Is IDDSI an Evidence-Based Framework? A Relevant Question for the Frail Older Population

Abstract
:1. Introduction
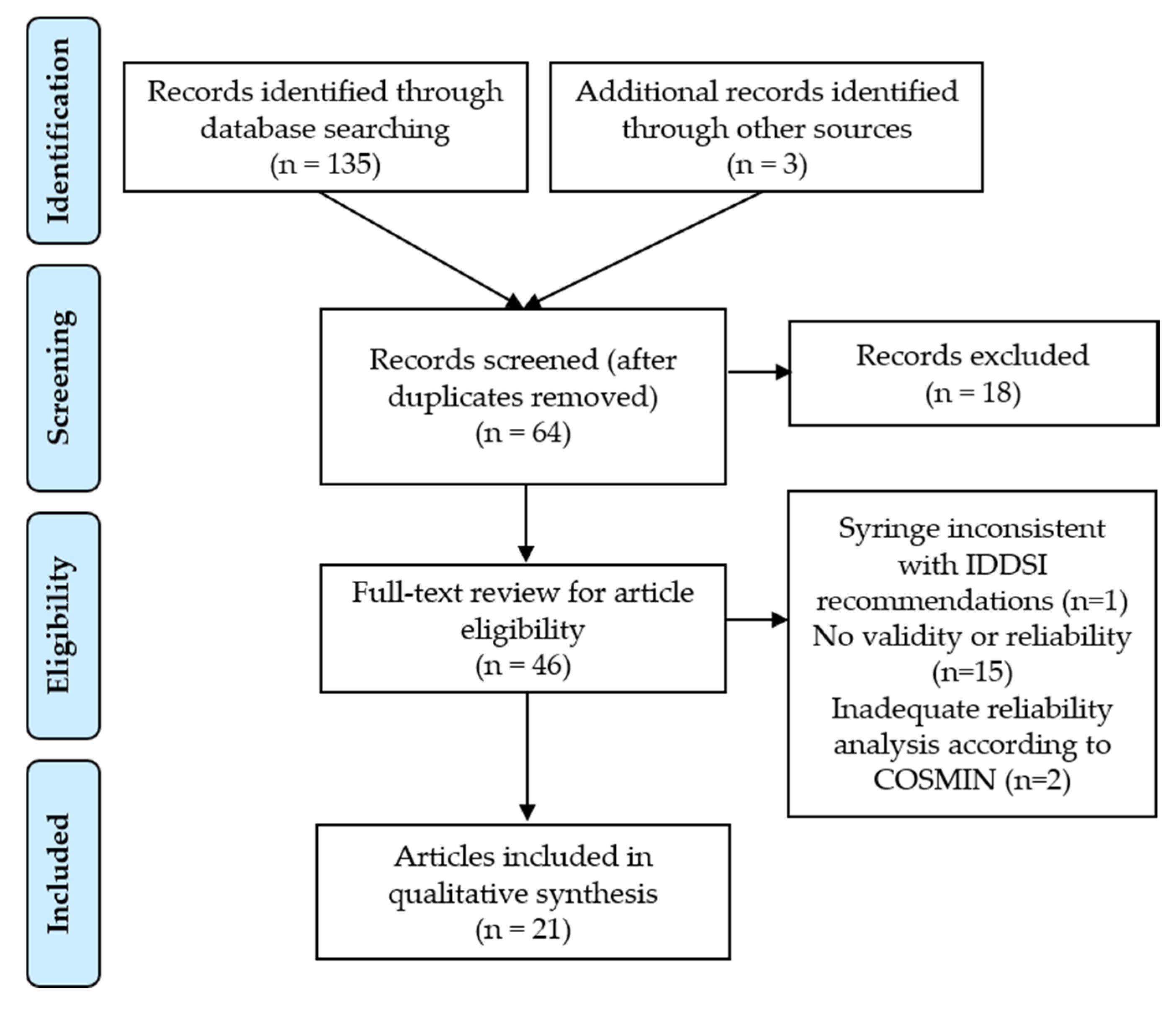
2. Materials and Methods
3. Results
3.1. Content Validity
3.2. Construct Validity
3.2.1. Measurement Comparison of the IDDSI Flow Test with Other Related Tools
3.2.2. Discrimination Ability of the IDDSI Flow Test
3.3. Reliability
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ambali, A. Preventive geriatrics—A way towards active ageing. In Ageing Issues and Responses in India; Shankardass, M., Ed.; Springer: Singapore, 2020; pp. 25–43. [Google Scholar] [CrossRef]
- Nettore, I.C.; Ungaro, P.; Macchia, P.E. Food and nutrition as prime environmental factors. In Beyond Our Genes: Pathophysiology of Gene and Environment Interaction and Epigenetic Inheritance; Teperino, R., Ed.; Springer Cham: Berlin/Heidelberg, Germany, 2020; pp. 3–16. [Google Scholar] [CrossRef]
- Wakabayashi, H. Role of nutrition and rehabilitation in the prevention and management of sarcopenia and frailty. In Recent Advances of Sarcopenia and Frailty in CKD; Kato, A., Kanda, E., Kanno, Y., Eds.; Springer: Singapore, 2020; pp. 117–138. [Google Scholar] [CrossRef]
- Blanař, V.; Hödl, M.; Lohrmann, C.; Amir, Y.; Eglseer, D. Dysphagia and factors associated with malnutrition risk: A 5-year multicentre study. J. Adv. Nurs. 2019, 75, 3566–3576. [Google Scholar] [CrossRef] [PubMed]
- Popman, A.; Richter, M.; Allen, J.; Wham, C. High nutrition risk is associated with higher risk of dysphagia in advanced age adults newly admitted to hospital. Nutr. Diet. 2018, 75, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Azzolino, D.; Passarelli, P.C.; De Angelis, P.; Piccirillo, G.B.; D’addona, A.; Cesari, M. Poor oral health as a determinant of malnutrition and sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okazaki, T.; Ebihara, S.; Mori, T.; Izumi, S.; Ebihara, T. Association between sarcopenia and pneumonia in older people. Geriatr. Gerontol. Int. 2020, 20, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, H. Presbyphagia and sarcopenic dysphagia: Association between aging, sarcopenia and deglutition disorders. J. Frailty Aging 2014, 3, 97–103. [Google Scholar]
- Granic, A.; Martin-Ruiz, C.; Dodds, R.M.; Robinson, L.; Spyridopoulos, I.; Kirkwood, T.B.; von Zglinicki, T.; Sayer, A.A. Immunosenescence profiles are not associated with muscle strength, physical performance and sarcopenia risk in very old adults: The Newcastle 85+ Study. Mech. Ageing Dev. 2020, 190. [Google Scholar] [CrossRef]
- Pae, M.; Wu, D. Nutritional modulation of age-related changes in the immune system and risk of infection. Nutr. Res. 2017, 41, 14–35. [Google Scholar] [CrossRef] [Green Version]
- Altuna-Venegas, S.; Aliaga-Vega, R.; Maguiña, J.L.; Parodi, J.F.; Runzer-Colmenares, F.M. Risk of community-acquired pneumonia in older adults with sarcopenia of a hospital from Callao, Peru 2010–2015. Arch. Gerontol. Geriatr. 2019, 82, 100–105. [Google Scholar] [CrossRef]
- Botigué, T.; Masot, O.; Miranda, J.; Nuin, C.; Viladrosa, M.; Lavedán, A.; Zwakhalen, S. Prevalence and risk factors associated with low fluid intake in institutionalized older residents. J. Am. Med. Dir. Assoc. 2019, 20, 317–322. [Google Scholar] [CrossRef]
- Curtis, J.A.; Molfenter, S.; Troche, M.S. Predictors of residue and airway invasion in Parkinson’s disease. Dysphagia 2020, 35, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Val, C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef] [Green Version]
- Yoshimatsu, Y.; Tobino, K.; Ko, Y.; Yasuda, M.; Ide, H.; Oku, Y. Careful history taking detects initially unknown underlying causes of aspiration pneumonia. Geriatr. Gerontol. Int. 2020, 20, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. 2015, 34, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Carrión, S.; Roca, M.; Costa, A.; Arreola, V.; Ortega, O.; Palomera, E.; Serra-Prat, M.; Cabré, M.; Clavé, P. Nutritional status of older patients with oropharyngeal dysphagia in a chronic versus an acute clinical situation. Clin. Nutr. 2017, 36, 1110–1116. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, S.; Lauretani, F.; Pelá, G.; Meschi, T.; Maggio, M. The risk of dysphagia is associated with malnutrition and poor functional outcomes in a large population of outpatient older individuals. Clin. Nutr. 2019, 38, 2684–2689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, C.M.; Alsanei, W.A.; Ayanikalath, S.; Barbon, C.E.A.; Chen, J.; Cichero, J.A.Y.; Coutts, K.; Dantas, R.O.; Duivestein, J.; Giosa, L.; et al. The influence of food texture and liquid consistency modification on swallowing physiology and function: A systematic review. Dysphagia 2015, 30, 2–26. [Google Scholar] [CrossRef] [Green Version]
- Yamada, Y. Physiological significance of taste on ingestion and swallowing. J. Health Sci. 2009, 55, 664–666. [Google Scholar] [CrossRef] [Green Version]
- Germain, I.; Dufresne, T.; Gray-Donald, K. A novel dysphagia diet improves the nutrient intake of institutionalized elders. J. Am. Diet. Assoc. 2006, 106, 1614–1623. [Google Scholar] [CrossRef]
- Ilhamto, N.; Keller, H.H.; Duizer, L.M. The effect of varying ingredient composition on the sensory and nutritional properties of a pureed meat and vegetable. J. Nutr. Gerontol. Geriatr. 2014, 33, 229–248. [Google Scholar] [CrossRef]
- Keller, H.H.; Carrier, N.; Slaughter, S.E.; Lengyel, C.; Steele, C.M.; Duizer, L.; Morrison, J.; Brown, K.S.; Chaudhury, H.; Yoon, M.N.; et al. Prevalence and determinants of poor food Intake of residents living in long-term care. J. Am. Med. Dir. Assoc. 2017, 18, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Hwang, H.I.; Song, K.W.; Lee, J. Sensory and rheological characteristics of thickened liquids differing concentrations of a xanthan gum-based thickener. J. Texture Stud. 2017, 48, 571–585. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, B.M.; Han, T.R. Factors associated with compliance with viscosity-modified diet among dysphagic patients. Ann. Rehabil. Med. 2013, 37, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Vucea, V.; Keller, H.H.; Morrison, J.M.; Duizer, L.M.; Duncan, A.M.; Carrier, N.; Lengyel, C.O.; Slaughter, S.E.; Steele, C.M. Modified texture food use is associated with malnutrition in long term care: An analysis of Making the Most of Mealtimes (M3) Project. J. Nutr. Health Aging 2018, 22, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Lengyel, C.; Keller, H.; Morrison, J.; Duncan, A.M.; Slaughter, S.E.; Carrier, N. Are therapeutic or modified texture diets associated with food intake and nutritional status of residents in long-term care homes? The Making the Most of Mealtimes (M3) study... Canadian Foundation for Dietetic Research: Dietetic Research Event: June 8 and 9, 2017, St John ’s, Newfoundland. Can. J. Diet. Pract. Res. 2017, 78, 155–156. [Google Scholar] [CrossRef] [Green Version]
- Vucea, V.; Keller, H.H.; Morrison, J.M.; Duizer, L.M.; Duncan, A.M.; Steele, C.M. Prevalence and characteristics associated with modified texture food use in long term care: An analysis of Making the Most of Mealtimes (M3) Project. Can. J. Diet. Pract. Res. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gillman, A.; Winkler, R.; Taylor, N.F. Implementing the Free Water Protocol does not result in aspiration pneumonia in carefully selected patients with dysphagia: A systematic review. Dysphagia 2017, 32, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Doeltgen, S.; Miller, M.; Scholten, I. Does a water protocol improve the hydration and health status of individuals with thin liquid inspiration following stroke? A randomized controlled trial. Dysphagia 2016, 31, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Flynn, E.; Smith, C.H.; Walsh, C.D.; Walshe, M. Modifying the consistency of food and fluids for swallowing difficulties in dementia. Cochrane Database Syst. Rev. 2018, 9, Cd011077. [Google Scholar] [CrossRef] [Green Version]
- Loeb, M.B.; Becker, M.; Eady, A.; Walker-Dilks, C. Interventions to prevent aspiration pneumonia in older adults: A systematic review. J. Am. Geriatr. Soc. 2003, 51, 1018–1022. [Google Scholar] [CrossRef]
- Felt, P. The National Dysphagia Diet project: The Science and practice. Nutr. Clin. Prac. 1999, 14, S60–S65. [Google Scholar] [CrossRef]
- Tymchuck, D. Textural property considerations of food for dysphagia. Nutr. Clin. Prac. 1999, 14, S57–S59. [Google Scholar] [CrossRef]
- IDDSI. IDDSI Framework-Evidence Statement. Available online: https://iddsi.org/Documents/IDDSIFramework-EvidenceStatement.pdf (accessed on 10 October 2020).
- Cichero, J.A.Y.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Duivestein, J.; Kayashita, J.; Lecko, C.; Murray, J.; et al. Development of international terminology and definitions for texture-modified foods and thickened fluids used in dysphagia management: The IDDSI framework. Dysphagia 2017, 32, 293–314. [Google Scholar] [CrossRef] [Green Version]
- IDDSI. Food and Drinks Classification and Testing-Adult. Available online: https://ftp.iddsi.org/Documents/IDDSI_Whole_Framework_A3_Poster_Final.pdf (accessed on 10 October 2020).
- Mokkink, L.B.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.C.W.; Terwee, C.B. COSMIN Study Design Checklist for Patient-Reported Outcome Measurement Intruments. Available online: http://cosmin.nl (accessed on 10 October 2020).
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. COSMIN Checklist Manual; VU University Medical Center: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Su, M.; Zheng, G.; Chen, Y.; Xie, H.; Han, W.; Yang, Q.; Sun, J.; Lv, Z.; Chen, J. Clinical applications of IDDSI framework for texture recommendation for dysphagia patients. J. Texture Stud. 2018, 49, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbon, C.E.A.; Steele, C.M. Thickened Liquids for Dysphagia Management: A Current Review of the Measurement of Liquid Flow. Curr. Phys. Med. Rehabil. Rep. 2018, 6, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Hadde, E.K.; Cichero, J.A.Y.; Zhao, S.; Chen, W.; Chen, J. The importance of extensional rheology in bolus control during swallowing. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Hanson, B.; Jamshidi, R.; Redfearn, A.; Begley, R.; Steele, C.M. Experimental and computational investigation of the IDDSI flow test of liquids used in dysphagia management. Ann. Biomed. Eng. 2019, 47, 2296–2307. [Google Scholar] [CrossRef] [Green Version]
- Hron, B.; Rosen, R. Viscosity of commercial food based formulas and home prepared blenderized feeds. J. Pediatr. Gastroenterol. Nutr. 2020. [Google Scholar] [CrossRef]
- Kim, Y.H.; Jeong, G.Y.; Yoo, B. Comparative study of IDDSI flow test and line-spread test of thickened water prepared with different dysphagia thickeners. J. Texture Stud. 2018, 49, 653–658. [Google Scholar] [CrossRef]
- Ong, J.J.-X.; Steele, C.M.; Duizer, L.M. Challenges to assumptions regarding oral shear rate during oral processing and swallowing based on sensory testing with thickened liquids. Food Hydrocoll. 2018, 84, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.-X.; Steele, C.M.; Duizer, L.M. Sensory characteristics of liquids thickened with commercial thickeners to levels specified in the International Dysphagia Diet Standardisation Initiative (IDDSI) framework. Food Hydrocoll. 2018, 79, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Redfearn, A. An In-Vitro Simulator to Study Non-Newtonian Fluid Mechanics during the Oral Phase of Swallowing. Ph.D. Thesis, University College London, London, UK, 2019. [Google Scholar]
- Steele, C.M.; Peladeau-Pigeon, M.; Barbon, C.A.E.; Guida, B.T.; Namasivayam-MacDonald, A.M.; Nascimento, W.V.; Smaoui, S.; Tapson, M.S.; Valenzano, T.J.; Waito, A.A.; et al. Reference values for healthy swallowing across the range from thin to extremely thick liquids. J. Speech Lang. Hear. Res. 2019, 62, 1338–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, C.M.; Peladeau-Pigeon, M.; Barbon, C.A.E.; Guida, B.T.; Tapson, M.S.; Valenzano, T.J.; Wolkin, T.S.; Waito, A.A.; Hanson, B.; Ong, J.J.X.; et al. Modulation of tongue pressure according to liquid flow properties in healthy swallowing. J. Speech Lang. Hear. Res. 2019, 62, 22–33. [Google Scholar] [CrossRef] [Green Version]
- Barbon, C.E.A.; Steele, C.M. Characterizing the flow of thickened barium and non-barium liquid recipes using the IDDSI flow test. Dysphagia 2019, 34, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Dantas, R.O.; Oliveira, L. Influence of the syringe model on the results of the International Dysphagia Diet Standardisation initiative flow test. J. Rev. CEFAC 2018, 20, 382–387. [Google Scholar] [CrossRef]
- Garcia, J.M.; Chambers, E.I.; Noll, K.S. Gravity flow test comparisons for mildly thick consistency. J. Texture Stud. 2020, 51, 308–313. [Google Scholar] [CrossRef]
- Martínez, O.; Vicente, M.S.; De Vega, M.C.; Salmerón, J. Sensory perception and flow properties of dysphagia thickening formulas with different composition. Food Hydrocoll. 2019, 90, 508–514. [Google Scholar] [CrossRef]
- Matsuyama, S.; Nakauma, M.; Funami, T.; Yamagata, Y.; Kayashita, J. The influence of syringe geometry on the International Dysphagia Diet Standardisation Initiative flow test. Int. J. Food Sci. Technol. 2020. [Google Scholar] [CrossRef]
- Rule, D. Implementation strategies for the International Dysphagia Diet Standardisation Initiative (IDDSI). Ph.D. Thesis, University of Cincinnati, Cincinnati, OH, USA, 2019. [Google Scholar]
- Rule, D.W.; Kelchner, L.; Mulkern, A.; Couch, S.; Silbert, N.; Welden, K. Implementation strategies for the International Dysphagia Diet Standardisation Initiative (IDDSI), part I: Quantitative analysis of IDDSI performance among varied participants. Am. J. Speech-Lang. Pathol. 2020, 1–15. [Google Scholar] [CrossRef]
- Côté, C.; Germain, I.; Dufresne, T.; Gagnon, C. Comparison of two methods to categorize thickened liquids for dysphagia management in a clinical care setting context: The Bostwick consistometer and the IDDSI Flow Test. Are we talking about the same concept? J. Texture Stud. 2019, 50, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Kutter, A.; Singh, J.P.; Rauh, C.; Delgado, A. Improvement of the prediction of mouthfeel attributes of liquid foods by a posthumus funnel. J. Texture Stud. 2011, 42, 217–227. [Google Scholar] [CrossRef]
- Van Vliet, T. On the relation between texture perception and fundamental mechanical parameters for liquids and time dependent solids. Food Qual. Prefer. 2002, 13, 227–236. [Google Scholar] [CrossRef]
- Cichero, J.A.Y. Evaluating chewing function: Expanding the dysphagia field using food oral processing and the IDDSI framework. J. Texture Stud. 2019. [Google Scholar] [CrossRef] [PubMed]
- Szczesniak, A.S. Correlating sensory with instrumental texture measurements—An overview of recent developments. J. Texture Stud. 1987, 18, 1–15. [Google Scholar] [CrossRef]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: White paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.-J.; Bi, X.; Song, L.; Liu, Z.-H.; Zhang, J.-M.; Huang, Q. Value of applying water swallowing test for patients with dysphagia after acute stroke. J. Shanghai Jiatong Univ. (Med. Sci.) 2016, 36, 1049–1053. [Google Scholar]
- Pax, L.A. Evaluation of Characteristics of Baby Food in Correlation to an International Diet Standardisation Protocol. Master’s Thesis, Miami University, Miami, FL, USA, 2019. [Google Scholar]
- Summerford, M.S. All Purees Are not Created Equal: Thickness, Adhesiveness, and Cohesiveness of Commercially Available First Foods. Master’s Thesis, University of Alabama, University of Alabama Libraries, Tuscaloosa, AL, USA, 2019. [Google Scholar]
- Kwong, J.S.W.; Chen, H.; Sun, X. Development of evidence-based recommendations: Implications for preparing expert consensus statements. Chin. Med. J. (Engl.) 2016, 129, 2998–3000. [Google Scholar] [CrossRef]
- Clave, P.; de Kraa, M.; Arreola, V.; Girvent, M.; Farre, R.; Palomera, E.; Serra-Prat, M. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment. Pharmacol. Ther. 2006, 24, 1385–1394. [Google Scholar] [CrossRef]
- Kaneoka, A.; Pisegna, J.M.; Saito, H.; Lo, M.; Felling, K.; Haga, N.; LaValley, M.P.; Langmore, S.E. A systematic review and meta-analysis of pneumonia associated with thin liquid vs. thickened liquid intake in patients who aspirate. Clin. Rehabil. 2017, 31, 1116–1125. [Google Scholar] [CrossRef]
- Germain, I.; Dufresne, T.; Ramaswamy, H.S. Rheological characterization of thickened beverages used in the treatment of dysphagia. J. Food Eng. 2006, 73, 64–74. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Levels | Food | Drinks | IDDSI Flow Test (Volume Remaining in the 10 mL Syringe after 10 s of Flow) |
|---|---|---|---|
| 7 | Regular/easy to chew | ||
| 6 | Soft and bite-sized | ||
| 5 | Minced and moist | ||
| 4 | Pureed | Extremely thick | 10 mL |
| 3 | Liquidized | Moderately thick | 8–10 mL |
| 2 | Mildly thick | 4–8 mL | |
| 1 | Slightly thick | 1–4 mL | |
| 0 | Thin | ˂1 mL |
| Keywords | Databases | Results (Ntotal = 135) |
|---|---|---|
| “IDDSI” OR “International Dysphagia Diet Standardisation Initiative” OR “International Dysphagia Diet Standardisation Initiative” | Medline | 42 |
| Cinahl | 29 | |
| Scopus | 43 | |
| Proquest Dissertation and Thesis | 4 | |
| Proquest | 17 |
| (a) Construct Validity Assessment. | ||||||
| Authors | IDDSI | Country | Type of Study/Participants (nb and Age) | Tested Products | T°C | Evaluations Completed |
| Barbon et al., 2018 [43] | X | Canada | In vitro | Water + ThickenUp®® Water + ThickenUp Clear®® | 25° | IDDSI Flow Test—IDDSI Levels 0 to 4 Bostwick Consistometer Line-Spread Test |
| Hadde et al., 2019 [44] | X | China | In vitro In vivo | Water + ThickenUp®® + Barium Water + ThickenUp Clear®® + Barium Water + Hehongchun + Barium | 25° | IDDSI Flow Test—IDDSI Levels 1 to 3 Fork Drip Test—IDDSI Level 4 Videofluoroscopy Viscosity Maximal Extensional Viscosity |
| Hanson et al., 2019 [45] | X | United Kingdom | In vitro Mathematical Model | Water + ThickenUp®® Water + ThickenUp Clear®® Glycerol + Water (Newtonian) | 21° | IDDSI Flow Test—IDDSI Levels 1 to 3 Viscosity |
| Hron et al., 2020 [46] | USA | In vitro Pediatrics | Homemade purees Commercial purees Infants formula thickened with baby cereal | N/A | IDDSI Flow Test—IDDSI Levels 1 to 3 Fork Drip Test—IDDSI Level 4 (milliliter values not provided) Viscosity | |
| Kim et al., 2018 [47] | South Korea | In vitro | Water + Starch and/or gums Xanthan mainly | 20° | IDDSI Flow Test—IDDSI Levels 1 to 3 Line-Spread Test | |
| Ong et al., 2018a [48] | X | Canada | In vitro Sensory University students n = 29 untrained n = 10 trained | Water + Carboxymethyl cellulose gum Water + Xanthan gum Water + Guar gum | 25° | IDDSI Flow Test—IDDSI Levels 1 to 3 Viscosity Description and magnitude estimation scaling: Ease of swallowing, slipperiness, perceived viscosity |
| Ong et al., 2018b [49] | X | Canada | In vitro Sensory University students n = 30 untrained n = 23 trained | Water + ThickenUp®® Water + ThickenUp®® + Barium Water + ThickenUp Clear®® Water + ThickenUp Clear®® + Barium | 25° | IDDSI Flow Test—IDDSI Levels 1 to 3 Viscosity Description of sensory attributes (sweet, salty, lemon, adhesiveness, graininess, slipperiness, perceived viscosity, ease of manipulation and ease of swallowing) Projective Mapping and Ultra-Flash Profile |
| Redfearn, A. 2019 [50] | X | United Kingdom | In vitro | Water + Thick & Easy™ Clear Water + Thick & Easy™ | 19.5° | IDDSI Flow Test—IDDSI Levels 1 to 4 Viscosity |
| Steele et al., 2019a [51] | X | Canada | In vivo n = 40 (50% Males) Healthy Mean Age: 34 yr. (21–58 yr.) | Water + ThickenUp Clear®® + Barium (Same samples as Ref. 6 and 10) | ≈22° | IDDSI Flow Test—IDDSI Levels 0 to 4 Videofluoroscopy Sip volume Number of swallows per bolus Penetration-Aspiration Scale Timing measures of swallow Bolus location measures |
| Steele et al., 2019b [52] | X | Canada | In vivo n = 40 (50% Males) Healthy Mean Age: 34 yr. (21–58 yr.) | Water + ThickenUp®® Water + ThickenUp®® + Barium Water + ThickenUp Clear®® Water + ThickenUp Clear®® + Barium (Same samples as Ref. 6) | ≈22° | IDDSI Flow Test—IDDSI Levels 0 to 3 Lingual manometry Sip volume |
| Su et al., 2018 [42] | X | China | Clinical n = 26 (85% Males) Dysphagia Mean Age: 88 yr. (53–105 yr.) | Water + Ourdiet Swallow | N/A | IDDSI Flow Test—at critical values between IDDSI Levels 0/1, 1/2, 2/3 and 3/4 Viscosity Water Drinking Test Volume-Viscosity Swallow Test |
| (b) Reliability Assessment | ||||||
| Authors | IDDSI | Country | Type of Study/Participants (nb and Age) | Tested Products | T°C | Evaluations Completed |
| Barbon et al., 2019 [53] | X | Canada | In vitro | Water + ThickenUp®® Water + ThickenUp®® + Barium Water + ThickenUp Clear®® Water + ThickenUp Clear®® + Barium | 4° ≈22° | IDDSI Flow Test—IDDSI Levels 1 to 3 |
| Dantas et al., 2018 [54] | X | Brazil | In vitro | Water + Xanthan + Maltodextrin Barium + Xanthan + Maltodextrin | ≈22° | IDDSI Flow Test—IDDSI Levels 1 to 3 Flow Test with syringe with different technical specifications than IDDSI Flow Test syringe |
| Garcia et al. 2019 [55] | USA | In vitro | Water, coffee, prune juice and 2% M.F. milk Lyons Ready Care Thick & Easy™ Simply Thick Thick & Easy™ Clear | N/A | IDDSI Flow Test—IDDSI Levels 0 to 4 Flow Test with syringe with different technical specifications than IDDSI Flow Test syringe Line-Spread Test | |
| Martinez et al., 2019 [56] | Spain | Sensory n = 23 Healthy Age: 20–70 yr. | Water + ThickenUp®® Water + Visco®® Instant | 21° | IDDSI Flow Test—IDDSI Levels 0 to 4 Viscosity Discrimination Tests: Duo-Trio Test Ranking Test | |
| Matsuyama et al., 2020 [57] | X | Japan | In vitro | Glucose syrup + Water (Newtonian) Water + Homemade Starch Water + Toromerin | 20° | IDDSI Flow Test—IDDSI Levels 0 to 3 Flow Test with syringe with different technical specifications than IDDSI Flow Test syringe Viscosity |
| Rule, D., 2019 [58] Rule, D et al. 2020 [59] | USA | In vitro In vivo n = 68 Healthy Age: 18–24 yr. (48.5%) 25–34 yr. (33.8%) 35–44 yr. (10.3%) 45–54 yr. (1.5%) 55+ yr. (5.9%) | Food and liquid items of various textures and consistencies Liquid items thickened with SimplyThick®® EasyMix™ | 23° | IDDSI Levels 0 to 7 IDDSI Flow Test—IDDSI Levels 1 to 4 Spoon Tilt Test Fork Drip Test Fork Pressure Test and Spoon Pressure Test Quiz pre- and post- self-study training Hands-on training Food and liquid classification task | |
| (c) Construct Validity and Reliability Assessment | ||||||
| Authors | IDDSI | Country | Type of Study/Participants (nb and Age) | Tested Products | T°C | Evaluations Completed |
| Côté et al., 2019 [60] | Canada | In vitro | Water and juices (apple, orange, cranberry) pre-thickened (Xanthan/Starch) | 8° | IDDSI Flow Test—IDDSI Levels 2 and 3 Bostwick Consistometer | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Côté, C.; Giroux, A.; Villeneuve-Rhéaume, A.; Gagnon, C.; Germain, I. Is IDDSI an Evidence-Based Framework? A Relevant Question for the Frail Older Population. Geriatrics 2020, 5, 82. https://doi.org/10.3390/geriatrics5040082
Côté C, Giroux A, Villeneuve-Rhéaume A, Gagnon C, Germain I. Is IDDSI an Evidence-Based Framework? A Relevant Question for the Frail Older Population. Geriatrics. 2020; 5(4):82. https://doi.org/10.3390/geriatrics5040082
Chicago/Turabian StyleCôté, Claudia, Amélie Giroux, Annie Villeneuve-Rhéaume, Cynthia Gagnon, and Isabelle Germain. 2020. "Is IDDSI an Evidence-Based Framework? A Relevant Question for the Frail Older Population" Geriatrics 5, no. 4: 82. https://doi.org/10.3390/geriatrics5040082
APA StyleCôté, C., Giroux, A., Villeneuve-Rhéaume, A., Gagnon, C., & Germain, I. (2020). Is IDDSI an Evidence-Based Framework? A Relevant Question for the Frail Older Population. Geriatrics, 5(4), 82. https://doi.org/10.3390/geriatrics5040082