Evaluation of a Combined HIV and Geriatrics Clinic for Older People Living with HIV: The Silver Clinic in Brighton, UK



Abstract
:1. Introduction
2. Methods
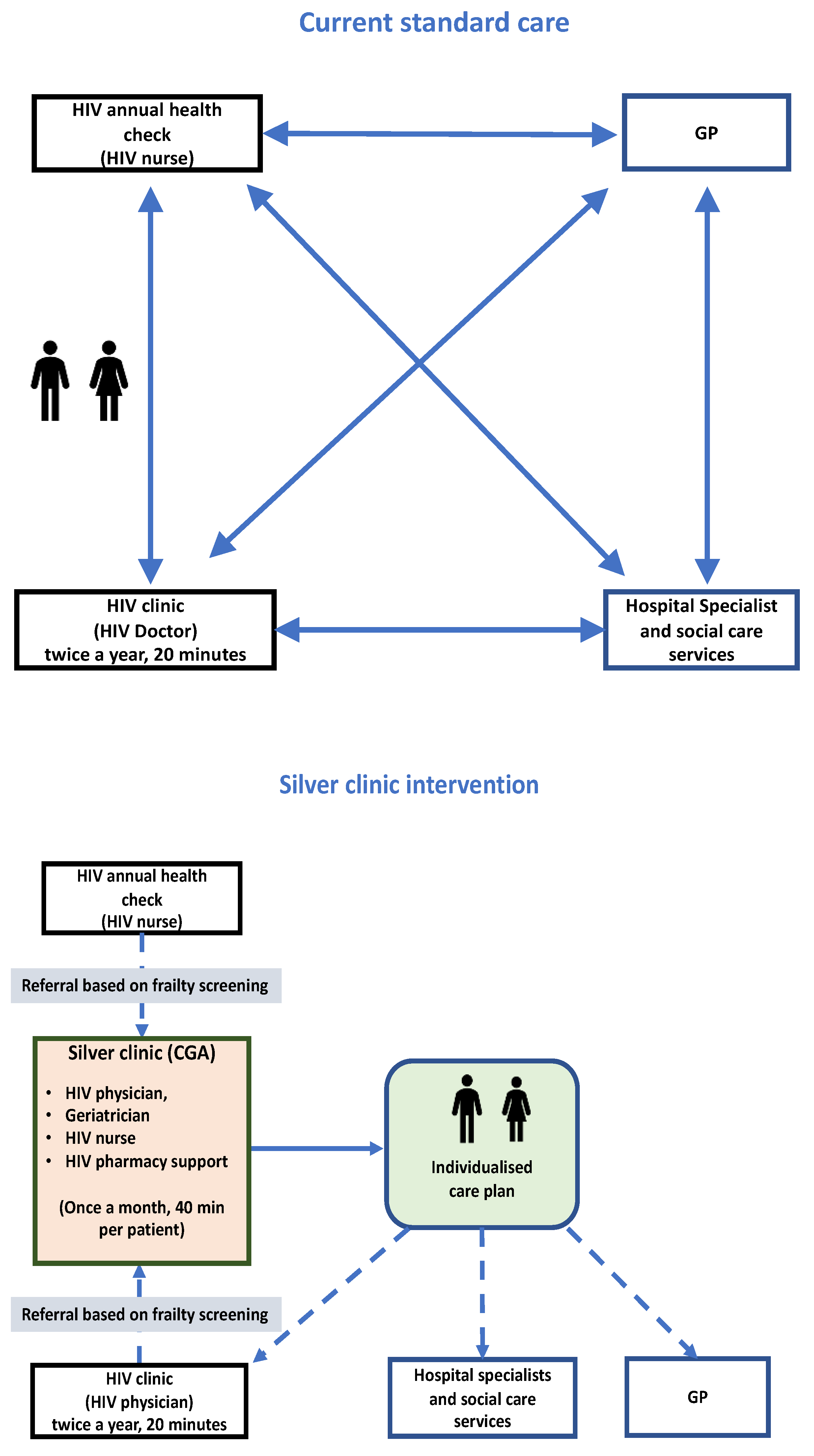
2.1. Clinic Process
2.2. Clinical Assessments
2.3. Patient and Healthcare Professional Satisfaction
2.4. Statistical Analysis
3. Results
3.1. Patient-Reported Outcomes
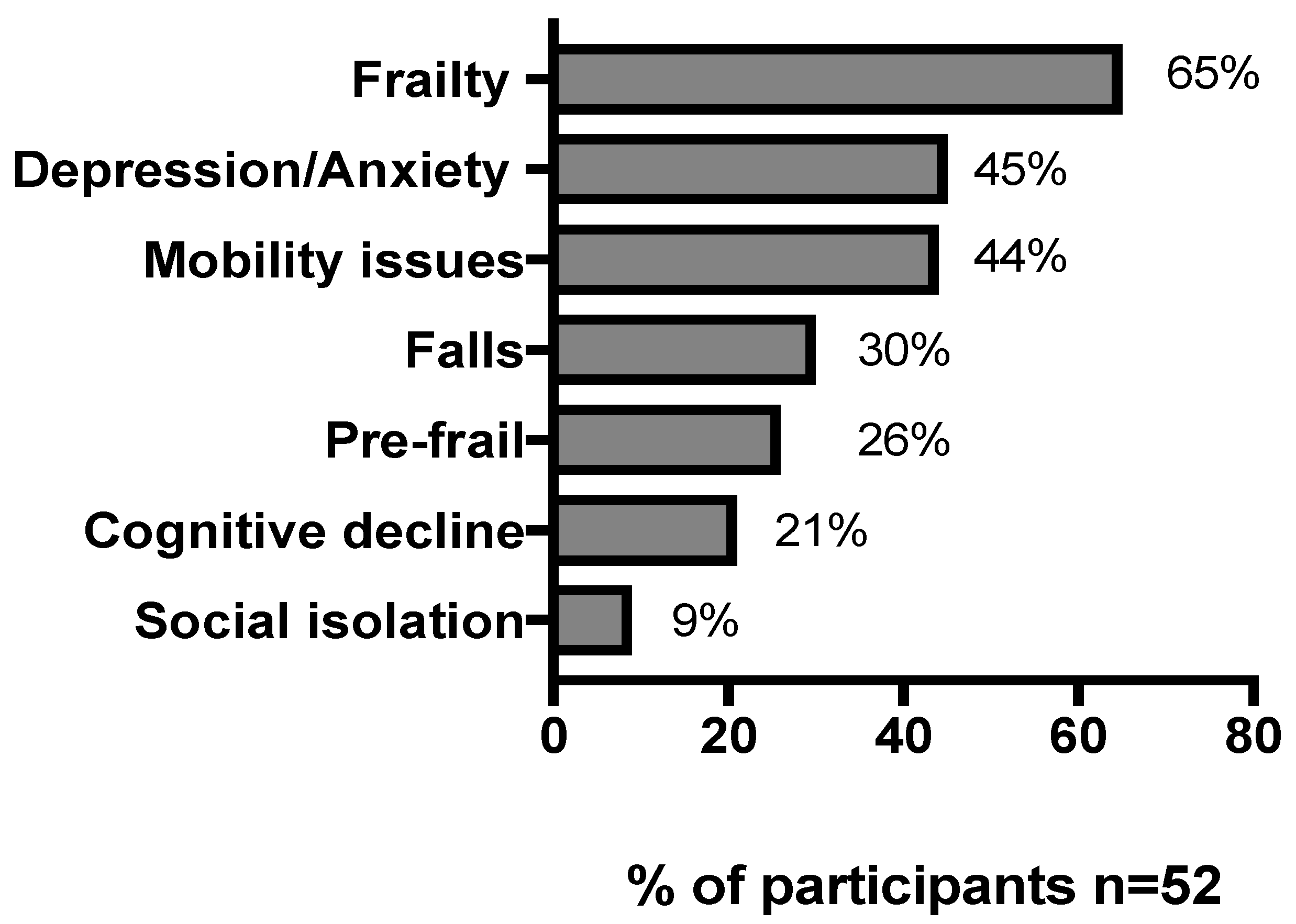
3.2. Clinic Outcomes
Case Study
- Proactive treatment of constipation (causing overflow incontinence) and opioid reduction.
- Fall prevention through occupational and physiotherapy referral and bone scan with subsequent osteoporosis treatment to reduce fracture risk.
- Medicines rationalisation with ART modification to a one tablet regimen (Rezolsta: Darunavir/Cobistat), which in turn allowed Zopiclone withdrawal.
- Signposting to community peer services aimed at increasing socialisation and an application for a disabled parking “Blue Badge” was supported.
- Referral to Cognitive Behavioural Therapy with the hope that improvements in mental health may also stem from comorbidity optimisation.
3.3. Patient Satisfaction
3.4. Healthcare Professionals’ Views of the Silver Clinic
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Harris, T.G.; Rabkin, M.; El-Sadr, W.M. Achieving the fourth 90. AIDS 2018, 32, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Nash, S.; Desai, S.; Croxford, S.; Guerra, L.; Lowndes, C.; Connor, N.; Gill, O.N. Progress towards Ending the HIV Epidemic in the United Kingdom: 2018 Report; Public Health England: London, UK, 2018. [Google Scholar]
- Smit, M.; Brinkman, K.; Geerlings, S.; Smit, C.; Thyagarajan, K.; Van Sighem, A.; De Wolf, F.; Hallett, T.B. Future challenges for clinical care of an ageing population infected with HIV: A modelling study. Lancet Infect. Dis. 2015, 15, 810–818. [Google Scholar] [CrossRef] [Green Version]
- Schouten, J.; Wit, F.W.; Stolte, I.G.; Kootstra, N.A.; Van Der Valk, M.; Geerlings, S.E.; Prins, M.; Reiss, P.; Kooij, K.W.; Van Zoest, R.A.; et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: The AGEhIV cohort study. Clin. Infect. Dis. 2014, 59, 1787–1797. [Google Scholar] [CrossRef] [PubMed]
- Althoff, K.N.; Jacobson, L.P.; Cranston, R.D.; Detels, R.; Phair, J.P.; Li, X.; Margolick, J.B.; for the Multicenter AIDS cohort study (MACS). Age, comorbidities, and AIDS predict a frailty phenotype in men who have sex with men. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 69, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Guaraldi, G.; Orlando, G.; Zona, S.; Menozzi, M.; Carli, F.; Garlassi, E.; Berti, A.; Rossi, E.; Roverato, A.; Palella, F. Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin. Infect. Dis. 2011, 53, 1120–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halloran, M.; Boyle, C.; Kehoe, B.; Bagkeris, E.; Mallon, P.; A Post, F.; Vera, J.; Williams, I.; Anderson, J.; Winston, A.; et al. Polypharmacy and drug–drug interactions in older and younger people living with HIV: The POPPY study. Antivir. Ther. 2019, 24, 193–201. [Google Scholar] [CrossRef]
- Greene, M.; Covinsky, K.E.; Valcour, V.; Miao, Y.; Madamba, J.; Lampiris, H.; Cenzer, I.S.; Martin, J.; Deeks, S.G. Geriatric syndromes in older HIV-infected adults. J. Acquir. Immune Defic. Syndr. 2015, 69, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guaraldi, G.; Rockwood, K. Geriatric-HIV medicine is born. Clin. Infect. Dis. 2017, 65, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, K.L.; Brown, T.T.; Margolick, J.B.; Erlandson, K.M. Geriatric syndromes: New frontiers in HIV and sarcopenia. AIDS 2017, 31, S137–S146. [Google Scholar] [CrossRef]
- Singh, H.K.; Del Carmen, T.; Freeman, R.; Glesby, M.J.; Siegler, E.L. From one syndrome to many: Incorporating geriatric consultation into HIV care. Clin. Infect. Dis. 2017, 65, 501–506. [Google Scholar] [CrossRef]
- McClure, M.; Singh, G.J.; Rayment, M.; Jones, R.; Levy, J.B. Clinical outcomes of a combined HIV and renal clinic. Clin. Kidney J. 2012, 5, 530–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koganti, S.; Loes, S.K.-D.; Hutchinson, S.; Johnson, M.; Rakhit, R.D. Management of cardiovascular conditions in a cohort of patients with HIV: Experience from a joint HIV/cardiology clinic. Clin. Med. 2015, 15, 442–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, L.; Patterson, B.; Scourfield, A.; Hughes, A.; De Silva, S.; Gazzard, B.; Barton, S.; Asboe, D.; Pozniak, A.; Boffito, M. A dedicated clinic for HIV-positive individuals over 50 years of age: A multidisciplinary experience. Int. J. STD AIDS 2012, 23, 546–552. [Google Scholar] [CrossRef]
- NHS England; LTC Team. Toolkit for General Practice in Supporting Older People Living with Frailty; NHS England: London, UK, 2017. [Google Scholar]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Tassiopoulos, K.; Abdo, M.; Wu, K.; Koletar, S.L.; Palella, F.J.; Kalayjian, R.; Taiwo, B.; Erlandson, K.M. Frailty is strongly associated with increased risk of recurrent falls among older HIV-infected adults. AIDS 2017, 31, 2287–2294. [Google Scholar] [CrossRef]
- Guaraldi, G.; Brothers, T.D.; Zona, S.; Stentarelli, C.; Carli, F.; Malagoli, A.; Santoro, A.; Menozzi, M.; Mussi, C.; Mussini, C.; et al. A frailty index predicts survival and incident multimorbidity independent of markers of HIV disease severity. AIDS 2015, 29, 1633–1641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akgun, K.M.; Tate, J.P.; Crothers, K.; Crystal, S.; Leaf, D.A.; Womack, J.; Brown, T.T.; Justice, A.C.; Oursler, K.K. An adapted frailty-related phenotype and the VACS index as predictors of hospitalization and mortality in HIV-infected and uninfected individuals. J. Acquir. Immune Defic. Syndr. 2014, 67, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Collard, R.M.; Comijs, H.C.; Naarding, P.; Penninx, B.W.; Milaneschi, Y.; Ferrucci, L.; Voshaar, R.C.O. Frailty as a predictor of the incidence and course of depressed mood. J. Am. Med. Dir. Assoc. 2015, 16, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Underwood, J.; Robertson, K.R.; Winston, A. Could antiretroviral neurotoxicity play a role in the pathogenesis of cognitive impairment in treated HIV disease? AIDS 2015, 29, 253–261. [Google Scholar] [CrossRef] [Green Version]
- British Geriatric Society, Fit for Frailty. 2017. Available online: https://www.bgs.org.uk/sites/default/files/content/resources/files/2018-05-14/fff2_short.pdf (accessed on 1 June 2019).
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017. [CrossRef] [Green Version]
- Stuck, A.E.; Iliffe, S. Comprehensive geriatric assessment for older adults. BMJ 2011, 343, d6799. [Google Scholar] [CrossRef]
- Garrard, J.W.; Cox, N.J.; Dodds, R.M.; Roberts, H.C.; Sayer, A.A. Comprehensive geriatric assessment in primary care: A systematic review. Aging Clin. Exp. Res. 2019, 32, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrence Higgins Trust, Uncharted Territory: A Report into the First Generation Growing Older with HIV. 2017. Available online: https://www.tht.org.uk/sites/default/files/2018-03/uncharted_territory_final_low-res.pdf (accessed on 13 October 2020).
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowling, A.; Hankins, M.; Windle, G.; Bilotta, C.; Grant, R. A short measure of quality of life in older age: The performance of the brief older people’s quality of life questionnaire (OPQOL-brief). Arch. Gerontol. Geriatr. 2013, 56, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Kaambwa, B.; Gill, L.; McCaffrey, N.; Lancsar, E.; Cameron, I.D.; Crotty, M.; Gray, L.; Ratcliffe, J. An empirical comparison of the OPQoL-Brief, EQ-5D-3 L and ASCOT in a community dwelling population of older people. Health Qual. Life Outcomes 2015, 13, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Dyer, M.T.D.; A Goldsmith, K.; Sharples, L.S.; Buxton, M.J. A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health Qual. Life Outcomes 2010, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G. Quick and Simple FRAIL Scale predicts incident activities of daily living (ADL) and instrumental ADL (IADL) disabilities: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 1063–1068. [Google Scholar] [CrossRef]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Bagkeris, E.; Burgess, L.; Mallon, P.W.; Post, F.A.; Boffito, M.; Sachikonye, M.; Anderson, J.; Asboe, D.; Garvey, L.; Vera, J.; et al. Cohort profile: The Pharmacokinetic and clinical observations in PeoPle over fiftY (POPPY) study. Int. J. Epidemiol. 2018, 47, 1391–1392e. [Google Scholar] [CrossRef] [Green Version]
- Greysen, S.R.; Horwitz, L.I.; Covinsky, K.E.; Gordon, K.; Ohl, M.; Justice, A.C. Does social isolation predict hospitalization and mortality among HIV+ and uninfected older veterans? J. Am. Geriatr. Soc. 2013, 61, 1456–1463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levett, T.J.; Cresswell, F.V.; Malik, M.A.; Fisher, M.; Wright, J. Systematic Review of Prevalence and predictors of frailty in individuals with human immunodeficiency virus. J. Am. Geriatr. Soc. 2016, 64, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; I Nicholl, B.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323–e332. [Google Scholar] [CrossRef]
- Kojima, G. Frailty Defined by FRAIL Scale as a predictor of mortality: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 480–483. [Google Scholar] [CrossRef]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Malagoli, A.; Calcagno, A.; Mussi, C.; Celesia, B.M.; Carli, F.; Piconi, S.; De Socio, G.V.; Cattelan, A.M.; Orofino, G.; et al. The increasing burden and complexity of multi-morbidity and polypharmacy in geriatric HIV patients: A cross sectional study of people aged 65–74 years and more than 75 years. BMC Geriatr. 2018, 18, 99. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, M.J.; Ray, G.T.; Saunders, K.; Rutter, C.M.; Campbell, C.I.; Merrill, J.O.; Sullivan, M.D.; Banta-Green, C.J.; Von Korff, M.; Weisner, C. Prescription long-term opioid use in HIV-infected patients. Clin. J. Pain 2012, 28, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Erlandson, K.M.; Allshouse, A.A.; Jankowski, C.M.; Duong, S.; Mawhinney, S.; Kohrt, W.M.; Campbell, T.B. Risk factors for falls in HIV-infected persons. J. Acquir. Immune Defic. Syndr. 2012, 61, 484–489. [Google Scholar] [CrossRef] [Green Version]
- NICE, Multimorbidity: Clinical Assessment and Management. National Institute of Health Research Guidelines. 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 13 October 2020).
- Greene, M.; Justice, A.C.; Covinsky, K.E. Assessment of geriatric syndromes and physical function in people living with HIV. Virulence 2016, 8, 586–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levett, T.; Wright, J. How to assess and manage frailty in patients with HIV. Sex. Transm. Infect. 2017, 93, 476–477. [Google Scholar] [CrossRef] [PubMed]
- Langebeek, N.; Kooij, K.W.; Wit, F.W.; Stolte, I.G.; Sprangers, M.A.G.; Reiss, P.; Nieuwkerk, P.T. Impact of comorbidity and ageing on health-related quality of life in HIV-positive and HIV-negative individuals. AIDS 2017, 31, 1471–1481. [Google Scholar] [CrossRef] [PubMed]
- Vargas, R.B.; Cunningham, W.E. Evolving trends in medical care-coordination for patients with HIV and AIDS. Curr. HIV/AIDS Rep. 2006, 3, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, F.; Levett, T. Specialist care of older adults with HIV infection in the UK: A service evaluation. HIV Med. 2017, 18, 519–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegler, E.L.; O Burchett, C.; Glesby, M.J. Older people with HIV are an essential part of the continuum of HIV care. J. Int. AIDS Soc. 2018, 21, e25188. [Google Scholar] [CrossRef] [Green Version]
- Pollard, A.; Llewellyn, C.; Cooper, V.; Sachikonye, M.; Perry, N.; Nixon, E.; Miners, A.; Youssef, E.; Sabin, C. Patients’ perspectives on the development of HIV services to accommodate ageing with HIV: A qualitative study. Int. J. STD AIDS 2017, 29, 483–490. [Google Scholar] [CrossRef] [Green Version]
- European AIDS Clinical Society EACS. Available online: https://www.eacsociety.org/files/2019_guidelines-10.0_final.pdf (accessed on 13 October 2020).
- BHIVA, Standards of Care for People Living with HIV. 2018. Available online: https://www.bhiva.org/file/KrfaFqLZRlBhg/BHIVA-Standards-of-Care-2018.pdf (accessed on 13 October 2020).



{kind=link}
{kind=link}
| Test Category | |
|---|---|
| Blood Tests | Calcium, TFTs, PSA, HbA1c, B12/Folate, Vitamin D |
| HIV clinical data | Year of diagnosis, nadir and current CD4 cell count, current CD8 cell count, CD4:CD8 ratio, antiretroviral history |
| Other clinical data | Urinalysis, height, weight, body mass index, blood pressure (lying and standing) |
| Mood assessment | Hospital Anxiety and Depression Scale |
| Frailty assessment | FRAIL scale |
| Patient reported outcome measures | Euroqol-5D-5L Older Peoples’ Quality of Life Questionnaire |
| Clinical Characteristics (n = 52) | Median (IQR) Otherwise Stated |
|---|---|
| Age (years) | 67 (53–87) |
| Male, n (%) | 47 (90) |
| White ethnicity, n (%) | 50 (96) |
| Identified sexuality, n (%) | |
| MSM | 41 (78) |
| Heterosexual | 9 (17) |
| Other | 2 (4) |
| Current smoker, n (%) | 17 (32) |
| Alcohol use, n (%) | |
| Less than 10 units per week | 41(77) |
| Between 10 and 20 units per week | 5 (9) |
| >20 units per week | 3 (4) |
| Recreational drug use n (%) | 6 (11) |
| Comorbidities | 7 (2–19) |
| Comedications | 9 (1–15) |
| QRISK3 * | 25 (6–52) |
| Bone densitometry, n (%) | |
| Osteoporosis | 15 (28) |
| Osteopenia | 33 (63) |
| Normal BMD | 4 (7) |
| HIV Clinical Parameters | |
| Time since HIV diagnosis: years (median; range) | 17 (6–34) |
| Duration of cART: years (median; range) | 17 (5–30) |
| cART-based regimen n (%) | |
| Protease inhibitor | 28 (53) |
| NNRTI | 12 (23) |
| INSTI | 12 (23) |
| HIV RNA < 50 copies/mL, n (%) | 52 (100) |
| Nadir CD4 (cells/μL) | 287 (223) |
| Current CD4 (cells/μL) | 563 (368) |
| CD4:CD8 ratio | 0.60 (0.1) |
| Medical Comorbidities | Comedications |
|---|---|
| Type 2 diabetes Depression Osteopenia Dyslipidaemia Chronic back pain secondary to (degenerative disease and C-spine injury) Peripheral neuropathy (ART-related) Chronic inflammatory demyelinating polyneuropathy unresponsive to immunoglobulin | 1. Paroxetine 40 mg daily 2. Gabapentin 400 mg twice daily 3. Aspirin 75 mg daily 4. Zopiclone 7.5 mg at night 5. Pravastatin 10 mg at night 6. Zomorph MR 60 mg twice daily 7. Metformin 1 g twice daily 8. Folic Acid 5 mg daily 9. Oramorph 5−10 mg as needed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levett, T.; Alford, K.; Roberts, J.; Adler, Z.; Wright, J.; Vera, J.H. Evaluation of a Combined HIV and Geriatrics Clinic for Older People Living with HIV: The Silver Clinic in Brighton, UK. Geriatrics 2020, 5, 81. https://doi.org/10.3390/geriatrics5040081
Levett T, Alford K, Roberts J, Adler Z, Wright J, Vera JH. Evaluation of a Combined HIV and Geriatrics Clinic for Older People Living with HIV: The Silver Clinic in Brighton, UK. Geriatrics. 2020; 5(4):81. https://doi.org/10.3390/geriatrics5040081
Chicago/Turabian StyleLevett, Tom, Katie Alford, Jonathan Roberts, Zoe Adler, Juliet Wright, and Jaime H. Vera. 2020. "Evaluation of a Combined HIV and Geriatrics Clinic for Older People Living with HIV: The Silver Clinic in Brighton, UK" Geriatrics 5, no. 4: 81. https://doi.org/10.3390/geriatrics5040081
APA StyleLevett, T., Alford, K., Roberts, J., Adler, Z., Wright, J., & Vera, J. H. (2020). Evaluation of a Combined HIV and Geriatrics Clinic for Older People Living with HIV: The Silver Clinic in Brighton, UK. Geriatrics, 5(4), 81. https://doi.org/10.3390/geriatrics5040081