soc. 1999, 47, 1229–1237. [Google Scholar] [CrossRef]
- Yao, J.; Fang, J.; Lou, Q.; Anderson, R.M. A systematic review of the identification of seniors at risk (ISAR) tool for the prediction of adverse outcome in elderly patients seen in the emergency department. Int. J. Clin. Exp. Med. 2015, 8, 4778–4786. [Google Scholar] [PubMed]
- Centers for Diease Control and Prevention (CDC). The Timed Up and Go (TUG) Test. Stopping Elderly Accidents Deaths & Injuries. Available online: http://www.cdc.gov/steadi/pdf/tug_test-a.pdf (accessed on 7 March 2016).
- Han, J.H.; Wilson, A.; Vasilevskis, E.E.; Shintani, A.; Schnelle, J.F.; Dittus, R.S.; Graves, A.J.; Storrow, A.B.; Shuster, J.; Ely, E.W. Diagnosing delirium in older emergency department patients: Validity and reliability of the Delirium Triage Screen and the Brief Confusion Assessment Method. Ann. Emerg. Med. 2013, 62, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.; Dresden, S.M.; Rosenberg, M.S.; Garrido, M.M.; Loo, G.; Sze, J.; Gravenor, S.; Courtney, D.M.; Zhu, C.W.; Vargas-Torres, C.; Grudzen, C.R.; Richardson, L.D. GEDI WISE Investigators. Geriatr. Emerg. Dep. Innov. Transit. Care Nurses Hosp. Use J. Am. Geriatr. Soc. 2018, 66, 459–466. [Google Scholar]
- Hamilton, C.; Ronda, L.; Hwang, U.; Abraham, G.; Baumlin, K.; Morano, B.; Nassisi, D.; Richardson, L. The Evolving Role of Geriatric Emergency Department Social Work in the Era of Health Care Reform. Soc. Work Health Care 2015, 54, 849–868. [Google Scholar] [CrossRef] [PubMed]
- Leff, B.; Burton, L.; Mader, S.L.; Naughton, B.; Burl, J.; Inouye, S.K.; Greenough, W.B.; Guido, S.; Langston, C.; Frick, K.D.; et al. Hospital at Home: Feasibility and Outcomes of a Program to Provide Hospital-Level Care at Home for Acutely Ill Older Patients. Ann. Intern. Med. 2005, 143, 798–808. [Google Scholar] [CrossRef] [PubMed]
- Terrell, K.M.; Hustey, F.M.; Hwang, U.; Gerson, L.W.; Wenger, N.S.; Miller, D.K. Quality indicators for geriatric emergency care. Acad. Emerg. Med. 2009, 16, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C.R.; Bromley, M.; Caterino, J.M.; Chun, A.; Gerson, L.W.; Greenspan, J.; Hwang, U.; John, D.P.; Lyons, W.L.; Platts-Mills, T.F.; Mortensen, B. Optimal older adults emergency care: Introducing multidisciplinary geriatric emergency department guidelines from the american college of emergency physicians, american geriatrics society, emergency nurses association, and society for academic emergency medicine. J. Am. Geriatr. Soc. 2014, 62, 1360–1363. [Google Scholar] [PubMed]
- Carpenter, C.; Hwang, U.; Biese, K.; Carter, D.; Hogan, T.; Karounos, M.; Malone, M.; Melady, D.; Rosen, A.; Rosenberg, M.; et al. ACEP Accredits Geriatric Emergency Care for Emergency Departments. Available online: https://www.acepnow.com/article/acep-accredits-geriatric-emergency-care-emergency-departments/2/ (accessed on 12 July 2018).
- American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association, Society for Academic Emergency Medicine. Geriatric Emergency Department Guidelines. Available online: https://www.acep.org/globalassets/uploads/uploaded-files/acep/clinical-a (accessed on 10 July 2018).
- American Geriatrics Society. Geriatrics Emergency Department Collaborative. Available online: https://www.americangeriatrics.org/programs/geriatrics-emergency-departm (accessed on 12 July 2018).
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}