
The Relationship between Subclinical Hypothyroidism and Carotid Intima-Media Thickness as a Potential Marker of Cardiovascular Risk: A Systematic Review and a Meta-Analysis

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Method
2.2. Selection Criteria
2.3. Data Collection and Analysis
2.4. Quality Assessment
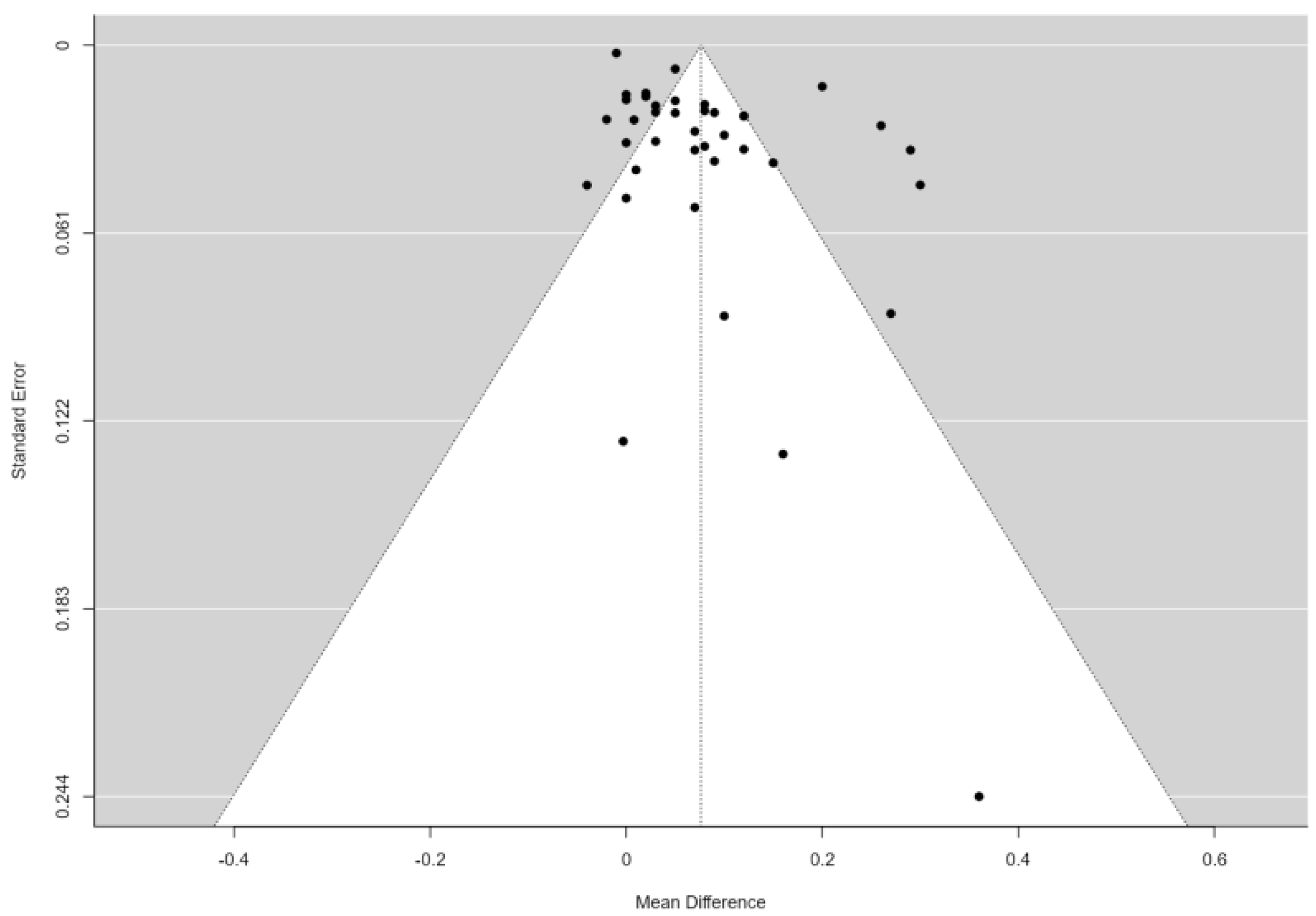
2.5. Statistical Analysis and Risk of Bias
3. Results
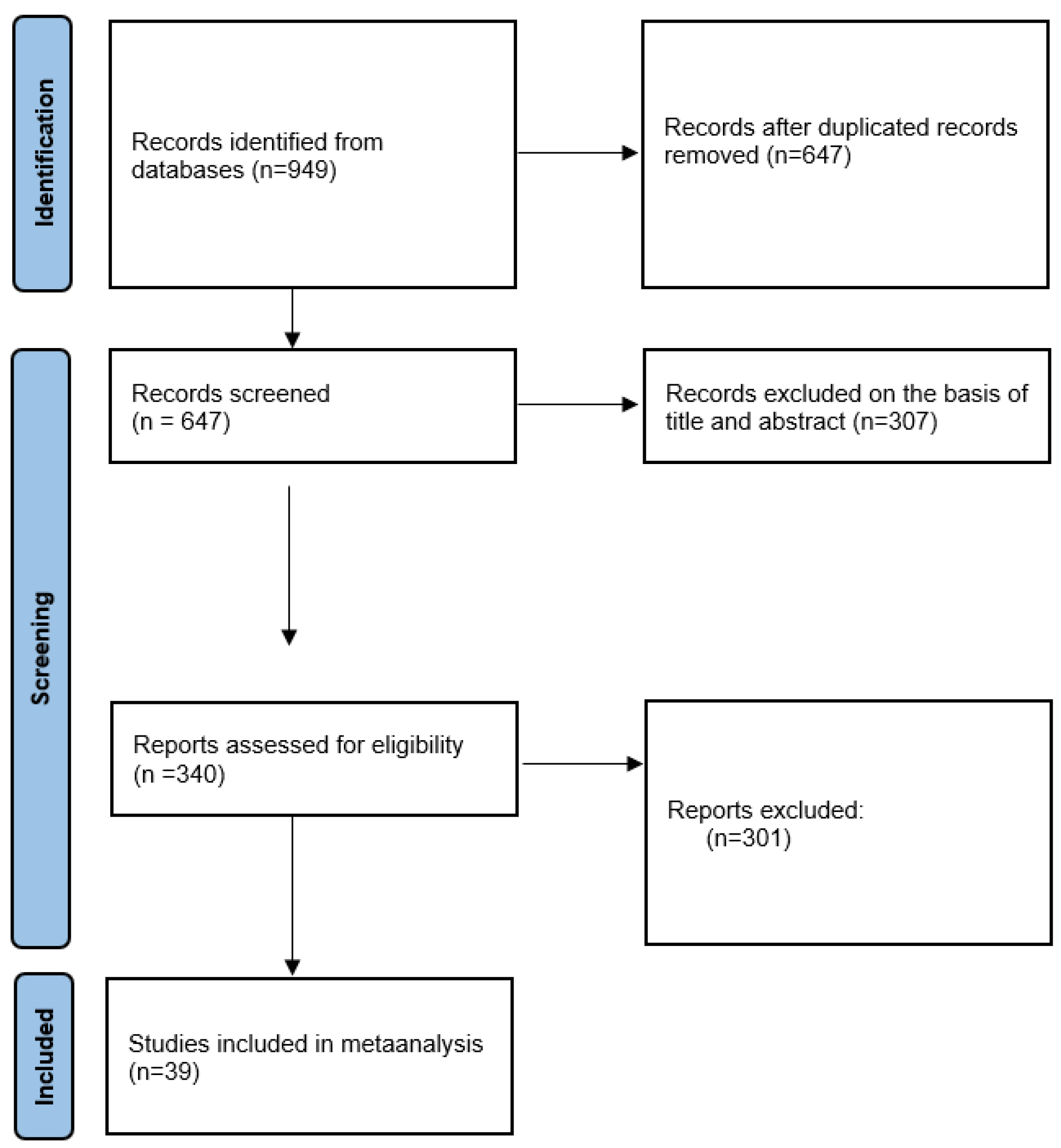
3.1. Study Selection
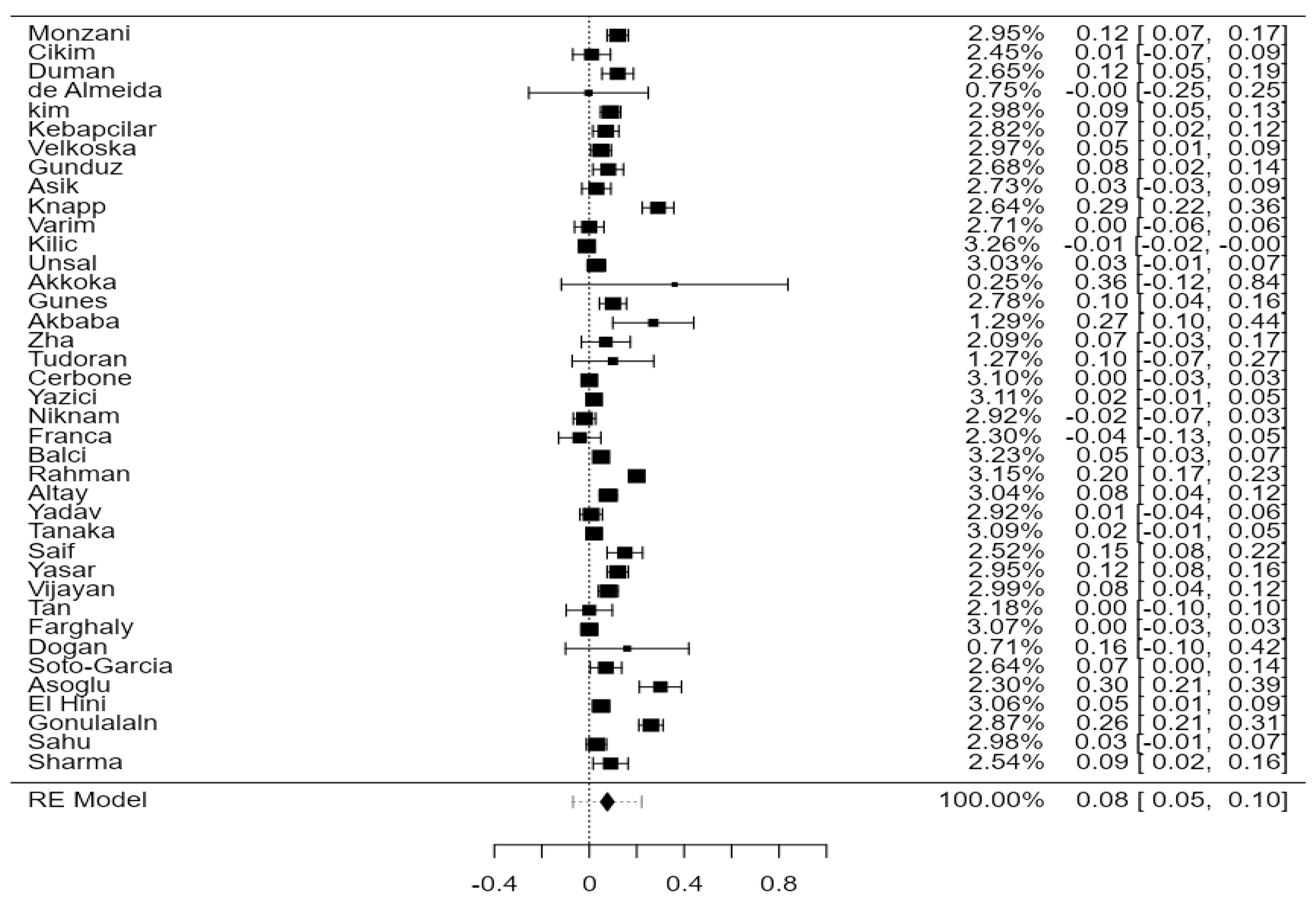
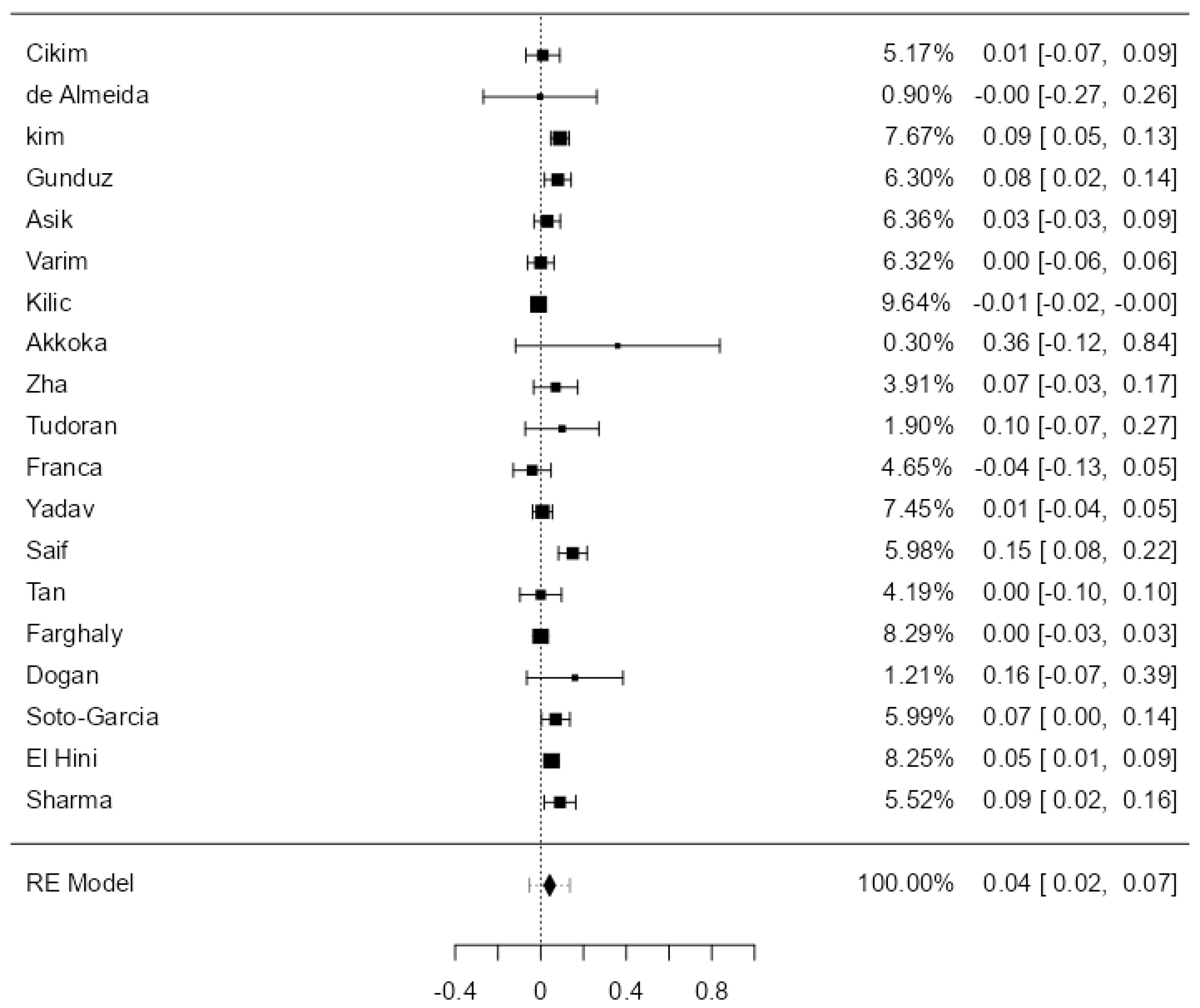
3.2. CIMT in SCH Versus EU
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cooper, D.S. Clinical Practice. Subclinical hypothyroidism. N. Engl. J. Med. 2001, 345, 260–265. [Google Scholar] [CrossRef]
- Al Eidan, E.; Rahman, S.U.; Al Qahtani, S.; Al Farhan, A.I.; Abdulmajeed, I. Prevalence of subclinical hypothyroidism in adults visiting primary health-care setting in Riyadh. J. Community Hosp. Intern. Med. Perspect. 2018, 8, 11–15. [Google Scholar] [CrossRef]
- Rohil, V.; Mishra, A.K.; Shrewastawa, M.K.; Mehta, K.D.; Lamsal, M.; Baral, N.; Majhi, S. Subclinical hypothyroidism in eastern Nepal: A hospital based study. Kathmandu Univ. Med. J. (KUMJ) 2010, 8, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Risal, P.; Adhikari, B.; Shrestha, R.; Manandhar, S.; Bhatt, R.D.; Hada, M. Analysis of Factors Associated with Thyroid Dysfunction: A Hospital Based Study. Kathmandu Univ. Med. J. (KUMJ) 2019, 17, 88–92. [Google Scholar] [PubMed]
- Abu-Helalah, M.; Alshraideh, H.A.; Al-Sarayreh, S.A.; Al Shawabkeh, A.H.K.; Nesheiwat, A.; Younes, N.; Al-Hader, A. A Cross-Sectional Study to Assess the Prevalence of Adult Thyroid Dysfunction Disorders in Jordan. Thyroid 2019, 29, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [CrossRef] [PubMed]
- Cobble, M.; Bale, B. Carotid intima-media thickness: Knowledge and application to everyday practice. Postgrad. Med. 2010, 122, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Hak, A.E.; Pols, H.A.; Visser, T.J.; Drexhage, H.A.; Hofman, A.; Witteman, J.C. Subclinical hypothyroidism is an independent risk factor for atherosclerosis and myocardial infarction in elderly women: The Rotterdam Study. Ann. Intern. Med. 2000, 132, 270–278. [Google Scholar] [CrossRef]
- Razvi, S.; Weaver, J.U.; Vanderpump, M.P.; Pearce, S.H.S. The incidence of ischemic heart disease and mortality in people with subclinical hypothyroidism: Reanalysis of the Whickham Survey cohort. J. Clin. Endocrinol. Metab. 2010, 95, 1734–1740. [Google Scholar] [CrossRef]
- Türemen, E.E.; Çetinarslan, B.; Sahin, T.; Cantürk, Z.; Tarkun, I. Endothelial dysfunction and low grade chronic inflammation in subclinical hypothyroidism due to autoimmune thyroiditis. Endocr. J. 2011, 58, 349–354. [Google Scholar] [CrossRef]
- Dardano, A.; Ghiadoni, L.; Plantinga, Y.; Caraccio, N.; Bemi, A.; Duranti, E.; Taddei, S.; Ferrannini, E.; Salvetti, A.; Monzani, F. Recombinant human thyrotropin reduces endothelium-dependent vasodilation in patients monitored for differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 4175–4178. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Wang, J.; Jiang, F.; Wang, B.; Chen, Y.; Li, M.; Liu, H.; Li, C.; Xue, H.; Li, N.; et al. The relationship between serum thyrotropin and components of metabolic syndrome. Endocr. J. 2011, 58, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Yang, C.-B.; Gao, L.; Zhao, J.-J. Mechanism of subclinical hypothyroidism accelerating endothelial dysfunction (Review). Exp. Ther. Med. 2015, 9, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. Available online: https://www.bmj.com/content/372/bmj.n71 (accessed on 18 December 2022). [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023). Cochrane. 2023. Available online: www.training.cochrane.org/handbook (accessed on 3 December 2023).
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- HKBU-Math, Estimating the Sample Mean and Standard Deviation (SD) from the Five-Number Summary and Its Application in Meta-Analysis. Available online: https://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html (accessed on 20 January 2023).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 January 2023).
- Monzani, F.; Caraccio, N.; Kozàkowà, M.; Dardano, A.; Vittone, F.; Virdis, A.; Taddei, S.; Palombo, C.; Ferrannini, E. Effect of levothyroxine replacement on lipid profile and intima-media thickness in subclinical hypothyroidism: A double-blind, placebo-controlled study. J. Clin. Endocrinol. Metab. 2004, 89, 2099–2106. [Google Scholar] [CrossRef]
- Cikim, A.S.; Oflaz, H.; Ozbey, N.; Cikim, K.; Umman, S.; Meric, M.; Sencer, E.; Molvalilar, S. Evaluation of Endothelial Function in Subclinical Hypothyroidism and Subclinical Hyperthyroidism. Thyroid 2004, 14, 605–609. [Google Scholar] [CrossRef]
- Duman, D.; Demirtunc, R.; Sahin, S.; Esertas, K. The effects of simvastatin and levothyroxine on intima-media thickness of the carotid artery in female normolipemic patients with subclinical hypothyroidism: A prospective, randomized-controlled study. J. Cardiovasc. Med. 2007, 8, 1007–1011. [Google Scholar] [CrossRef]
- Almeida, C.A.d.; Teixeira, P.d.F.d.S.; Soares, D.V.; Cabral, M.D.; Costa, S.M.d.; Salles, E.F.d.; Silva, N.A.d.O.e.; de Morais, F.F.; Buescu, A.; Henriques, J.M.; et al. Espessura íntima-média carotídea como marcador de risco cardiovascular em pacientes com hipotireoidismo subclínico. Arq. Bras. Endocrinol. Metabol. 2007, 51, 472–477. [Google Scholar] [CrossRef]
- Kim, S.-K.; Kim, S.-H.; Park, K.-S.; Park, S.-W.; Cho, Y.-W. Regression of the increased common carotid artery-intima media thickness in subclinical hypothyroidism after thyroid hormone replacement. Endocr. J. 2009, 56, 753–758. [Google Scholar] [CrossRef]
- Kebapcilar, L.; Comlekci, A.; Tuncel, P.; Solak, A.; Secil, M.; Gencel, O.; Sahin, M.; Sari, I.; Yeşil, S. Effect of levothyroxine replacement therapy on paraoxonase-1 and carotid intima-media thickness in subclinical hypothyroidism. Med. Sci. Monit. 2010, 16, 47. [Google Scholar]
- Valentina, V.N.; Marijan, B.; Chedo, D.; Branka, K. Subclinical hypothyroidism and risk to carotid atherosclerosis. Arq. Bras. Endocrinol. Metabol. 2011, 55, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Gunduz, M.; Gunduz, E.; Kircelli, F.; Okur, N.; Ozkaya, M. Role of surrogate markers of atherosclerosis in clinical and subclinical thyroidism. Int. J. Endocrinol. 2012, 2012, 109797. [Google Scholar] [CrossRef]
- Asik, M.; Sahin, S.; Ozkul, F.; Anaforoglu, I.; Ayhan, S.; Karagol, S.; Gunes, F.; Algun, E. Evaluation of epicardial fat tissue thickness in patients with Hashimoto thyroiditis. Clin. Endocrinol. 2013, 79, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M.; Lisowska, A.; Sobkowicz, B.; Tycińska, A.; Sawicki, R.; Musiał, W.J. Myocardial perfusion and intima-media thickness in patients with subclinical hypothyroidism. Adv. Med. Sci. 2013, 58, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Varim, C.; Yldiz, M. Assessment of carotid artery intima media thicknes in patients with subclinical hypothyroidism. Ortadogu Med. J. 2013, 5, 6–12. [Google Scholar]
- Kilic, I.D.; Tanriverdi, H.; Fenkci, S.; Akin, F.; Uslu, S.; Kaftan, A. Noninvasive indicators of atherosclerosis in subclinical hypothyroidism. Indian J. Endocrinol. Metab. 2013, 17, 271–275. [Google Scholar] [CrossRef]
- Unsal, I.O.; Topaloglu, O.; Cakir, E.; Bozkurt, N.C.; Karbek, B.; Gungunes, A.; Arslan, M.S.; Akkaymak, E.T.; Ucan, B.; Demirci, T.; et al. Effect of L-thyroxin therapy on thyroid volume and carotid artery lntima-media thickness in the patients with subclinical hypothyroidism. J. Med. Disord. 2014, 2, 1. [Google Scholar] [CrossRef]
- Akkoca, A.N.; Özdemir, Z.T.; Özler, G.S.; Karabulut, L. The evaluation of carotid intima thickness in clinical and subclinical hypothyroidism and effects of thyroid hormone treatment. Am. J. Clin. Exp. Med. 2014, 2, 59–63. [Google Scholar]
- Gunes, F.; Asik, M.; Temiz, A.; Vural, A.; Sen, H.; Binnetoglu, E.; Bozkurt, N.; Tekeli, Z.; Erbag, G.; Ukinc, K.; et al. Serum H-FABP levels in patients with hypothyroidism. Wien. Klin. Wochenschr. 2014, 126, 727–733. [Google Scholar] [CrossRef]
- Akbaba, G.; Berker, D.; Isık, S.; Tuna, M.M.; Koparal, S.; Vural, M.; Yılmaz, F.M.; Topcuoglu, C.; Guler, S. Changes in the before and after thyroxine treatment levels of adipose tissue, leptin, and resistin in subclinical hypothyroid patients. Wien. Klin. Wochenschr. 2016, 128, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Zha, K.; Zuo, C.; Wang, A.; Zhang, B.; Zhang, Y.; Wang, B.; Wang, Y.; Zhao, J.; Gao, L.; Xu, C. LDL in patients with subclinical hypothyroidism shows increased lipid peroxidation. Lipids Health Dis. 2015, 14, 95. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, M.; Tudoran, C. Particularities of endothelial dysfunction in hypothyroid patients. Kardiol. Pol. 2015, 73, 337–343. [Google Scholar] [CrossRef]
- Yazıcı, D.; Özben, B.; Toprak, A.; Yavuz, D.; Aydın, H.; Tarçın, Ö.; Deyneli, O.; Akalın, S. Effects of restoration of the euthyroid state on epicardial adipose tissue and carotid intima media thickness in subclinical hypothyroid patients. Endocrine 2015, 48, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Niknam, N.; Khalili, N.; Khosravi, E.; Nourbakhsh, M. Endothelial dysfunction in patients with subclinical hypothyroidism and the effects of treatment with levothyroxine. Adv. Biomed. Res. 2016, 5, 38. [Google Scholar] [CrossRef]
- França, M.M.; Nogueira, C.R.; Hueb, J.C.; Mendes, A.L.; Padovani, C.R.; Mazeto, G.M.F.d.S. Higher Carotid Intima-Media Thickness in Subclinical Hypothyroidism Associated with the Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2016, 14, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Cerbone, M.; Capalbo, D.; Wasniewska, M.; Alfano, S.; Raso, G.M.; Oliviero, U.; Cittadini, A.; De Luca, F.; Salerno, M. Effects of L-thyroxine treatment on early markers of atherosclerotic disease in children with subclinical hypothyroidism. Eur. J. Endocrinol. 2016, 175, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Isik-Balci, Y.; Agladioglu, S.; Agladioglu, K.; Kilic-Toprak, E.; Kilic-Erkek, O.; Ozhan, B.; Polat, A.; Bor-Kucukatay, M. Impaired Hemorheological Parameters and Increased Carotid Intima-Media Thickness in Children with Subclinical Hypothyroidism. Horm. Res. Paediatr. 2016, 85, 250–256. [Google Scholar] [CrossRef]
- Rahman, F.; Haque, F.S.; Biswas, S.K.; Begum, R.; Hossain, S.; Sharmin, S.; Rahman, M.; Hossain, S.; Nahar, K. Evaluation of Carotid Intima-Medica Thickness in Sub-clinical Hypothyroid Patients. Bangladesh J. Nucl. Med. 2016, 19, 123–127. [Google Scholar] [CrossRef]
- Altay, M.; Karakoç, M.A.; Çakır, N.; Demirtaş, C.Y.; Cerit, E.T.; Aktürk, M.; Ateş, İ.; Bukan, N.; Arslan, M. Serum Total Sialic Acid Level is Elevated in Hypothyroid Patients as an Atherosclerotic Risk Factor. J. Clin. Lab. Anal. 2017, 31, e22034. [Google Scholar] [CrossRef]
- Yadav, Y.; Saikia, U.K.; Sarma, D.; Hazarika, M. Cardiovascular Risk Factors in Children and Adolescents with Subclinical Hypothyroidism. Indian J. Endocrinol. Metab. 2017, 21, 823–829. [Google Scholar] [CrossRef]
- Tanaka, Y.; Furusyo, N.; Kato, Y.; Ueyama, T.; Yamasaki, S.; Ikezaki, H.; Murata, M.; Hayashi, J. Correlation between Thyroid Stimulating Hormone and Renal Function in Euthyroid Residents of Japan: Results from the Kyushu and Okinawa Population Study (KOPS). J. Atheroscler. Thromb. 2018, 25, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Saif, A.; Mousa, S.; Assem, M.; Tharwat, N.; Abdelhamid, A. Endothelial dysfunction and the risk of atherosclerosis in overt and subclinical hypothyroidism. Endocr. Connect. 2018, 7, 1075–1080. [Google Scholar] [CrossRef]
- Yasar, H.Y.; Demirpence, M.; Colak, A.; Yurdakul, L.; Zeytinli, M.; Turkon, H.; Ekinci, F.; Günaslan, A.; Yasar, E. Serum irisin and apelin levels and markers of atherosclerosis in patients with subclinical hypothyroidism. Arch. Endocrinol. Metab. 2019, 63, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, V.; Jayasingh, K.; Jayaraman, G.; Green, S.R.; Deyagarasan, E. Assessment of carotid intima-media thickness in hypothyroidism and the effect of thyroid replacement therapy. Int. J. Adv. Med. 2018, 5, 281–288. [Google Scholar] [CrossRef]
- Tan, M.; Korkmaz, H.; Aydin, H.; Doğuç, D.K. FABP4 levels in hypothyroidism and its relationship with subclinical atherosclerosis. Turk. J. Med. Sci. 2019, 49, 1490–1497. [Google Scholar] [CrossRef]
- Farghaly, H.S.; Metwalley, K.A.; Raafat, D.M.; Algowhary, M.; Said, G.M. Epicardial Fat Thickness in Children with Subclinical Hypothyroidism and Its Relationship to Subclinical Atherosclerosis: A Pilot Study. Horm. Res. Paediatr. 2019, 92, 99–105. [Google Scholar] [CrossRef]
- Doğan, A.; Karabulut, A.; Kilinç, F.; Pekkolay, Z.; Tuzcu, A.K. Evaluation of epicardial fat thickness and carotid intima-media thickness in the patients with subclinical and overt hypothyroidism. J. Contemp. Med. 2019, 9, 145–150. [Google Scholar] [CrossRef]
- Soto-García, A.J.; Elizondo-Riojas, G.; Rodriguez-Gutiérrez, R.; Mancillas-Adame, L.G.; González-González, J.G. Carotid Intima-Media Thickness in Patients with Subclinical Hypothyroidism: A Prospective Controlled Study. Clin. Investig. Med. 2021, 44, E39–E45. [Google Scholar] [CrossRef]
- Asoğlu, E.; Akbulut, T.; Doğan, Z.; Asoğlu, R. Evaluation of the aortic velocity propagation, epicardial fat thickness, and carotid intima-media thickness in patients with subclinical hypothyroidism. Rev. Cardiovasc. Med. 2021, 22, 959–966. [Google Scholar] [CrossRef] [PubMed]
- El Hini, S.H.; Mahmoud, Y.Z.; Saedii, A.A.; Mahmoud, S.S.; Amin, M.A.; Mahmoud, S.R.; Matta, R.A. Angiopoietin-like proteins 3, 4 and 8 are linked to cardiovascular function in naïve sub-clinical and overt hypothyroid patients receiving levothyroxine therapy. Endocr. Connect. 2021, 10, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Gönülalan, G.; Tanrikulu, Y. The New Anthropometric Measures in Patients with Hypothyroidism Hipotiro idi Hastalarında Yeni Antropometrik Ölçümler. J. Harran Univ. Med. Fac. 2021, 18, 149–154. [Google Scholar]
- Sahu, M.; Mishra, I.; Baliarsinha, A.K.; Choudhury, A.K.; Routray, S.N. Utility of Epicardial Fat Thickness in Subclinical Hypothyroid Children to Determine Existence of Subclinical Atherosclerosis in Them. Indian J Endocrinol. Metab. 2022, 26, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Singh, R.; Kaur, H.; Jasdeep, K.G. Study of carotid intima media thickness (Cimt) in patients of subclinical hypothyroidism (SCH). Eur. J. Mol. Clin. Med. 2022, 9, 572–577. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Gao, N.; Zhang, W.; Zhang, Y.-Z.; Yang, Q.; Chen, S.-H. Carotid intima-media thickness in patients with subclinical hypothyroidism: A meta-analysis. Atherosclerosis 2013, 227, 18–25. [Google Scholar] [CrossRef]
- Yao, K.; Zhao, T.; Zeng, L.; Yang, J.; Liu, Y.; He, Q.; Zou, X. Non-invasive markers of cardiovascular risk in patients with subclinical hypothyroidism: A systematic review and meta-analysis of 27 case control studies. Sci. Rep. 2018, 8, 4579. [Google Scholar] [CrossRef]
- Sahoo, R.; Krishna, V.; Subrahmaniyan, D.; Dutta, T.; Elangovan, S. Common carotid intima-media thickness in acute ischemic stroke: A case control study. Neurol. India 2009, 57, 627–630. [Google Scholar] [CrossRef]
- Polak, J.F.; Pencina, M.J.; Pencina, K.M.; O’Donnell, C.J.; Wolf, P.A.; D’Agostino, R.B., Sr. Carotid-Wall Intima–Media Thickness and Cardiovascular Events. N. Engl. J. Med. 2011, 365, 213–221. [Google Scholar] [CrossRef]
- Inoue, K.; Ritz, B.; Brent, G.A.; Ebrahimi, R.; Rhee, C.M.; Leung, A.M. Association of Subclinical Hypothyroidism and Cardiovascular Disease with Mortality. JAMA Netw. Open 2020, 3, e1920745. [Google Scholar] [CrossRef] [PubMed]
- Vayá, A.; Giménez, C.; Sarnago, A.; Alba, A.; Rubio, O.; Hernández-Mijares, A.; Cámara, R. Subclinical hypothyroidism and cardiovascular risk. Clin. Hemorheol. Microcirc. 2014, 58, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Godinjak, A.; Velija-Ašimi, Z.; Bureković, A.; Kulić, M.; Gicić, S.; Serdarević, F. Subclinical inflammation: The link between increased cardiovascular riskand subclinical hypothyroidism in postmenopausal women. In CMBEBIH 2017: Proceedings of the International Conference on Medical and Biological Engineering 2017, Sarajevo, Bosnia and Herzegovina, 16–18 March 2017; Badnjevic, A., Ed.; Springer: Singapore, 2017; pp. 235–240. [Google Scholar]
- Rizos, C.V.; Elisaf, M.S.; Liberopoulos, E.N. Effects of thyroid dysfunction on lipid profile. Open Cardiovasc. Med. J. 2011, 5, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Åsvold, B.O.; Vatten, L.J.; Nilsen, T.I.; Bjøro, T. The association between TSH within the reference range and serum lipid concentrations in a population-based study. The HUNT Study. Eur. J. Endocrinol. 2007, 156, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kc, R.; Khatiwada, S.; Deo Mehta, K.; Pandey, P.; Lamsal, M.; Majhi, S. Cardiovascular Risk Factors in Subclinical Hypothyroidism: A Case Control Study in Nepalese Population. J. Thyroid. Res. 2015, 2015, 305241. [Google Scholar] [CrossRef]
- Balagopal, P.; De Ferranti, S.D.; Cook, S.; Daniels, S.R.; Gidding, S.S.; Hayman, L.L.; McCrindle, B.W.; Mietus-Snyder, M.L.; Steinberger, J. Nontraditional Risk Factors and Biomarkers for Cardiovascular Disease: Mechanistic, Research, and Clinical Considerations for Youth. Circulation 2021, 123, 2749–2769. [Google Scholar] [CrossRef] [PubMed]
- Wells, B.J.; Hueston, W.J. Are thyroid peroxidase antibodies associated with cardiovascular disease risk in patients with subclinical hypothyroidism? Clin. Endocrinol. 2005, 62, 580–584. [Google Scholar] [CrossRef]
- Yoo, W.S.; Chung, H.K. Subclinical Hypothyroidism: Prevalence, Health Impact, and Treatment Landscape. Endocrinol. Metab. 2021, 36, 500–505. [Google Scholar] [CrossRef]
- Urgatz, B.; Razvi, S. Subclinical hypothyroidism, outcomes and management guidelines: A narrative review and update of recent literature. Curr. Med. Res. Opin. 2023, 39, 351–365. [Google Scholar] [CrossRef]
- Sato, Y.; Yoshihisa, A.; Kimishima, Y.; Kiko, T.; Watanabe, S.; Kanno, Y.; Abe, S.; Miyata, M.; Sato, T.; Suzuki, S.; et al. Subclinical Hypothyroidism Is Associated with Adverse Prognosis in Heart Failure Patients. Can. J. Cardiol. 2018, 34, 80–87. [Google Scholar] [CrossRef]
- Kannan, L.; Shaw, P.A.; Morley, M.P.; Brandimarto, J.; Fang, J.C.; Sweitzer, N.K.; Cappola, T.P.; Cappola, A.R. Thyroid Dysfunction in Heart Failure and Cardiovascular Outcomes. Circ. Heart Fail. 2018, 11, e005266. [Google Scholar] [CrossRef]
- Corona, G.; Croce, L.; Sparano, C.; Petrone, L.; Sforza, A.; Maggi, M.; Chiovato, L.; Rotondi, M. Thyroid and heart, a clinically relevant relationship. J. Endocrinol. Investig. 2021, 44, 2535–2544. [Google Scholar] [CrossRef]
- Zhao, T.; Chen, B.; Zhou, Y.; Wang, X.; Zhang, Y.; Wang, H.; Shan, Z. Effect of levothyroxine on the progression of carotid intima-media thickness in subclinical hypothyroidism patients: A meta-analysis. BMJ Open 2017, 7, e016053. [Google Scholar] [CrossRef]
- Aziz, M.; Kandimalla, Y.; Machavarapu, A.; Saxena, A.; Das, S.; Younus, A.; Nguyen, M.; Malik, R.; Anugula, D.; Latif, M.A.; et al. Effect of Thyroxin Treatment on Carotid Intima–Media Thickness (CIMT) Reduction in Patients with Subclinical Hypothyroidism (SCH): A Meta-Analysis of Clinical Trials. J. Atheroscler. Thromb. 2017, 24, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Tschiderer, L.; Allara, E.; Reuber, K.; Seekircher, L.; Gao, L.; Liao, X.; Lonn, E.; Gerstein, H.C.; Yusuf, S.; et al. Carotid Intima-Media Thickness Progression as Surrogate Marker for Cardiovascular Risk: Meta-Analysis of 119 Clinical Trials Involving 100 667 Patients. Circulation 2020, 142, 621–642. [Google Scholar] [CrossRef]
- Blum, M.R.; Gencer, B.; Adam, L.; Feller, M.; Collet, T.-H.; da Costa, B.R.; Moutzouri, E.; Dopheide, J.; Depairon, M.; Sykiotis, G.P.; et al. Impact of Thyroid Hormone Therapy on Atherosclerosis in the Elderly With Subclinical Hypothyroidism: A Randomized Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2988–2997. [Google Scholar] [CrossRef] [PubMed]
- Pearce, S.H.; Brabant, G.; Duntas, L.H.; Monzani, F.; Peeters, R.P.; Razvi, S.; Wemeau, J.-L. 2013 ETA Guideline: Management of Subclinical Hypothyroidism. Eur. Thyroid. J. 2013, 2, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Razvi, S.; Weaver, J.U.; Butler, T.J.; Pearce, S.H.S. Levothyroxine treatment of subclinical hypothyroidism, fatal and nonfatal cardiovascular events, and mortality. Arch. Intern. Med. 2012, 172, 811–817. [Google Scholar] [CrossRef]
- Surks, M.I.; Hollowell, J.G. Age-specific distribution of serum thyrotropin and antithyroid antibodies in the US population: Implications for the prevalence of subclinical hypothyroidism. J. Clin. Endocrinol. Metab. 2007, 92, 4575–4582. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | TSH Cut off Value (mUI/mL) | Participants (SCH/EU) | Age (SCH/EU) | NOS |
|---|---|---|---|---|---|---|
| Monzani [20] | 2004 | Italy | >3.6 | 45/32 | 37 ± 1/35 ± 1 | 8 |
| Cikim [21] | 2004 | Turkey | >4.20 | 25/23 | 32.2 ±9.6/35.8 ± 7.9 | 7 |
| Duman [22] | 2007 | Turkey | >4.2 | 40/20 | 37 ± 12.6/36.7 ± 12.2 | 7 |
| de Almeida [23] | 2007 | Brazil | >4 | 30/27 | 43 ± 9.7/43.1 ± 8.3 | 8 |
| Kim [24] | 2009 | Korea | >5.5 | 36/32 | 36 ± 6.2/36.1 ± 5.4 | 7 |
| Kebapcilar [25] | 2010 | Turkey | >5 | 38/19 | 49.7 ± 10/49.9 ± 8.1 | 8 |
| Velkoska [26] | 2011 | Macedonia | >4.2 | 67/30 | 42.4 ± 16.2/43.6 ± 12.8 | 7 |
| Gunduz [27] | 2012 | Turkey | >4 | 16/20 | 40.8 ± 11.8/32.8 ± 5.7 | 7 |
| Asik [28] | 2013 | Turkey | >5.49 | 33/32 | 38.1 ± 15/39.4 ± 9.7 | 8 |
| Knapp [29] | 2013 | Poland | – | 40/15 | 34.8 ± 4.1/31.6 ± 9.3 | 4 |
| Varim [30] | 2013 | Turkey | >4.5 | 50/50 | 29.5 ± 8.9/29.8 ± 7.6 | 7 |
| Kilic [31] | 2013 | Turkey | >4.2 | 32/29 | 41.5 ± 12/38.1 ± 11.4 | 5 |
| Unsal [32] | 2014 | Turkey | >4.2 | 56/46 | 41.3 ± 14.4/36 ± 10.5 | 7 |
| Akkoca [33] | 2014 | Turkey | >4.2 | 20/20 | 34.4 ± 1.4/35.2 ± 2.2 | 7 |
| Gunes [34] | 2014 | Turkey | >4.2 | 39/29 | 40.4 ± 15.3/41 ± 13.8 | 8 |
| Akbaba [35] | 2015 | Turkey | >4 | 51/43 | 36.9 ± 10/34.9 ± 8.4 | 8 |
| Zha [36] | 2015 | China | >4.5 | 10/10 | 53.2 ± 5.4/52 ± 5.7 | 7 |
| Tudoran [37] | 2015 | Romania | >4.2 | 15/15 | 36.7 ± 5.2/42.1 ± 6.8 | 4 |
| Yazici [38] | 2015 | Turkey | >4 | 43/30 | 35.2 ± 1/34.5 ± 8.2 | 8 |
| Niknam [39] | 2016 | Iran | >4 | 25/25 | 35.9 ± 7.6/37.5 ± 7.3 | 8 |
| Fraca [40] | 2016 | Brazil | >4.5 | 16/15 | 39.6 ± 10.1/45 ± 7.4 | 5 |
| Cerbone [41] | 2016 | Italy | >4.2 | 39/39 | 9.1 ± 3.5/9.4 ± 3.6 | 8 |
| Isik-Balci [42] | 2016 | Turkey | NA | 53/31 | 9.2 ± 4.2/7.1 ± 5.1 | 4 |
| Rahman [43] | 2016 | Bangladesh | >5 | 26/30 | 30 ± 7.4/32 ± 8.7 | 8 |
| Altay [44] | 2017 | Turkey | NA | 35/30 | 34.4 ± 10.3/32.5 ± 7.5 | 5 |
| Yadav [45] | 2017 | India | >7.5 | 27/20 | 10.9 ± 2.3/10.8 ± 2.4 | 8 |
| Tanaka [46] | 2018 | Japan | >4.5 | 55/674 | 60.1 ± 7/56.1 ± 9.4 | 5 |
| Saif [47] | 2018 | Egypt | >4.8 | 30/40 | 34 ± 8/36 ± 4.8 | 8 |
| Yasar [48] | 2018 | Turkey | >5.6 | 160/86 | 39.5 ± 14.8/40.4 ± 10.0 | 7 |
| Vijayan [49] | 2018 | India | >4.2 | 30/30 | 33.9 ± 10.6/37.9 ± 9.7 | 8 |
| Tan [50] | 2019 | Turkey | >4.94 | 40/40 | 32 ± 27/28 ± 19 | 8 |
| Farghaly [51] | 2019 | Egypt | >4 | 32/32 | 13.6 ± 2.4/13.2 ± 2.1 | 8 |
| Dogan [52] | 2019 | Turkey | >4.2 | 50/37 | 35.3 ± 9.5/35.6 ± 1.9 | 6 |
| Soto-Garcia [53] | 2020 | Mexic | >4 | 18/18 | 37 ± 12.9/36.8 ± 12.7 | 8 |
| Asoglu [54] | 2021 | Turkey | >4.2 | 80/43 | 44.0 ± 13.1/46.7 ± 8.3 | 7 |
| El Hini [55] | 2021 | Egypt | >4.5 | 36/36 | 40.2 ± 8.6/35.6 ± 9.9 | 6 |
| Gonulalaln [56] | 2021 | Turkey | >4 | 30/52 | 35 ± 13.6/38.7 ± 10.4 | 7 |
| Sahu [57] | 2022 | India | >5 | 42/50 | 10.3 ± 3.7/10.1 ± 3.1 | 7 |
| Sharma [58] | 2022 | India | >4.2 | 35/35 | 46.2 ± 10/41.1 ± 11.1 | 6 |
| Authors | Year | CIMT Assay | TSH Assay |
|---|---|---|---|
| Monzani [20] | 2004 | High-resolution ultrasonography using multiple equipment types and 7.5 MHz linear transducer—multiple measurements of both carotid arteries and internal carotid arteries | Ultrasensitive immunoradiometric assay (IRMA) method |
| Cikim [21] | 2004 | High-resolution ultrasound imaging (Vingmed System Five, 10 mH linear probe)—both common carotid arteries; three measurements from each subject | Autoanalyzer Roche/Hitachi Modular System—method not specified |
| Duman [22] | 2007 | High-resolution ultrasonography with a 7.5 MHz linear array transducer using a vascular ultrasound system (ATL-3500-HDI; Philips Medical Systems, Andover, MA, USA)—multiple measurements of both common carotid arteries | Roche/Hitachi modular analytics SWA—immunoassay |
| de Almeida [23] | 2007 | High-resolution ultrasound with Acusson Aspem Advanced and 10 MHz linear transducer—multiple measurements of both common carotid arteries and bifurcation | Imunometric measurement (IMMULITE DPC®) |
| Kim [24] | 2009 | High-resolution ultrasonographic system (Prosound α10) with 10.0 MHz linear transducer—multiple measurements in the mid and distal portion of the common carotid arteries | Chemiluminescent immunometric assay |
| Kebapcilar [25] | 2010 | High-definition ultrasonography (Philips HDI 5000) with L12-5 linear wide-band probe—two measurements, one proximal and one distal for each common carotid artery | Chemiluminescent immunometric assay (Immulite 2000) |
| Velkoska [26] | 2011 | Ultrasound system HP Agilent S4500 with 7.5–10.0 MHz linear transducer—two measurements of the right carotid artery | Immulite 2000 chemiluminescent analyzer |
| Gunduz [27] | 2012 | Gray-scale high-resolution color Doppler ultrasound (Prosound SSD—3500 SV ALOKA)—one measurement for each common carotid artery | Immulite 2000 chemiluminescent analyzer |
| Asik [28] | 2013 | Echocardiography machine VIVID 3 equipped with linear-array imaging probe—one measurement 10 mm proximal to the right carotid artery bifurcation | Chemiluminometric method (ADVIA Centaur analyzer |
| Knapp [29] | 2013 | Ultrasound imaging (Philips iE33) with 1–5 MHz sector transducer and 3–11 MHz linear-array high-resolution transducer—two measurements for each common carotid artery | Method not specified |
| Varim [30] | 2013 | Ultrasound with Siemens Sonoline Ultrasound using a 10 MHz linear probe—three measurements for each common carotid artery | Method not specified |
| Kilic [31] | 2013 | Ultrasound imaging (Vivid 7 dimensions) with 12 MHz linear array transducer—two measurements for each common carotid artery | Immunochemiluminescence method (Cobalt 6000 analyzer) |
| Unsal [32] | 2014 | High-resolution ultrasonography (Hitachi EUB 7000 HV) with 13 MHz probe—three measurements for each common carotid artery | Chemiluminescence assay (Advia Centaur) and specific electrochemiluminescence immunoassay (Elecsys 2010 Cobas) |
| Akkoca [33] | 2014 | Gray-scale, high-resolution color Doppler ultrasound (Siemens) with 13 MHz linear transducer—one measurement for each carotid artery | Chemiluminescence method (Immulite 2000) |
| Gunes [34] | 2014 | Ultrasound imaging (VIVID 3 machine) with 2.5 MHz linear-array probe—three measurements approximately 10 mm proximal of the carotid bifurcation for the right common carotid artery | Electro-chemiluminescence immunoassay “ECLIA” (Roche Cobas E601 analyzer) |
| Akbaba [35] | 2015 | High-resolution B-mode ultrasound (Loqic 3 device) with 11 MHz linear array transducer—three measurements for each common carotid artery | Chemiluminescence micro-particle immunoassay (Abbot Architect 2000) |
| Zha [36] | 2015 | Color ultrasound (Toshiba Aplio 500) with 9 Mhz linear-array transducer—three measurements for each common carotid artery | Chemiluminescence procedure (Roche Cobas E610) |
| Tudoran [37] | 2015 | Echocardiography device (Aloka CV Prosound SSD-4000 SV) with 10 MHz linear transducer—five measurements for each carotid artery beginning from carotid bulb dilation | Method not specified |
| Yazici [38] | 2015 | Ultrasound imaging (GE Vingmed) with 10 MHz broadband linear probe—number of measurements and sites not specified | Method not specified |
| Nikna [39] | 2015 | Sonogram B-mode imaging—number of measurements and sites not specified | Method not specified |
| França [40] | 2016 | Ultrasound imaging with 7.5 MHz multifrequency linear array probe (device not specified)—three measurements of the common carotid artery | Electrochemiluminescence immunoassay (Roche Diagnostics kits) |
| Cerbone [41] | 2016 | Ultrasound imaging (GE Vivid I) with 7.0 MHz—multiple measurements above the carotid sinus for both common carotid arteries | Chemiluminescence method (Immulite 2000) |
| Isik-Balci [42] | 2016 | Ultrasound imaging (Logiq E9 ultrasound) with a 6–15 MHz linear array probe—three measurements 20 mm proximal to the carotid bifurcation | Electrochemiluminescence (Roche Cobas 6000) |
| Rahman [43] | 2016 | Ultrasound imaging (DC-7 scanner) with 7.5–10 MHz linear transducer—one measurement 1.5 cm superior to the carotid bifurcation for each carotid artery | Immunoradiometric assay |
| Altay [44] | 2017 | Ultrasound imaging (General Electric Logic 5 Pro) with 12 MHz—five measurements for each common carotid artery, 1 cm distal to the main carotid artery bulb | Method not specified |
| Yadav [45] | 2017 | B-mode ultrasound imaging (Siemens) with 10 MHz linear transducer—number of measurements and sites not specified | Chemiluminescence immunoassay (IMMULITE 1000) |
| Tanaka [46] | 2018 | High-resolution B-mode ultrasonography (UF-4300R) with 7.5 MHz linear array probe—unspecified number of measurements for both common carotid arteries 20 mm proximal to the carotid bulb | CLIA immunoassay |
| Saif [47] | 2018 | High-resolution color-codded Doppler ultrasonography (ALT HDI) with 12 MHz linear array probe—four measurements for both common carotid arteries | Method not specified |
| Yasar [48] | 2018 | Ultrasound imaging (Toshiba Aplio 300) with 9–13 MHz linear probe—unspecified number of measurements 2 cm proximal to the carotid bulb | Chemiluminescent method (Immulite 2000) |
| Vijayan [49] | 2018 | Ultrasound imaging (Mindray DC-8) with 7 MHz linear transducer—unspecified number of measurements 10 mm proximal to the right common carotid artery | Chemiluminescent immunometric assay |
| Tan [50] | 2019 | B-mode ultrasonography with 7.5–13.5 MHz multifrequency linear array probe—three measurements for each common carotid artery | Electrochemiluminescence method (Abbot Aeroset kit) |
| Farghaly [51] | 2019 | Color duplex flow imaging (Acuson 128 XP)—three measurements at 1–2 cm proximal to the carotid bulb for each common carotid artery | Ultrasensitive immunometric assay (Immulite 2000 Third Generation) |
| Dogan [52] | 2019 | Ultrasonography (Aloka Prosound SSD 5000) with 7.5 MHz linear probe—unspecified number of measurements 10 mm proximal to the bifurcation for each common carotid artery | Electrochemiluminescence assay |
| Soto-Garcia [53] | 2020 | B-mode ultrasonography with 7.5–13.5 MHz multifrequency linear array probe—three measurements for each common carotid artery | Method not specified |
| Asoglu [54] | 2021 | Unspecified equipment and number of measurements 1–2 cm proximal to the carotid artery bifurcation | Chemiluminescence methods |
| El Hini [55] | 2021 | Method not specified | Enzyme-linked fluorescence immunoassay (BioMerieux Mini Vidas) |
| Gonulalaln [56] | 2021 | B-mode ultrasonography (LOGIQ P5)—three measurements 1 cm proximal to the bifurcation for each common carotid artery | Method not specified |
| Sahu [57] | 2022 | Color duplex flow imaging (Samsung HS 70 A) with 7 MHz probe—unspecified number of measurements for both common carotid arteries | Electrochemiluminescence assay (Roche Cobas 411) |
| Sharma [58] | 2022 | Unspecified equipment and number of measurements 1 cm proximal to the carotid artery bifurcation | Method not specified |
| Authors | SCH_BMI | EU_BMI | SCH_CIMT | EU_CIMT |
|---|---|---|---|---|
| Monzani [20] | 24.7 ± 3.5 | 24.2 ± 3.7 | 0.75 ± 0.13 | 0.63 ± 0.07 |
| Cikim [21] | 26.03 ± 6.21 | 27.04 ± 4.95 | 0.55 ± 0.14 | 0.54 ± 0.14 |
| Duman [22] | 25.1 ± 4.3 | 24.7 ± 2.5 | 0.66 ± 0.16 | 0.54 ± 0.10 |
| de Almeida [23] | 27.3 ± 4.6 | 25.41 ± 4.38 | 0.57 ± 0.70 | 0.57 ± 0.68 |
| Kim [24] | 23.1 ± 2.8 | 23.3 ± 3.1 | 0.66 ± 0.10 | 0.57 ± 0.08 |
| Kebapcilar [25] | 28.58 ± 5.81 | 28.45 ± 5.25 | 0.64 ± 0.13 | 0.57 ± 0.08 |
| Velkoska [26] | 27.8 ± 5.6 | 25.4 ± 5.1 | 0.61 ± 0.1 | 056 ± 0.1 |
| Gunduz [27] | 26.72 ± 2.32 | 24.34 ± 2.43 | 0.61 ± 0.11 | 0.53 ± 0.08 |
| Asik [28] | 30.37 ± 7.67 | 27.79 ± 3.64 | 0.54 ± 0.14 | 0.51 ± 0.11 |
| Knapp [29] | 24.43 ± 4.3 | 21.8 ± 1.48 | 0.61 ± 0.14 | 0.32 ± 0.1 |
| Varim [30] | 25.7 ± 4 | 25.66 ± 4.24 | 0.4 ± 0.2 | 0.4 ± 0.1 |
| Kilic [31] | 28.6 ± 5.9 | 24.9 ± 6.5 | 0.05 ± 0.01 | 0.06 ± 0.01 |
| Unsal [32] | - | - | 0.53 ± 0.11 | 0.5 ± 0.86 |
| Akkoca [33] | 28.42 ± 1.86 | 27.97 ± 4.15 | 0.74 ± 0.8 | 0.38 ± 0.74 |
| Gunes [34] | 28.79 ± 6.6 | 27.46 ± 5.35 | 0.65 ± 0.13 | 0.55 ± 0.11 |
| Akbaba [35] | 26.1 ± 5.5 | 25.7 ± 4.2 | 0.74 ± 0.3 | 0.47 ± 0.5 |
| Zha [36] | 24.4 ± 1.8 | 24 ± 1.6 | 0.82 ± 0.14 | 0.75 ± 0.09 |
| Tudoran [37] | 26.24 ± 2.7 | 27.5 ± 6.71 | 0.72 ± 0.14 | 0.62 ± 0.31 |
| Yazici [38] | 25.1 ± 5.6 | 25.0 ± 4.1 | 0.50 ± 0.09 | 0.48 ± 0.04 |
| Niknam [39] | 26 ± 2 | 25.82 ± 2 | 0.56 ± 0.09 | 0.58 ± 0.08 |
| França [40] | 26.5 ± 4.4 | 24.6 ± 2.98 | 0.62 ± 0.11 | 0.66 ± 0.14 |
| Cerbone [41] | - | - | 0.44 ± 0.08 | 0.44 ± 0.06 |
| Isik-Balci [42] | 17.56 ± 3.61 | 17.56 ± 2.47 | 0.5 ± 0.09 | 0.43 ± 0.03 |
| Rahman [43] | 25.6 ± 4.7 | - | 0.08 ± 0.05 | 0.6 ± 0.05 |
| Altay [44] | 27.6 ± 5.9 | 23.7 ± 3.9 | 0.63 ± 0.10 | 0.55 ± 0.05 |
| Yadav [45] | 17.79 ± 4.11 | 15.99 ± 1.69 | 0.48 ± 0.07 | 0.47 ± 0.08 |
| Tanaka [46] | 22.1 ± 2.7 | 22.1 ± 3.1 | 0.59 ± 0.12 | 0.57 ± 0.1 |
| Saif [47] | 26 ± 3.6 | 24 ± 2.3 | 0.6 ± 0.2 | 0.45 ± 0.07 |
| Yasar [48] | 30.22 ± 5.71 | 29.6 ± 6.12 | 0.55 ± 0.13 | 0.43 ± 0.19 |
| Vijayan [49] | 24.66 ± 4.13 | 22.86 ± 3.01 | 0.55 ± 0.10 | 0.47 ± 0.06 |
| Tan [50] | 23.67 ± 5.37 | 21.39 ± 3.52 | 0.5 ± 0.27 | 0.5 ± 0.16 |
| Farghaly [51] | - | - | 0.44 ± 0.08 | 0.44 ± 0.06 |
| Dogan [52] | 25.2 ± 3.8 | 31.4 ± 44.9 | 0.59 ± 0.12 | 0.43 ± 0.8 |
| Soto-Garcia [53] | 26.8 ± 4.7 | 29.6 ± 3.6 | 0.49 ± 0.12 | 0.42 ± 0.07 |
| Asoglu [54] | 26.5 ± 2.4 | 26.2 ± 2.4 | 0.8 ± 0.3 | 0.5 ± 0.2 |
| El Hini [55] | 26.7 ± 2 | 23.3 ± 0.84 | 0.56 ± 0.09 | 0.51 ± 0.06 |
| Gonulalaln [56] | 29.87 ± 5.09 | 29.12 ± 5.83 | 0.61 ± 0.11 | 0.35 ± 0.12 |
| Sahu [57] | 20.39 ± 2.51 | 18.81 ± 3.13 | 0.52 ± 0.12 | 0.49 ± 0.08 |
| Sharma [58] | 23.76 ± 1.77 | 23.12 ± 1.73 | 0.68 ± 0.14 | 0.59 ± 0.17 |
| Author | Year | TSH Cut off Value (mUI/mL) | SCH_CIMT | EU_CIMT |
|---|---|---|---|---|
| Monzani [20] | 2004 | >3.6 | 0.75 ± 0.13 | 0.63 ± 0.07 |
| Cikim [21] | 2004 | >4.20 | 0.55 ± 0.14 | 0.54 ± 0.14 |
| Duman [22] | 2007 | >4.2 | 0.66 ± 0.16 | 0.54 ± 0.10 |
| de Almeida [23] | 2007 | >4 | 0.57 ± 0.70 | 0.57 ± 0.68 |
| Kim [24] | 2009 | >5.5 | 0.66 ± 0.10 | 0.57 ± 0.08 |
| Kebapcilar [25] | 2010 | >5 | 0.64 ± 0.13 | 0.57 ± 0.08 |
| Velkoska [26] | 2011 | >4.2 | 0.61 ± 0.1 | 056 ± 0.1 |
| Gunduz [27] | 2012 | >4 | 0.61 ± 0.11 | 0.53 ± 0.08 |
| Asik [28] | 2013 | >5.49 | 0.54 ± 0.14 | 0.51 ± 0.11 |
| Knapp [29] | 2013 | – | 0.61 ± 0.14 | 0.32 ± 0.1 |
| Varim [30] | 2013 | >4.5 | 0.4 ± 0.2 | 0.4 ± 0.1 |
| Kilic [31] | 2013 | >4.2 | 0.05 ± 0.01 | 0.06 ± 0.01 |
| Unsal [32] | 2014 | >4.2 | 0.53 ± 0.11 | 0.5 ± 0.86 |
| Akkoca [33] | 2014 | >4.2 | 0.74 ± 0.8 | 0.38 ± 0.74 |
| Gunes [34] | 2014 | >4.2 | 0.65 ± 0.13 | 0.55 ± 0.11 |
| Akbaba [35] | 2015 | >4 | 0.74 ± 0.3 | 0.47 ± 0.5 |
| Zha [36] | 2015 | >4.5 | 0.82 ± 0.14 | 0.75 ± 0.09 |
| Tudoran [37] | 2015 | >4.2 | 0.72 ± 0.14 | 0.62 ± 0.31 |
| Yazici [38] | 2015 | >4 | 0.50 ± 0.09 | 0.48 ± 0.04 |
| Niknam [39] | 2016 | >4 | 0.56 ± 0.09 | 0.58 ± 0.08 |
| Franca [40] | 2016 | >4.5 | 0.62 ± 0.11 | 0.66 ± 0.14 |
| Cerbone [41] | 2016 | >4.2 | 0.44 ± 0.08 | 0.44 ± 0.06 |
| Isik-Balci [42] | 2016 | NA | 0.5 ± 0.09 | 0.43 ± 0.03 |
| Rahman [43] | 2016 | >5 | 0.08 ± 0.05 | 0.6 ± 0.05 |
| Altay [44] | 2017 | NA | 0.63 ± 0.10 | 0.55 ± 0.05 |
| Yadav [45] | 2017 | >7.5 | 0.48 ± 0.07 | 0.47 ± 0.08 |
| Tanaka [46] | 2018 | >4.5 | 0.59 ± 0.12 | 0.57 ± 0.1 |
| Saif [47] | 2018 | >4.8 | 0.6 ± 0.2 | 0.45 ± 0.07 |
| Yasar [48] | 2018 | >5.6 | 0.55 ± 0.13 | 0.43 ± 0.19 |
| Vijayan [49] | 2018 | >4.2 | 0.55 ± 0.10 | 0.47 ± 0.06 |
| Tan [50] | 2019 | >4.94 | 0.5 ± 0.27 | 0.5 ± 0.16 |
| Farghaly [51] | 2019 | >4 | 0.44 ± 0.08 | 0.44 ± 0.06 |
| Dogan [52] | 2019 | >4.2 | 0.59 ± 0.12 | 0.43 ± 0.8 |
| Soto-Garcia [53] | 2020 | >4 | 0.49 ± 0.12 | 0.42 ± 0.07 |
| Asoglu [54] | 2021 | >4.2 | 0.8 ± 0.3 | 0.5 ± 0.2 |
| El Hini [55] | 2021 | >4.5 | 0.56 ± 0.09 | 0.51 ± 0.06 |
| Gonulalaln [56] | 2021 | >4 | 0.61 ± 0.11 | 0.35 ± 0.12 |
| Sahu [57] | 2022 | >5 | 0.52 ± 0.12 | 0.49 ± 0.08 |
| Sharma [58] | 2022 | >4.2 | 0.68 ± 0.14 | 0.59 ± 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isailă, O.-M.; Stoian, V.E.; Fulga, I.; Piraianu, A.-I.; Hostiuc, S. The Relationship between Subclinical Hypothyroidism and Carotid Intima-Media Thickness as a Potential Marker of Cardiovascular Risk: A Systematic Review and a Meta-Analysis. J. Cardiovasc. Dev. Dis. 2024, 11, 98. https://doi.org/10.3390/jcdd11040098
Isailă O-M, Stoian VE, Fulga I, Piraianu A-I, Hostiuc S. The Relationship between Subclinical Hypothyroidism and Carotid Intima-Media Thickness as a Potential Marker of Cardiovascular Risk: A Systematic Review and a Meta-Analysis. Journal of Cardiovascular Development and Disease. 2024; 11(4):98. https://doi.org/10.3390/jcdd11040098
Chicago/Turabian StyleIsailă, Oana-Maria, Victor Eduard Stoian, Iuliu Fulga, Alin-Ionut Piraianu, and Sorin Hostiuc. 2024. "The Relationship between Subclinical Hypothyroidism and Carotid Intima-Media Thickness as a Potential Marker of Cardiovascular Risk: A Systematic Review and a Meta-Analysis" Journal of Cardiovascular Development and Disease 11, no. 4: 98. https://doi.org/10.3390/jcdd11040098
APA StyleIsailă, O. -M., Stoian, V. E., Fulga, I., Piraianu, A. -I., & Hostiuc, S. (2024). The Relationship between Subclinical Hypothyroidism and Carotid Intima-Media Thickness as a Potential Marker of Cardiovascular Risk: A Systematic Review and a Meta-Analysis. Journal of Cardiovascular Development and Disease, 11(4), 98. https://doi.org/10.3390/jcdd11040098