
Elevated Levels of Neutrophil-to Monocyte Ratio Are Associated with the Initiation of Paroxysmal Documented Atrial Fibrillation in the First Two Months after Heart Transplantation: A Uni-Institutional Retrospective Study

 , , and
, , and
Abstract
:1. Introduction
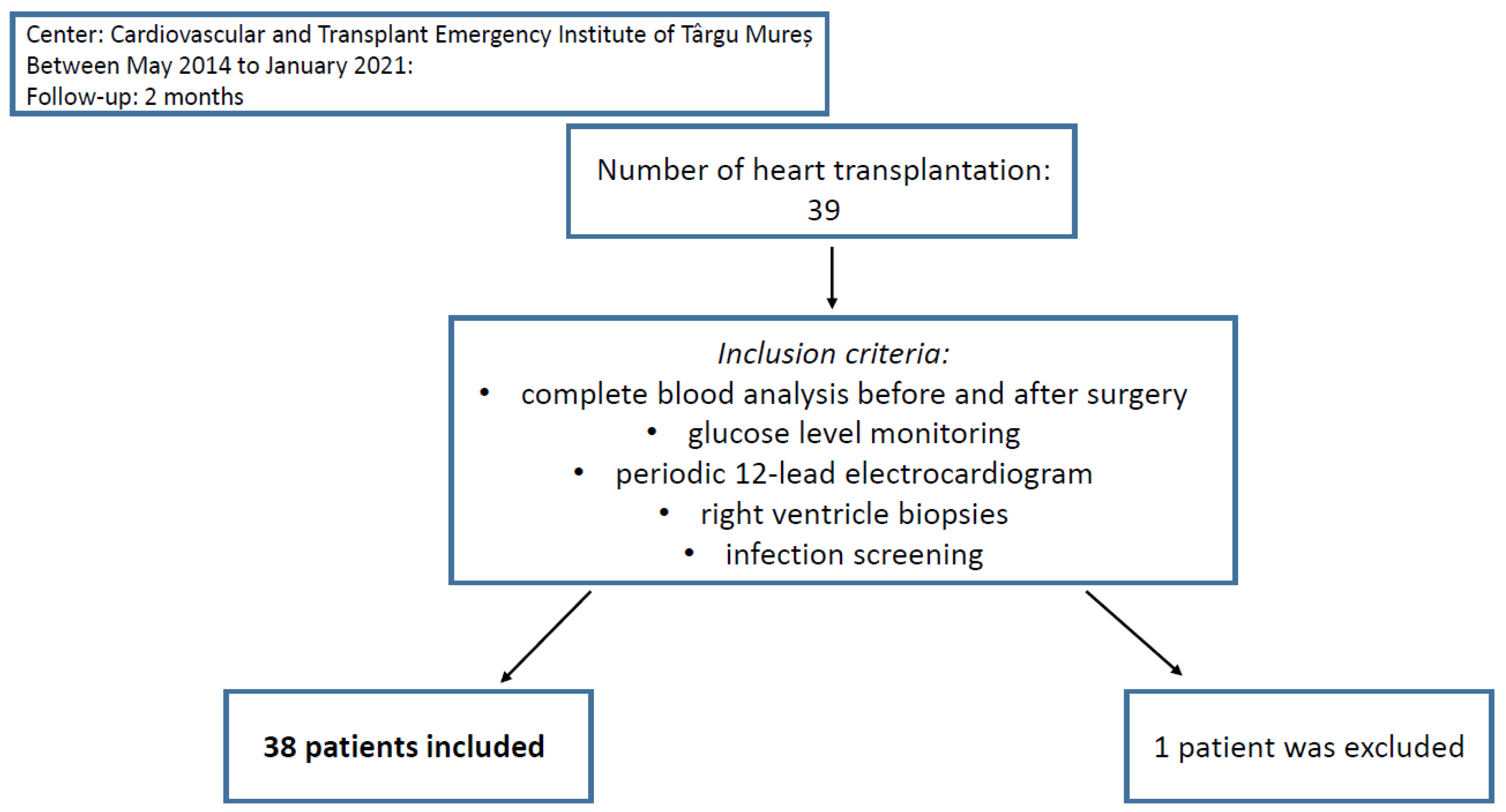
2. Materials and Methods
2.1. Management & Follow-Up
2.2. Data Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alraies, M.C.; Eckman, P. Adult heart transplant: Indications and outcomes. J. Thorac. Dis. 2014, 6, 1120–1128. [Google Scholar] [CrossRef] [PubMed]
- Brink, J.G.; Hassoulas, J. The first human heart transplant and further advances in cardiac transplantation at Groote Schuur Hospital and the University of Cape Town—With reference to: The operation. A human cardiac transplant: An interim report of a successful operation performed at Groote Schuur Hospital, Cape Town. Cardiovasc. J. Afr. 2009, 20, 31–35. [Google Scholar] [PubMed]
- Stehlik, J.; Leah, B.E.; Anna, Y.K.; Christian, B.; Jason, D.C.; Fabienne, D.; Richard, K.; Axel, O.R.; Marshall, I.H. The Registry of the International Society for Heart and Lung Transplantation: Twenty-Eighth Adult Heart Transplant Report—2011. J. Heart Lung Transplant. 2011, 30, 1078–1094. [Google Scholar] [CrossRef] [PubMed]
- Anyanwu, A.C. Intrathoracic Organ Transplantation in the United Kingdom 1995-99: Results from the UK Cardiothoracic Transplant Audit. Heart 2002, 87, 449–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruparelia, N.; Joshua, T.C.; Edward, A.F.; Robin, P.C. Inflammatory Processes in Cardiovascular Disease: A Route to Targeted Therapies. Nat. Rev. Cardiol. 2017, 14, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiordelisi, A.; Guido, I.; Carmine, M.; Enrico, C.; Daniela, S. NFkappaB Is a Key Player in the Crosstalk between Inflammation and Cardiovascular Diseases. Int. J. Mol. Sci. 2019, 20, 1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braza, F.; Sophie, B.; Steve, C.; Daniel, R.G. Role of Tlrs and Damps in Allograft Inflammation and Transplant Outcomes. Nat. Rev. Nephrol. 2016, 12, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Mortaz, E.; Shamila, D.A.; Ian, M.A.; Sharon, M.; Leo, K. Update on Neutrophil Function in Severe Inflammation. Front. Immunol. 2018, 9, 2171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero-Cervera, A.; Oliver, S.; Ellinor, K. Neutrophils in Chronic Inflammatory Diseases. Cell. Mol. Immunol. 2022, 19, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Eric, G.P. Monocyte Recruitment during Infection and Inflammation. Nat. Rev. Immunol. 2011, 11, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Akan, O.Y.; Bilgir, O. Effects of Neutrophil/Monocyte, Neutrophil/Lymphocyte, Neutrophil/Platelet Ratios and C-Reactive Protein Levels on the Mortality and Intensive Care Need of the Patients with COVID-19. Eurasian J. Med. Investig. 2021, 5, 21–26. [Google Scholar] [CrossRef]
- Yuan, C.; Li, N.; Mao, X.; Liu, Z.; Ou, W.; Wang, S.Y. Elevated Pretreatment Neutrophil/White Blood Cell Ratio and Monocyte/Lymphocyte Ratio Predict Poor Survival in Patients with Curatively Resected Non-Small Cell Lung Cancer: Results from a Large Cohort. Thorac. Cancer 2017, 8, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Avram, C.; Mărușteri, M. Normality Assessment, Few Paradigms and Use Cases. Rev. Romana Med. Lab. 2022, 30, 251–260. [Google Scholar] [CrossRef]
- Hu, Y.F.; Chen, Y.J.; Lin, Y.J.; Chen, S.A. Inflammation and the Pathogenesis of Atrial Fibrillation. Nat. Rev. Cardiol. 2015, 12, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Shahid, F.; Lip, G.Y.H.; Shantsila, E. Role of Monocytes in Heart Failure and Atrial Fibrillation. J. Am. Heart Assoc. 2018, 7, e007849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaul, D.S.; Sokrates, S.; Matter, C.M. Neutrophils in Cardiovascular Disease. Eur. Heart J. 2017, 38, 1702–1704. [Google Scholar] [CrossRef] [Green Version]
- Weymann, A.; Ali-Hasan-Al-Saegh, S.; Sabashnikov, A.; Popov, A.F.; Mirhosseini, S.J.; Liu, T.; Lotfaliani, M.; de Sá, M.P.O.; Baker, W.L.; Yavuz, S.; et al. Prediction of New-Onset and Recurrent Atrial Fibrillation by Complete Blood Count Tests: A Comprehensive Systematic Review with Meta-Analysis. Med. Sci. Monit. Basic Res. 2017, 23, 179–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ertaş, G.; Osman, S.; Murat, T.; Şeref, K.; Ercan, E.; Tasal, A.; Bacaksiz, A.; Vatankulu, M.A.; Altıntaş, Ö.; Uyarel, H.; et al. Neutrophil/Lymphocyte Ratio Is Associated with Thromboembolic Stroke in Patients with Non-Valvular Atrial Fibrillation. J. Neurol. Sci. 2013, 324, 49–52. [Google Scholar] [CrossRef]
- Kawasaki, M.; Meulendijks, E.R.; van den Berg, N.W.; Nariswari, F.A.; Neefs, J.; Wesselink, R.; Baalman, S.W.; Jongejan, A.; Schelfhorst, T.; Piersma, S.R.; et al. Neutrophil Degranulation Interconnects Over-Represented Biological Processes in Atrial Fibrillation. Sci. Rep. 2021, 11, 2972. [Google Scholar] [CrossRef]
- Rizos, I.; Rigopoulos, A.G.; Kalogeropoulos, A.S.; Tsiodras, S.; Dragomanovits, S.; Sakadakis, E.A.; Faviou, E.; Kremastinos, D.T. Hypertension and Paroxysmal Atrial Fibrillation: A Novel Predictive Role of High Sensitivity C-Reactive Protein in Cardioversion and Long-Term Recurrence. J. Hum. Hypertens. 2010, 24, 447–457. [Google Scholar] [CrossRef]
- Richter, B.; Gwechenberger, M.; Socas, A.; Zorn, G.; Albinni, S.; Marx, M.; Bergler-Klein, J.; Binder, T.; Wojta, J.; Gössinger, H.D. Markers of Oxidative Stress after Ablation of Atrial Fibrillation Are Associated with Inflammation, Delivered Radiofrequency Energy and Early Recurrence of Atrial Fibrillation. Clin. Res. Cardiol. 2011, 101, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, M.S.; Chen, H.J.; Warshofsky, M.K.; Sciacca, R.R.; Wasserman, H.S.; Schwartz, A.; Rabbani, L.E. Elevated levels of plasma C-reactive protein are associated with decreased graft survival in cardiac transplant recipients. Circulation 2000, 102, 2100–2104. [Google Scholar] [CrossRef] [PubMed]
- Labarrere, C.A.; Lee, J.B.; Nelson, D.R.; Al-Hassani, M.; Miller, S.J.; Pitts, D.E. C-reactive protein, arterial endothelial activation, and development of transplant coronary artery disease: A prospective study. Lancet 2002, 360, 1462–1467. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, N.F.; Elsurer, R.; Ibis, A.; Arat, Z.; Haberal, M. Serum C-reactive protein surge in renal transplant recipients: Link with allograft survival. Transplant. Proc. 2007, 39, 934–937. [Google Scholar] [CrossRef] [PubMed]
- Sezer, S.; Akcay, A.; Ozdemir, F.N.; Kulah, E.; Arat, Z.; Haberal, M. Post-transplant C-reactive protein monitoring can predict chronic allograft nephropathy. Clin. Transplant. 2004, 18, 722–725. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yao, L.; Xiang, P.; Lin, P.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-Lymphocyte Ratio Predicts Critical Illness Patients with 2019 Coronavirus Disease in the Early Stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Berhane, M.; Mulugeta, M.; Anteneh, A.; Enawgaw, B.; Getaneh, Z.; Asrie, F. The Role of Neutrophil to Lymphocyte Count Ratio in the Differential Diagnosis of Pulmonary Tuberculosis and Bacterial Community-Acquired Pneumonia: A Cross-Sectional Study at Ayder and Mekelle Hospitals, Ethiopia. Clin. Lab. 2019, 65, 10–7754. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.L.; Zhang, H.F.; Zhang, Q.; Zhu, X.Y.; Liu, C.H.; Wang, N.; Zhang, J.B.; Chen, H.; Chen, Y.; Li, W.Q.; et al. Neutrophil-to-Lymphocyte Ratio in Adult Community-Acquired Pneumonia Patients Correlates with Unfavorable Clinical Outcomes. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef] [PubMed]
- Cupp, M.A.; Margarita, C.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A.J. Neutrophil to Lymphocyte Ratio and Cancer Prognosis: An Umbrella Review of Systematic Reviews and Meta-Analyses of Observational Studies. BMC Med. 2020, 18, 360. [Google Scholar] [CrossRef] [PubMed]
- Zahorec, R. Neutrophil-to-Lymphocyte Ratio, Past, Present and Future Perspectives. Bratisl. Med. J. 2021, 122, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Olasińska-Wiśniewska, A.; Michalak, M.; Rodzki, M.; Witkowska, A.; Straburzyńska-Migaj, E.; Perek, B.; Jemielity, M. Neutrophil to Lymphocyte Ratio (NLR) as an Easily Accessible Parameter for Monitoring Tacrolimus Overdose after Heart Transplantation-Experimental Study. Diagnostics 2021, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.; Pamecha, V.; Sinha, P.K.; Patil, N.; Mahapatra, N. Neutrophil Lymphocyte Ratio can Preempt Development of Sepsis After Adult Living Donor Liver Transplantation. J. Clin. Exp. Hepatol. 2022, 12, 1142–1149. [Google Scholar] [CrossRef]
- Halazun, K.J.; Hardy, M.A.; Rana, A.A.; Woodland, D.C.; Luyten, E.J.; Mahadev, S.; Witkowski, P.; Siegel, A.B.; Brown, R.S.; Emond, J.C. Negative impact of neutrophil-lymphocyte ratio on outcome after liver transplantation for hepatocellular carcinoma. Ann. Surg. 2009, 250, 141–151. [Google Scholar] [CrossRef]
- Mikulski, D.; Kościelny, K.; Nowicki, M.; Wawrzyniak, E.; Kalwas, M.; Kowalik, M.; Pryt, M.; Sęczkowska, E.; Świątek, A.; Wierzbowska, A.; et al. Neutrophil to lymphocyte ratio (NLR) impact on the progression-free survival and overall survival of multiple myeloma patients treated with high-dose chemotherapy and autologous stem cell transplantation. Leuk. Lymphoma 2022, 64, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Penghui, D.; Qiongqiong, W.; Ke, G.Z.W.; Huan, C.; Ting, L.; Muhan, L.M.D.; Gang, L. The Neutrophil-to-Monocyte Ratio and Platelet-to-White Blood Cell Ratio Represent Novel Prognostic Markers in Patients with Pancreatic Cancer. Gastroenterol. Res. Pract. 2021, 2021, 6693028. [Google Scholar] [CrossRef] [PubMed]
- Rizo-Téllez, S.A.; Méndez-García, L.A.; Flores-Rebollo, C.; Alba-Flores, F.; Alcántara-Suárez, R.; Manjarrez-Reyna, A.N.; Baltazar-López, N.; Hernández-Guzmán, V.A.; León-Pedroza, J.I.; Zapata-Arenas, R.; et al. The Neutrophil-to-Monocyte Ratio and Lymphocyte-to-Neutrophil Ratio at Admission Predict In-Hospital Mortality in Mexican Patients with Severe SARS-CoV-2 Infection (COVID-19). Microorganisms 2020, 8, 1560. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.B.; Qiong-qiong, Z.; Ze-xiong, L.; Feng, Z. Association of Platelet-to-White Blood Cell Ratio and Platelet-to-Neutrophil Ratio with the Risk of Fatal Stroke Occurrence in Middle-Aged to Older Chinese. BMC Geriatr. 2022, 22, 430. [Google Scholar] [CrossRef]
- He, W.; Yiting, R.; Chengxiang, Y.; Qianqian, C.; Haoran, C.; Yaying, Z.; Yunbin, C.; Guiqian, H.; Huijun, C.; Jincai, H. High Neutrophil-to-Platelet Ratio Is Associated with Hemorrhagic Transformation in Patients with Acute Ischemic Stroke. Front. Neurol. 2019, 10, 1310. [Google Scholar] [CrossRef]
- Cheng, H.R.; Jia-Ying, S.; Yi-Nuo, Z.; Yun-Bin, C.; Gang-Qiang, L.; Gui-Qian, H.; Jin-Cai, H.; Zhen, W. High Monocyte-to-Lymphocyte Ratio Is Associated with Stroke-Associated Pneumonia. Front. Neurol. 2020, 11, 575809. [Google Scholar] [CrossRef]
- Chen, H.; Min, L.; Lei, L.; Xiawei, D.; Danjun, Z.; Gang, T. Monocyte/Lymphocyte Ratio Is Related to the Severity of Coronary Artery Disease and Clinical Outcome in Patients with Non-St-Elevation Myocardial Infarction. Medicine 2019, 98, e16267. [Google Scholar] [CrossRef]
- Zhang, M.; Qiuxia, G.; Tengfei, Q.; Yaman, W.; Xiaohong, X.; Xiang, Z.; Jun, Z. Prognostic Value of Lymphocyte-to-White Blood Cell Ratio for in-Hospital Mortality in Infective Endocarditis Patients. Int. J. Clin. Pract. 2022, 2022, 8667054. [Google Scholar] [CrossRef] [PubMed]
- Feng, F.; Li, S.; Gaozan, Z.; Shushang, L.; Zhen, L.; Guanghui, X.; Man, G.; Xiao, L.; Daiming, F.; Hongwei, Z. Low Lymphocyte-to-White Blood Cell Ratio and High Monocyte-to-White Blood Cell Ratio Predict Poor Prognosis in Gastric Cancer. Oncotarget 2016, 8, 5281–5291. [Google Scholar] [CrossRef] [Green Version]
- Gawiński, C.; Michalski, W.; Mróz, A.; Wyrwicz, L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in Left-Sided Colorectal Cancer Patients. Biology 2022, 11, 385. [Google Scholar] [CrossRef]
- Lang, C.; Egger, F.; Hoda, M.A.; Querner, A.S.; Ferencz, B.; Lungu, V.; Szegedi, R.; Bogyo, L.; Torok, K.; Oberndorfer, F.; et al. Lymphocyte-to-monocyte ratio is an independent prognostic factor in surgically treated small cell lung cancer: An international multicenter analysis. Lung Cancer 2022, 169, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, J.; Haocheng, L.; Scott, A.N.; Raya, L.A.; Jo-An, S.; Nisha, M.; Caroline, C.; Lee-Ying, R.; Heng, D.Y.; Sridhar, S.; et al. The prognostic role of the change in neutrophil-to-lymphocyte ratio during neoadjuvant chemotherapy in patients with muscle-invasive bladder cancer: A retrospective, multi-institutional study. Bladder Cancer 2018, 4, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Bacușcă, A.E.; Burlacu, A.; Tinică, G.; Enache, M.; Ţărus, A.; Gavriluţă, C.; Brinza, C.; Hanganu, B.; Ioan, B.G. Organ Procurement, Donation, and Transplant Awareness in an Urban Eastern European Region: A General Population Survey. Ann. Transplant. 2022, 27, e938016. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Receipt |
|---|---|
Age (years)
| 41.21 (13.71) 10 61 |
Body Mass Index (kg/m2)
| 23.81 (5.18) 13.2 33.9 |
Ejection fraction (%)
| 26.54 (13.23) 15 65 |
Pulmonary artery pressure (mmHg)
| 52.08 (15.70) 22 82 |
Hemoglobin (g/dL)
| 13.08 (2.44) 8.1 19.0 |
White Blood Cell count (×109/L)
| 8.99 (4.26) 3.47 24.7 |
Neutrophil count (×109/L)
| 6.51 (4.17) 2.09 22.4 |
Lymphocyte count (×109/L)
| 1.61 (0.76) 0.38 3.17 |
Monocyte count (×109/L)
| 0.77 (0.34) 0.17 1.89 |
Platelet count (×109/L)
| 202.11 (62.61) 82 327 |
Creatinine level (md/dL)
| 1.07 (0.32) 0.54 1.82 |
Estimated glomerular filtration rate (mL/min/1.73 m2)
| 91.79 (29.06) 45 156 |
Total cholesterol level (mg/dL)
| 164.74 (44.94) 68 269 |
Low-density lipoprotein cholesterol (mg/dL)
| 106.05 (33.52) 42 182 |
High-density lipoprotein cholesterol (mg/dL)
| 36.47 (10.43) 13 59 |
Triglycerides level (mg/dL)
| 112.53 (53.32) 57 281 |
Prior percutaneous coronary intervention
| 4 10.53% |
Prior cardiac surgery
| 5 13.15% |
Heart valve surgery
| 4 10.53% |
Donors
| 31.39 (10.67) 26 (68.4%) 12 (31.6%) |
Gender mismatch
| 14 (36.8%) 3 (7.9%) 11 (28.9%) |
| Markers | Preoperative | Postoperative | p Values |
CRP *
| 0.43 0.24 0.88 | 6.37 4.19 11.69 | <0.0001 |
NMR *
| 8.23 5.97 9.82 | 17.54 10.92 23.11 | <0.0001 |
NLR *
| 3.39 2.38 5.89 | 21.54 13.74 35.58 | <0.0001 |
NPR *
| 0.027 0.021 0.036 | 0.112 0.087 0.155 | <0.0001 |
NWR *
| 0.69 0.64 0.79 | 0.89 0.87 0.92 | <0.0001 |
MLR *
| 0.46 0.33 0.76 | 1.33 0.07 2.08 | 0.0001 |
PLR *
| 124.4 80.8 221.6 | 224 110 296.3 | 0.0268 |
MWR *
| 0.09 0.07 0.11 | 0.05 0.03 0.07 | <0.0001 |
LWR *
| 0.20 0.12 0.25 | 0.04 0.02 0.06 | <0.0001 |
| Complications ORR/95% CI | Type 2 DM ORR/95% CI | Paroxysmal AFib ORR/95% CI | Acute Rejection ORR/95% CI | Infections ORR/95% CI | |
|---|---|---|---|---|---|
| NMR > 8.9 | 0.73 0.07–7.46 | 0.38 0.02–6.89 | 70.71 3.39–1473.64 | 0.41 0.01–10.59 | 0.25 0.01–3.37 |
| NLR > 2.9 | 0.81 0.10–6.14 | 0.85 0.14–5.18 | 3.38 0.33–34.58 | 1.44 0.19–10.53 | 1.41 0.25–7.82 |
| NLR > 2.06 | 0.67 0.02–16.82 | - * - | - * - | 0.17 0.007–4.31 | 3.68 0.11–121.37 |
| NPR > 0.018 | 0.97 0.04–19.96 | - * - | - * - | 0.82 0.05–11.35 | 0.52 0.03–6.98 |
| NWR > 0.55 | - * - | - * - | - * - | - * - | - * - |
| MLR > 0.35 | 2.80 0.33–23.31 | 0.75 0.09 -5.67 | 1.70 0.15–19.10 | 0.54 0.05–5.01 | 2.28 0.28–18.67 |
| PLR > 204 | 3.35 0.25–43.66 | 0.98 0.12–8.08 | 0.42 0.03–5.18 | 0 - | 1.21 0.20–7.17 |
| MWR > 0.09 | 14.74 1.05–206.59 | 0.96 0.11–8.10 | 0.04 0.003–0.58 | 1.56 0.12–19.97 | 2.67 0.32–21.97 |
| LWR > 0.28 | 1.56 0.10–23.82 | 0.66 0.05–7.81 | 0 - | 0.55 0.04–7.07 | 1.66 0.20–13.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baba, D.-F.; Suciu, H.; Avram, C.; Gyorgy, M.; Danilesco, A.; Huma, L.; Sin, I.A. Elevated Levels of Neutrophil-to Monocyte Ratio Are Associated with the Initiation of Paroxysmal Documented Atrial Fibrillation in the First Two Months after Heart Transplantation: A Uni-Institutional Retrospective Study. J. Cardiovasc. Dev. Dis. 2023, 10, 81. https://doi.org/10.3390/jcdd10020081
Baba D-F, Suciu H, Avram C, Gyorgy M, Danilesco A, Huma L, Sin IA. Elevated Levels of Neutrophil-to Monocyte Ratio Are Associated with the Initiation of Paroxysmal Documented Atrial Fibrillation in the First Two Months after Heart Transplantation: A Uni-Institutional Retrospective Study. Journal of Cardiovascular Development and Disease. 2023; 10(2):81. https://doi.org/10.3390/jcdd10020081
Chicago/Turabian StyleBaba, Dragos-Florin, Horatiu Suciu, Calin Avram, Manuela Gyorgy, Alina Danilesco, Laurentiu Huma, and Ileana Anca Sin. 2023. "Elevated Levels of Neutrophil-to Monocyte Ratio Are Associated with the Initiation of Paroxysmal Documented Atrial Fibrillation in the First Two Months after Heart Transplantation: A Uni-Institutional Retrospective Study" Journal of Cardiovascular Development and Disease 10, no. 2: 81. https://doi.org/10.3390/jcdd10020081
APA StyleBaba, D. -F., Suciu, H., Avram, C., Gyorgy, M., Danilesco, A., Huma, L., & Sin, I. A. (2023). Elevated Levels of Neutrophil-to Monocyte Ratio Are Associated with the Initiation of Paroxysmal Documented Atrial Fibrillation in the First Two Months after Heart Transplantation: A Uni-Institutional Retrospective Study. Journal of Cardiovascular Development and Disease, 10(2), 81. https://doi.org/10.3390/jcdd10020081