
Combining Stress Speckle Tracking with High-Sensitivity C-Reactive Protein in Diagnosis of Coronary Artery Disease


Abstract
:1. Introduction
2. Methods
2.1. Echocardiography
2.2. Dobutamine Echocardiography
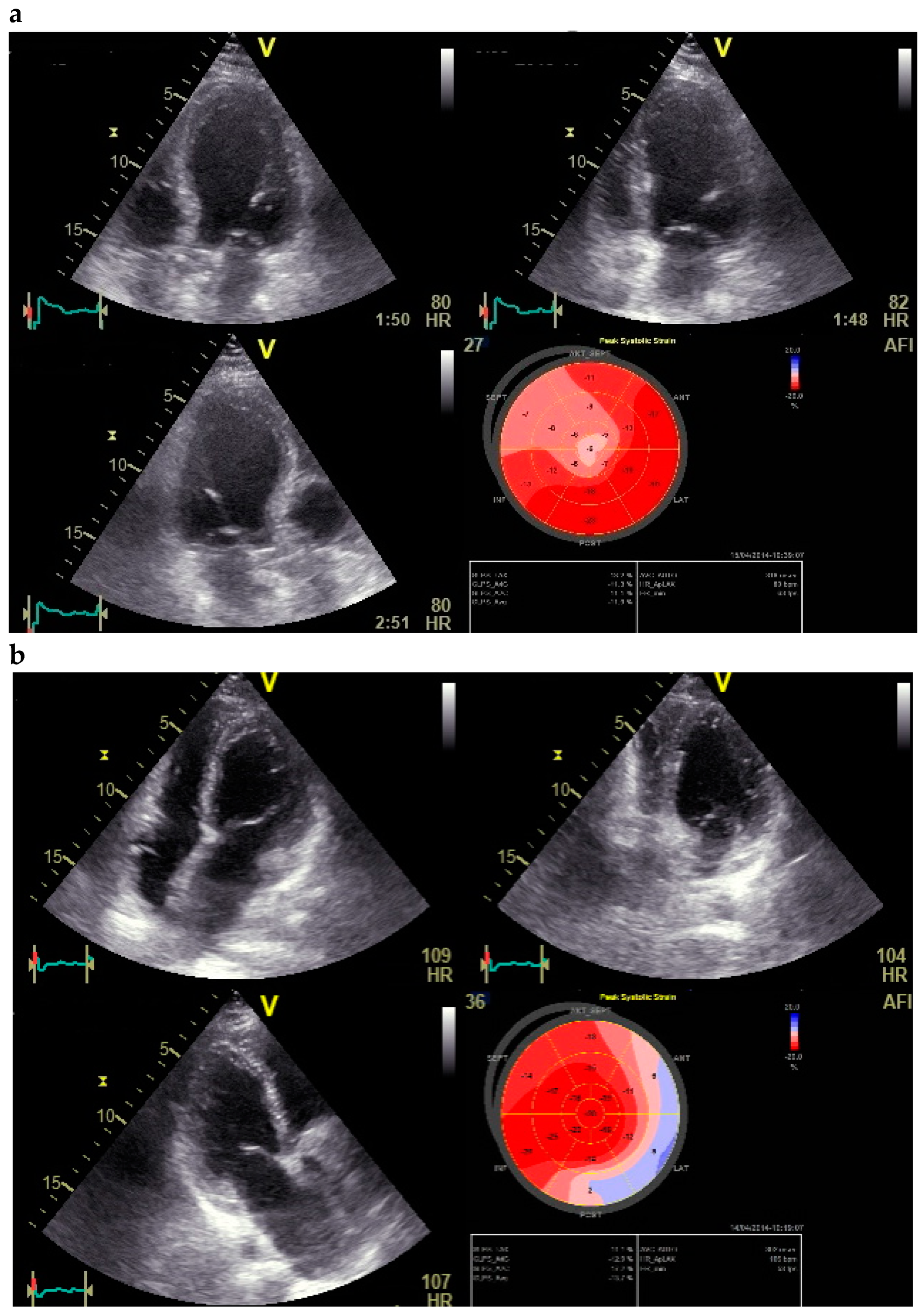
2.3. Quantification of Strain Measurements
2.4. Statistical Analysis
3. Results
3.1. Demographic Features
3.2. Reproducibility of Obtained Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hausmann, H.; Topp, H.; Siniawski, H.; Holz, S.; Hetzer, R. Decision Making in End-Stage Coronary Artery Disease: Revascularization or Heart Transplantation? Ann. Thorac. Surg. 1997, 64, 1296–1302. [Google Scholar] [CrossRef]
- Hoffmann, R.; Lethen, H.; Marwick, T.; Arnese, M.; Fioretti, P.; Pingitore, A.; Picano, E.; Buck, T.; Erbel, R.; Flachskampf, F.A.; et al. Analysis of interinstitutional observer agreement in interpretation of dobutamine stress echocardiograms. J. Am. Coll. Cardiol. 1996, 27, 330–336. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Lattanzi, F.; Orlandini, A.; Marini, C.; L’Abbate, A. Stress echocardiography and the human factor: The importance of being expert. J. Am. Coll. Cardiol. 1991, 17, 666–669. [Google Scholar] [CrossRef] [Green Version]
- Franke, A.; Hoffmann, R.; Kuhl, H.P.; Lepper, W.; Breithardt, O.A.; Schormann, M.; Hanrath, P. Non-contrast second harmonic imaging improves interobserver agreement and accuracy of dobutamine stress echocardiography in patients with impaired image quality. Heart 2000, 83, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, R.; Marwick, T.H.; Poldermans, D.; Lethen, H.; Ciani, R.; van der Meer, P.; Tries, H.-P.; Gianfagna, P.; Fioretti, P.; Bax, J.J.; et al. Refinements in stress echocardiographic techniques improve inter-institutional agreement in interpretation of dobutamine stress echocardiograms. Eur. Heart J. 2002, 23, 821–829. [Google Scholar] [CrossRef] [Green Version]
- Støylen, A.; Heimdal, A.; Bjørnstad, K.; Wiseth, R.; Vik-Mo, H.; Torp, H.; Angelsen, B.; Skjærpe, T. SRI by ultrasonography in the diagnosis of coronary artery disease. J. Am. Soc. Echocardiogr. 2000, 13, 1053–1064. [Google Scholar] [CrossRef]
- Jamal, F.; Strotmann, J.; Weidemann, F.; Kukulski, T.; D’Hooge, J.; Bijnens, B.; Van de Werf, F.; De Scheerder, I.; Sutherland, G.R. Noninvasive quantification of the contractile reserve of stunned myocardium by ultrasonic strain rate and strain. Circulation 2001, 104, 1059–1065. [Google Scholar] [CrossRef] [Green Version]
- Weidemann, F.; Jamal, F.; Sutherland, G.R.; Claus, P.; Kowalski, M.; Hatle, L.; De Scheerder, I.; Bijnens, B.; Rademakers, F.E. Myocardial function defined by strain rate and strain during alterations in inotropic states and heart rate. Am. J. Physiol. 2002, 283, H792–H799. [Google Scholar] [CrossRef] [Green Version]
- Abraham, T.P.; Belohlavek, M.; Thomson, H.; Pislaru, C.; Khandheria, B.; Seward, J.B.; Pellikka, P.A. Time to onset of regional relaxation: Feasibility, variability and utility of a novel index of regional myocardial function by SRI. J. Am. Coll. Cardiol. 2002, 39, 1531–1537. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Mao, L.; Chen, J.; Zhang, T.; Weng, S.; Guo, X.; Kuang, J.; Yu, B.; Peng, D. High-sensitivity CRP may be a marker of HDL dysfunction and remodeling in patients with acute coronary syndrome. Sci. Rep. 2021, 11, 11444. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, S.; Fang, S.; Yu, B. Prognostic Role of High Sensitivity C-Reactive Protein in Patients with Acute Myocardial Infarction. Front. Cardiovasc. Med. 2021, 8, 659446. [Google Scholar] [CrossRef] [PubMed]
- Shimoni, S.; Gendelman, G.; Ayzenberg, O.; Smirin, N.; Lysyansky, P.; Edri, O.; Deutsch, L.; Caspi, A.; Friedman, Z. Differential effects of coronary artery stenosis on myocardial function: The value of myocardial strain analysis for the detection of coronary artery disease. J. Am. Soc. Echocardiogr. 2011, 24, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, D.E.; Puthumana, J.J.; Fox, J.M.; Ogunyankin, K.O. Global longitudinal strain aids the detection of nonobstructive coronary artery disease in the resting echocardiogram. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 579–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.O.; Cho, S.W.; Song, Y.B.; Cho, S.J.; Song, B.G.; Lee, S.-C.; Park, S.W. Longitudinal 2D strain at rest predicts the presence of left main and three vessel coronary artery disease in patients without regional wall motion abnormality. Eur. J. Echocardiogr. 2009, 10, 695–701. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, S.; Dahlslett, T.; Grenne, B.; Sjøli, B.; Smiseth, O.; Edvardsen, T.; Brunvand, H. Global longitudinal strain is a more reproducible measure of left ventricular function than ejection fraction regardless of echocardiographic training. Cardiovasc. Ultrasound 2019, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Biering-Sorensen, T.; Hoffmann, S.; Mogelvang, R.; Iversen, A.Z.; Galatius, S.; Fritz-Hansen, T.; Bech, J.; Jense, J.S. Myocardial strain analysis by 2-dimensional speckle tracking echocardiography improves diagnostics of coronary artery stenosis in stable angina pectoris. Circ. Cardiovascular. Imaging 2014, 7, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Daimon, M.; Ishii, K.; Kawata, T.; Miyazaki, S.; Hirose, K.; Ichikawa, R.; Chiang, S.-J.; Suzuki, H.; Miyauchi, K.; et al. Prediction of coronary artery stenosis at rest in patients with normal left ventricular wall motion. Segmental analyses using strain imaging diastolic index. Int. Heart J. 2013, 54, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Stanković, I.; Putnikovic, B.; Cvjetan, R.; Milicevic, P.; Panic, M.; Kalezic-Radmili, T.; Mandaric, T.; Vidakovic, R.; Cvorovic, V.; Neskovic, A.N. Visual assessment vs. strain imaging for the detection of critical stenosis of the left anterior descending coronary artery in patients without a history of myocardial infarction. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Hanekom, L.; Cho, G.-Y.; Leano, R.; Jeffriess, L.; Marwick, T.H. Comparison of two-dimensional speckle and tissue Doppler strain measurement during dobutamine stress echocardiography: An angiographic correlation. Eur. Heart J. 2007, 28, 1765–1772. [Google Scholar] [CrossRef]
- dos Santos, N.S.; Vilela, A.A.; Barretto, R.B.; Vale, M.P.; Rezende, M.O.; Ferreira, M.C.; Andrade, A.J.A.; Scorsioni, N.H.G.; de Queiroga, O.X.; Le Bihan, D. Aplicabilidade do Strain Longitudinal do Ventrículo Esquerdo na Angina Instável. Arq. Bras. Cardiol. 2018, 110, 354–361. [Google Scholar]
- Scharrenbroich, J.; Hamada, S.; Keszei, A.; Schröder, J.; Napp, A.; Almalla, M.; Becker, M.; Altioket, E. Use of two-dimensional speckle tracking echocardiography to predict cardiac events: Comparison of patients with acute myocardial infarction and chronic coronary artery disease. Clin. Cardiol. 2018, 41, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas, A.K.; Haque, T.; Banik, D.; Choudhury, S.R.; Khan, S.R.; Malik, F.-T.-N. Identification of significant coronary artery disease in patients with non-ST segment elevation acute coronary syndrome by myocardial strain analyses using three-dimensional speckle tracking echocardiography. Echocardiography 2018, 35, 1988–1996. [Google Scholar] [CrossRef] [PubMed]
- Mandoli, G.E.; Pastore, M.C.P.; Vasilijevaite, K.; Cameli, P.; D’Ascenzi, F.; Focardi, M.; Mondillo, S.; Cameli, M. Speckle tracking stress echocardiography: A valuable diagnostic technique or a burden for everyday practice? Echocardiography 2020, 37, 2123–2129. [Google Scholar] [CrossRef] [PubMed]
- Zito, C.; Longobardo, L.; Citro, R.; Galderisi, M.; Oreto, L.; Carerj, M.L.; Manganaro, R.; Cusmà-Piccione, M.; Todaro, M.C.; Di Bella, G.; et al. Ten Years of 2D Longitudinal Strain for Early Myocardial Dysfunction Detection: A Clinical Overview. Biomed. Res. Int. 2018, 5, 8979407. [Google Scholar] [CrossRef]
- Penson, P.E.; Long, D.L.; Howard, G.; Toth, P.P.; Muntner, P.; Howard, V.J.; Safford, M.M.; Jones, S.R.; Martin, S.S.; Mazidi, M.; et al. Associations between very low concentrations of low density lipoprotein cholesterol, high sensitivity C-reactive protein, and health outcomes in the Reasons for Geographical and Racial Differences in Stroke (REGARDS) study. Eur. Heart J. 2018, 39, 3641–3653. [Google Scholar] [CrossRef]
- Arroyo-Espliguero, R.; Avanzas, P.; Cosin-Sales, J.; Aldama, G.; Pizzi, C.; Kaski, J.C. C-reactive protein elevation and disease activity in patients with coronary artery disease. Eur. Heart J. 2004, 25, 401–408. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No CAD | CAD | p-Value | |
|---|---|---|---|
| Age (years) | 65 ± 12 | 63 ± 9 | 0.52 |
| Men no. | 13 | 41 | 0.05 |
| Hypertension no. (%) | 27 (77.1) | 60 (82.2) | 0.35 |
| DM no. (%) | 21 (60.0) | 31 (42.5) | 0.06 |
| Hyperlipidemia no. (%) | 12 (34.3) | 28 (38.4) | 0.42 |
| BMI kg/m2 | 24.7 ± 4.5 | 25.9 ± 4.2 | 0.17 |
| Medications | |||
| Aspirin | 2 (5.7) | 11 (15) | 0.17 |
| ACE-Blocker | 22 (62) | 51 (69) | 0.41 |
| Statins | 2 (5.7) | 3 (4.1) | 0.76 |
| Betablocker | 6 (17) | 38 (52) | 0.06 |
| Echocardiographic parameters | |||
| EF (%) | 58.0 ± 6.4 | 48.9 ± 5.9 | <0.001 |
| E/A ratio | 0.89 ± 0.5 | 0.89 ± 0.3 | 0.82 |
| E/E’ ratio | 8.1 ± 2.6 | 8.4 ± 3.2 | 0.27 |
| E/SRe ratio | 0.61 ± 0.45 | 0.56 ± 0.17 | 0.29 |
| WMA in stress echocardiography (no.) | 31 | 77 | 0.006 |
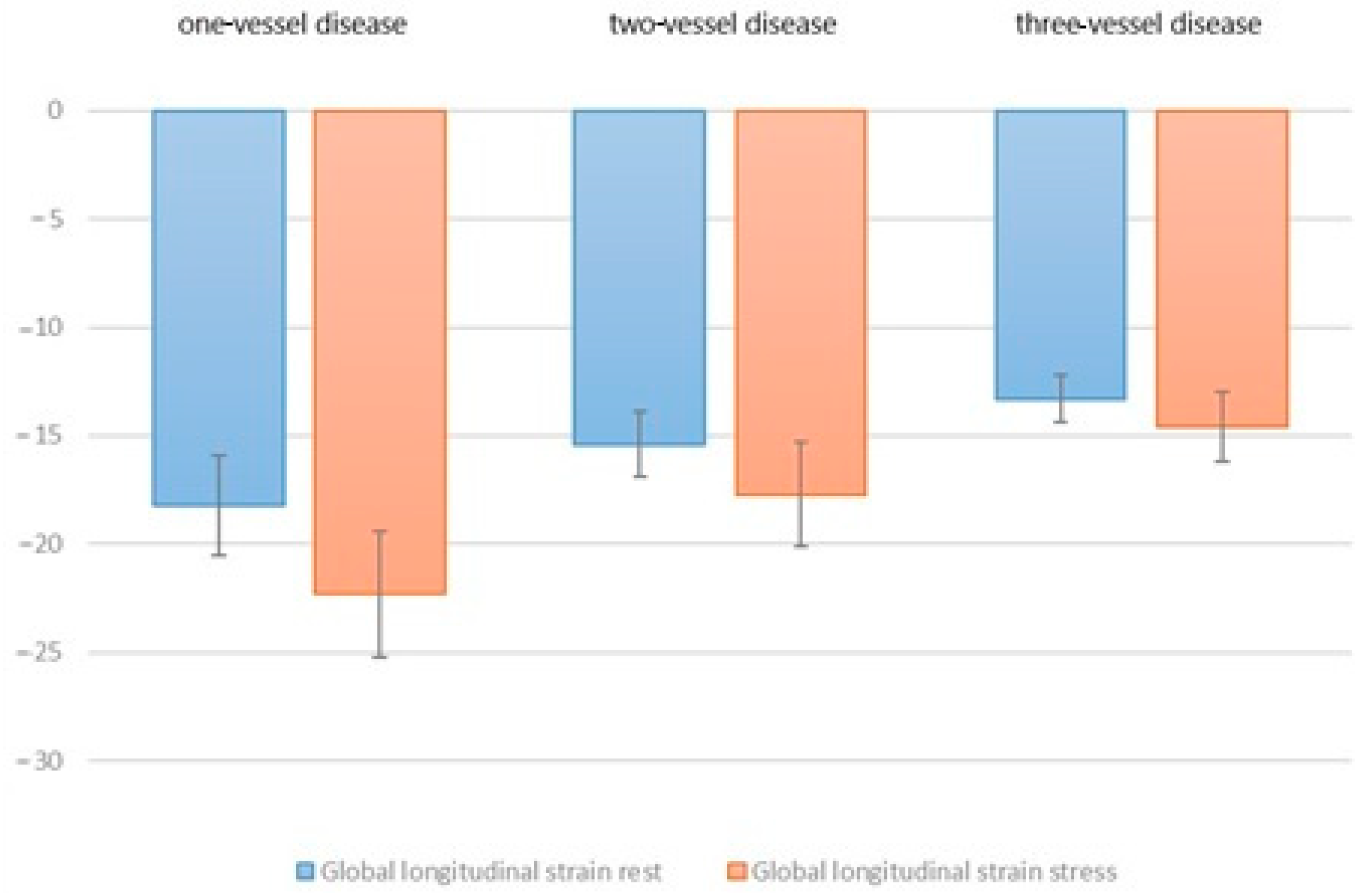
| GLS at rest (%) | −18.4 ± 3.1 | −16.9 ± 2.8 | <0.001 |
| GLS under stress (%) | −21.9 ± 3.7 | −20.8 ± 3.3 | 0.01 |
| Laboratory findings | |||
| Troponin (ng/mL) | 0.068 ± 0.02 | 0.081 ± 0.07 | 0.31 |
| Hs-CRP mg/L | 1.9 ± 1.5 | 3.2 ± 1.8 | <0.001 |
| Visual WMA | Global Longitudinal Strain at Rest | Global Longitudinal Strain under Stress | |
|---|---|---|---|
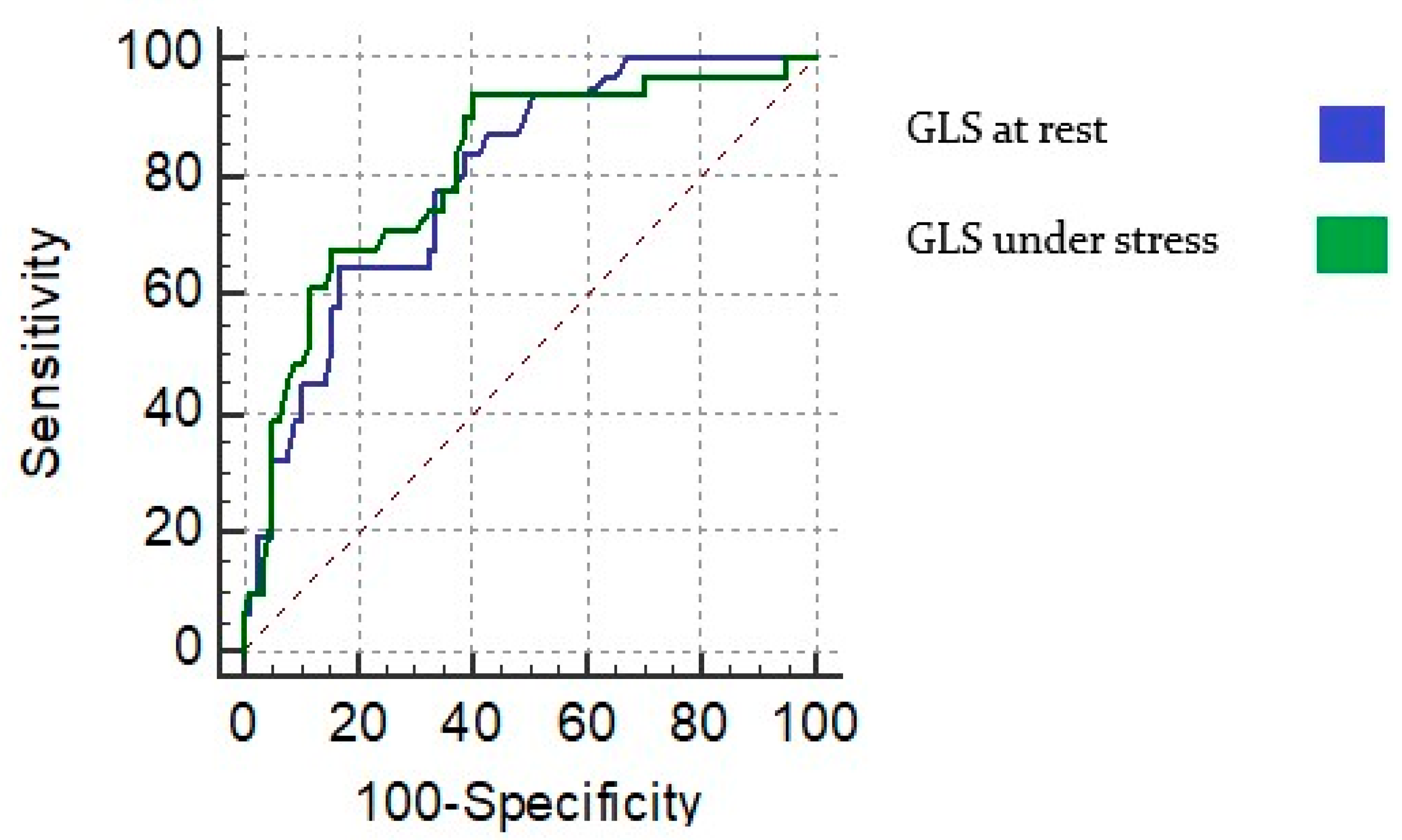
| Sensitivity | 61.2 (42.2–78.2) | 70.9 (51.9−85.7) | 74.2 (55.3–88.1) |
| Specificity | 67.5 (55.9–77.8) | 68.8 (57.3–78.9) | 76.7 (65.5–85.5) |
| Positive predictive value | 44.2 (33.9–54.9) | 47.8 (38.0–57.7) | 56.1 (44.7–66.8) |
| Negative predictive value | 81.2 (73.1–87.3) | 85.5 (76.9–91.2) | 88.1 (80.0–93.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saleh, A.M.; Zintl, K.; Brachmann, J. Combining Stress Speckle Tracking with High-Sensitivity C-Reactive Protein in Diagnosis of Coronary Artery Disease. J. Cardiovasc. Dev. Dis. 2022, 9, 123. https://doi.org/10.3390/jcdd9050123
Saleh AM, Zintl K, Brachmann J. Combining Stress Speckle Tracking with High-Sensitivity C-Reactive Protein in Diagnosis of Coronary Artery Disease. Journal of Cardiovascular Development and Disease. 2022; 9(5):123. https://doi.org/10.3390/jcdd9050123
Chicago/Turabian StyleSaleh, Ahmed M., Konstantin Zintl, and Johannes Brachmann. 2022. "Combining Stress Speckle Tracking with High-Sensitivity C-Reactive Protein in Diagnosis of Coronary Artery Disease" Journal of Cardiovascular Development and Disease 9, no. 5: 123. https://doi.org/10.3390/jcdd9050123
APA StyleSaleh, A. M., Zintl, K., & Brachmann, J. (2022). Combining Stress Speckle Tracking with High-Sensitivity C-Reactive Protein in Diagnosis of Coronary Artery Disease. Journal of Cardiovascular Development and Disease, 9(5), 123. https://doi.org/10.3390/jcdd9050123