
Metabolic Dysfunction Associated Liver Disease in Patients Undergoing Coronary Computed Tomography Angiography

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
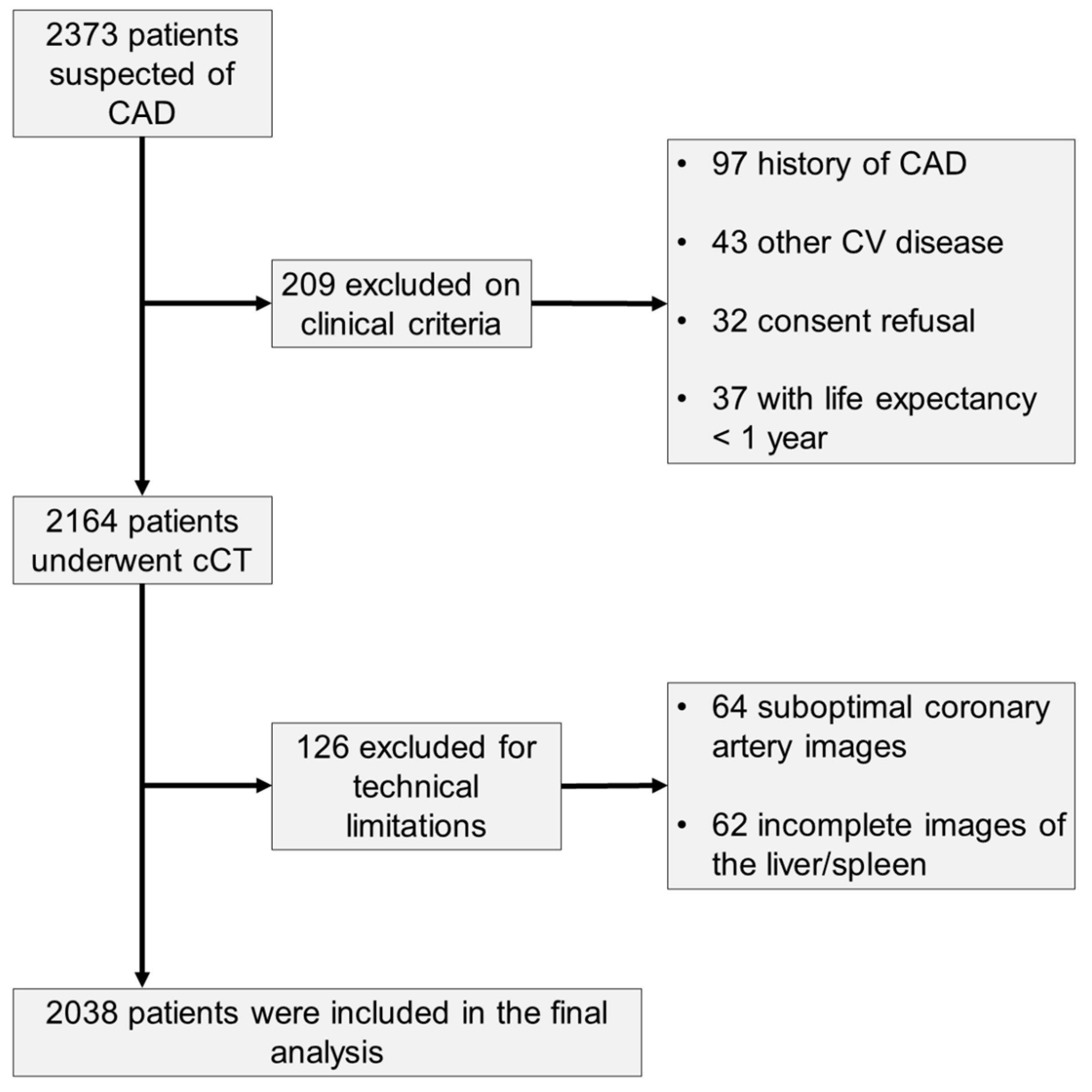
2.1. Study Population
2.2. Medical History and Clinical Examination
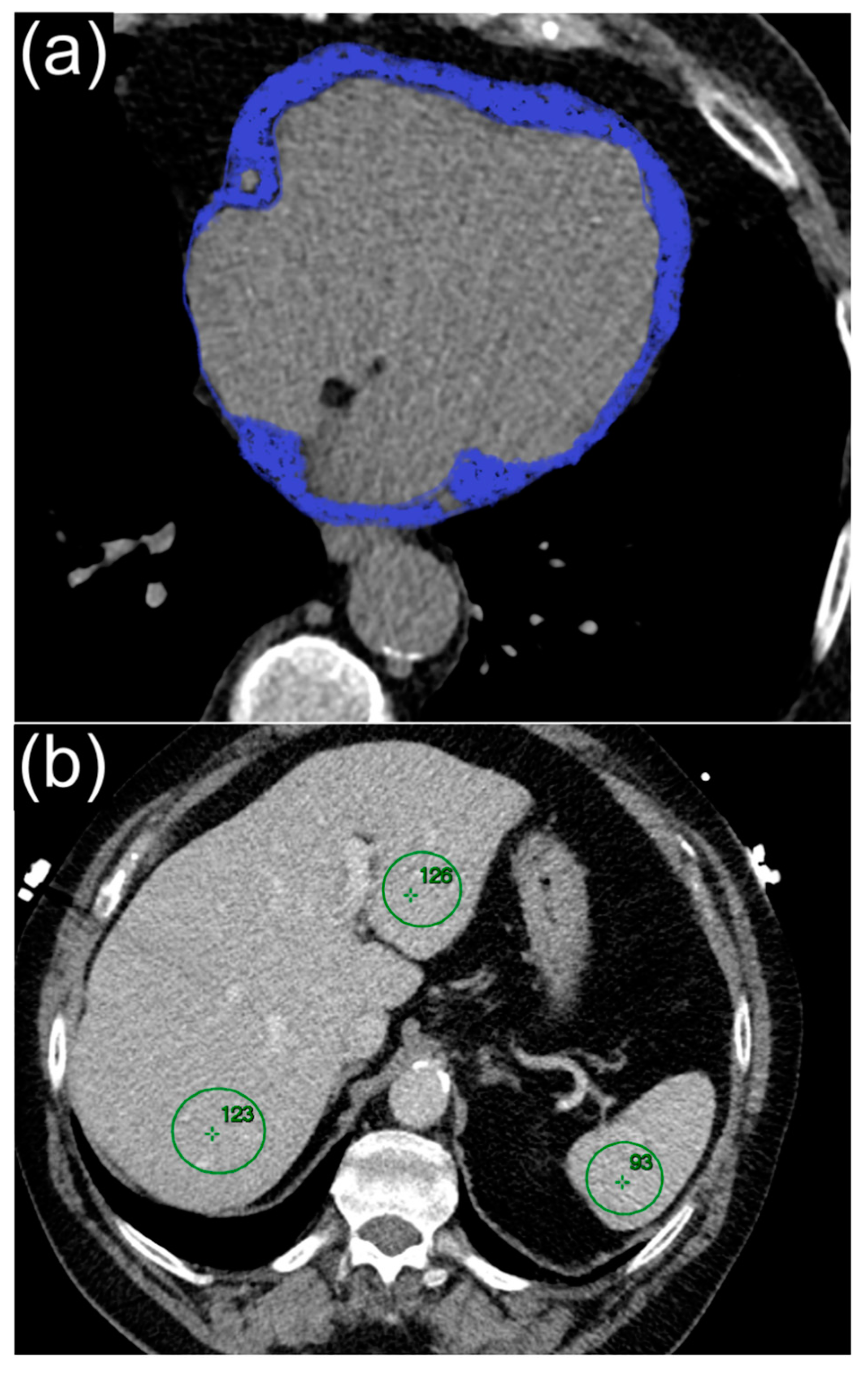
2.3. Cardiac Computed Tomography
2.4. Liver Fat Measurement
2.5. Clinical Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics and CT Measurements
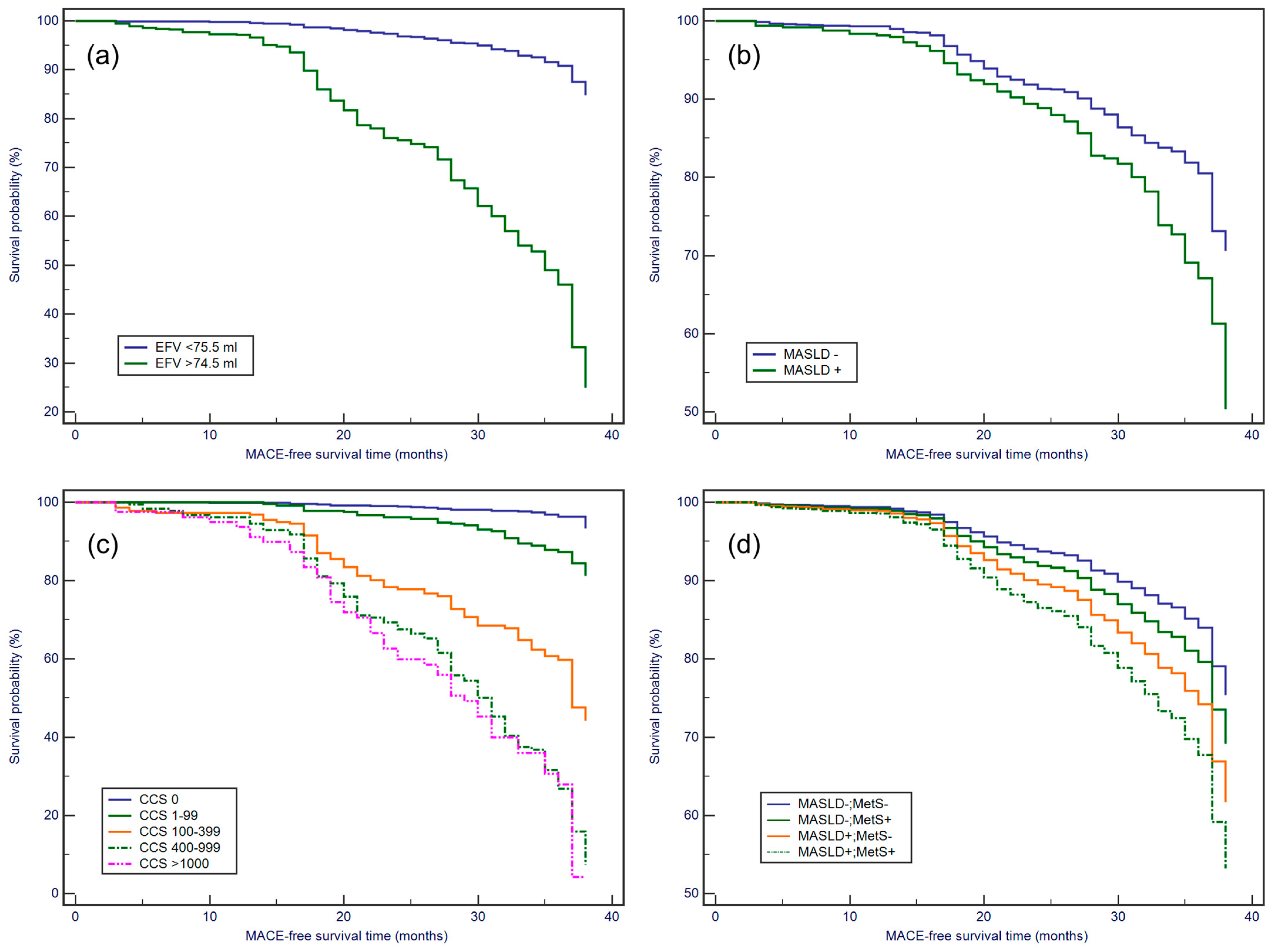
3.2. Kaplan–Meier Survival Analysis
3.3. Association of CCS, NoP, EFV, MASLD and MetS with MACE Risk in Multivariable Cox Regression
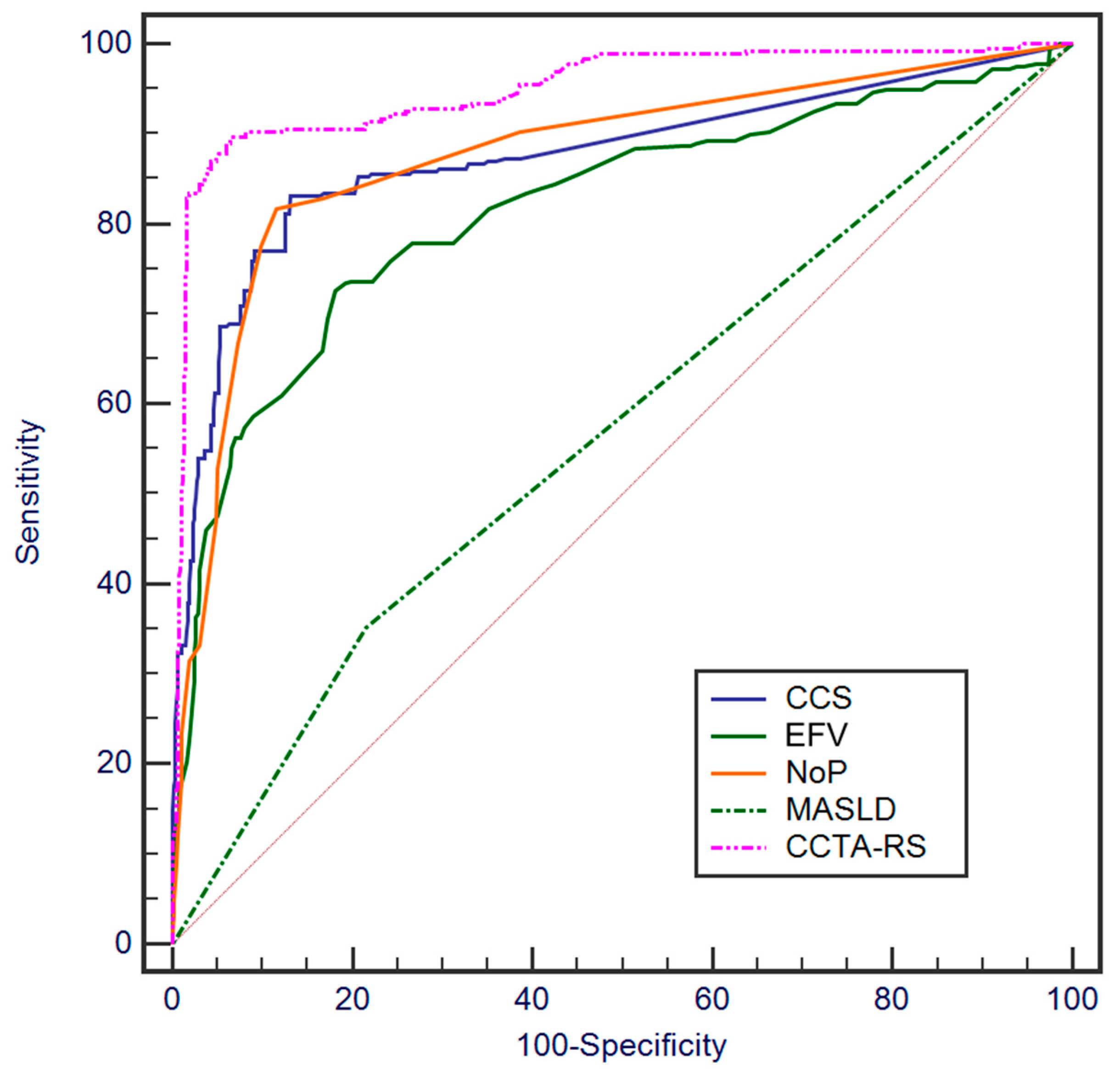
3.4. ROC Curve Analysis for Assessing the Ability to Predict MACE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASCVD | Atherosclerotic Cardiovascular Disease |
| AUC | area under the curve |
| BMI | body mass index |
| CAD | coronary artery disease |
| CCS | coronary calcium score |
| CCTA | coronary computed tomography angiography |
| CT | cardiac computed tomography |
| DM | diabetes mellitus |
| ECG | electrocardiogram |
| EFV | epicardial fat volume |
| eGFR | estimated glomerular filtration rate |
| HDL-C | high-density lipoprotein cholesterol |
| HU | Hounsfield Units |
| IQR | interquartile range |
| LDL-C | low-density lipoprotein cholesterol |
| MACEs | major adverse cardiovascular events |
| MASLD | metabolic dysfunction associated steatotic liver disease |
| NoPs | number of coronary plaques |
| NPV | negative predictive value |
| PPV | positive predictive value |
| ROC | receiver operating characteristics |
| Se | sensitivity |
| Sp | specificity |
References
- Bril, F.; Sanyal, A.; Cusi, K. Metabolic syndrome and its association with nonalcoholic steatohepatitis. Clin. Liver Dis. 2023, 27, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Riazi, K.; Azhari, H.; Charette, J.H.; E Underwood, F.; A King, J.; Afshar, E.E.; Swain, M.G.; E Congly, S.; Kaplan, G.G.; Shaheen, A.-A. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Meyersohn, N.M.; Mayrhofer, T.; Corey, K.E.; Bittner, D.O.; Staziaki, P.V.; Szilveszter, B.; Hallett, T.; Lu, M.T.; Puchner, S.B.; Simon, T.G.; et al. Association of hepatic steatosis with major adverse cardiovascular events, independent of coronary artery disease. Clin. Gastroenterol. Hepatol. 2021, 19, 1480–1488.e14. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Roelstraete, B.; Hagström, H.; Sundström, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef]
- Poyraz, N.; Özer, H.; Baloğlu, İ.; Kadıyoran, C.; Yılmaz, P.D.; Sertdemir, A.L.; Türkmen, K. Liver-spleen ratio: Can it be used for the prediction of Coronary Artery Disease? Anatol. J. Cardiol. 2022, 26, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Yerramasu, A.; Dey, D.; Venuraju, S.; Anand, D.V.; Atwal, S.; Corder, R.; Berman, D.S.; Lahiri, A. Increased volume of epicardial fat is an independent risk factor for accelerated progression of sub-clinical coronary atherosclerosis. Atherosclerosis 2012, 220, 223–230. [Google Scholar] [CrossRef]
- Orci, L.A.; Jornayvaz, F.R.; Toso, C.; Gariani, K. Systematic review and meta-analysis of the usefulness of epicardial fat thickness as a non-invasive marker of the presence and severity of nonalcoholic fatty liver disease. Biomedicines 2022, 10, 2204. [Google Scholar] [CrossRef]
- Park, S.; Lee, S.; Kim, Y.; Lee, Y.; Kang, M.W.; Han, K.; Han, S.S.; Lee, H.; Lee, J.P.; Joo, K.W.; et al. Altered risk for cardiovascular events with changes in the metabolic syndrome status: A nationwide population-based study of approximately 10 million persons. Ann. Intern. Med. 2019, 171, 875–884. [Google Scholar] [CrossRef]
- Scuteri, A.; Laurent, S.; Cucca, F.; Cockcroft, J.; Cunha, P.G.; Mañas, L.R.; Raso, F.U.M.; Muiesan, M.L.; Ryliškytė, L.; Rietzschel, E.; et al. Metabolic syndrome across Europe: Different clusters of risk factors. Eur. J. Prev. Cardiol. 2015, 22, 486–491. [Google Scholar] [CrossRef]
- Lin, A.; Wong, N.D.; Razipour, A.; McElhinney, P.A.; Commandeur, F.; Cadet, S.J.; Gransar, H.; Chen, X.; Cantu, S.; Miller, R.J.H.; et al. Metabolic syndrome, fatty liver, and artificial intelligence-based epicardial adipose tissue measures predict long-term risk of cardiac events: A prospective study. Cardiovasc. Diabetol. 2021, 20, 27. [Google Scholar] [CrossRef]
- Osborne-Grinter, M.; Kwiecinski, J.; Doris, M.; McElhinney, P.; Cadet, S.; Adamson, P.D.; Moss, A.J.; Alam, S.; Hunter, A.; Shah, A.S.V.; et al. Association of coronary artery calcium score with qualitatively and quantitatively assessed adverse plaque on coronary CT angiography in the SCOT-HEART trial. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1210–1221. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- American Diabetes Association Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 33, S62–S69. [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.-U. The Definition, Classification, and Prognosis of Chronic Kidney Disease: A KDIGO Controversies Conference Report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Leipsic, J.; Abbara, S.; Achenbach, S.; Cury, R.; Earls, J.P.; Mancini, G.J.; Nieman, K.; Pontone, G.; Raff, G.L. SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J. Cardiovasc. Comput. Tomogr. 2014, 8, 342–358. [Google Scholar] [CrossRef] [PubMed]
- Einstein, A.; Sanz, J.; Dellegrottaglie, S.; Milite, M.; Sirol, M.; Henzlova, M.; Rajagopalan, S. Radiation dose and cancer risk estimates in 16-slice computed tomography coronary angiography. J. Nucl. Cardiol. 2008, 15, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Chen, Y.; Zhang, Y.; Wang, H.; Tan, Y.; Liu, Y.; Huang, L.; Zhang, H.; Ma, Y.; Cong, H. Epicardial fat volume improves the prediction of obstructive coronary artery disease above traditional risk factors and coronary calcium score: Development and validation of new pretest probability models in Chinese populations. Circ. Cardiovasc. Imaging 2019, 12, e008002. [Google Scholar] [CrossRef] [PubMed]
- Kodama, Y.; Ng, C.S.; Wu, T.T.; Ayers, G.D.; Curley, S.A.; Abdalla, E.K.; Vauthey, J.N.; Charnsangavej, C. Comparison of CT methods for determining the fat content of the liver. Am. J. Roentgenol. 2007, 188, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Newsome, P.N.; Francque, S.M.; Kanwal, F.; Terrault, N.A.; Rinella, M.E. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 2023, 79, E93–E94. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Zinman, B.; Gross, J.L.; Canani, L.H.; Rodrigues, T.C.; Azevedo, M.J.; Retnakaran, R. Coronary artery calcium score prediction of all cause mortality and cardiovascular events in people with type 2 diabetes: Systematic review and meta-analysis. BMJ 2013, 346, f1654. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.K.; Yoon, J.W.; Lee, D.-H.; Kim, K.M.; Choi, S.H.; Park, K.S.; Jang, H.C.; Kim, M.-K.; Park, H.E.; Choi, S.-Y.; et al. Impact of metabolic syndrome on the progression of coronary calcium and of coronary artery disease assessed by repeated cardiac computed tomography scans. Cardiovasc. Diabetol. 2016, 15, 92. [Google Scholar] [CrossRef]
- Ahn, H.-J.; Lee, H.; Park, H.E.; Han, D.; Chang, H.-J.; Chun, E.J.; Han, H.-W.; Sung, J.; Jung, H.O.; Choi, S.-Y. Changes in metabolic syndrome burden and risk of coronary artery calcification progression in statin-naïve young adults. Atherosclerosis 2022, 360, 27–33. [Google Scholar] [CrossRef]
- Hoffmann, U.; Bamberg, F.; Chae, C.U.; Nichols, J.H.; Rogers, I.S.; Seneviratne, S.K.; Truong, Q.A.; Cury, R.C.; Abbara, S.; Shapiro, M.D.; et al. Coronary computed tomography angiography for early triage of patients with acute chest pain: The ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J. Am. Coll. Cardiol. 2009, 53, 1642–1650. [Google Scholar] [CrossRef]
- Eisenberg, E.; McElhinney, P.A.; Commandeur, F.; Chen, X.; Cadet, S.; Goeller, M.; Razipour, A.; Gransar, H.; Cantu, S.; Miller, R.J.; et al. Deep learning-based quantification of epicardial adipose tissue volume and attenuation predicts major adverse cardiovascular events in asymptomatic subjects. Circ. Cardiovasc. Imaging 2020, 13, e009829. [Google Scholar] [CrossRef]
- SCORE2 Working Group and ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 2038 | MASLD − n = 1540 | MASLD + n = 498 | p-Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| 57.2 (10.7) | 57.0 (10.8) | 58.0 (10.5) | 0.553 |
| 1060 (52.0) | 813 (52.8) | 247 (49.6) | 0.215 |
| 28.7 (5.5) | 27.5 (5.4) | 32.4 (5.8) | <0.001 |
| 137.4 (20.1) | 136.8 (20.2) | 139.2 (19.8) | 0.02 |
| 82.0 (12.1) | 81.8 (12.2) | 82.5 (11.7) | 0.261 |
| 7.1 (2.7–15.0) | 6.9 (2.6–14.8) | 8.2 (3.2–15.6) | 0.03 |
| CAD risk factors, n (%) | ||||
| 1295 (63.6) | 980 (63.7) | 315 (63.3) | 0.877 |
| 298 (14.6) | 201 (13.0) | 97 (19.4) | <0.001 |
| 1127 (55.3) | 743 (48.2) | 384 (77.1) | <0.001 |
| 779 (38.2) | 565 (36.7) | 214 (43.0) | 0.01 |
| 1009 (38.1) | 667 (43.3) | 342 (68.7) | <0.001 |
| 925 (45.4) | 614 (39.9) | 311 (62.4) | <0.001 |
| Biomarker levels, mean (SD) | ||||
| 108.7 (32.4) | 107.6 (30.1) | 112.1 (38.5) | <0.01 |
| 123.4 (42.5) | 123.4 (42.9) | 123.6 (43.1) | 0.928 |
| 45.9 (14.7) | 46.4 (14.3) | 44.3 (15.9) | <0.01 |
| 166.1 (28.9) | 165.1 (28.1) | 169.1 (31.2) | <0.01 |
| 90.2 (23.2) | 90.8 (23.3) | 88.7 (22.6) | 0.078 |
| Medications, n (%) | ||||
| 1515 (74.4) | 1134 (73.7) | 381 (76.5) | 0.202 |
| 978 (48.0) | 722 (46.9) | 256 (51.4) | 0.079 |
| 401 (19.7) | 321 (20.9) | 80 (16.1) | 0.02 |
| 928 (45.5) | 590 (38.3) | 338 (67.8) | <0.001 |
| 425 (20.8) | 301 (19.5) | 124 (24.9) | 0.01 |
| 520 (25.5) | 390 (25.3) | 130 (26.2) | 0.728 |
| Coronary Computer Tomographic Angiography | ||||
| 4.6 (0.0–109.7) | 2.9 (0.0–102.1) | 16.1 (1.4–118.6) | 0.01 |
| ||||
| 0 | 805 (39.5) | 681 (44.2) | 124 (24.9) | <0.001 |
| 1–99 | 543 (26.6) | 408 (26.5) | 135 (27.1) | 0.787 |
| 100–399 | 324 (15.9) | 206 (13.4) | 118 (23.7) | <0.001 |
| 400–999 | 286 (14.1) | 194 (12.6) | 92 (18.5) | 0.001 |
| >1000 | 80 (3.9) | 51 (3.3) | 29 (5.8) | 0.01 |
| ||||
| 0 | 776 (38.1) | 611 (39.7) | 165 (33.2) | 0.01 |
| 1–5 | 514 (25.2) | 366 (23.8) | 148 (29.7) | <0.01 |
| 6–10 | 692 (34.0) | 545 (35.4) | 147 (29.5) | 0.02 |
| >10 | 56 (2.7) | 18 (1.1) | 38 (7.6) | <0.001 |
| 64.1 (20.4) | 63.5 (20.2) | 65.9 (21.1) | 0.02 |
| 63.3 (7.7) | 65.0 (6.9) | 59.6 (8.5) | <0.01 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||
| Age | 1.25 (1.15–1.35) (p < 0.001) | 1.03 (1.02–1.04) (p < 0.001) | 1.011 (1.001–1.021) (p = 0.03) | 1.003 (0.993–1.013) (p = 0.51) | 1.01 (1.00–1.03) (p = 0.02) | 1.005 (0.995–1.014) (p = 0.36) |
| Male gender | 1.87 (1.51–.2.31) (p < 0.001) | 2.23 (1.32–3.77) (p = 0.003) | 1.57 (0.93–2.67) (p = 0.09) | 1.43 (0.84–2.42) (p = 0.18) | 1.56 (0.92–2.63) (p = 0.09) | 1.297 (0.761–2.211) (p = 0.34) |
| MetS | 1.56 (1.13–1.98) (p < 0.001) | 1.16 (0.68–1.98) (p = 0.59) | 1.21 (0.71–2.07) (p = 0.49) | 1.19 (0.69–2.03) (p = 0.52) | 1.08 (0.63–1.85) (p = 0.78) | 1.05 (0.61–1.79) (p = 0.86) |
| CCS | 1.0013 (1.0012–1.0014) (p < 0.001) | – | 1.0012 (1.0011–1.0013) (p < 0.001) | – | – | 1.001 (1.000–1.001) (p < 0.001) |
| NoP | 1.16 (1.15–1.18) (p < 0.001) | – | – | 1.16 (1.14–1.18) (p < 0.001) | – | 1.097 (1.075–1.119) (p < 0.001) |
| EFV | 1.053 (1.047–1.058) (p < 0.001) | – | – | – | 1.05 (1.04–1.06) (p < 0.001) | 1.035 (1.030–1.041) (p < 0.001) |
| MASLD | 1.67 (1.34–2.07) (p < 0.001) | – | – | – | – | 1.843 (1.475–2.303) (p < 0.001) |
| p-value Hosmer–Lemeshow | <0.001 | <0.0001 | <0.001 | <0.001 | <0.0001 | |
| CCTA–RS vs. | Δ AUC | p |
|---|---|---|
| NoP | 0.072 (0.058–0.086) | <0.001 |
| CCS | 0.075 (0.058–0.091) | <0.0001 |
| EFV | 0.132 (0.106–0.158) | <0.0001 |
| MASLD | 0.381 (0.347–0.415) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzan, R.I.; Gligor, R.I.; Agoston, R.; Cionca, C.; Zlibut, A.; Pais, R.; Seicean, A.; Agoston-Coldea, L. Metabolic Dysfunction Associated Liver Disease in Patients Undergoing Coronary Computed Tomography Angiography. J. Cardiovasc. Dev. Dis. 2024, 11, 77. https://doi.org/10.3390/jcdd11030077
Orzan RI, Gligor RI, Agoston R, Cionca C, Zlibut A, Pais R, Seicean A, Agoston-Coldea L. Metabolic Dysfunction Associated Liver Disease in Patients Undergoing Coronary Computed Tomography Angiography. Journal of Cardiovascular Development and Disease. 2024; 11(3):77. https://doi.org/10.3390/jcdd11030077
Chicago/Turabian StyleOrzan, Rares Ilie, Rares Ioan Gligor, Renata Agoston, Carmen Cionca, Alexandru Zlibut, Raluca Pais, Andrada Seicean, and Lucia Agoston-Coldea. 2024. "Metabolic Dysfunction Associated Liver Disease in Patients Undergoing Coronary Computed Tomography Angiography" Journal of Cardiovascular Development and Disease 11, no. 3: 77. https://doi.org/10.3390/jcdd11030077
APA StyleOrzan, R. I., Gligor, R. I., Agoston, R., Cionca, C., Zlibut, A., Pais, R., Seicean, A., & Agoston-Coldea, L. (2024). Metabolic Dysfunction Associated Liver Disease in Patients Undergoing Coronary Computed Tomography Angiography. Journal of Cardiovascular Development and Disease, 11(3), 77. https://doi.org/10.3390/jcdd11030077