
Gene Expression Profiling of Markers of Inflammation, Angiogenesis, Coagulation and Fibrinolysis in Patients with Coronary Artery Disease with Very High Lipoprotein(a) Levels Treated with PCSK9 Inhibitors



Abstract
:1. Introduction
2. Materials and Methods
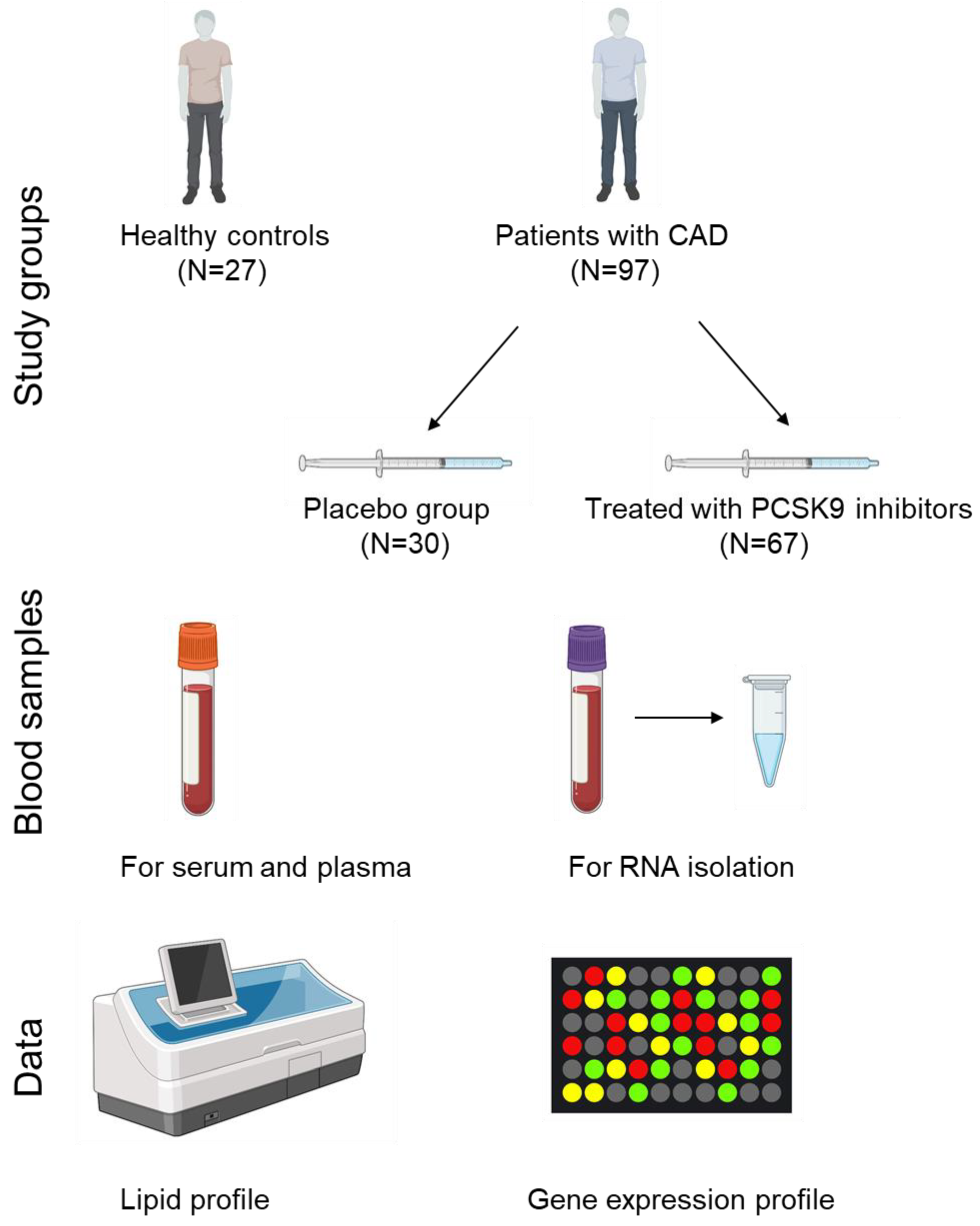
2.1. Study Subjects
2.2. Blood Collection and Lipid Profile Determination
2.3. Total RNA Isolation and Evaluation
2.4. Gene Expression Profiling
2.5. Statistical Analysis
3. Results
3.1. Study Groups
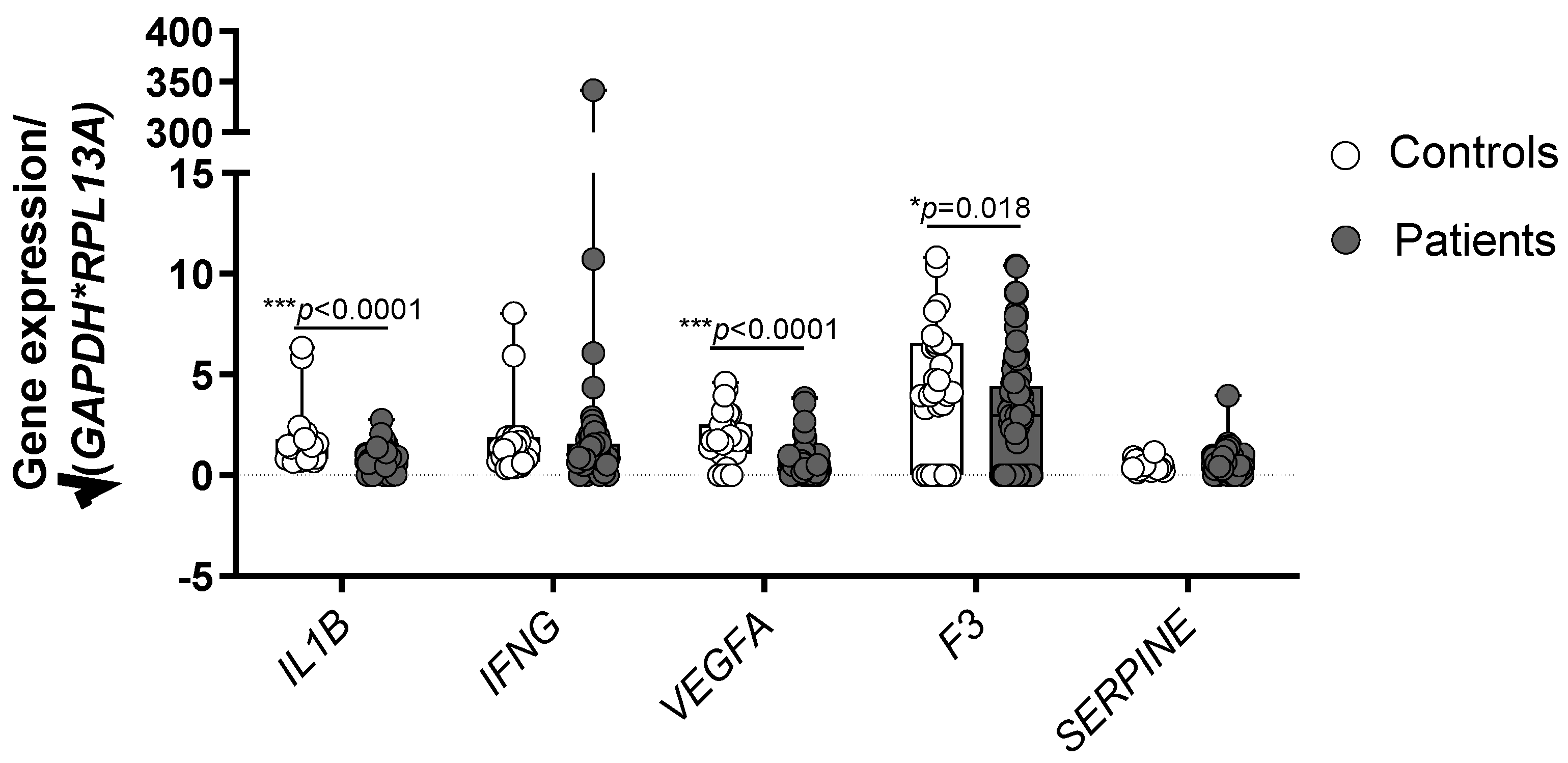
3.2. Healthy Controls Show Higher Expression of IL1B, VEGFA and F3 in Comparison with CAD Patients
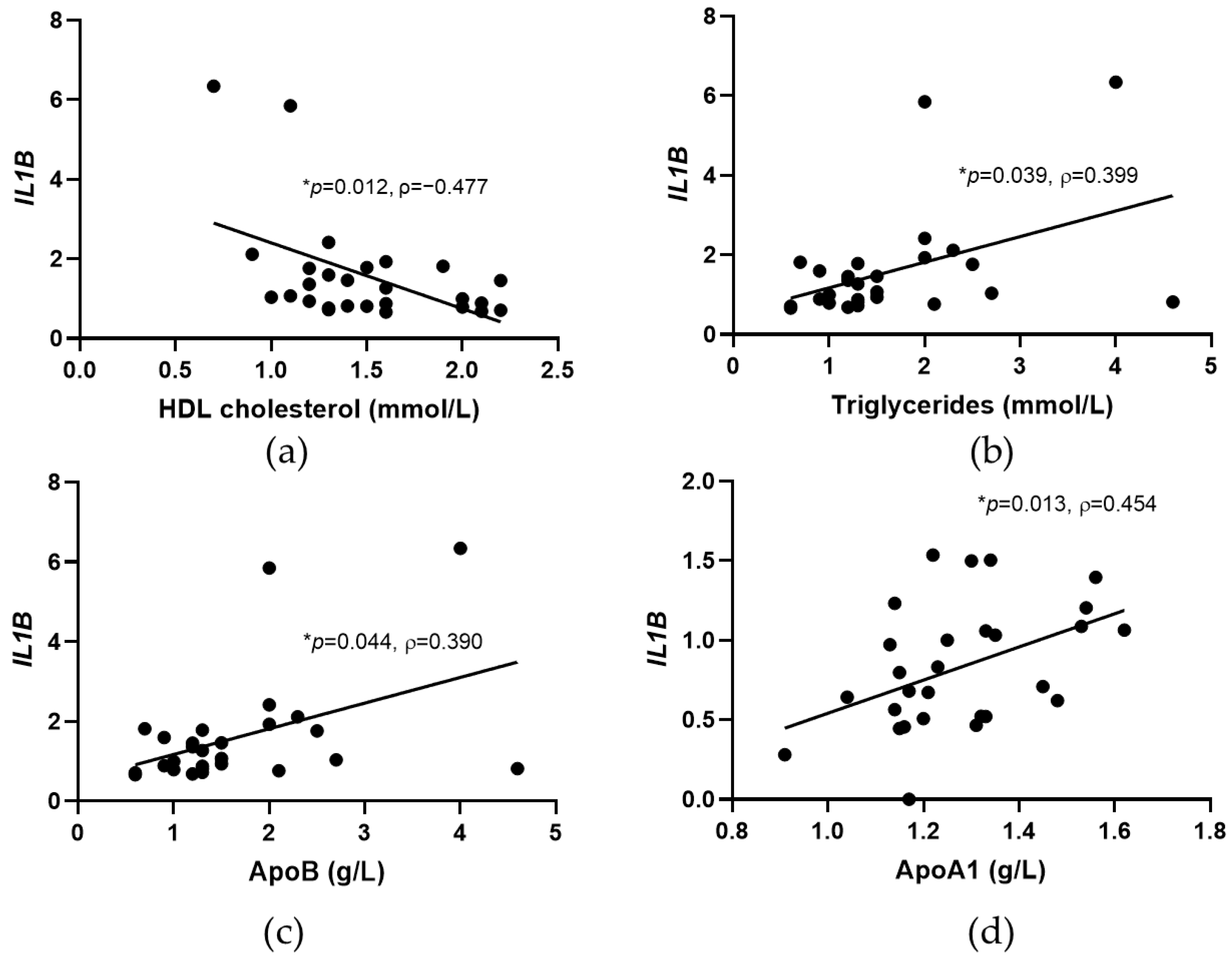
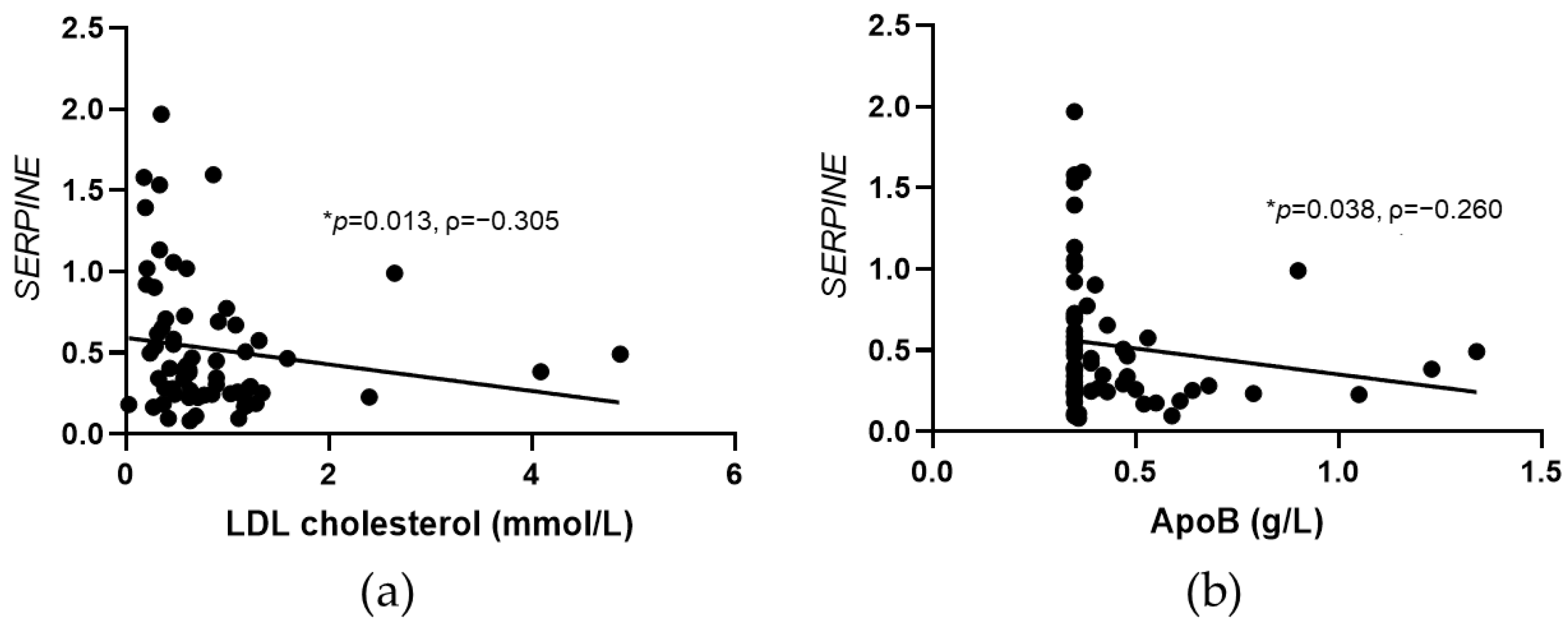
3.3. Significant Correlations between IL1B and SERPINE Expression and Lipid Parameters in Controls and CAD Patients
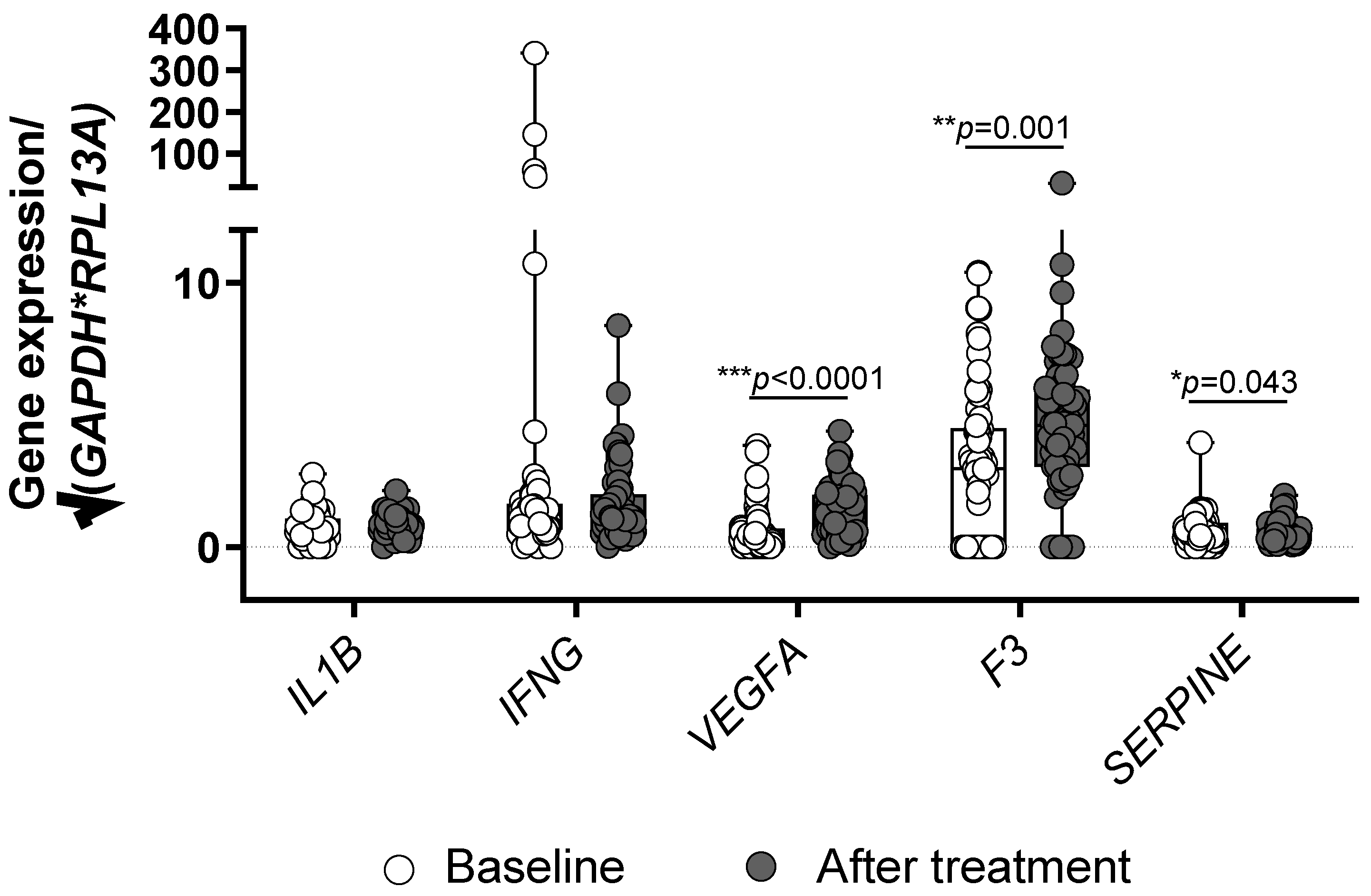
3.4. Treatment with PCSK9 Inhibitors Influences the Expression of VEGFA, F3 and SERPINE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ApoA1 | apolipoprotein A1 |
| ApoB | apolipoprotein B |
| CAD | coronary artery disease |
| HDL cholesterol | high density lipoprotein cholesterol |
| hsCRP | high sensitivity C reactive protein |
| IFN-γ | interferon-γ |
| IL-1β | Interleukin-1β |
| LDL cholesterol | low density lipoprotein cholesterol |
| Lp(a) | lipoprotein(a) |
| PAI-1 | tissue plasminogen activator inhibitor-1 |
| PCSK9 | proprotein convertase subtilisin/kexin type 9 |
| TF | tissue factor |
| VEGF-A | vascular endothelial growth factor-A |
References
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskina, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, R.; Frohlich, J. Lipoprotein (a), an independent cardiovascular risk marker. Clin. Diabetes Endocrinol. 2016, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ugovšek, S.; Šebeštjen, M. Lipoprotein(a)-the crossroads of atherosclerosis, atherothrombosis and inflammation. Biomolecules 2021, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Biros, E.; Reznik, J.E.; Moran, C.S. Role of inflammatory cytokines in genesis and treatment of atherosclerosis. Trends Cardiovasc. Med. 2022, 32, 138–142. [Google Scholar] [CrossRef]
- Libby, P. Interleukin-1 Beta as a target for atherosclerosis therapy: Biological basis of CANTOS and beyond. J. Am. Coll. Cardiol. 2017, 70, 2278–2289. [Google Scholar] [CrossRef] [PubMed]
- Eržen, B.; Šilar, M.; Šabovič, M. Stable phase post-MI patients have elevated VEGF levels correlated with inflammation markers, but not with atherosclerotic burden. BMC Cardiovasc. Disord. 2014, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Tremoli, E.; Camera, M.; Toschi, V.; Colli, S. Tissue factor in atherosclerosis. Atherosclerosis 1999, 144, 273–283. [Google Scholar] [CrossRef]
- Grover, S.P.; Mackman, N. Tissue factor in atherosclerosis and atherothrombosis. Atherosclerosis 2020, 307, 80–86. [Google Scholar] [CrossRef]
- Fuster, V.; Badimon, L.; Badimon, J.J.; Chesebro, J.H. The pathogenesis of coronary artery disease and the acute coronary syndromes (2). N. Engl. J. Med. 1992, 326, 310–318. [Google Scholar] [CrossRef]
- Levy, G.A.; Schwartz, B.S.; Curtiss, L.K.; Edgington, T.S. Plasma lipoprotein induction and suppression of the generation of cellular procoagulant activity in vitro. J. Clin. Investig. 1981, 67, 1614–1622. [Google Scholar] [CrossRef] [PubMed]
- Konkle, B.A. Bleeding and thrombosis. In Harrison’s Principles of Internal Medicine; Jameson, J., Fauci, A.S., Kasper, D.L., Hauser, S.L., Longo, D.L., Loscalzo, J., Eds.; McGraw Hill: New York, NY, USA, 2018; Chapter 61. [Google Scholar]
- Nilsson, T.; Wallen, P. The fibrinolytic system: Biochemistry and assay methods. In Clinical Aspects of Fibrinolysis; Nilsson, T.K., Boman, K., Jansson, J.H., Eds.; Almqvist & Wiksell International: Stockholm, Sweden, 1991; pp. 9–53. [Google Scholar]
- van Meijer, M.; Pannekoek, H. Structure of plasminogen activator inhibitor 1 (PAI-1) and its function in fibrinolysis: An update. Fibrinolysis 1995, 9, 263–276. [Google Scholar] [CrossRef]
- Tanaka, K.; Sueishi, K. Biology of disease. The coagulation and fibrinolysis systems and atherosclerosis. Lab. Investig. 1993, 69, 5–18. [Google Scholar] [PubMed]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.H.; Genest, J.; Gotto, A.M.; Kastelein, J.J.P.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šebeštjen, M.; Keber, I.; Žegura, B.; Simčič, S.; Božič, M.; Fressart, M.M.; Stegnar, M. Statin and fibrate treatment of combined hyperlipidemia: The effects on some novel risk factors. Thromb. Haemost. 2004, 92, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.X.; Li, S.; Liu, H.H.; Li, J.J. Impact of PCSK9 monoclonal antibodies on circulating hs-CRP levels: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2018, 8, e022348. [Google Scholar] [CrossRef] [Green Version]
- Likozar, A.R.; Blinc, A.; Podkrajšek, K.T.; Šebeštjen, M. LPA genotypes and haplotypes are associated with lipoprotein(a) levels but not arterial wall properties in stable post-coronary event patients with very high lipoprotein(a) levels. J. Cardiovasc. Dev. Dis. 2021, 8, 181. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G * Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Pombo-Suarez, M.; Calaza, M.; Gomez-Reino, J.J.; Gonzalez, A. Reference genes for normalization of gene expression studies in human osteoarthritic articular cartilage. BMC Mol. Biol. 2008, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Zupan, J.; Komadina, R.; Marc, J. The relationship between osteoclastogenic and anti-osteoclastogenic pro-inflammatory cytokines differs in human osteoporotic and osteoarthritic bone tissues. J. Biomed. Sci. 2012, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Vrtačnik, P.; Zupan, J.; Mlakar, V.; Kranjc, T.; Marc, J.; Kern, B.; Ostanek, B. Epigenetic enzymes influenced by oxidative stress and hypoxia mimetic in osteoblasts are differentially expressed in patients with osteoporosis and osteoarthritis. Sci. Rep. 2018, 8, 16215. [Google Scholar] [CrossRef] [PubMed]
- OriGene Technologies, I. Product Datasheet for HP200569. Available online: https://cdn.origene.com/datasheet/hp200569.pdf (accessed on 12 March 2022).
- OriGene Technologies, I. Product Datasheet for HP205750. Available online: https://cdn.origene.com/datasheet/hp205750.pdf (accessed on 12 March 2022).
- Liberale, L.; Carbone, F.; Camici, G.G.; Montecucco, F. IL-1β and statin treatment in patients with myocardial infarction and diabetic cardiomyopathy. J. Clin. Med. 2019, 8, 1764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Sim, M.M.S.; Wood, J.P. Recent insights into the regulation of coagulation and thrombosis. Arterioscler. Thromb. Vasc. Biol. 2020, 40, E119–E125. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Bharadwaj, D.; Prasad, G.; Grechko, A.V.; Sazonova, M.A.; Orekhov, A.N. Renin-angiotensin system in pathogenesis of atherosclerosis and treatment of CVD. Int. J. Mol. Sci. 2021, 22, 6702. [Google Scholar] [CrossRef] [PubMed]
- Vrablik, M.; Corsini, A.; Tůmová, E. Beta-blockers for atherosclerosis prevention: A missed opportunity? Curr. Atheroscler. Rep. 2022, 24, 161–169. [Google Scholar] [CrossRef]
- Siwik, D.; Gajewska, M.; Karoń, K.; Pluta, K.; Wondołkowski, M.; Wilimski, R.; Szarpak, Ł.; Filipiak, K.J.; Gąsecka, A. Pleiotropic effects of acetylsalicylic acid after coronary artery bypass grafting-beyond platelet inhibition. J. Clin. Med. 2021, 10, 2317. [Google Scholar] [CrossRef]
- Braile, M.; Marcella, S.; Cristinziano, L.; Galdiero, M.R.; Modestino, L.; Ferrara, A.L.; Varricchi, G.; Marone, G.; Loffredo, S. VEGF-A in cardiomyocytes and heart diseases. Int. J. Mol. Sci. 2020, 21, 5294. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N.; Gerber, H.P.; LeCouter, J. The biology of VEGF and its receptors. Nat. Med. 2003, 9, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Teixeira Silva, C.; Cândido, A.P.C.; Pala, D.; Oliveira Barbosa, P.; Machado-Coelho, G.L.L.; Pereira De Oliveira, F.L.; Pinheiro Volp, A.C.; Nascimento De Freitas, R. Clustered cardiovascular risk factors are associated with inflammatory markers in adolescents. Ann. Nutr. Metab. 2017, 70, 259–267. [Google Scholar] [CrossRef]
- Barter, P.J.; Nicholls, S.; Rye, K.A.; Anantharamaiah, G.M.; Navab, M.; Fogelman, A.M. Antiinflammatory properties of HDL. Circ. Res. 2004, 95, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicki, A.S.; Kim, E.J.; Esan, O.; Ramachandran, R. Hypertriglyceridaemia: An update. J. Clin. Pathol. 2022. [Google Scholar] [CrossRef]
- Orsó, E.; Schmitz, G. Lipoprotein(a) and its role in inflammation, atherosclerosis and malignancies. Clin. Res. Cardiol. Suppl. 2017, 12, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsimikas, S.; Witztum, J.L. The role of oxidized phospholipids in mediating lipoprotein(a) atherogenicity. Curr. Opin. Lipidol. 2008, 19, 369–377. [Google Scholar] [CrossRef]
- Hoogeveen, R.M.; Opstal, T.S.J.; Kaiser, Y.; Stiekema, L.C.A.; Kroon, J.; Knol, R.J.J.; Bax, W.A.; Verberne, H.J.; Cornel, J.H.; Stroes, E.S.G. PCSK9 antibody alirocumab attenuates arterial wall inflammation without changes in circulating inflammatory markers. JACC. Cardiovasc. Imaging 2019, 12, 2571–2573. [Google Scholar] [CrossRef] [PubMed]
- Stiekema, L.C.A.; Stroes, E.S.G.; Verweij, S.L.; Kassahun, H.; Chen, L.; Wasserman, S.M.; Sabatine, M.S.; Mani, V.; Fayad, Z.A. Persistent arterial wall inflammation in patients with elevated lipoprotein(a) despite strong low-density lipoprotein cholesterol reduction by proprotein convertase subtilisin/kexin type 9 antibody treatment. Eur. Heart J. 2019, 40, 2775–2781. [Google Scholar] [CrossRef] [Green Version]
- Marques, P.; Domingo, E.; Rubio, A.; Martinez-Hervás, S.; Ascaso, J.F.; Piqueras, L.; Real, J.T.; Sanz, M.J. Beneficial effects of PCSK9 inhibition with alirocumab in familial hypercholesterolemia involve modulation of new immune players. Biomed. Pharmacother. 2022, 145, 112460. [Google Scholar] [CrossRef]
- Dzobo, K.E.; Kraaijenhof, J.M.; Stroes, E.S.G.; Nurmohamed, N.S.; Kroon, J. Lipoprotein(a): An underestimated inflammatory mastermind. Atherosclerosis 2022, 349, 101–109. [Google Scholar] [CrossRef]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Thögersen, A.M.; Jansson, J.H.; Boman, K.; Nilsson, T.K.; Weinehall, L.; Huhtasaari, F.; Hallmans, G. High plasminogen activator inhibitor and tissue plasminogen activator levels in plasma precede a first acute myocardial infarction in both men and women: Evidence for the fibrinolytic system as an independent primary risk factor. Circulation 1998, 98, 2241–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golukhova, E.Z.; Grigorian, M.V.; Ryabinina, M.N.; Bulaeva, N.I.; Fortmann, S.; Serebruany, V.L. Independent predictors of major adverse events following coronary stenting over 28 months of follow-up. Cardiology 2015, 132, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Catena, C.; Ray, K.K.; Vallejo-Vaz, A.J.; Reiner, Ž.; Sechi, L.A.; Colussi, G.L. Impact of statin therapy on plasma levels of plasminogen activator inhibitor-1. A systematic review and meta-analysis of randomised controlled trials. Thromb. Haemost. 2016, 116, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Basiak, M.; Hachula, M.; Kosowski, M.; Okopien, B. Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia. J. Clin. Med. 2022, 11, 2542. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls (N = 27) | Placebo (N = 30) | Treated (N = 67) | p (Controls vs. Placebo) | p (Controls vs. Treated) | |
|---|---|---|---|---|---|
| Age at inclusion (years) | 51 (47–52) | 49 (43–55) | 53 (46–56) | 0.108 | |
| M/F | 21/6 | 29/1 | 58/9 | 0.103 | |
| Total cholesterol (mmol/L) | 5.72 (5.22–6.18) | 4.08 (3.55–4.84) | 4.24 (3.69–4.74) | *** < 0.0001 | *** < 0.0001 |
| HDL cholesterol (mmol/L) | 1.37 (1.20–1.87) | 1.05 (0.95–1.31) | 1.15 (1.00–1.32) | *** < 0.0001 | * 0.003 |
| LDL cholesterol (mmol/L) | 3.40 (3.18–4.00) | 2.31 (1.70–2.69) | 2.34 (1.73–2.65) | *** < 0.0001 | *** < 0.0001 |
| Triglycerides (mmol/L) | 1.32 (1.01–2.03) | 1.64 (1.02–2.20) | 1.41 (1.05–2.13) | 0.853 | |
| Lp(a) (mg/L) | 11.0 (4.0–18.0) | 1477 (1113–1702) | 1400 (1187–1664) | *** < 0.0001 | *** < 0.0001 |
| ApoA1 (g/L) | 1.14 (1.03–1.26) | 0.79 (0.73–0.985) | 0.82 (0.63–0.97) | * 0.004 | 0.054 |
| ApoB (g/L) | 1.42 (1.29–1.58) | 1.23 (1.16–1.35) | 1.30 (1.20–1.46) | *** < 0.0001 | *** < 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrovat, K.; Rehberger Likozar, A.; Zupan, J.; Šebeštjen, M. Gene Expression Profiling of Markers of Inflammation, Angiogenesis, Coagulation and Fibrinolysis in Patients with Coronary Artery Disease with Very High Lipoprotein(a) Levels Treated with PCSK9 Inhibitors. J. Cardiovasc. Dev. Dis. 2022, 9, 211. https://doi.org/10.3390/jcdd9070211
Hrovat K, Rehberger Likozar A, Zupan J, Šebeštjen M. Gene Expression Profiling of Markers of Inflammation, Angiogenesis, Coagulation and Fibrinolysis in Patients with Coronary Artery Disease with Very High Lipoprotein(a) Levels Treated with PCSK9 Inhibitors. Journal of Cardiovascular Development and Disease. 2022; 9(7):211. https://doi.org/10.3390/jcdd9070211
Chicago/Turabian StyleHrovat, Katja, Andreja Rehberger Likozar, Janja Zupan, and Miran Šebeštjen. 2022. "Gene Expression Profiling of Markers of Inflammation, Angiogenesis, Coagulation and Fibrinolysis in Patients with Coronary Artery Disease with Very High Lipoprotein(a) Levels Treated with PCSK9 Inhibitors" Journal of Cardiovascular Development and Disease 9, no. 7: 211. https://doi.org/10.3390/jcdd9070211
APA StyleHrovat, K., Rehberger Likozar, A., Zupan, J., & Šebeštjen, M. (2022). Gene Expression Profiling of Markers of Inflammation, Angiogenesis, Coagulation and Fibrinolysis in Patients with Coronary Artery Disease with Very High Lipoprotein(a) Levels Treated with PCSK9 Inhibitors. Journal of Cardiovascular Development and Disease, 9(7), 211. https://doi.org/10.3390/jcdd9070211