
Surgical Aortic Valve Replacement with Concomitant Aortic Surgery in Patients with Purely Bicuspid Aortic Valve and Associated Aortopathy


Abstract
:1. Introduction
2. Methods
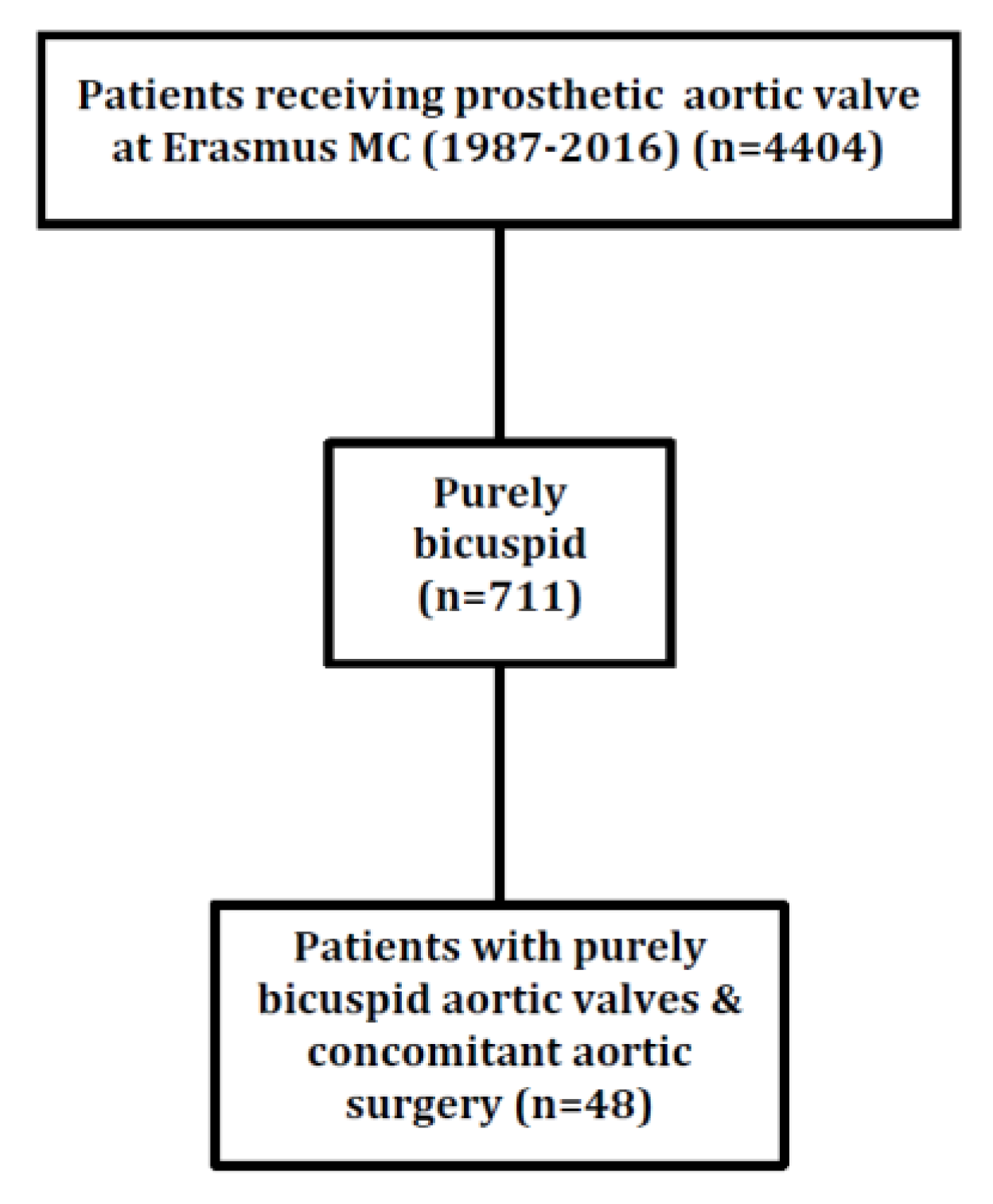
2.1. Study Design
2.2. Endpoints and Definitions
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients with Bicuspid Aortic Valves
3.2. Procedural Characteristics
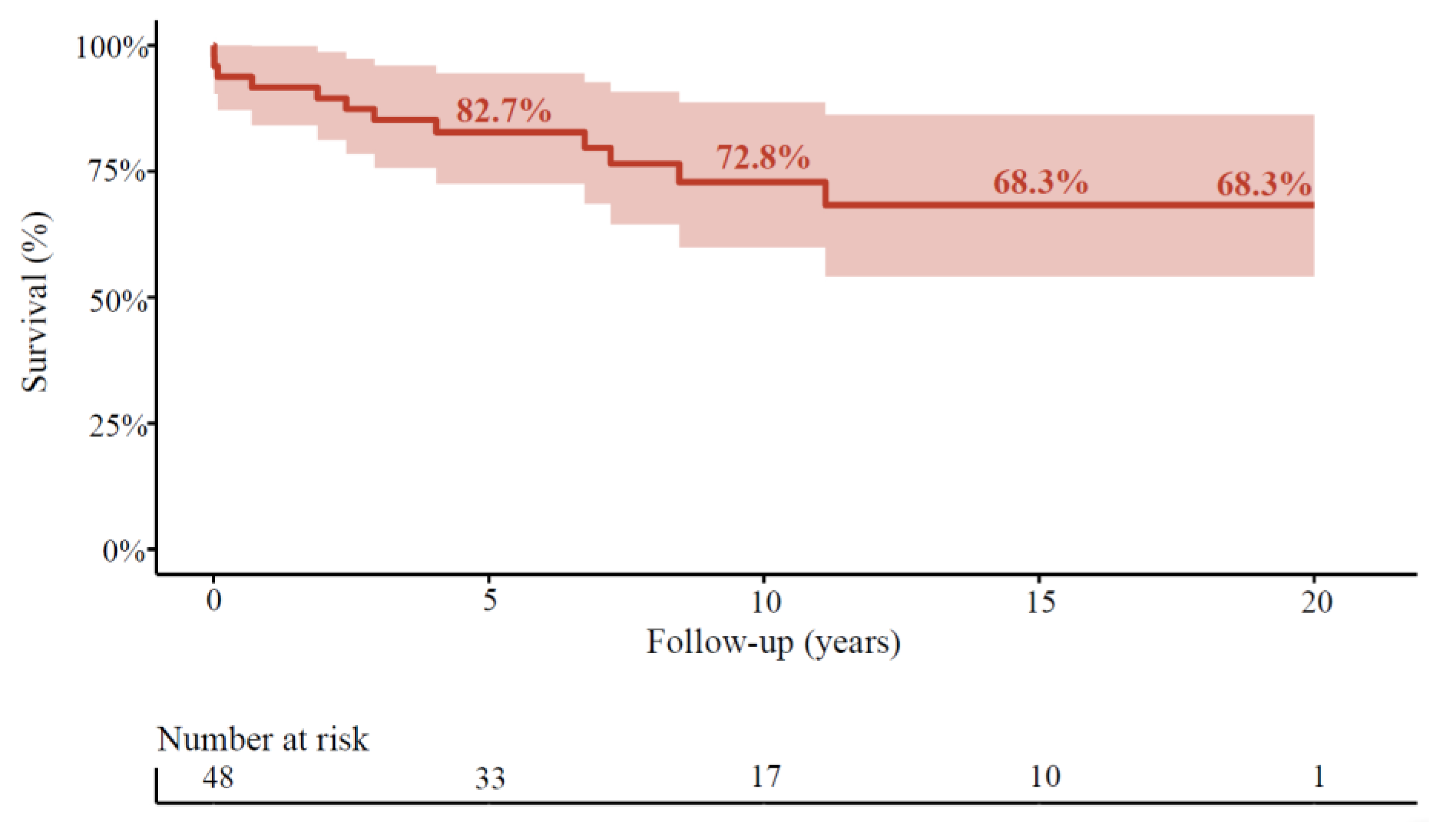
3.3. Long-Term Outcomes after Surgery
3.4. Factors Associated with Survival during Follow-Up in the Age-Matched Population
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nistri, S.; Basso, C.; Marzari, C.; Mormino, P.; Thiene, G. Frequency of bicuspid aortic valve in young male conscripts by echocardiogram. Am. J. Cardiol. 2005, 96, 718–721. [Google Scholar] [CrossRef]
- Braverman, A.C.; Guven, H.; Beardslee, M.A.; Makan, M.; Kates, A.M.; Moon, M.R. The bicuspid aortic valve. Curr. Probl. Cardiol. 2005, 30, 470–522. [Google Scholar] [CrossRef]
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Fedak, P.W.; Verma, S.; David, T.E.; Leask, R.L.; Weisel, R.D.; Butany, J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation 2002, 106, 900–904. [Google Scholar] [CrossRef]
- Mordi, I.; Tzemos, N. Bicuspid aortic valve disease: A comprehensive review. Cardiol. Res. Pract. 2012, 2012, 196037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perme, M.P.; Pavlic, K. Nonparametric Relative Survival Analysis with the R Package relsurv. J. Stat. Softw. 2018, 87, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Database, H.M. The Human Mortality Database. 2019. Available online: https://www.mortality.org/ (accessed on 29 January 2021).
- Pohar, M.; Stare, J. Relative survival analysis in R. Comput. Methods Programs Biomed. 2006, 81, 272–278. [Google Scholar] [CrossRef]
- Pohar, M.; Stare, J. Making relative survival analysis relatively easy. Comput. Biol. Med. 2007, 37, 1741–1749. [Google Scholar] [CrossRef]
- Gittenberger-de Groot, A.C.; Bartelings, M.M.; Deruiter, M.C.; Poelmann, R.E. Basics of cardiac development for the understanding of congenital heart malformations. Pediatr. Res. 2005, 57, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartelings, M.M.; Bogers, A.J.; Galantowicz, M.E.; Gittenberger-De Groot, A.C. Anatomy of the aortic and pulmonary roots. Semin. Thorac. Cardiovasc. Surg. 1998, 1, 157–164. [Google Scholar] [CrossRef]
- Peterson, J.C.; Wisse, L.J.; Wirokromo, V.; Van Herwaarden, T.; Smits, A.M.; Groot, A.C.G.-D.; Goumans, M.-J.T.H.; VanMunsteren, J.C.; Jongbloed, M.R.M.; DeRuiter, M.C. Disturbed nitric oxide signalling gives rise to congenital bicuspid aortic valve and aortopathy. Dis. Model. Mech. 2020, 13, dmm044990. [Google Scholar] [CrossRef]
- Bergwerff, M.; Verberne, M.E.; DeRuiter, M.C.; Poelmann, R.E.; Gittenberger-de Groot, A.C. Neural crest cell contribution to the developing circulatory system: Implications for vascular morphology? Circ. Res. 1998, 82, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappetein, A.P.; Gittenberger-de Groot, A.C.; Zwinderman, A.H.; Rohmer, J.; Poelmann, R.E.; Huysmans, H.A. The neural crest as a possible pathogenetic factor in coarctation of the aorta and bicuspid aortic valve. J. Thorac. Cardiovasc. Surg. 1991, 102, 830–836. [Google Scholar] [CrossRef]
- Kimura, N.; Nakamura, M.; Komiya, K.; Nishi, S.; Yamaguchi, A.; Tanaka, O.; Misawa, Y.; Adachi, H.; Kawahito, K. Patient-specific assessment of hemodynamics by computational fluid dynamics in patients with bicuspid aortopathy. J. Thorac. Cardiovasc. Surg. 2017, 153, S52–S62. [Google Scholar] [CrossRef] [Green Version]
- Youssefi, P.; Gomez, A.; He, T.; Anderson, L.; Bunce, N.; Sharma, R.; Figueroa, C.A.; Jahangiri, M. Patient-specific computational fluid dynamics-assessment of aortic hemodynamics in a spectrum of aortic valve pathologies. J. Thorac. Cardiovasc. Surg. 2017, 153, 8–20. [Google Scholar] [CrossRef] [Green Version]
- Hayman, S.; Wright, G.; West, C.; Burstow, D.; Scalia, G.M. True Bicuspid Aortic Valves are Rare Compared with Functionally Bicuspid Aortic Valves. Heart Lung Circ. 2008, 17, S63. [Google Scholar] [CrossRef]
- Robicsek, F.; Thubrikar, M.J.; Cook, J.W.; Fowler, B. The congenitally bicuspid aortic valve: How does it function? Why does it fail? Ann. Thorac. Surg. 2004, 77, 177–185. [Google Scholar] [CrossRef]
- Hope, M.D.; Hope, T.A.; Meadows, A.K.; Ordovas, K.G.; Urbania, T.H.; Alley, M.T.; Higgins, C.B. Bicuspid aortic valve: Four-dimensional MR evaluation of ascending aortic systolic flow patterns. Radiology 2010, 255, 53–61. [Google Scholar] [CrossRef]
- Barker, A.J.; Markl, M.; Bürk, J.; Lorenz, R.; Bock, J.; Bauer, S.; Schulz-Menger, J.; Von Knobelsdorff-Brenkenhoff, F. Bicuspid aortic valve is associated with altered wall shear stress in the ascending aorta. Circ. Cardiovasc. Imaging 2012, 5, 457–466. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Siu, S.C. Aortic dilatation in patients with bicuspid aortic valve. N. Engl. J. Med. 2014, 370, 1920–1929. [Google Scholar] [CrossRef] [Green Version]
- Tadros, T.M.; Klein, M.D.; Shapira, O.M. Ascending aortic dilatation associated with bicuspid aortic valve: Pathophysiology, molecular biology, and clinical implications. Circulation 2009, 119, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Nkomo, V.T.; Enriquez-Sarano, M.; Ammash, N.M.; Melton, L.J.; Bailey, K.R.; Desjardins, V.; Horn, R.A.; Tajik, A.J. Bicuspid aortic valve associated with aortic dilatation: A community-based study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, W.K.; Regeer, M.V.; Ng, A.C.; McCormack, L.; Poh, K.K.; Yeo, T.C.; Shanks, M.; Parent, S.; Enache, R.; Popescu, B.A.; et al. Sex Differences in Phenotypes of Bicuspid Aortic Valve and Aortopathy: Insights From a Large Multicenter, International Registry. Circ. Cardiovasc. Imaging. 2017, 10, e005155. [Google Scholar] [CrossRef] [Green Version]
- Wallby, L.; Janerot-Sjoberg, B.; Steffensen, T.; Broqvist, M. T lymphocyte infiltration in non-rheumatic aortic stenosis: A comparative descriptive study between tricuspid and bicuspid aortic valves. Heart 2002, 88, 348–351. [Google Scholar] [CrossRef] [Green Version]
- Ward, C. Clinical significance of the bicuspid aortic valve. Heart 2000, 83, 81–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstone, A.B.; Chiu, P.; Woo, Y.J. Prosthesis Type for Aortic- and Mitral-Valve Replacement. N. Engl. J. Med. 2018, 378, 778–779. [Google Scholar] [PubMed]
- Aicher, D.; Holz, A.; Feldner, S.; Kollner, V.; Schafers, H.J. Quality of life after aortic valve surgery: Replacement versus reconstruction. J. Thorac. Cardiovasc. Surg. 2011, 142, e19–e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panduranga, P.; Al-Mukhaini, M.; Al-Muslahi, M.; Haque, M.A.; Shehab, A. Management dilemmas in patients with mechanical heart valves and warfarin-induced major bleeding. World J. Cardiol. 2012, 4, 54–59. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall Cohort | |
|---|---|
| Age at operation | 58.7 ± 13.2 |
| Gender (female) | 16 (33.3) |
| Indication | - |
| AS | 30 (62) |
| AR | 9 (19) |
| Combined | 9 (19) |
| Previous cardiac operation | 6 (13) |
| Creatinine | 0.93 (0.86–1.07) |
| ≥2 mg/dL | 0 |
| Atrial fibrillation | 5 (10) |
| Diabetes mellitus | 2 (4) |
| Decompensation cordis | 4 (8) |
| Hypertension | 15 (32) |
| Hypercholesterolemia | 5 (10) |
| Previous myocardial infarction | 3 (6) |
| Previous PCI | 1 (2) |
| COPD | 1 (2) |
| Endocarditis | 2 (4) |
| History of cancer | 3 (6) |
| Stroke/TIA | 2 (4) |
| Stroke | 1 (2) |
| TIA | 2 (4) |
| Arterial disease | 3 (6) |
| Carotid | 1 (2) |
| Peripheral | 2 (4) |
| Concomitant CABG | 8 (17) |
| Aortic surgery | - |
| Aortic root replacement | 10 (21) |
| Supracoronay ascendens replacement | 38 (79) |
| Ascendens + Hemi(arch) | 13 (27) |
| Valve size | 24.8 ± 2.3 |
| Urgency | - |
| Emergent | 3 (7) |
| Not emergent | 42 (93) |
| LVEF | - |
| Preserved | 35 (76) |
| Mildly reduced | 3 (7) |
| Moderately reduced | 6 (13) |
| Severely reduced | 2 (4) |
| Valve (mechanical) | 29 (60) |
| Characteristics | Univariable HR (95% CI); p-Value |
|---|---|
| Age | 1.04 (1.00–1.10); p = 0.20 |
| Sex (female) | 1.7 (0.5–5.4); p = 0.37 |
| AS | 1.7 (0.4–6.1); p = 0.44 |
| AR | 0.2 (0.01–3.3); p = 0.25 |
| Hypertension | 1.1 (0.3–3.7); p = 0.86 |
| Hypercholesterolemia | 1.0 (0.8–1.1); p = 0.29 |
| Diabetes mellitus | 1.4 (0.9–2.1); p = 0.14 |
| Arterial disease | 2.3 (0.3–18.4); p = 0.44 |
| Renal failure | 1.3 (0.6–3.0); p = 0.49 |
| Previous MI | 3.1 (0.7–14.3); p = 0.14 |
| Previous PCI | 1.1 (0.6–2.1); p = 0.74 |
| Decompensated heart failure | 0.8 (0.1–6.1); p = 0.82 |
| LVEF < 50% | 1.8 (0.5–6.2); p = 0.35 |
| Atrial fibrillation | 0.7 (0.1–6.0); p = 0.80 |
| Previous stroke or TIA | 2.0 (0.2–15.3); p = 0.52 |
| COPD | 1.9 (1.3–2.8); p = 0.002 |
| Concomitant CABG | 1.4 (0.4–5.1); p = 0.64 |
| Emergent SAVR versus non-emergent | 1.7 (0.2–13.5); p = 0.62 |
| Mechanical prosthesis | 1.0 (0.2–4.3); p = 0.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çelik, M.; Mahtab, E.A.F.; Bogers, A.J.J.C. Surgical Aortic Valve Replacement with Concomitant Aortic Surgery in Patients with Purely Bicuspid Aortic Valve and Associated Aortopathy. J. Cardiovasc. Dev. Dis. 2021, 8, 16. https://doi.org/10.3390/jcdd8020016
Çelik M, Mahtab EAF, Bogers AJJC. Surgical Aortic Valve Replacement with Concomitant Aortic Surgery in Patients with Purely Bicuspid Aortic Valve and Associated Aortopathy. Journal of Cardiovascular Development and Disease. 2021; 8(2):16. https://doi.org/10.3390/jcdd8020016
Chicago/Turabian StyleÇelik, Mevlüt, Edris A. F. Mahtab, and Ad J. J. C. Bogers. 2021. "Surgical Aortic Valve Replacement with Concomitant Aortic Surgery in Patients with Purely Bicuspid Aortic Valve and Associated Aortopathy" Journal of Cardiovascular Development and Disease 8, no. 2: 16. https://doi.org/10.3390/jcdd8020016
APA StyleÇelik, M., Mahtab, E. A. F., & Bogers, A. J. J. C. (2021). Surgical Aortic Valve Replacement with Concomitant Aortic Surgery in Patients with Purely Bicuspid Aortic Valve and Associated Aortopathy. Journal of Cardiovascular Development and Disease, 8(2), 16. https://doi.org/10.3390/jcdd8020016