
Ocular Sporotrichosis


Abstract
:1. Introduction
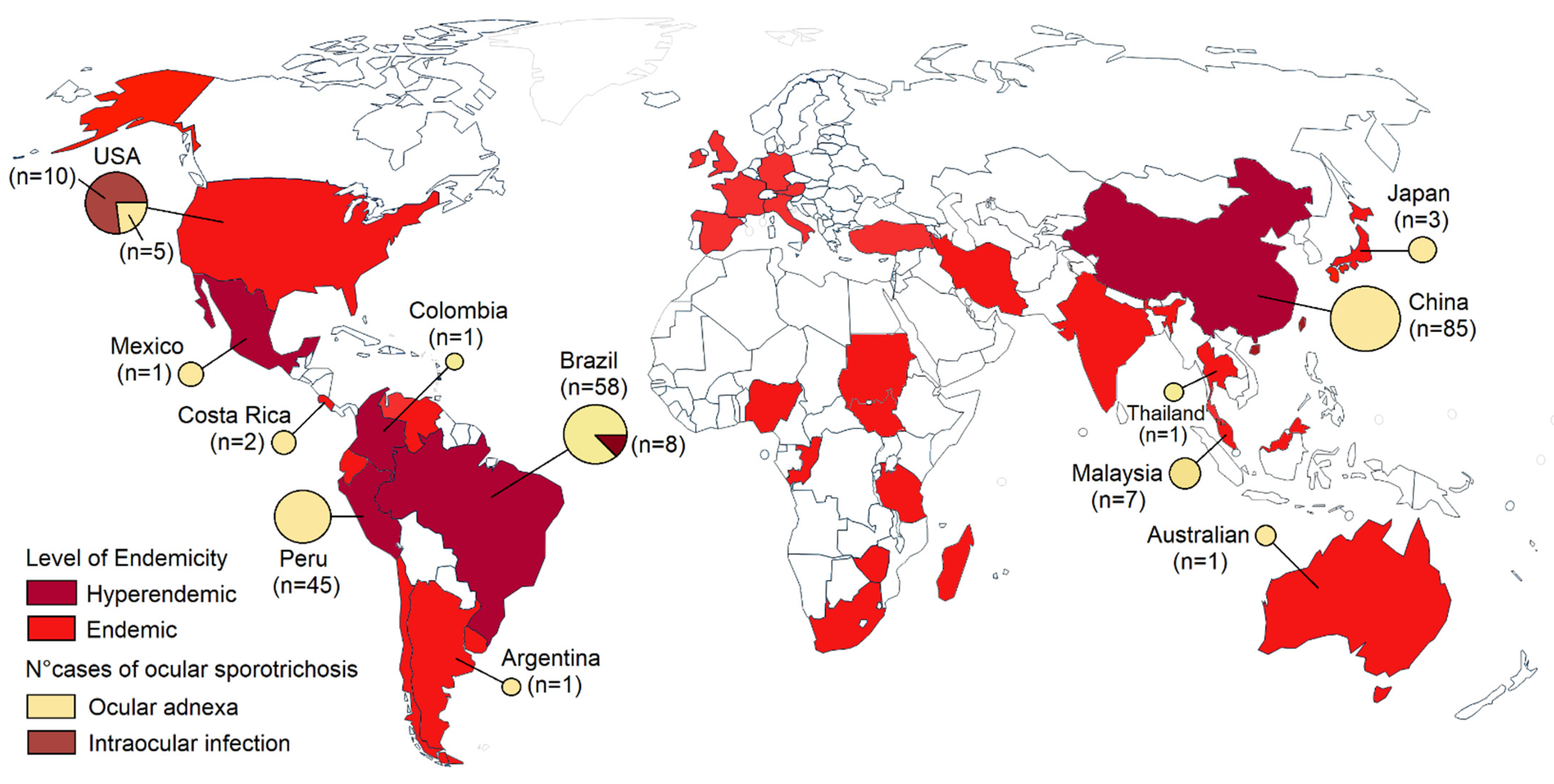
2. Epidemiology and Etiology
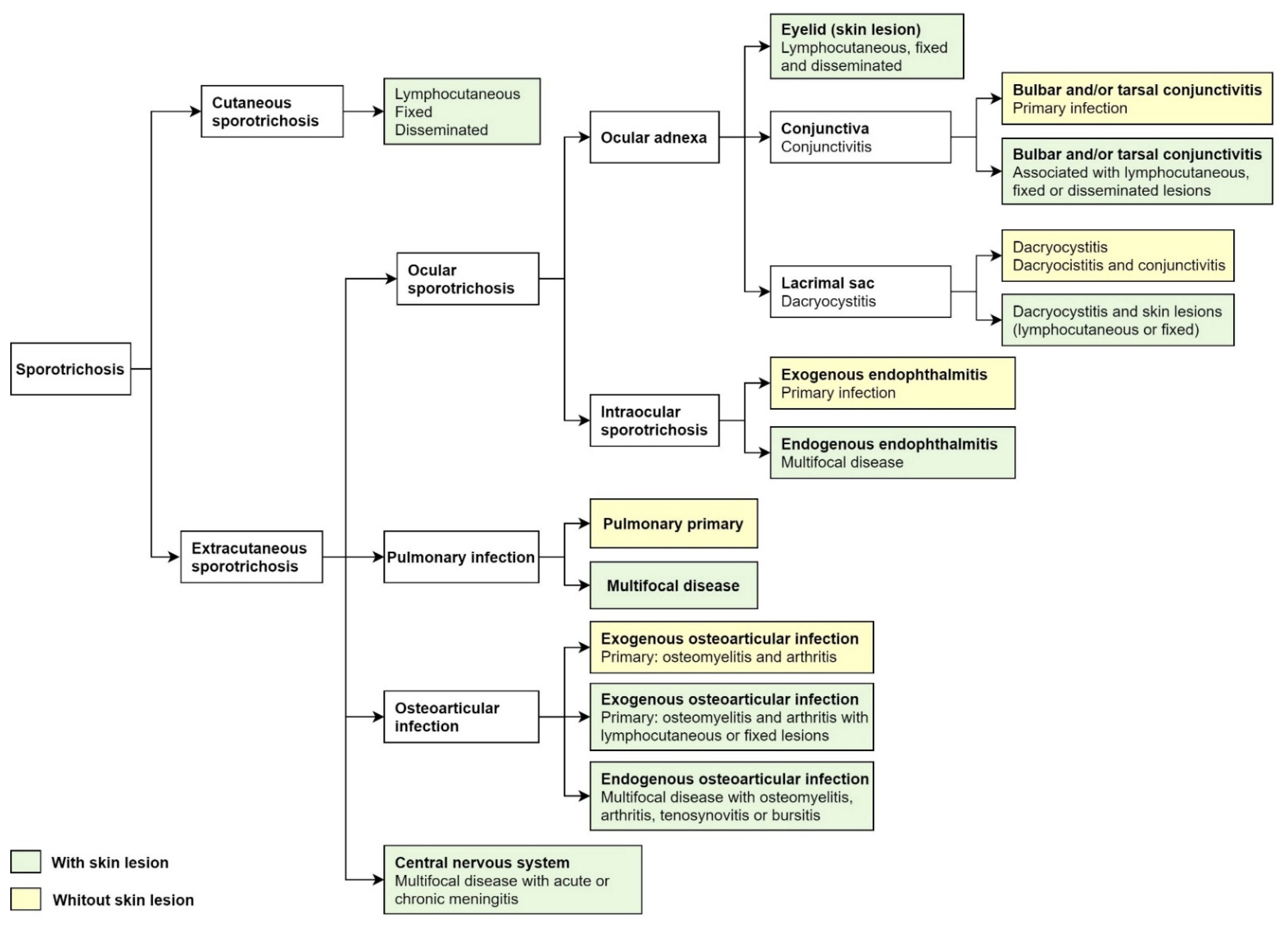
3. Clinical Presentation
3.1. Ocular Adnexa Sporotrichosis
3.1.1. Sporotrichosis Palpebral
3.1.2. Conjunctival Sporotrichosis
3.1.3. Dacryocystitis Due to Sporothrix
3.2. Intraocular Sporotrichosis
3.2.1. Exogenous Endophthalmitis
3.2.2. Endogenous Endophthalmitis
4. Differential Diagnoses
5. Laboratory Diagnosis
6. Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barros, M.B.D.L.; de Almeida Paes, R.; Schubach, A.O. Sporothrix schenckii and Sporotrichosis. Clin. Microbiol. Rev. 2011, 24, 633–654. [Google Scholar] [CrossRef] [Green Version]
- Chakrabarti, A.; Bonifaz, A.; Gutierrez-Galhardo, M.C.; Mochizuki, T.; Li, S. Global epidemiology of sporotrichosis. Med. Mycol. 2015, 53, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.M.; Della Terra, P.P.; Gremião, I.D.; Pereira, S.A.; Orofino-Costa, R.; de Camargo, Z.P. The threat of emerging and re-emerging pathogenic Sporothrix species. Mycopathologia 2020, 185, 813–842. [Google Scholar] [CrossRef]
- Queiroz-Telles, F.; Fahal, A.H.; Falci, D.R.; Caceres, D.H.; Chiller, T.; Pasqualotto, A.C. Neglected endemic mycoses. Lancet Infect. Dis. 2017, 17, 367–377. [Google Scholar] [CrossRef]
- Bonifaz, A.; Tirado-Sánchez, A. Cutaneous Disseminated and Extracutaneous Sporotrichosis: Current Status of a Complex Disease. J. Fungi 2017, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Orofino-Costa, R.; de Macedo, P.M.; Rodrigues, A.M.; Bernardes-Engemann, A.R. Sporotrichosis: An update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics. An. Bras. Dermatol. 2017, 92, 606–620. [Google Scholar] [CrossRef]
- Gutierrez-Galhardo, M.C.; Freitas, D.F.S.; Valle, A.C.F.D. Clinical Forms of Human Sporotrichosis and Host Immunocompetence. In Sporotrichosis; Springer: Berlin/Heidelberg, Germany, 2015; pp. 73–82. [Google Scholar]
- Soto, M.C.R. Sporotrichosis in the Ocular Adnexa: 21 Cases in an Endemic Area in Peru and Review of the Literature. Am. J. Ophthalmol. 2016, 162, 173–179.e3. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C. Differences in clinical ocular outcomes between exogenous and endogenous endophthalmitis caused by Sporothrix: A systematic review of published literature. Br. J. Ophthalmol. 2018, 102, 977–982. [Google Scholar] [CrossRef]
- Ramírez-Oliveros, J.F.; Casz Schechtman, R.; de Vries, H.J.; Lora, L.; Arinelli, A.C.; da Costa Nery, J.A.; Freitas, D.F.S. Ocular adnexal sporotrichosis: A case series. JAAD Case Rep. 2021, 13, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Y.; Cong, L.; Yang, H.; Cong, X. Eyelid sporotrichosis: Unique clinical findings in 72 patients. Australas. J. Dermatol. 2016, 57, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Arinelli, A.; Aleixo, A.L.Q.D.C.; Freitas, D.F.S.; Valle, A.C.F.D.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C.; Curi, A.L.L. Ocular Sporotrichosis: 26 Cases with Bulbar Involvement in a Hyperendemic Area of Zoonotic Transmission. Ocul. Immunol. Inflamm. 2020, 28, 764–771. [Google Scholar] [CrossRef]
- Gremião, I.D.F.; Oliveira, M.M.E.; De Miranda, L.H.M.; Freitas, D.F.S.; Pereira, S.A. Geographic Expansion of Sporotrichosis, Brazil. Emerg. Infect. Dis. 2020, 26, 621–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, L.; Song, Y.; Zhou, J.-F.; Cui, Y.; Li, S.-S. Epidemiological and clinical comparisons of paediatric and adult sporotrichosis in Jilin Province, China. Mycoses 2020, 63, 308–313. [Google Scholar] [CrossRef]
- Toriello, C.; Brunner-Mendoza, C.; Ruiz-Baca, E.; Duarte-Escalante, E.; Pérez-Mejía, A.; Del Rocío Reyes-Montes, M. Sporotrichosis in Mexico. Braz. J. Microbiol. 2021, 52, 49–62. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C. Sporotrichosis: The Story of an Endemic Region in Peru over 28 Years (1985 to 2012). PLoS ONE 2015, 10, e0127924. [Google Scholar] [CrossRef]
- Lopes-Bezerra, L.M.; Mora-Montes, H.M.; Zhang, Y.; Nino-Vega, G.; Rodrigues, A.M.; De Camargo, Z.P.; De Hoog, S. Sporotrichosis between 1898 and 2017: The evolution of knowledge on a changeable disease and on emerging etiological agents. Med. Mycol. 2018, 56, 126–143. [Google Scholar] [CrossRef] [PubMed]
- Gremião, I.D.F.; Miranda, L.H.M.; Reis, E.G.; Rodrigues, A.M.; Pereira, S.A. Zoonotic Epidemic of Sporotrichosis: Cat to Human Transmission. PLoS Pathog. 2017, 13, e1006077. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Troy, G.C. Deep mycotic infections in cats. J. Am. Anim. Hosp. Assoc. 1996, 32, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Sato, H.; Watanabe, S.; Takahashi, H.; Koide, K.; Hasegawa, A. Sporothrix schenckii isolated from a cat in Japan. Mycoses 1996, 39, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Soto, M.C.; Malaga, G. Subcutaneous mycoses in Peru: A systematic review and meta-analysis for the burden of disease. Int. J. Dermatol. 2017, 56, 1037–1045. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Aguilar-Ancori, E.G.; Tirado-Sánchez, A.; Bonifaz, A. Ecological Determinants of Sporotrichosis Etiological Agents. J. Fungi 2018, 4, 95. [Google Scholar] [CrossRef] [Green Version]
- Morrison, A.S.; Lockhart, S.R.; Bromley, J.G.; Kim, J.Y.; Burd, E.M. An environmental Sporothrix as a cause of corneal ulcer. Med Mycol. Case Rep. 2013, 2, 88–90. [Google Scholar] [CrossRef]
- Queiroz-Telles, F.; Buccheri, R.; Benard, G. Sporotrichosis In Immunocompromised Hosts. J. Fungi 2019, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Jordan, D.; Mawn, L.; Anderson, R.L. Surgical Anatomy of the Ocular Adnexa: A Clinical Approach; Oxford University Press: Melbourne, Australia, 2012. [Google Scholar]
- Filho, A.R.G.; Estacia, C.T.; Gameiro, R.R.; Vieira, L.D.M.F.; da Costa, D.S. Ocular and cutaneous sporotrichosis. Am. J. Ophthalmol. Case Rep. 2020, 20, 100885. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Liu, Y.; Yuan, N.; Zhang, X.; Cao, M.; Dong, J.; Zhang, J. Fixed Cutaneous Sporotrichosis Due to Sporothrix globosa. Clin. Cosmet. Investig. Dermatol. 2021, 14, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.; Wang, J.-F.; Zheng, B.; Qi, X.-Z.; Song, J.-Y.; Li, G.-Y. Clinical features of 10 cases of eyelid sporotrichosis in Jilin Province (Northeast China). Can. J. Ophthalmol. 2016, 51, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Miranda, H. Clinical profile and incidence of palpebral sporotrichosis: 16 new cases. Folia Dermatol. Peru. 2006, 17, 9–15. [Google Scholar]
- Carrada-Bravo, T. Facial sporotrichosis in childhood: Clinical and laboratory diagnosis, treatments and review. Bol. Med. Hosp. Infant. Mex. 2005, 62, 207–213. [Google Scholar]
- Solano, E. Sporotrichosis in children. Rev. Med. Costa Rica 1965, 22, 211–215. [Google Scholar] [PubMed]
- Inokuma, D.; Shibaki, A.; Shimizu, H. Two cases of cutaneous sporotrichosis in continental/microthermal climate zone: Global warming alert? Clin. Exp. Dermatol. 2010, 35, 668–669. [Google Scholar] [CrossRef] [PubMed]
- Fulgenzi, A.; Negroni, R.; Maiolo, E.; Arechavala, A.; Santiso, G.; Bianchi, M.H. Problemas clínicos en Micología Médica: Problema no 23 [Clinical cases in Medical Mycology. Case No. 23]. Rev. Iberoam. Micol. 2006, 23, 251–253. (In Spanish) [Google Scholar] [CrossRef]
- Ahmad-Fauzi, S.; Abd-Mana, N.; Yusof, N.S.; Ibrahim, M.; Mohamad, S.A.; Muhammed, J. Ocular sporotrichosis from a tertiary referral center in Malaysia and review of literature in Southeast Asia. Taiwan J. Ophthalmol. 2021. Available online: https://www.e-tjo.org/preprintarticle.asp?id=312511 (accessed on 1 November 2021).
- Wee, E.; Lin, M.J.; Gin, D. An ulcerated eyelid plaque with nodular lymphangitis. BMJ 2018, 361, k2147. [Google Scholar] [CrossRef]
- Soto, M.C.R.; Andagua-Castro, J.; Lizárraga-Trujillo, J. Palpebral sporotrichosis in a 6-year-old child. Int. J. Dermatol. 2016, 55, e625–e626. [Google Scholar] [CrossRef] [PubMed]
- Yamagata, J.P.M.; Rudolph, F.B.; Nobre, M.C.L.; Nascimento, L.V.; Sampaio, F.M.S.; Arinelli, A.; Freitas, D.F. Ocular Spo-rotrichosis: A frequently misdiagnosed cause of granulomatous conjunctivitis in epidemic areas. Am. J. Ophthalmol. Case Rep. 2017, 8, 35–38. [Google Scholar] [CrossRef]
- Medeiros, K.B.; Landeiro, L.G.; Diniz, L.M.; Falqueto, A. Disseminated cutaneous sporotrichosis associated with ocular le-sion in an immunocompetent patient. An. Bras. Dermatol. 2016, 91, 537–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hampton, D.E.; Adesina, A.; Chodosh, J. Conjunctival Sporotrichosis in the Absence of Antecedent Trauma. Cornea 2002, 21, 831–833. [Google Scholar] [CrossRef]
- Schubach, A.; de Lima Barros, M.B.; Schubach, T.M.; Francesconi-do-Valle, A.C.; Gutierrez-Galhardo, M.C.; Sued, M.; de Matos Salgueiro, M.; Fialho-Monteiro, P.C.; Reis, R.S.; Marzochi, K.B.; et al. Primary conjunctival sporotrichosis: Two cases from a zoonotic epidemic in Rio de Janeiro, Brazil. Cornea 2005, 24, 491–493. [Google Scholar] [CrossRef]
- Lee, H.Y.; Ramli, N.; Govindasamy, G.; Tham, J.H.; Goh, S.Y. Primary ocular sporotrichosis with granulomatous conjunctivitis. Eye Rep. 2020, 7, 14–17. [Google Scholar]
- Kashima, T.; Honma, R.; Kishi, S.; Hirato, J. Bulbar Conjunctival Sporotrichosis Presenting as a Salmon-Pink Tumor. Cornea 2010, 29, 573–576. [Google Scholar] [CrossRef]
- Ferreira, T.A.; Sodre, C.T.; Costa, J.M.; Setta, C.R.P.; Ramos-E-Silva, M. Primary conjunctival sporotrichosis: An atypical presentation of the disease. JAAD Case Rep. 2018, 4, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Reinprayoon, U.; Jermjutitham, M.; Tirakunwichcha, S.; Banlunara, W.; Tulvatana, W.; Chindamporn, A. Conjunctival sporotrichosis from cat to human: Case report. Am. J. Ophthalmol. Case Rep. 2020, 20, 100898. [Google Scholar] [CrossRef] [PubMed]
- Matos, A.M.F.; Moreira, L.; Barczewski, B.F.; de Matos, L.X.; de Oliveira, J.B.V.; Pimentel, M.I.F.; Almeida-Paes, R.; Oliveira, M.G.; Pinto, T.C.A.; Lima, N.; et al. Identification by MALDI-TOF MS of Sporothrix brasiliensis Isolated from a Subconjunctival Infiltrative Lesion in an Immunocompetent Patient. Microorganisms 2019, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Liborio Neto, A.O.; Rubim Caetano, T.; Pestana Gervasio, N.H.; Camargo Carneiro, R. Conjunctival and bulbar Sporotrichosis as Parinaud’s oculoglandular syndrome acquired by blood inoculation. GMS Ophthalmol. Cases 2021, 11, Doc02. [Google Scholar] [PubMed]
- Ribeiro, C.R.; Silva, B.P.; Almeida Costa, A.A.; Neto, A.B.; Vieira, L.A.; Lima, M.A.; Lima, M.H.C. Ocular Sporotrichosis. Am. J. Ophthalmol. Case Rep. 2020, 19, 100865. [Google Scholar] [CrossRef]
- Freitas, D.F.; de Siqueira Hoagland, B.; do Valle, A.C.; Fraga, B.B.; de Barros, M.B.; de Oliveira Schubach, A.; de Almeida-Paes, R.; Cuzzi, T.; Rosalino, C.M.; Zancopé-Oliveira, R.M.; et al. Sporotrichosis in HIV-infected patients: Report of 21 cases of endemic sporotrichosis in Rio de Janeiro, Brazil. Med. Mycol. 2012, 50, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Lemes, L.R.; Veasey, J.V.; Mayor, S.S.; Proença, C.C. Ocular involvement in sporotrichosis: Report of two cases in children. An. Bras. Dermatol. 2021, 96, 349–351. [Google Scholar] [CrossRef]
- Ling, J.L.L.; Koh, K.L.; Tai, E.; Sakinah, Z.; Nor Sharina, Y.; Hussein, A. A Case of Acute Granulomatous Conjunctivitis Caused by Cat-transmitted Sporothrix schenckii. Cureus 2018, 10, e3428. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, C.P.; Nery, J.A.; de Almeida, A.C.; Ferreira, L.C.; Corte-Real, S.; Conceição-Silva, F. Parinaud’s oculoglandular syndrome associated with Sporothrix schenckii. IDCases 2014, 1, 38–39. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.S.A.; Bisol, T.; Menezes, M.S. Parinaud’s oculoglandular syndrome caused by Sporotrichosis. Rev. Bras. Oftalmol. 2010, 69, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, R.; López-Villegas, A. Primary ocular sporotrichosis. Am. J. Ophthalmol. 1966, 62, 150–151. [Google Scholar] [CrossRef]
- Paiva, A.C.M.; Biancardi, A.L.; Curi, A.L.L. Different clinical manifestations of ocular sporotrichosis in the same patient: An alert to ophthalmologists in nonendemic areas. Arq. Bras. Oftalmol. 2020, 83, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Lacerda Filho, A.M.; Cavalcante, C.M.; Da Silva, A.B.; Inácio, C.P.; de Lima-Neto, R.G.; de Andrade, M.C.L.; Magalhães, O.M.C.; Dos Santos, F.A.G.; Neves, R.P. High-Virulence Cat-Transmitted Ocular Sporotrichosis. Mycopathologia 2019, 184, 547–549. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.; Lima, I.A.; Curi, C.L.; Jordão, L.; Zancopé-Oliveira, R.M.; Valle, A.C.; Galhardo, M.C.; Curi, A.L. Acute dacryocystitis: Another clinical manifestation of sporotrichosis. Memórias Inst. Oswaldo Cruz 2014, 109, 262–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Macedo, P.M.; Sztajnbok, D.C.; Camargo, Z.P.; Rodrigues, A.M.; Lopes-Bezerra, L.M.; Bernardes-Engemann, A.R.; Orofino-Costa, R. Dacryocystitis due to Sporothrix brasiliensis: A case report of a successful clinical and serological outcome with low-dose potassium iodide treatment and oculoplastic surgery. Br. J. Dermatol. 2015, 172, 1116–1119. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Dong, Y.; Wang, X.; Shan, B.; Zhang, M. Dacryocystitis due to Sporothrix inoculated vis an unusual mode: Case report. Medicine 2018, 97, e11182. [Google Scholar] [CrossRef] [PubMed]
- Brunette, I.; Stulting, R.D. Sporothrix schenckii scleritis. Am. J. Ophthalmol. 1992, 114, 370–371. [Google Scholar] [CrossRef]
- Witherspoon, C.D.; Kuhn, F.; Owens, S.D.; White, M.F.; Kimble, J.A. Endophthalmitis due to Sporothrix schenckii after penetrating ocular injury. Ann. Ophthalmol. 1990, 22, 385–388. [Google Scholar]
- Cassady, J.R.; Foerster, H.C. Sporotrichum schenckii endophthalmitis. Arch. Ophthalmol. 1971, 85, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.H. Intraocular sporotrichosis. Report of a case. Arch. Ophthalmol. 1971, 85, 574–579. [Google Scholar] [CrossRef]
- Cartwright, M.J.; Promersberger, M.; Stevens, G.A. Sporothrix schenckii endophthalmitis presenting as granulomatous uveitis. Br. J. Ophthalmol. 1993, 77, 61–62. [Google Scholar] [CrossRef] [Green Version]
- Agger, W.A.; Caplan, R.H.; Maki, D.G. Ocular sporotrichosis mimicking mucormycosis in a diabetic. Ann. Ophthalmol. 1978, 10, 767–771. [Google Scholar]
- Font, R.L.; Jakobiec, F.A. Granulomatous necrotizing retinochoroiditis caused by Sporotrichum schenkii. Report of a case including immunofluorescence and electron microscopical studies. Arch. Ophthalmol. 1976, 94, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, A.; Pollock, S.C.; Collins, M.P.; Kraff, C.R.; Tso, M.O. Sporothrix schenckii endophthalmitis in a patient with human immunodeficiency virus infection. Arch. Ophthalmol. 1988, 106, 376–380. [Google Scholar] [CrossRef]
- Silva-Vergara, M.L.; de Camargo, Z.P.; Silva, P.F.; Abdalla, M.R.; Sgarbieri, R.N.; Rodrigues, A.M.; dos Santos, K.C.; Barata, C.H.; Ferreira-Paim, K. Disseminated Sporothrix brasiliensis infection with endocardial and ocular involvement in an HIV-infected patient. Am. J. Trop. Med. Hyg. 2012, 86, 477–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biancardi, A.L.; Freitas, D.F.; Valviesse, V.R.; Andrade, H.B.; de Oliveira, M.M.; do Valle, A.C.; Zancope-Oliveira, R.M.; Galhardo, M.C.; Curi, A.L. Multifocal choroiditis in disseminated sporotrichosis in patients with HIV/AIDS. Retin. Cases Brief Rep. 2017, 11, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Vieira-Dias, D.; Sena, C.M.; Oréfice, F.; Tanure, M.A.; Hamdan, J.S. Ocular and concomitant cutaneous sporotrichosis. Mycoses 1997, 40, 197–201. [Google Scholar] [CrossRef]
- Curi, A.L.; Félix, S.; Azevedo, K.M.; Estrela, R.; Villar, E.G.; Saraça, G. Retinal granuloma caused by Sporothrix schenckii. Am. J. Ophthalmol. 2003, 136, 205–207. [Google Scholar] [CrossRef]
- Castro, R.M.; de Sabogal, M.F.; Cuce, L.C.; Salebian, A. Disseminate sporotrichosis-report of a clinical case with mucocutaneous, osteo-articular, and ocular lesions. Mykosen 1981, 24, 92–96. [Google Scholar] [CrossRef]
- Hassan, K.; Turker, T.; Zangeneh, T. Disseminated Sporotrichosis in an immunocompetent patient. Case Rep. Plast. Surg. Hand Surg. 2016, 3, 44–47. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.F.; Fernandes, S.R.; Samara, A.M. Sporothrix schenckii infection mimicking sarcoidosis. Rheumatology 2004, 43, 248–249. [Google Scholar] [CrossRef] [Green Version]
- Zambrano, A.I.; Church, E.C.; McKay, K.M.; Carnes, S.K.; Morse, R.J.; Leveque, T.K.; Roxby, A.C. A Disfiguring Rash. Open Forum Infect. Dis. 2021, 8, ofab332. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Bezerra, L.M.; Mora-Montes, H.M.; Bonifaz, A. Sporothrix and Sporotrichosis. In Current Progress in Medical Mycology; Springer: Berlin/Heidelberg, Germany, 2017; Chapter 9; pp. 309–331. [Google Scholar]
- Bonifaz, A.; Toriello, C.; Araiza, J.; Ramírez-Soto, M.C.; Tirado-Sánchez, A. Sporotrichin Skin Test for the Diagnosis of Sporotrichosis. J. Fungi 2018, 4, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, C.A.; Bustamante, B.; Chapman, S.W.; Pappas, P.G.; Infectious Diseases Society of America. Clinical practice guidelines for the management of Sporotrichosis: 2007 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 1255–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, K.; Zaitz, C.; Framil, V.M.; Muramatu, L.H. Cutaneous sporotrichosis treatment with potassium iodide: A 24-year experience in São Paulo State, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2011, 53, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Xue, S.; Gu, R.; Wu, T.; Zhang, M.; Wang, X. Oral potassium iodide for the treatment of sporotrichosis. Cochrane Database Syst. Rev. 2009, 7, CD006136. [Google Scholar]
- Macedo, P.M.; Lopes-Bezerra, L.M.; Bernardes-Engemann, A.R.; Orofino-Costa, R. New posology of potassium iodide for the treatment of cutaneous sporotrichosis: Study of efficacy and safety in 102 patients. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 719–724. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Bonifaz, A.; Tirado-Sánchez, A. Endophthalmitis in patients co-infected by HIV and Sporotrichosis: A systematic review of published case reports. Eye 2018, 32, 1678–1680. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Ocular Adnexal Sporotrichosis [8,11,12] | Intraocular Sporotrichosis [9] | |
|---|---|---|
| Epidemiology (most commonly found in) | Eyelid sporotrichosis in China and Peru Conjunctivitis and dacryocystitis in Brazil | The United States and Brazil |
| Age group | 2–89 years | 12–75 years |
| Occurs in children | Yes (frequent) | Yes (rare) |
| Clinical course | Less aggressive | Aggressive |
| Site of lesion | Eyelid, conjunctiva, and lacrimal sac | Scleral, cornea, retina, choroid, and optic nervous |
| Complications | Rare (cases of bulbar conjunctivitis) | Irreversible vision loss (endophthalmitis) |
| Risk factor | Traumatic inoculation with plant material and contact with cats | Traumatic inoculation with plant material, HIV infection, and residence in a hyperendemic area of sporotrichosis |
| Author [Ref.]/Year | Country | N° of Cases, Sex | Age | Risk Factor | Type Lesion | Clinical Manifestation | Isolated Species |
|---|---|---|---|---|---|---|---|
| Ramírez-Soto [8]/2016 | Peru, Brazil, Japan, Mexico, Costa Rica, and Argentina | 53 cases, male (54%)/female (46%) | 45 children (78%)/8 adults (22%) | Traumatic inoculation Contact with cats and sporotrichosis cats | Lymphocutaneous (52%) Fixed (32%) Disseminated (1.5%) | Lesions may be papular, nodular, ulcerative, or plaque-like or may show a combination of these features | Sporothrix schenckii Sporothrix spp. |
| Zhang et al. [11]/2016 | China | 72 cases, not specified | 43 children (60%)/22 adults (40%) | History of trauma with vegetal material and wood | Lymphocutaneous (57%) Fixed cutaneous (35%) Disseminated (8%) | Lesions may be granuloma annulare-like plaque, abscess, and cyst-like | S. schenckii |
| Fan et al. [28]/2016 | China | 10 cases, six females | 3–81 years (mean 46.5 years) | Not specified | Fixed cutaneous (6 cases) Lymphocutaneous (3 cases) Eyelid abscess (1 case) | Lesions in form nodular, ulcerative, plaque-like, cysts, verrucous lesions, or abscesses | S. schenckii |
| Ramirez-Oliveros et al. [10]/2021 | Brazil | Two females | Case 1, 7 years Case 2, 65 years | Sporotrichosis cat in one case | Fixed (2 cases) | One or multiple erythematous papules on the eyelid | Sporothrix spp. |
| Gameiro Filho et al. [26]/2020 | Brazil | Female | 13 years | Contact with cat | Lymphocutaneous | Eyelid granulomatous conjunctivitis lesion and conjunctivitis | S. brasiliensis |
| Liu et al. [27]/2021 | China | Male | 50 years | Not specified | Fixed | Small mass on the eyelid with rough keratinization | S. globosa |
| Ahmad-Fauzi et al. [34]/2021 | Malaysia | Female | 56 years | Exposure to cats | Fixed | Eyelid swelling and erythematous nodules with crusted skin | S. schenckii |
| Wee E [35]/2018 | Australian | Female | 22 years | Cat scratched her eyelid | Lymphocutaneous | Ulcerated right lower eyelid plaque | S. schenckii |
| Ramírez-Soto et al. [36]/2016 | Peru | Male | 6 years | Not specified | Lymphocutaneous | Ulcerated right lower eyelid plaque with nodule on the face | Sporothrix spp. |
| Author [Ref], Year | Age/Sex | Country | Clinical Form | Conjunctivitis | Eyelid/Parinaud | Isolated Species | Sequelae |
|---|---|---|---|---|---|---|---|
| Yamagata et al. [37], 2017 | 68/F | Brazil | Lymphocutaneous | Granulomatous conjuntivitis (right eye) involving the inferior tarsal and bulbar conjunctiva and conjuntival hyperemia | Parinaud | Sporothrix sp. | Fibrosis of the inferior tarsal and bulbar conjunctiva |
| 46/F | Brazil | Lymphocutaneous | Conjunctival hyperemia with infiltration (left eye) | Periocular edema/Parinaud | Sporothrix sp. | Symblefaron on the superior conjunctiva | |
| 14/M | Brazil | Lymphocutaneous | Granulomatous conjunctivitis affecting the lower tarsal conjunctiva (right eye) | Right eyelid edema/Parinaud | Sporothrix sp. | -- | |
| Madeiros et al. [38], 2016 | 59/F | Brazil | Disseminated | Pain and burning sensation on the left bulbar conjunctiva | Parinaud | Sporothrix spp. | |
| Hampton et al. [39], 2002 | 34/M | USA | Lymphocutaneous | 1cm diameter, elevated mobile mass without ulceration on the inferotemporal bulbar conjunctiva of the right eye without surrounding episcleral injection | Parinaud | HxPx suppurative granulomatous inflammation and tiny budding yeasts. Culture and electron microscopy (S. schenckii) | Asymptomatic and visually insignificant subepithelial corneal infiltrates developed |
| Schubach et al. [40], 2005 | 28/F | Brazil | Lymphocutaneous | Granulomatous hyperemic lesion covered with whitish secretion on the lower right conjunctiva, tarsus region | Parinaud | The isolates were on subcultivation | -- |
| 49/F | Brazil | Lymphocutaneous | 5 mm granulomatous lesion in the lateral region of the lower right conjunctiva. Conjunctival secretion of 10 days’ duration | Right palpebral edema/Parinaud | Conjunctival swab culture (S. schenckii) | ||
| Gameiro et al. [26], 2020 | 13/F | Brazil | Lymphocutaneous | Follicles in the lower tarsal conjunctiva with conjunctival hyperemia | Nodules in the nasal area of the upper and lower eyelid of the left eye. Lower eyelid swelling/Parinaud | Culture + S. brasiliensis | A small scar left the malar region and lower eyelid Margin of the left eye |
| Lee et al. [41], 2020 | 15/F | Malaysia | Cutaneous | Multiple nodules with central ulceration over the bulbar and forniceal conjunctiva. Generalized conjunctival injection of the left eye. Ulcerated granulomatous on the upper and lower tarsal conjunctiva | Periorbital edema | PCR + S schenckii | |
| Kashima et al. [42], 2010 | 62/F | Japan | Extracutaneous | Subconjunctival salmon-pink tumor and conjunctival injection around corneal limbus (left eye) | Palpebral edema | Histopathologically, epithelioid granuloma with microabscesses and infiltration of plasma cells with yeast-like spherules | |
| Ferreira et al. [43], 2018 | 78/F | Brazil | Extracutaneous | Infiltration of bulbar conjunctiva but without infiltration of the palpebral conjunctiva | Periorbital edema (left eye) | Culture (conjunctiva) Sporothrix spp. | |
| Reinprayoon et al. [44], 2020 | 42/F | Thailand | Cutaneous | A chronic, painless ulcerated lesion with a whitish plaque on the left lower tarsal conjunctiva after a keloid-like conjunctival lesion was excised one month ago | PCR (conjunctiva) S. schenckii. | ||
| Matos et al. [45], 2020 | 68/F | Brazil | Lymphocutaneous | A subconjunctival infiltrative lesion in the right eye, occupying the upper and lower fornix | Suppurative nodular lesions on lower right eyelid/Parinaud | S. brasiliensis. | Diffuse symblepharon after resolution of the acute phase, with restriction of ocular abduction |
| Liborio et al. [46], 2020 | 40/F | Brazil | Lymphocutaneous | Conjunctival granulomas in lower and upper tarsus | Granulomatous lesion on the lower eyelid left eye/Parinaud oculoglandular syndrome | ||
| Arinelli et al. [12], 2019 | 31.8 ± 23.4/F = 16 (76); M = 5 (24) | Brazil | NS | NS | Eyelids 4 (19); Parinaud 16 (76) | Sporothrix sp. | Symblefaron = 3 (14.3); conjuntival fibrosis = 2 (9.5) |
| Ribeiro et al. [47], 2020 | 69/F | Brazil | Cutaneous | Conjunctival hyperemia, follicles | Several granulomas in the upper and lower eyelid | Culture of the scrapings and conjunctival secretions + Sporothrix schenckii | |
| 13/F | Brazil | Lymphocutaneous | Conjunctival hyperemia, nodules in the inferior tarsal conjunctiva | Mild upper eyelid edema and granulomas in the lower and upper eyelid (right eye) | Culture of the scrapings and conjunctival secretions + Sporothrix schenckii | ||
| 22/M | Brazil | Lymphocutaneous | Granulomatous lesion near the caruncle, mucopurulent secretion and papillae in the tarsal conjunctiva, conjunctival hyperemia | Upper eyelid edema | Culture of the scrapings and conjunctival secretions + Sporothrix schenckii | ||
| 18/F | Brazil | Lymphocutaneous | Conjunctival hyperemia 1+/ 4 + serous secretion in the fornix | Mild upper eyelid edema in the right eye; several granulomas in the right lower eyelid, one granuloma in the nasal region of the right upper eyelid. Several granulomas in the temporal area of the right upper eyelid | Culture of the scrapings and conjunctival secretions Sporothrix schenckii | ||
| 21/F | Brazil | Extracutaneous | Conjunctival hyperemia (1+/4+), granulomas in the inferior tarsal conjunctiva of the left eye with serous secretion in the fornix | Culture of the scrapings and conjunctival secretions + Sporothrix schenckii | |||
| 15/M | Brazil | Lymphocutaneous | A granulomatous lesion in the inferior tarsal conjunctiva, and papillae in the tarsal, conjunctiva with serous secretion in the fornix; conjunctival hyperemia | Culture of the scrapings and conjunctival secretions + Sporothrix schenckii | |||
| Freitas et al. [48], 2012 | 59/M | Brazil | Disseminated | Granulomatous conjunctivitis of the right eye | Skin exudate conjunctival swab | ||
| Lemes et al. [49], 2020 | 3/M | Brazil | Lymphocutaneous | Granulomatous erythematous lesion on the lower portion of the tarsal conjunctiva | Parinaud ocular syndrome | Culture + Sporothrix spp. | |
| 12/M | Brazil | Lymphocutaneous | Conjunctivitis on the left eye (sneezing by a sick cat) | Culture + Sporothrix spp. | |||
| Ling et al. [50], 2018 | 18/F | Malaysia | Lymphocutaneous | Granulomatous conjunctival lesion covered with thin whitish discharge | Several small nodular lesions on the left inferior palpebral conjunctiva | Culture (conjunctival fornix) + S. schenckii. | |
| Ferreira et al. [51], 2014 | 21/M | Brazil | Disseminated | A lesion in the lower tarsal conjunctiva | Parinaud’s oculoglandular syndrome | Culture of hand lesion, Sporothrix schenckii (+) | |
| Ribeiro et al. [52], 2010 | 34/F | Brazil | Lymphocutaneous | Nodules in inferior tarsal conjunctiva | Parinaud’s oculoglandular syndrome | Culture of hand lesion, Sporothrix schenckii (+) | |
| Alvarez and Lopez-Villegas [53], 1964 | 11/M | Colombia | Extracutaneous | Temporal bulbar conjunctiva | Temporal bulbar conjunctiva | Culture of hand lesion, Sporothrix schenckii (+) | |
| Ahmad et al. [34], 2021 | 36.5 ± 19.2/F = 4 (67); M = 2 (33) | Malaysia | NS | GC on palpebral conjunctiva | Right 3 (50), Left 3 (50). Eyelids 2 (33) | Culture + Sporothrix sp. | Symblefaron = 2 (33); skin scarring = 1 (16.6) |
| Paiva et al. [54], 2020 | 25/F | Brazil | Lymphocutaneous | Upper eyelid edema and nodular lesions, GC, and fistulizing dacryocystitis | Palpebral nodules. The left bulbar and lower tarsal conjunctiva | Culture + Sporothrix sp. | Persistent fistula |
| Lacerda et al. [55], 2019 | 25/M | Brazil | Lymphocutaneous | Acute redness with conjunctival granulomatous lesions | Left tarsal conjunctiva | PCR (conjunctiva) S. brasiliensis. |
| Tarsal Conjunctiva [26,34,37,40,44,47,49,50,51,52] | Bulbar Conjunctiva [38,39,43,53] | |
|---|---|---|
| Age group | 3–69 years | 11–78 years |
| Gender | Female (63%) | Male:Female 1:1 |
| Occurs in children | Yes (frequent) 36.8% | Yes (rare) 25% |
| Clinical course | Less aggressive | More aggressive |
| Type of lesion (most typical) | Lymphocutaneous or fixed | Lymphocutaneous, fixed, or disseminated |
| Primary ocular infection | Frequent: tarsal/bulbar conjunctivitis Rare: tarsal conjunctivitis alone | Rare: bulbar conjunctivitis alone |
| Complications | 36.8% of cases | 25% of cases |
| Treatment duration with itraconazole (months) | 100 mg = 9.5; 200 mg = 5.5; 400 mg = 5.5 | 100 mg =1; 200 mg = 2; 300 mg = 6; potassium iodide = 3 |
| Cure (%) | 79 | 75 |
| Exogenous Endophthalmitis | Endogenous Endophthalmitis | |
|---|---|---|
| Epidemiology | United States | Brazil and the United State |
| Pathogen | S. schenckii | S. schenckii and S. brasiliensis |
| Risk factor | Traumatic inoculation | HIV-infection and residence in a hyperendemic area |
| Age group | 13–75 years | 12–56 years |
| Occurs in children | Infrequent | Infrequent |
| Disease duration at diagnosis | 123.6 days | 76.5 days |
| Ocular manifestation | Scleritis, anterior and posterior uveitis | Anterior and posterior uveitis, panuveitis, choroiditis, choroidoretinitis, and retinitis |
| Clinical course | Aggressive | Aggressive |
| Complications | Blindness and irreversible vision loss | Blindness and irreversible vision loss |
| Type of Disease, Agent | Ocular Adnexal Sporotrichosis | Intraocular Sporotrichosis |
|---|---|---|
| Fungal infection |
|
|
| Bacterial infection |
|
|
| Viral infection |
|
|
| Non-infectious |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Soto, M.C.; Tirado-Sánchez, A.; Bonifaz, A. Ocular Sporotrichosis. J. Fungi 2021, 7, 951. https://doi.org/10.3390/jof7110951
Ramírez-Soto MC, Tirado-Sánchez A, Bonifaz A. Ocular Sporotrichosis. Journal of Fungi. 2021; 7(11):951. https://doi.org/10.3390/jof7110951
Chicago/Turabian StyleRamírez-Soto, Max Carlos, Andrés Tirado-Sánchez, and Alexandro Bonifaz. 2021. "Ocular Sporotrichosis" Journal of Fungi 7, no. 11: 951. https://doi.org/10.3390/jof7110951
APA StyleRamírez-Soto, M. C., Tirado-Sánchez, A., & Bonifaz, A. (2021). Ocular Sporotrichosis. Journal of Fungi, 7(11), 951. https://doi.org/10.3390/jof7110951