
Comparison of Mid-Term Prognosis in Intermediate-to-Low-Risk Contemporary Population with Guidelines-Oriented Age Cutoff

 , , , ,
, , , , 
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Baseline and Procedural Features
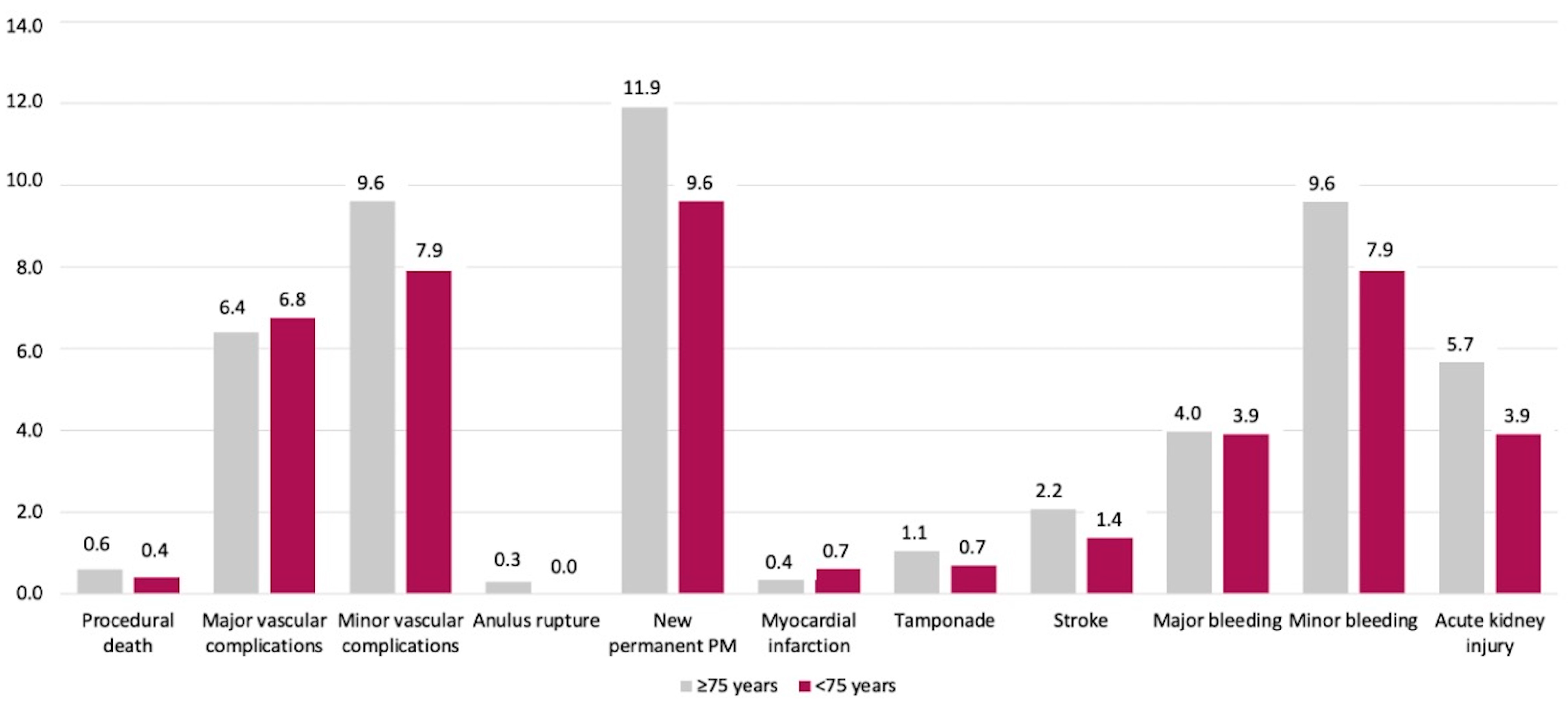
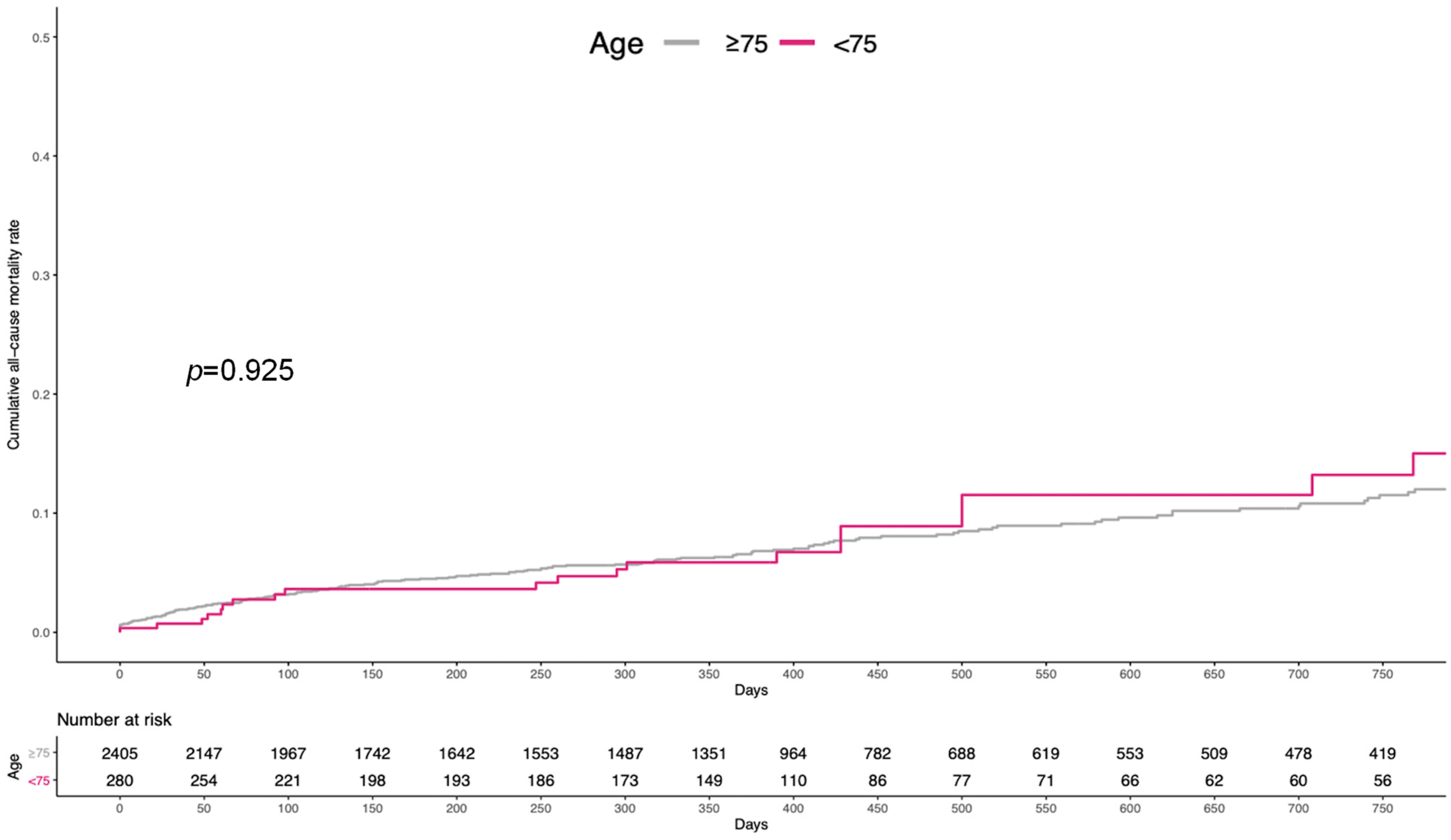
3.2. Clinical Outcomes
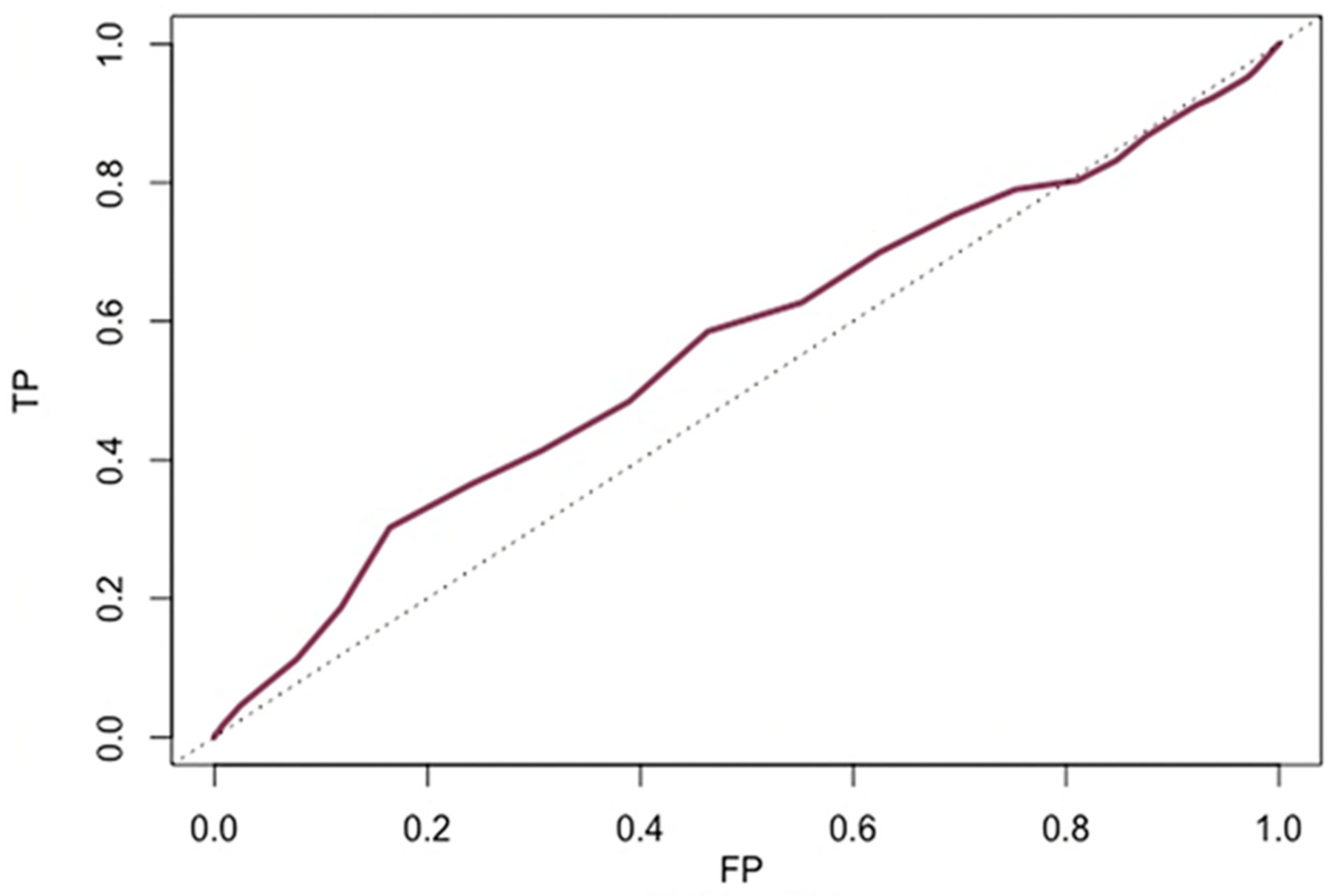
3.3. Accuracy of Age to Predict All-Cause Mortality
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Søndergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Landes, U.; Webb, J.G.; De Backer, O.; Sondergaard, L.; Abdel-Wahab, M.; Crusius, L.; Kim, W.-K.; Hamm, C.; Buzzatti, N.; Montorfano, M.; et al. Repeat Transcatheter Aortic Valve Replacement for Transcatheter Prosthesis Dysfunction. J. Am. Coll. Cardiol. 2020, 75, 1882–1893. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, L.; Steinbrüchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Ngo, A.T.; Olsen, N.T.; Chang, Y.; Franzen, O.W.; et al. Two-Year Outcomes in Patients With Severe Aortic Valve Stenosis Randomized to Transcatheter Versus Surgical Aortic Valve Replacement: The All-Comers Nordic Aortic Valve Intervention Randomized Clinical Trial. Circ. Cardiovasc. Interv. 2016, 9, e003665. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed]
- Galappatthy, G. Outcome of 511 Atrial Septal Defect Device Closures without Balloon Sizing. Catheter. Cardiovasc. Interv. 2013, 81, S23–S24. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Gallo, F.; Gallone, G.; Kim, W.K.; Reifart, J.; Veulemans, V.; Zeus, T.; Toggweiler, S.; De Backer, O.; Søndergaard, L.; Mangieri, A.; et al. Horizontal Aorta in Transcatheter Self-Expanding Valves: Insights From the HORSE International Multicentre Registry. Circ. Cardiovasc. Interv. 2021, 14, e010641. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; Van Es, G.A.; et al. Updated Standardized Endpoint Definitions for Transcatheter Aortic Valve Implantation: The Valve Academic Research Consortium-2 Consensus Document. Eur. Heart J. 2012, 33, 2403–2418. [Google Scholar] [CrossRef] [PubMed]
- Attinger-Toller, A.; Ferrari, E.; Tueller, D.; Templin, C.; Muller, O.; Nietlispach, F.; Toggweiler, S.; Noble, S.; Roffi, M.; Jeger, R.; et al. Age-Related Outcomes After Transcatheter Aortic Valve Replacement: Insights From the SwissTAVI Registry. JACC. Cardiovasc. Interv. 2021, 14, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Vlastra, W.; Chandrasekhar, J.; Vendrik, J.; Gutierrez-Ibanes, E.; Tchétché, D.; de Brito, F.S.; Barbanti, M.; Kornowski, R.; Latib, A.; D’Onofrio, A.; et al. Transfemoral TAVR in Nonagenarians: From the CENTER Collaboration. JACC. Cardiovasc. Interv. 2019, 12, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Delgado, V.; Bapat, V.; Baumgartner, H.; Collet, J.P.; Erbel, R.; Hamm, C.; Kappetein, A.P.; Leipsic, J.; Leon, M.B.; et al. Open Issues in Transcatheter Aortic Valve Implantation. Part 1: Patient Selection and Treatment Strategy for Transcatheter Aortic Valve Implantation. Eur. Heart J. 2014, 35, 2627–2638. [Google Scholar] [CrossRef] [PubMed]
- Laricchia, A.; Cereda, A.; Lucreziotti, S.; Sticchi, A.; Regazzoli, D.; Reimers, B.; Colombo, A.; Latib, A.; Mangieri, A. Expanding Our Horizons for the Use of Transcatheter Self-Expanding Valves: What Does the Future Hold? Expert Rev. Cardiovasc. Ther. 2022, 20, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Pibarot, P.; Hahn, R.T.; Genereux, P.; Kodali, S.K.; Kapadia, S.R.; Cohen, D.J.; Pocock, S.J.; et al. Transcatheter Aortic-Valve Replacement in Low-Risk Patients at Five Years. N. Engl. J. Med. 2023, 389, 1949–1960. [Google Scholar] [CrossRef] [PubMed]
- Forrest, J.K.; Deeb, G.M.; Yakubov, S.J.; Gada, H.; Mumtaz, M.A.; Ramlawi, B.; Bajwa, T.; Teirstein, P.S.; Tchétché, D.; Huang, J.; et al. 4-Year Outcomes of Patients With Aortic Stenosis in the Evolut Low Risk Trial. J. Am. Coll. Cardiol. 2023, 82, 2163–2165. [Google Scholar] [CrossRef]
- Eggebrecht, H.; Bestehorn, K.; Rassaf, T.; Bestehorn, M.; Voigtländer, T.; Fleck, E.; Schächinger, V.; Schmermund, A.; Mehta, R.H. In-Hospital Outcomes after Transcatheter or Surgical Aortic Valve Replacement in Younger Patients Less than 75 Years Old: A Propensity-Matched Comparison. EuroIntervention 2018, 14, 50–57. [Google Scholar] [CrossRef]
- Witberg, G.; Landes, U.; Codner, P.; Barbanti, M.; Valvo, R.; De Backer, O.; Ooms, J.F.; McInerney, A.; Masiero, G.; Werner, P.; et al. Clinical Outcomes of Transcatheter Aortic Valve Implantation in Patients Younger than 70 Years Rejected for Surgery: The AMTRAC Registry. EuroIntervention 2022, 17, 1289–1297. [Google Scholar] [CrossRef]
- Johnston, D.R.; Soltesz, E.G.; Vakil, N.; Rajeswaran, J.; Roselli, E.E.; Sabik, J.F.; Smedira, N.G.; Svensson, L.G.; Lytle, B.W.; Blackstone, E.H. Long-Term Durability of Bioprosthetic Aortic Valves: Implications from 12,569 Implants. Ann. Thorac. Surg. 2015, 99, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, A.A.; Ponticelli, F.; Zlahoda-Huzior, A.; Chandra, K.; Ruggiero, R.; Toselli, M.; Gallo, F.; Cereda, A.; Sticchi, A.; Laricchia, A.; et al. Coronary Access Following ACURATE Neo Implantation for Transcatheter Aortic Valve-in-Valve Implantation: Ex Vivo Analysis in Patient-Specific Anatomies. Front. Cardiovasc. Med. 2022, 9, 902564. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M. Alignment and Divergence in European and North American Aortic Stenosis Guidelines. EuroIntervention 2022, 17, E1123–E1125. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All N = 2685 | ≥75 Years N = 2405 | <75 Years N = 280 | p-Value | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age, years | 82 (79–86) | 83 (80–86) | 72 (69–73) | <0.001 |
| Male sex | 960 (36) | 835 (35) | 125 (45) | 0.001 |
| Body mass index, kg/m2 | 26.9 (24–31) | 26.7 (24–30) | 28.5 (24–33) | <0.001 |
| Hypertension | 2334 (87) | 2092 (87) | 242 (86) | 0.813 |
| Dyslipidemia | 1035 (52) | 925 (52) | 110 (51) | 0.933 |
| Diabetes | 705 (26) | 613 (25) | 92 (33) | 0.010 |
| Smoke | 228 (15) | 176 (7) | 52 (19) | <0.001 |
| Prior myocardial infarction | 482 (18) | 441 (18) | 41 (15) | 0.144 |
| Prior percutaneous coronary intervention | 731 (27) | 656 (27) | 75 (27) | 0.905 |
| Prior stroke | 287 (11) | 261 (11) | 26 (9) | 0.478 |
| Chronic obstructive pulmonary disease | 450 (17) | 381 (16) | 69 (25) | <0.001 |
| PM or ICD | 276 (10) | 259 (11) | 17 (6) | 0.019 |
| Atrial fibrillation | 2334 (87) | 795 (33) | 65 (23) | 0.010 |
| Chronic kidney disease | 1645 (61) | 1562 (65) | 83 (30) | <0.001 |
| Baseline creatinine, mg/dL | 1.10 (0.61) | 1.09 (0.55) | 1.19 (0.98) | 0.010 |
| Peripheral arterial disease | 333 (12) | 297 (12) | 36 (13) | 0.890 |
| NYHA III-IV | 1787 (67) | 1607 (67) | 180 (64) | 0.390 |
| STS score, % | 3.60 (2.50–5.03) | 3.73 (2.60–5.10) | 2.55 (1.75 4.10) | <0.001 |
| Low risk | 1520 (57) | 1318 (55) | 202 (72) | <0.001 |
| Intermediate risk | 1165 (43) | 1087 (45) | 78 (28) | <0.001 |
| Echocardiographic data | ||||
| Mean aortic valve gradient, mmHg | 45.1 (16.2) | 45.2 (16.3) | 44.9 (15.6) | 0.821 |
| Aortic valve area, mm2 | 0.76 (2.73) | 0.77 (2.87) | 0.73 (0.19) | 0.850 |
| Left ventricular ejection fraction, % | 57 (55–60) | 55 (52–58) | 60 (55–65) | 0.006 |
| Moderate-severe aortic regurgitation | 56 (3) | 51 (3) | 5 (2) | 0.966 |
| MDCT data | ||||
| Perimeter, mm | 70 (26–76) | 70 (26–76) | 71 (26–77) | 0.367 |
| Moderate–severe aortic valve calcification | 1173 (44) | 1055 (44) | 118 (42) | 0.971 |
| Moderate/severe LVOT calcification | 446 (16) | 408 (17) | 38 (14) | 0.224 |
| Porcelain aorta | 271 (10) | 225 (9) | 46 (16) | <0.001 |
| All N = 2685 | ≥75 Years N = 2405 | <75 Years N = 280 | p-Value | |
|---|---|---|---|---|
| Predilatation | 1452 (54) | 1309 (54) | 143 (51) | 0.309 |
| Valve type | ||||
| Evolute R | 1068 (40) | 963 (40) | 105 (38) | 0.449 |
| Evolute PRO | 301 (11) | 253 (11) | 48 (17) | 0.001 |
| ACURATE neo | 1316 (49) | 1189 (49) | 127 (45) | 0.219 |
| Valve size, mm | 0.025 | |||
| <23 | 423 (16) | 381 (16) | 42 (15) | |
| 23–26 | 1021 (38) | 933 (39) | 88 (31) | |
| ≥27 | 1241 (46) | 1091 (45) | 150 (54) | |
| Post-dilatation | 892 (33) | 788 (33) | 104 (37) | 0.153 |
| Contrast dose, ml | 110 (80–160) | 110 (80–160) | 110 (80–150) | 0.612 |
| Fluoroscopy time, minutes | 16 (10–24) | 16 (10–24) | 15 (10–23) | 0.244 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variable | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (1-year increase) | 1.01 (0.99–1.04) | 0.294 | ||
| Male sex | 1.14 (0.87–1.50) | 0.336 | ||
| Prior MI | 1.19 (0.84–1.68) | 0.323 | ||
| Diabetes | 1.05 (0.78–1.42) | 0.746 | ||
| NYHA III-IV | 1.92 (1.40–2.63) | <0.001 | 1.68 (1.23–2.35) | 0.001 |
| COPD | 1.12 (0.80–1.56) | 0.502 | ||
| Prior stroke | 1.02 (0.67–1.57) | 0.928 | ||
| PAD | 1.37 (0.96-.95) | 0.082 | ||
| CKD | 1.75 (1.30–2.37) | <0.001 | 1.47 (1.05–2.08) | 0.026 |
| AF | 1.48 (1.13–1.93) | 0.004 | 1.40 (1.06–1.84) | 0.016 |
| Baseline creatinine, mg/dL (1-unit increase) | 1.28 (1.09–1.50) | 0.002 | 1.12 (0.91–1.38) | 0.272 |
| Permanent PM or ICD | 1.20 (0.81–1.79) | 0.359 | ||
| STS score (1% increase) | 1.16 (1.08–1.26) | <0.001 | 1.12 (1.03–1.21) | 0.007 |
| EF (1% increase) | 0.99 (0.98–1.00) | 0.229 | ||
| Predilatation | 1.06 (0.82–1.39) | 0.648 | ||
| Post-dilatation | 1.02 (0.77–1.35) | 0.874 | ||
| Valve size, mm (vs. <23) | ||||
| 23–26 | 0.99 (0.65–1.53) | 0.993 | ||
| ≥27 | 1.28 (0.86–1.94) | 0.227 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benenati, S.; Gallo, F.; Kim, W.-k.; Khokhar, A.A.; Zeus, T.; Toggweiler, S.; Galea, R.; De Marco, F.; Mangieri, A.; Regazzoli, D.; et al. Comparison of Mid-Term Prognosis in Intermediate-to-Low-Risk Contemporary Population with Guidelines-Oriented Age Cutoff. J. Cardiovasc. Dev. Dis. 2024, 11, 33. https://doi.org/10.3390/jcdd11010033
Benenati S, Gallo F, Kim W-k, Khokhar AA, Zeus T, Toggweiler S, Galea R, De Marco F, Mangieri A, Regazzoli D, et al. Comparison of Mid-Term Prognosis in Intermediate-to-Low-Risk Contemporary Population with Guidelines-Oriented Age Cutoff. Journal of Cardiovascular Development and Disease. 2024; 11(1):33. https://doi.org/10.3390/jcdd11010033
Chicago/Turabian StyleBenenati, Stefano, Francesco Gallo, Won-keun Kim, Arif A. Khokhar, Tobias Zeus, Stefan Toggweiler, Roberto Galea, Federico De Marco, Antonio Mangieri, Damiano Regazzoli, and et al. 2024. "Comparison of Mid-Term Prognosis in Intermediate-to-Low-Risk Contemporary Population with Guidelines-Oriented Age Cutoff" Journal of Cardiovascular Development and Disease 11, no. 1: 33. https://doi.org/10.3390/jcdd11010033
APA StyleBenenati, S., Gallo, F., Kim, W. -k., Khokhar, A. A., Zeus, T., Toggweiler, S., Galea, R., De Marco, F., Mangieri, A., Regazzoli, D., Reimers, B., Nombela-Franco, L., Barbanti, M., Regueiro, A., Piva, T., Rodes-Cabau, J., Porto, I., Colombo, A., Giannini, F., & Sticchi, A. (2024). Comparison of Mid-Term Prognosis in Intermediate-to-Low-Risk Contemporary Population with Guidelines-Oriented Age Cutoff. Journal of Cardiovascular Development and Disease, 11(1), 33. https://doi.org/10.3390/jcdd11010033