A Systematic Histopathologic Evaluation of Type-A Aortic Dissections Implies a Uniform Multiple-Hit Causation


 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patients and Tissue Samples
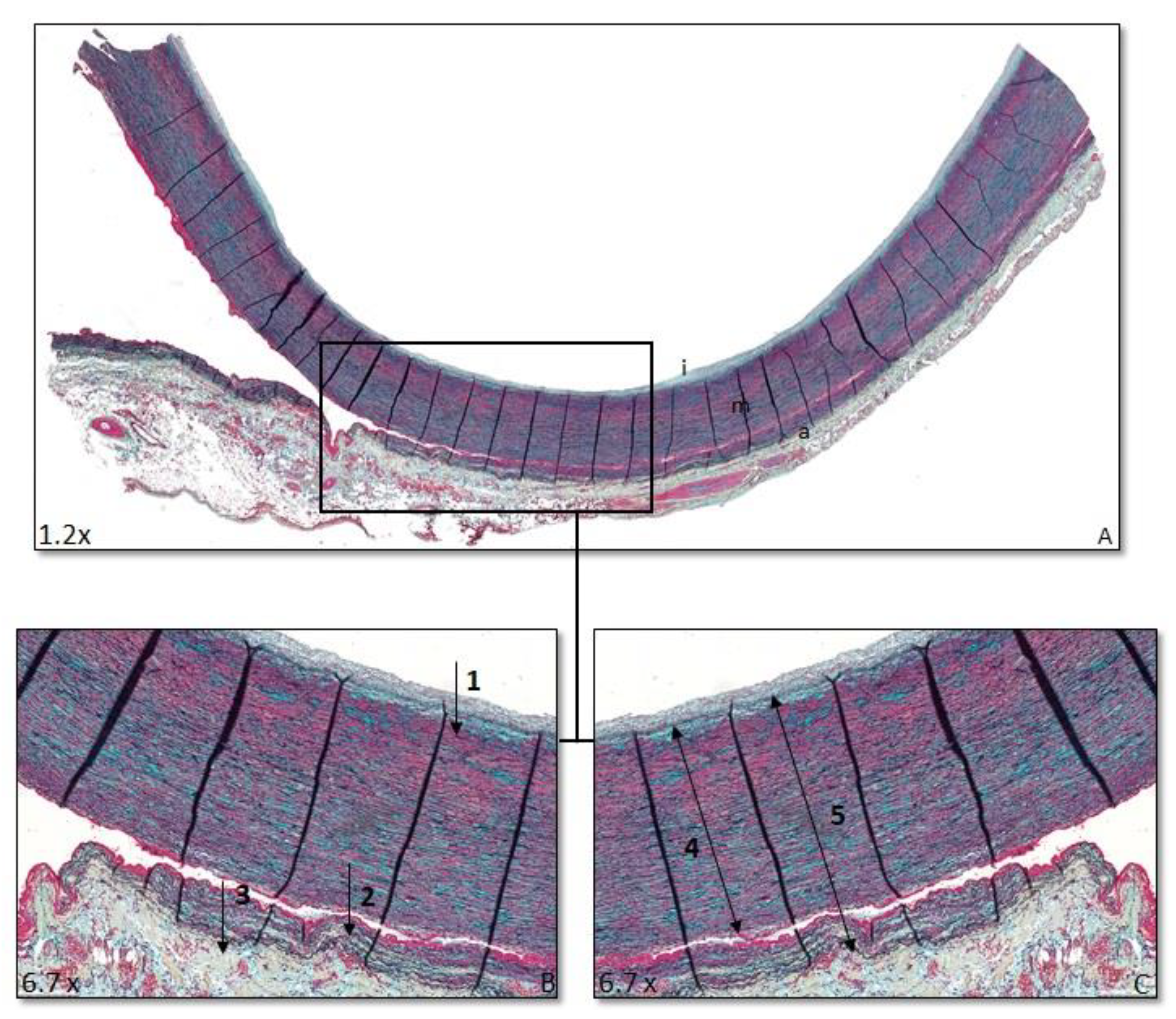
2.3. Morphology
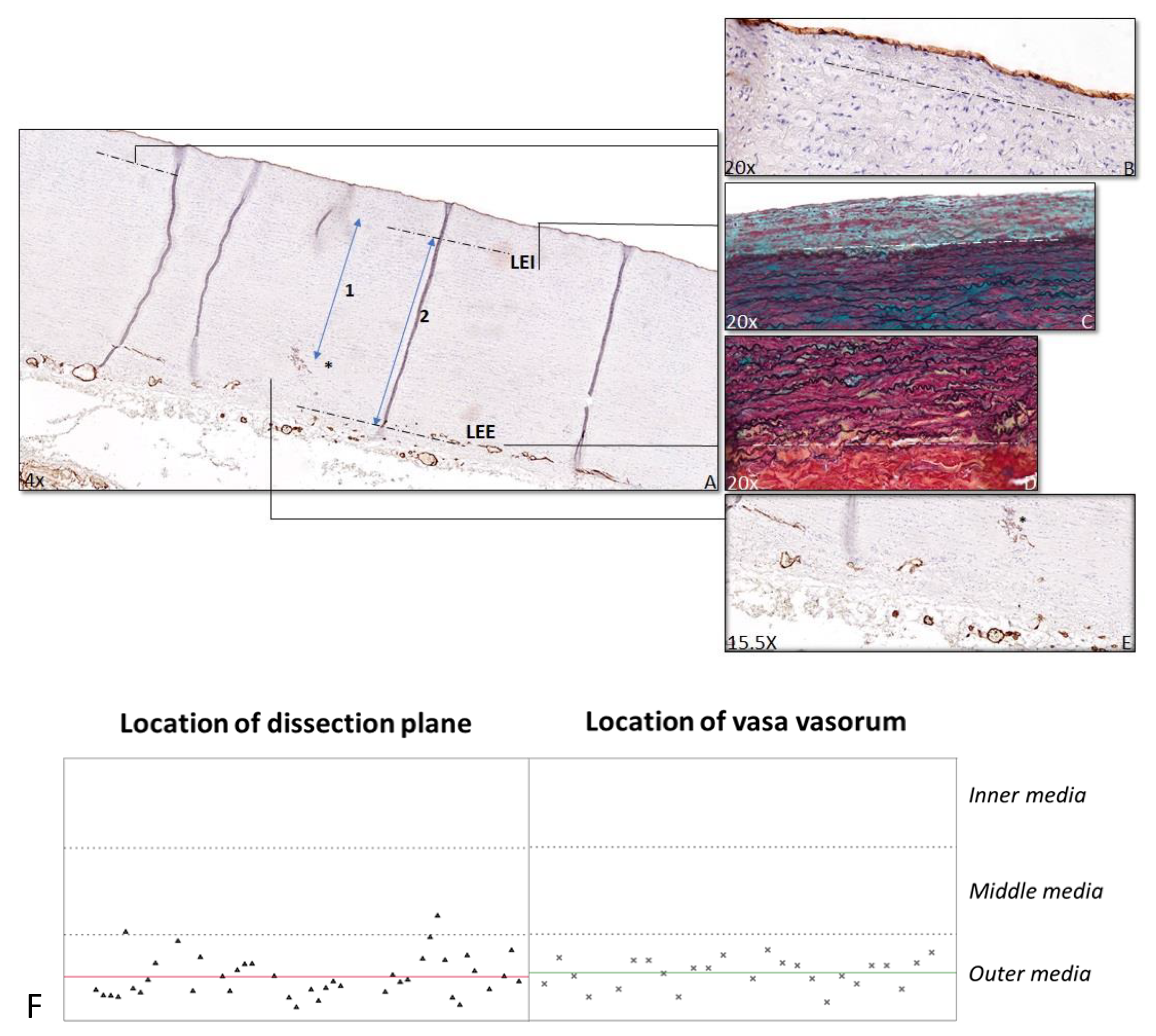
2.4. Anatomical Location of Dissection Plane
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
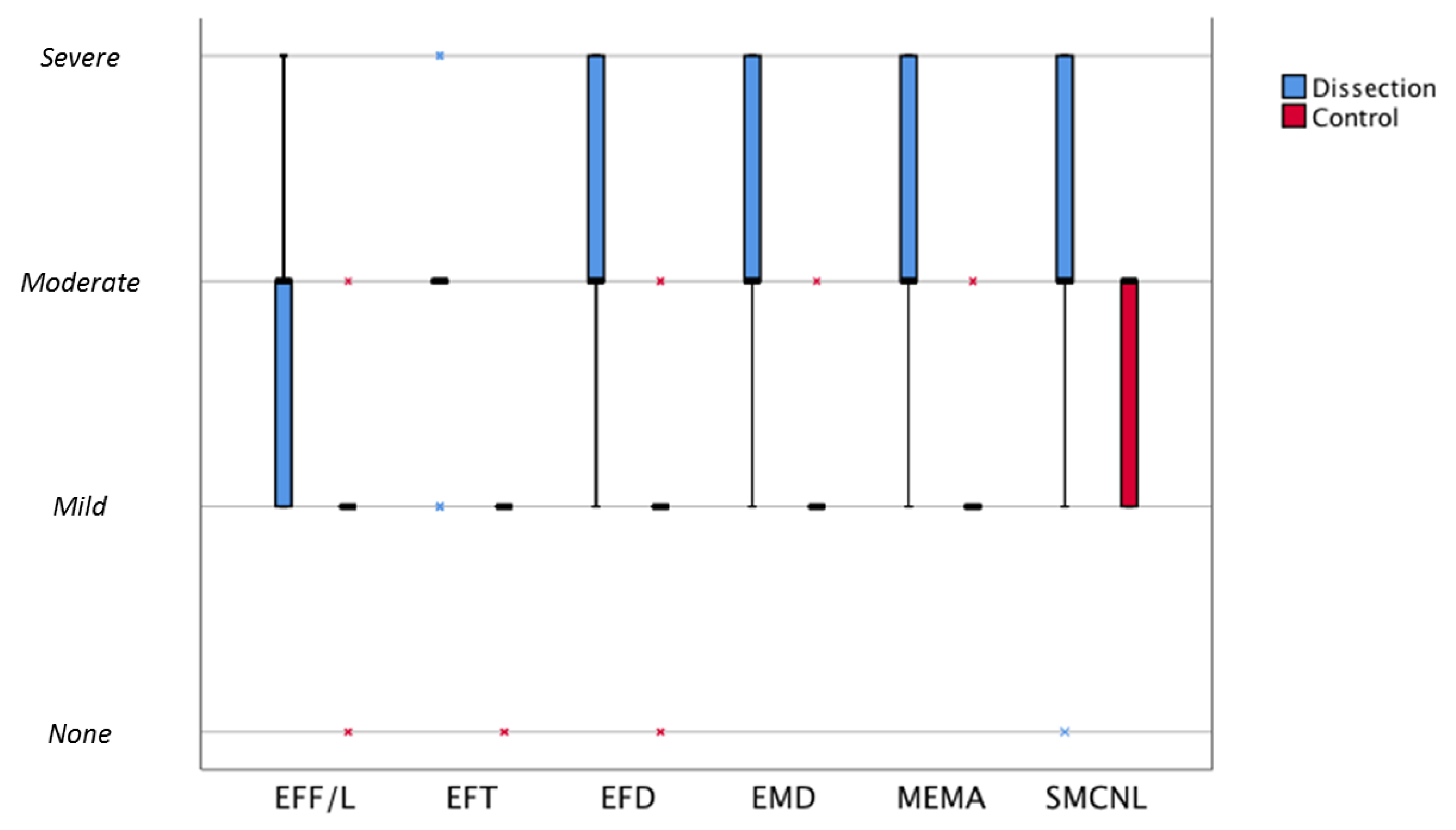
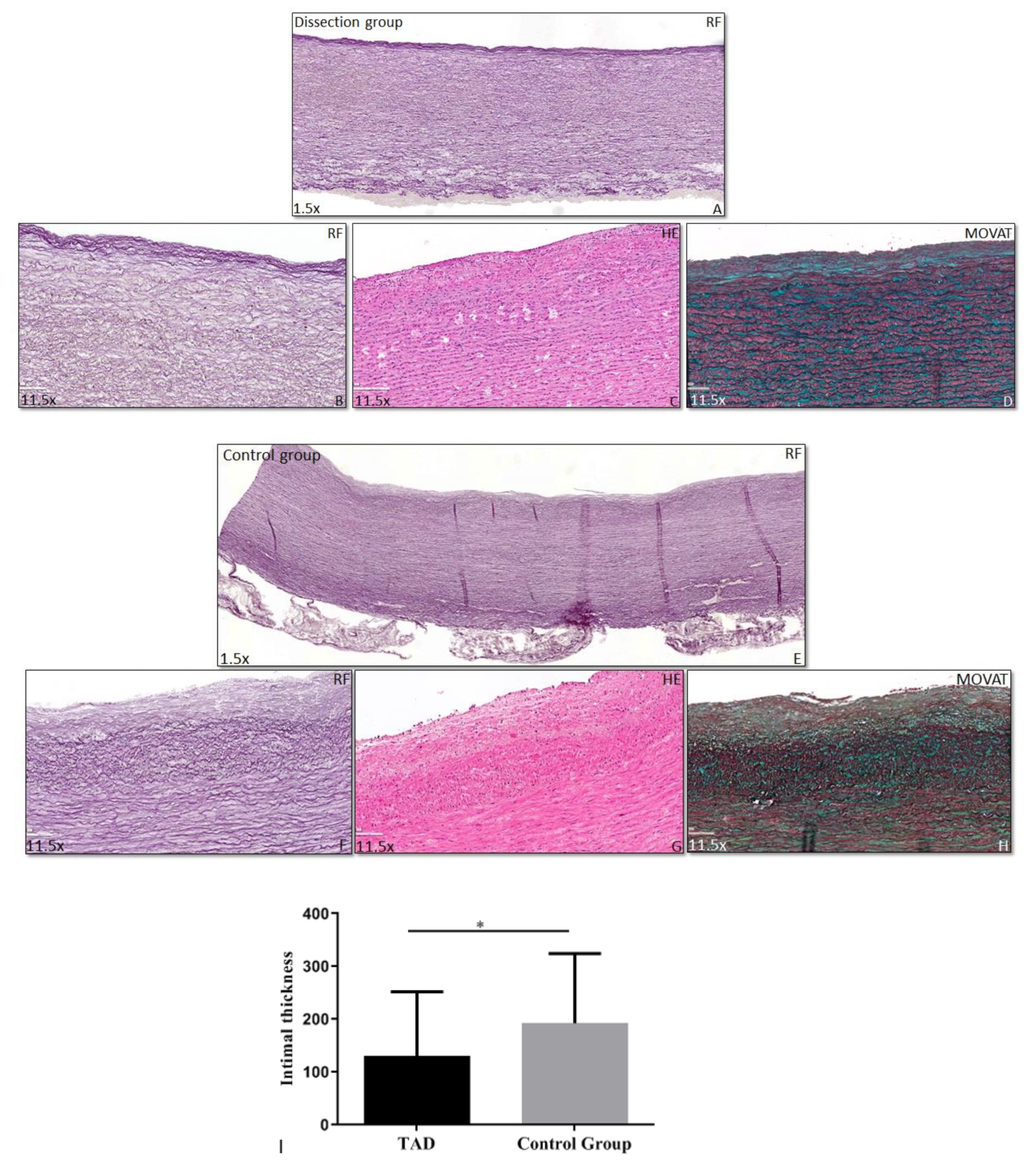
3.2. Histopathology of the Vascular Wall
3.3. Dissection Plane
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar]
- Wu, J.; Zafar, M.; Qiu, J.; Huang, Y.; Chen, Y.; Yu, C.; Elefteriades, J.A. A systematic review and meta-analysis of isolated abdominal aortic dissection. J. Vasc. Surg. 2019, 70, 2046–2053.e6. [Google Scholar] [CrossRef]
- Nienaber, C.A.; Clough, R.E. Management of acute aortic dissection. Lancet 2015, 385, 800–811. [Google Scholar] [CrossRef]
- Smedberg, C.; Steuer, J.; Leander, K.; Hultgren, R. Sex differences and temporal trends in aortic dissection: A population-based study of incidence, treatment strategies, and outcome in Swedish patients during 15 years. Eur. Heart J. 2020, 41, 2430–2438. [Google Scholar] [CrossRef] [PubMed]
- Daily, P.O.; Trueblood, H.W.; Stinson, E.B.; Wuerflein, R.D.; Shumway, N.E. Management of Acute Aortic Dissections. Ann. Thorac. Surg. 1970, 10, 237–247. [Google Scholar] [CrossRef]
- Kita, Y.; Nakamura, K.; Itoh, A.H. Histologic and Histometric Study of the Aortic Media in Dissecting Aneurysm Comparison with True Aneurysm and Age-matched Controls. Pathol. Int. 1990, 40, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Osada, H.; Kyogoku, M.; Matsuo, T.; Kanemitsu, N. Histopathological evaluation of aortic dissection: A comparison of congenital versus acquired aortic wall weakness. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 277–283. [Google Scholar] [CrossRef]
- Dingemans, K.P.; Teeling, P.; van der Wal, A.C.; Becker, A.E. Ultrastructural pathology of aortic dissections in patients with Marfan syndrome: Comparison with dissections in patients without Marfan syndrome. Cardiovasc. Pathol. 2006, 15, 203–212. [Google Scholar] [CrossRef]
- Halushka, M.K.; Angelini, A.; Bartoloni, G.; Basso, C.; Batoroeva, L.; Bruneval, P.; Buja, L.M.; Butany, J.; D’Amati, G.; Fallon, J.T.; et al. Consensus statement on surgical pathology of the aorta from the Society for Cardiovascular Pathology and the Association For European Cardiovascular Pathology: II. Noninflammatory degenerative diseases—nomenclature and diagnostic criteria. Cardiovasc. Pathol. 2016, 25, 247–257. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Hiratzka, L.F.; Creager, M.A.; Isselbacher, E.M.; Svensson, L.G.; Nishimura, R.A.; Bonow, R.O. Surgery for Aortic Dilatation in Patients With Bicuspid Aortic Valves: A Statement of Clarification From the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2016, 133, 680–686. [Google Scholar] [PubMed] [Green Version]
- Wang, L.; Zhang, J.; Fu, W.; Guo, D.; Jiang, J.; Wang, Y. Association of smooth muscle cell phenotypes with extracellular matrix disorders in thoracic aortic dissection. J. Vasc. Surg. 2012, 56, 1698–1709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, W.C.; Grande, C.M.; Hoyt, D.B. Trauma: Emergency Resuscitation, Perioperative Anesthesia, Surgical Management; CRC Press: Boca Raton, FL, USA, 2007; Volume II. [Google Scholar]
- Taylor, P.C.; Groves, L.K.; Loop, F.D.; Effler, D. Cannulation of the ascending aorta for cardiopulmonary bypass. Experience with 9,000 cases. J. Thorac. Cardiovasc. Surg. 1976, 71, 255–258. [Google Scholar] [CrossRef]
- Met, R.; Van Lienden, K.P.; Koelemay, M.J.W.; Bipat, S.; Legemate, D.A.; Reekers, J.A. Subintimal Angioplasty for Peripheral Arterial Occlusive Disease: A Systematic Review. Cardiovasc. Interv. Radiol. 2008, 31, 687–697. [Google Scholar] [CrossRef] [Green Version]
- Bergamini, T.M.; Seabrook, G.R.; Bandyk, D.F.; Towne, J.B. Symptomatic recurrent carotid stenosis and aneurysmal degeneration after endarterectomy. Surgenry 1993, 113, 580–586. [Google Scholar]
- Lindeman, J.H.; Ashcroft, B.A.; Beenakker, J.W.; van Es, M.; Koekkoek, N.B.; Prins, F.A.; Tielemans, J.F.; Abdul-Hussien, H.; Bank, R.A. Distinct defects in collagen microarchi-tecture underlie vessel-wall failure in advanced abdominal aneurysms and aneurysms in Marfan syndrome. Proc. Natl. Acad. Sci. USA 2010, 107, 862–865. [Google Scholar] [CrossRef] [Green Version]
- Niestrawska, J.A.; Haspinger, D.C.; Holzapfel, G.A. The influence of fiber dispersion on the mechanical response of aortic tissues in health and disease: A computational study. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 99–112. [Google Scholar] [CrossRef] [Green Version]
- Maleki, S.; Kjellqvist, S.; Paloschi, V.; Magné, J.; Branca, R.M.M.; Du, L.; Hultenby, K.; Petrini, J.; Fuxe, J.; Consortium, M.L.; et al. Mesenchymal state of intimal cells may explain higher propensity to ascending aortic aneurysm in bicuspid aortic valves. Sci. Rep. 2016, 6, 35712. [Google Scholar] [CrossRef] [Green Version]
- Grewal, N.; Franken, R.; Mulder, B.J.; Goumans, M.J.; Lindeman, J.H.; Jongbloed, M.R.; De Ruiter, M.C.; Klautz, R.J.M.; Bogers, A.J.C.C.; Poelmann, R.E.; et al. Histopathology of aortic complications in bicuspid aortic valve versus Marfan syndrome: Relevance for therapy? Heart Vessels 2015, 31, 795–806. [Google Scholar] [CrossRef] [Green Version]
- Grewal, N.; Groot, A.C.G.-D.; Poelmann, R.; Klautz, R.J.M.; Lindeman, J.H.; Goumans, M.-J.; Palmen, M.; Mohamed, S.A.; Sievers, H.-H.; Bogers, A.J.; et al. Ascending aorta dilation in association with bicuspid aortic valve: A maturation defect of the aortic wall. J. Thorac. Cardiovasc. Surg. 2014, 148, 1583–1590. [Google Scholar] [CrossRef] [Green Version]
- Grewal, N.; Groot, A.C.G.-D.; Von Der Thüsen, J.H.; Wisse, L.J.; Bartelings, M.M.; DeRuiter, M.C.; Klautz, R.J.M.; Poelmann, R. The Development of the Ascending Aortic Wall in Tricuspid and Bicuspid Aortic Valve: A Process from Maturation to Degeneration. J. Clin. Med. 2020, 9, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osada, H.; Kyogoku, M.; Ishidou, M.; Morishima, M.; Nakajima, H. Aortic dissection in the outer third of the media: What is the role of the vasa vasorum in the triggering process? European journal of cardio-thoracic surgery: Official journal of the European. Assoc. Cardio-Thoracic Surg. 2013, 43, e82–e88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angouras, D.; Sokolis, D.P.; Dosios, T.; Kostomitsopoulos, N.; Boudoulas, H.; Skalkeas, G.; Karayannacos, P.E. Effect of impaired vasa vasorum flow on the structure and mechanics of the thoracic aorta: Implications for the pathogenesis of aortic dissection. Eur. J. Cardio-Thoracic Surg. 2000, 17, 468–473. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Morphological Feature | Kappa |
|---|---|
| Elastic fiber fragmentation/Loss | 0.915 |
| Elastic fiber thinning | 0.880 |
| Elastic fiber degeneration | 0.801 |
| Mucoid extra cellular matrix accumulation | 0.938 |
| Smooth muscle cell nuclei loss | 0.978 |
| Overall medial degeneration | 0.879 |
| Variable | Type A Aortic Dissection Group n = 58 | Control Group n = 17 |
|---|---|---|
| Age, years | 63 ± 10.36 | 63 ± 5.46 |
| Gender | ||
|
|
|
| Arterial hypertension | ||
|
|
|
| Peripheral arterial disease | ||
|
|
|
| Valve Morphology | ||
|
|
|
| Connective tissue disorder | ||
|
|
|
| Diabetes Mellitus | ||
|
|
|
| Morphological Feature | Score | Type A Aortic Dissection Group N (%) | Control Group N (%) | p-Value |
|---|---|---|---|---|
| Elastic fiber fragmentation/loss |
|
|
| 0.000 |
| Elastic fiber thinning |
|
|
| 0.000 |
| Elastic fiber disorganization |
|
|
| 0.000 |
| Overall medial degeneration |
|
|
| 0.000 |
| Mucoid extracellular matrix accumulation |
|
|
| 0.000 |
| Smooth muscle cell nuclei loss |
|
|
| 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grewal, N.; Velders, B.J.J.; Gittenberger-de Groot, A.C.; Poelmann, R.; Klautz, R.J.M.; Van Brakel, T.J.; Lindeman, J.H.N. A Systematic Histopathologic Evaluation of Type-A Aortic Dissections Implies a Uniform Multiple-Hit Causation. J. Cardiovasc. Dev. Dis. 2021, 8, 12. https://doi.org/10.3390/jcdd8020012
Grewal N, Velders BJJ, Gittenberger-de Groot AC, Poelmann R, Klautz RJM, Van Brakel TJ, Lindeman JHN. A Systematic Histopathologic Evaluation of Type-A Aortic Dissections Implies a Uniform Multiple-Hit Causation. Journal of Cardiovascular Development and Disease. 2021; 8(2):12. https://doi.org/10.3390/jcdd8020012
Chicago/Turabian StyleGrewal, Nimrat, Bart J. J. Velders, Adriana C. Gittenberger-de Groot, Robert Poelmann, Robert J. M. Klautz, Thomas J. Van Brakel, and Jan H. N. Lindeman. 2021. "A Systematic Histopathologic Evaluation of Type-A Aortic Dissections Implies a Uniform Multiple-Hit Causation" Journal of Cardiovascular Development and Disease 8, no. 2: 12. https://doi.org/10.3390/jcdd8020012
APA StyleGrewal, N., Velders, B. J. J., Gittenberger-de Groot, A. C., Poelmann, R., Klautz, R. J. M., Van Brakel, T. J., & Lindeman, J. H. N. (2021). A Systematic Histopathologic Evaluation of Type-A Aortic Dissections Implies a Uniform Multiple-Hit Causation. Journal of Cardiovascular Development and Disease, 8(2), 12. https://doi.org/10.3390/jcdd8020012