Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
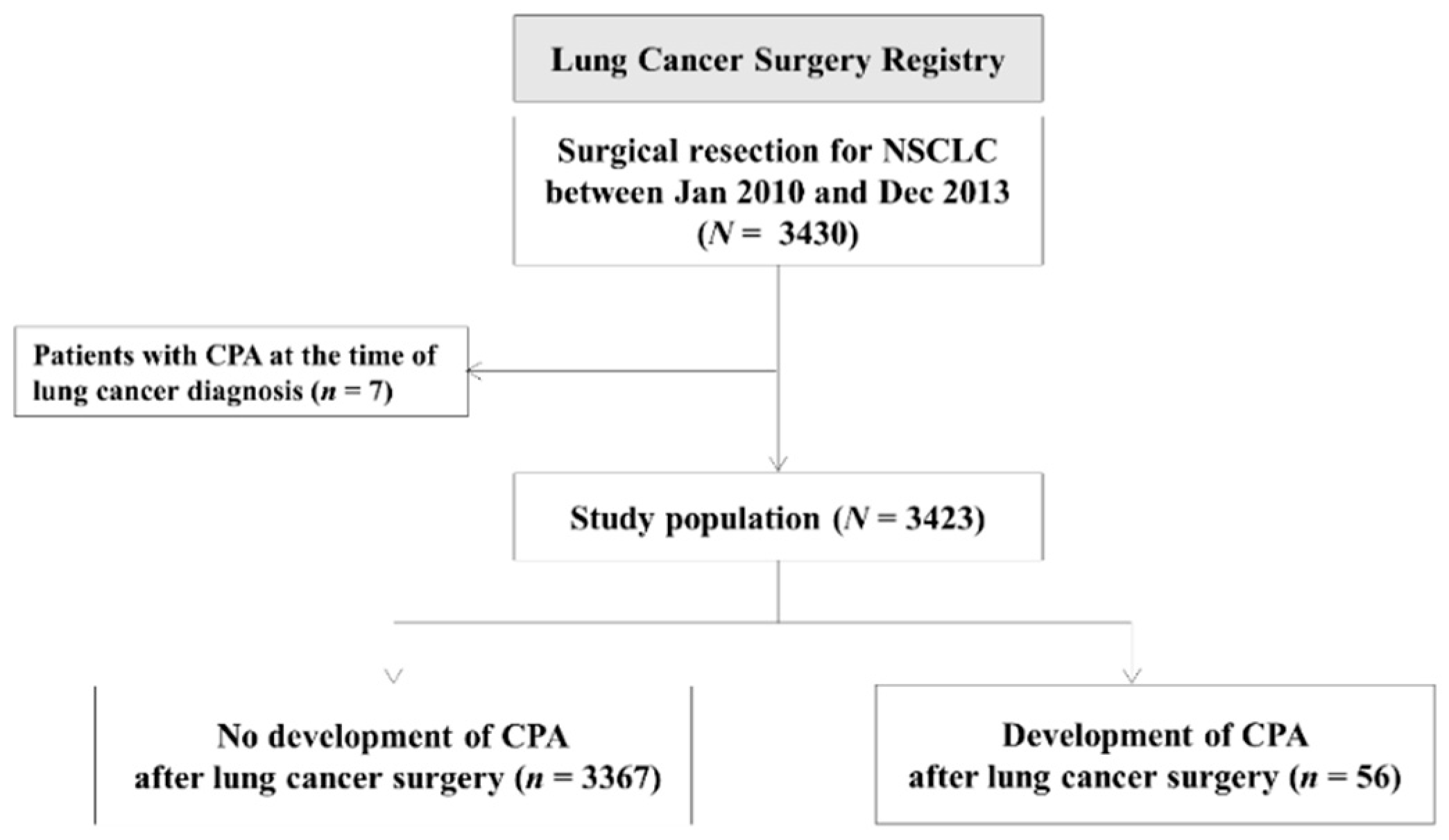
2.1. Study Population and Data Collection
2.2. Diagnosis of CPA
2.3. Statistical Analyses
3. Results
3.1. Study Population and Overall Survival
3.2. Development of CPA after Lung Cancer Surgery
3.3. Factors Associated with the Development of CPA
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| aHR | adjusted hazard ratio |
| BMI | body mass index |
| COPD | chronic obstructive pulmonary disease |
| CPA | chronic pulmonary aspergillosis |
| CI | confidence interval |
| CT | computed tomography |
| HR | hazard ratio |
| IQR | interquartile range |
| ILD | interstitial lung disease |
| IPF | idiopathic pulmonary fibrosis |
| NSCLC | non-small-cell lung cancer |
| OS | overall survival |
| PPC | postoperative pulmonary complication |
| TB | tuberculosis |
| VATS | video-assisted thoracoscopic surgery |
References
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- Henschke, C.I.; Yankelevitz, D.F.; Libby, D.M.; Pasmantier, M.W.; Smith, J.P.; Miettinen, O.S. Survival of patients with stage I lung cancer detected on CT screening. N. Engl. J. Med. 2006, 355, 1763–1771. [Google Scholar] [PubMed] [Green Version]
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; Sicks, J.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [PubMed] [Green Version]
- Um, S.W.; Kim, H.K.; Jung, S.H.; Han, J.; Lee, K.J.; Park, H.Y.; Choi, Y.S.; Shim, Y.M.; Ahn, M.J.; Park, K.; et al. Endobronchial ultrasound versus mediastinoscopy for mediastinal nodal staging of non-small-cell lung cancer. J. Thorac. Oncol. 2015, 10, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taioli, E.; Lee, D.S.; Lesser, M.; Flores, R. Long-term survival in video-assisted thoracoscopic lobectomy vs open lobectomy in lung-cancer patients: A meta-analysis. Eur. J. Cardiothorac. Surg. 2013, 44, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapadia, N.S.; Valle, L.F.; George, J.A.; Jagsi, R.; D’Amico, T.A.; Dexter, E.U.; Vigneau, F.D.; Kong, F.M. Patterns of Treatment and Outcomes for Definitive Therapy of Early Stage Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2017, 104, 1881–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2016, National Cancer Institute; Bethesda: Montgomery, MD, USA, 2019; based on November 2018 SEER data submission, posted to the SEER web site, April 2019. Available online: https://seer.cancer.gov/csr/1975_2016/results_merged/sect_15_lung_bronchus.pdf (accessed on 2 November 2020).
- Andalib, A.; Ramana-Kumar, A.V.; Bartlett, G.; Franco, E.L.; Ferri, L.E. Influence of postoperative infectious complications on long-term survival of lung cancer patients: A population-based cohort study. J. Thorac. Oncol. 2013, 8, 554–561. [Google Scholar] [CrossRef] [Green Version]
- Agostini, P.; Cieslik, H.; Rathinam, S.; Bishay, E.; Kalkat, M.S.; Rajesh, P.B.; Steyn, R.S.; Singh, S.; Naidu, B. Postoperative pulmonary complications following thoracic surgery: Are there any modifiable risk factors? Thorax 2010, 65, 815–818. [Google Scholar] [CrossRef] [Green Version]
- Lugg, S.T.; Agostini, P.J.; Tikka, T.; Kerr, A.; Adams, K.; Bishay, E.; Kalkat, M.S.; Steyn, R.S.; Rajesh, P.B.; Thickett, D.R.; et al. Long-term impact of developing a postoperative pulmonary complication after lung surgery. Thorax 2016, 71, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global burden of chronic pulmonary aspergillosis as a sequel to pulmonary tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, I.D.; Byanyima, R.; Hosmane, S.; Onyachi, N.; Opira, C.; Richardson, M.; Sawyer, R.; Sharman, A.; Denning, D.W. Chronic pulmonary aspergillosis commonly complicates treated pulmonary tuberculosis with residual cavitation. Eur. Respir. J. 2019, 53, e1801184. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A.; Suzuki, J.; Fukami, T.; Matsui, H.; Akagawa, S.; Ohta, K.; Hebisawa, A.; Takahashi, F. Chronic pulmonary aspergillosis as a sequel to lobectomy for lung cancer. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 650–656. [Google Scholar] [CrossRef] [Green Version]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Miskovic, A.; Lumb, A.B. Postoperative pulmonary complications. Br. J. Anaesth. 2017, 118, 317–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhun, B.W.; Jeon, K.; Eom, J.S.; Lee, J.H.; Suh, G.Y.; Kwon, O.J.; Koh, W.J. Clinical characteristics and treatment outcomes of chronic pulmonary aspergillosis. Med. Mycol. 2013, 51, 811–817. [Google Scholar] [CrossRef]
- Hillerdal, G. Pulmonary aspergillus infection invading the pleura. Thorax 1981, 36, 745–751. [Google Scholar] [CrossRef] [Green Version]
- Tokuishi, K.; Yamashita, S.; Hashimoto, T.; Moroga, T.; Miyawaki, M.; Chujo, M.; Yamamoto, S.; Kawahara, K.; Tokimatsu, I.; Kashima, K. Bronchial stump aspergillosis after stapled lobectomy for lung cancer. Ann. Thorac. Surg. 2012, 94, 1324–1326. [Google Scholar] [CrossRef] [PubMed]
- Ohba, H.; Miwa, S.; Shirai, M.; Kanai, M.; Eifuku, T.; Suda, T.; Hayakawa, H.; Chida, K. Clinical characteristics and prognosis of chronic pulmonary aspergillosis. Respir. Med. 2012, 106, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Jhun, B.W.; Jung, W.J.; Hwang, N.Y.; Park, H.Y.; Jeon, K.; Kang, E.S.; Koh, W.J. Risk factors for the development of chronic pulmonary aspergillosis in patients with nontuberculous mycobacterial lung disease. PLoS ONE 2017, 12, e0188716. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Li, M.; Jiang, M.; Zou, L.Q.; Luo, F.; Jiang, Y. Clinical characteristics of 45 patients with invasive pulmonary aspergillosis: Retrospective analysis of 1711 lung cancer cases. Cancer 2009, 115, 5018–5025. [Google Scholar] [CrossRef]
- Hiraki, T.; Gobara, H.; Mimura, H.; Sano, Y.; Takigawa, N.; Tanaka, T.; Kanazawa, S. Aspergilloma in a cavity formed after percutaneous radiofrequency ablation for lung cancer. J. Vasc. Interv. Radiol. 2009, 20, 1499–1500. [Google Scholar] [CrossRef]
- Tanaka, H.; Matsumura, A.; Ohta, M.; Ikeda, N.; Kitahara, N.; Iuchi, K. Late sequelae of lobectomy for primary lung cancer: Fibrobullous changes in ipsilateral residual lobes. Eur. J. Cardiothorac. Surg. 2007, 32, 859–862. [Google Scholar] [CrossRef] [Green Version]
- Bach, P.B.; Cramer, L.D.; Schrag, D.; Downey, R.J.; Gelfand, S.E.; Begg, C.B. The influence of hospital volume on survival after resection for lung cancer. N. Engl. J. Med. 2001, 345, 181–188. [Google Scholar] [CrossRef]
- Al-Shair, K.; Muldoon, E.G.; Morris, J.; Atherton, G.T.; Kosmidis, C.; Denning, D.W. Characterisation of fatigue and its substantial impact on health status in a large cohort of patients with chronic pulmonary aspergillosis (CPA). Respir. Med. 2016, 114, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Vijayvergia, N.; Shah, P.C.; Denlinger, C.S. Survivorship in Non-Small Cell Lung Cancer: Challenges Faced and Steps Forward. J. Natl. Compr. Canc. Netw. 2015, 13, 1151–1161. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Total (n = 3423) | CPA (−) (n = 3367) | CPA (+) (n = 56) | p-Value | CPA Incidence (%) |
|---|---|---|---|---|---|
| Age, years | 63 (56–69) | 63 (56–69) | 63 (54–69) | 0.789 | - |
| Sex, male | 2178 (63.6) | 2131 (63.3) | 47 (83.9) | 0.001 | 47/2178 (2.2) |
| Smoking status | <0.001 | ||||
| Never smoker | 1343 (39.2) | 1334 (39.6) | 9 (16.1) | 9/1343 (0.7) | |
| Ex-smoker | 1060 (31.0) | 1035 (30.7) | 25 (44.6) | 25/1060 (2.4) | |
| Current smoker | 1020 (29.8) | 998 (29.6) | 22 (39.3) | 22/1020 (2.2) | |
| Pack-years (n = 2080) | 35 (20–50) | 35 (20–50) | 40 (30–60) | 0.059 | - |
| BMI, kg/m2 | 23.8 (21.8–25.7) | 23.8 (21.9–25.7) | 22.1 (20.5–23.5) | <0.001 | - |
| Comorbidity | |||||
| Underlying pulmonary disease | |||||
| History of pulmonary TB | 385 (11.2) | 376 (11.2) | 9 (16.1) | 0.249 | 9/385 (2.3) |
| COPD/Asthma | 1158 (33.8) | 1140 (33.9) | 18 (32.1) | 0.788 | 18/1158 (1.6) |
| Interstitial lung disease | 44 (1.3) | 42 (1.2) | 2 (3.6) | 0.161 | 2/44 (4.5) |
| DM | 560 (16.4) | 550 (16.3) | 10 (17.9) | 0.760 | 10/560 (1.8) |
| Chronic heart disease | 213 (6.2) | 209 (6.2) | 4 (7.1) | 0.777 | 4/213 (1.9) |
| Chronic renal disease | 31 (0.9) | 31 (0.9) | 0 (0.0) | 1.000 | 0/31 (0.0) |
| Cerebrovascular disease | 144 (4.2) | 143 (4.2) | 1 (1.8) | 0.731 | 1/144 (0.7) |
| Previous history of malignancy | 479 (14.0) | 470 (14.0) | 9 (16.1) | 0.651 | 9/479 (1.9) |
| Clinical stage at diagnosis | <0.001 | ||||
| Stage I | 2254 (65.8) | 2236 (66.4) | 18 (32.1) | 18/2254 (0.8) | |
| Stage II | 611 (17.8) | 601 (17.8) | 10 (17.9) | 10/611 (1.6) | |
| Stage III | 514 (15.0) | 487 (14.5) | 27 (48.2) | 27/514 (5.3) | |
| Stage IV | 44 (1.3) | 43 (1.3) | 1 (1.8) | 1/44 (2.3) | |
| Tumor histology | 0.007 | ||||
| Adenocarcinoma | 2317 (67.7) | 2290 (68.0) | 27 (48.2) | 27/2317 (1.2) | |
| Squamous cell carcinoma | 866 (25.3) | 843 (25.0) | 23 (41.1) | 23/866 (2.7) | |
| Others* | 240 (7.0) | 234 (6.9) | 6 (10.7) | 6/240 (2.5) | |
| Location of lung cancer | 0.213 | ||||
| Right | 1990 (58.1) | 1962 (58.3) | 28 (50.0) | 28/1990 (1.4) | |
| Left | 1433 (41.9) | 1405 (41.7) | 28 (50.0) | 28/1433 (2.0) |
| Variables | Total (n = 3423) | CPA (−) (n = 3367) | CPA (+) (n = 56) | p-Value | CPA Incidence (%) |
|---|---|---|---|---|---|
| Neoadjuvant treatment | <0.001 | ||||
| No | 3067 (89.6) | 3032 (90.1) | 35 (62.5) | 35/3067 (1.1) | |
| Yes | 356 (10.4) | 335 (9.9) | 21 (37.5) | 21/356 (5.9) | |
| CCRT | 299 (8.7) | 279 (8.3) | 20 (35.7) | <0.001 | 20/299 (6.7) |
| Chemotherapy | 54 (1.6) | 53 (1.6) | 1 (1.8) | 0.593 | 1/54 (1.9) |
| Radiotherapy | 3 (0.1) | 3 (0.1) | 0 (0.0) | 1.000 | 0/3 (0.0) |
| Surgical approach | <0.001 | ||||
| VATS | 2033 (59.4) | 2027 (60.2) | 6 (10.7) | 6/2033 (0.3) | |
| Thoracotomy | 1390 (40.6) | 1340 (39.8) | 50 (89.3) | 50/1390 (3.6) | |
| Types of surgical resection | 0.287 | ||||
| Sublobar resection | 492 (14.4) | 488 (14.5) | 4 (7.1) | 4/492 (0.8) | |
| Wedge resection | 349 (10.2) | 346 (10.3) | 3 (5.4) | 0.228 | 3/349 (0.9) |
| Segmentectomy | 143 (4.2) | 142 (4.2) | 1 (1.8) | 0.730 | 1/143 (0.7) |
| Lobectomy | 2637 (77.0) | 2591 (77.0) | 46 (82.1) | 46/2637 (1.7) | |
| Bilobectomy | 153 (4.5) | 148 (4.4) | 5 (8.9) | 5/153 (3.3) | |
| Pneumonectomy | 141 (4.1) | 140 (4.2) | 1 (1.8) | 1/141 (0.7) | |
| Pathologic stage (n = 3389*) | 0.006 | ||||
| I | 2094 (61.8) | 2073 (62.1) | 21 (40.4) | 21/2094 (1.0) | |
| II | 661 (19.5) | 648 (19.4) | 13 (25.0) | 13/661 (2.0) | |
| III | 591 (17.4) | 574 (17.2) | 17 (32.7) | 17/591 (2.9) | |
| IV | 43 (1.3) | 42 (1.3) | 1 (1.9) | 1/43 (2.3) | |
| Postoperative pulmonary complication | |||||
| Early phase (within 30 days) | 636 (18.6)† | 617 (18.3) | 19 (33.9) | 0.003 | 19/636 (3.0) |
| Late phase (after 30 days) | 94 (2.7)‡ | 82 (2.4) | 12 (21.4) | <0.001 | 12/94 (12.8) |
| Adjuvant treatment (n = 3401§) | 0.016 | ||||
| No | 2380 (70.0) | 2349 (70.2) | 31 (55.4) | 31/2380 (1.3) | |
| Yes | 1021 (30.0) | 996 (29.8) | 25 (44.6) | 25/1021 (2.4) | |
| CCRT | 191 (5.6) | 185 (5.5) | 6 (10.7) | 0.128 | 6/191 (3.1) |
| Chemotherapy | 616 (18.1) | 608 (18.2) | 8 (14.3) | 0.466 | 8/616 (1.3) |
| Radiotherapy | 213 (6.3) | 202 (6.0) | 11 (19.6) | 0.001 | 11/213 (5.2) |
| Variables | Univariable Cox Regression | Multivariable Cox Regression | ||
|---|---|---|---|---|
| Unadjusted HR (95% CI) | p-Value | Adjusted HR (95% CI) | p-Value | |
| Host-related factors | ||||
| Age, years | 1.01 (0.98–1.04) | 0.524 | ||
| Sex, male | 3.73 (1.83–7.62) | <0.001 | ||
| Body mass index, kg/m2 | 0.82 (0.74–0.90) | <0.001 | 0.83 (0.76–0.91) | <0.001 |
| Smoking history | ||||
| No | Reference | Reference | ||
| Yes | 4.25 (2.08–8.67) | <0.001 | 2.42 (1.16–5.07) | 0.019 |
| Comorbidity | ||||
| Previous history of pulmonary tuberculosis | 1.56 (0.76–3.17) | 0.225 | ||
| COPD/Asthma | 0.95 (0.54–1.66) | 0.854 | ||
| Interstitial lung disease | 5.99 (1.45–24.71) | 0.013 | 5.80 (1.35–25.00) | 0.018 |
| Diabetes mellitus | 1.30 (0.66–2.57) | 0.456 | ||
| Previous history of malignancy | 1.19 (0.59–2.43) | 0.627 | 1.98 (0.94–4.19) | 0.073 |
| Cancer-related factors | ||||
| Tumor histology | ||||
| Adenocarcinoma | Reference | |||
| Squamous cell carcinoma | 3.10 (1.77–5.42) | <0.001 | ||
| Others* | 2.95 (1.22–7.15) | 0.017 | ||
| Treatment-related factors | ||||
| Surgical approach | ||||
| VATS | Reference | Reference | ||
| Thoracotomy | 16.69 (7.15–38.96) | <0.001 | 9.60 (3.86–23.85) | <0.001 |
| Types of Surgical resection | ||||
| Lobectomy | Reference | |||
| Sublobar resection | 0.45 (0.16–1.24) | 0.123 | ||
| Bilobectomy | 2.22 (0.88–5.60) | 0.090 | ||
| Pneumonectomy | 0.65 (0.09–4.68) | 0.664 | ||
| Postoperative pulmonary complication | ||||
| Early phase (within 30 days) † | 2.69 (1.54–4.67) | <0.001 | ||
| Late phase (after 30 days) ‡ | 14.60 (7.70–27.69) | <0.001 | 6.75 (3.49–13.04) | <0.001 |
| Neoadjuvant or Adjuvant treatment | ||||
| No | Reference | Reference | ||
| Chemotherapy only | 0.84 (0.32–2.20) | 0.723 | 0.43 (0.16–1.14) | 0.088 |
| Radiotherapy only | 4.31 (1.02–18.25) | 0.047 | 1.47 (0.34–6.37) | 0.604 |
| Chemotherapy and radiotherapy both | 5.93 (3.38–10.40) | <0.001 | 2.47 (1.33–4.58) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.H.; Kim, B.-G.; Kang, J.; Um, S.-W.; Kim, H.; Kim, H.K.; Kim, J.; Shim, Y.M.; Choi, Y.S.; Jeong, B.-H. Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery. J. Fungi 2020, 6, 271. https://doi.org/10.3390/jof6040271
Shin SH, Kim B-G, Kang J, Um S-W, Kim H, Kim HK, Kim J, Shim YM, Choi YS, Jeong B-H. Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery. Journal of Fungi. 2020; 6(4):271. https://doi.org/10.3390/jof6040271
Chicago/Turabian StyleShin, Sun Hye, Bo-Guen Kim, Jiyeon Kang, Sang-Won Um, Hojoong Kim, Hong Kwan Kim, Jhingook Kim, Young Mog Shim, Yong Soo Choi, and Byeong-Ho Jeong. 2020. "Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery" Journal of Fungi 6, no. 4: 271. https://doi.org/10.3390/jof6040271
APA StyleShin, S. H., Kim, B. -G., Kang, J., Um, S. -W., Kim, H., Kim, H. K., Kim, J., Shim, Y. M., Choi, Y. S., & Jeong, B. -H. (2020). Incidence and Risk Factors of Chronic Pulmonary Aspergillosis Development during Long-Term Follow-Up after Lung Cancer Surgery. Journal of Fungi, 6(4), 271. https://doi.org/10.3390/jof6040271