
Strategies for the Prevention of Invasive Fungal Infections after Lung Transplant

Abstract
:1. Epidemiology
2. Risk Factors
3. Diagnosis
4. Prevention Strategies
4.1. Definitions of Prophylaxis Strategies
4.2. Current Practice and Recommendations
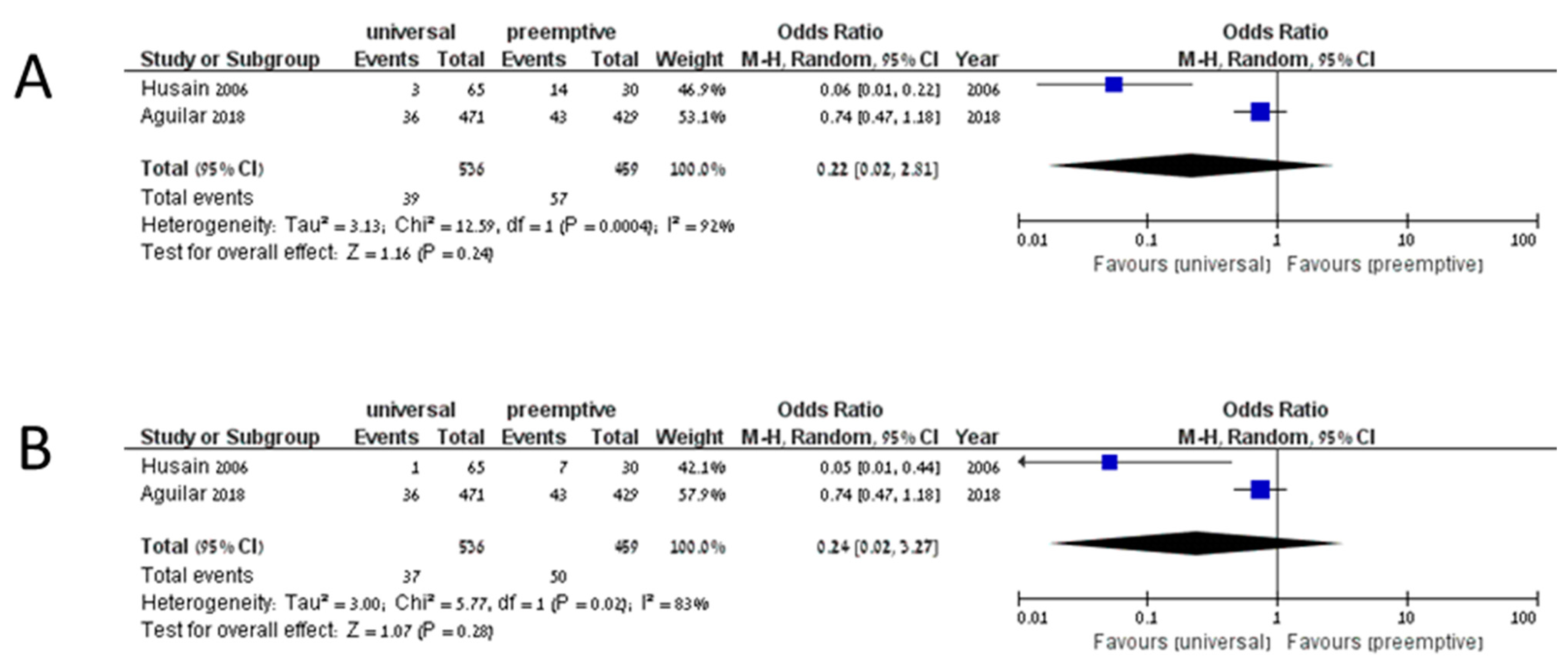
4.3. Current Data on Prevention Strategies
4.4. Choice of Drug
4.5. Duration
4.6. Toxicity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Health Resources and Services Administration. 2018 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1990–2018; Department of Health and Human Services, Health Resources and Services Administration, Healthcare: Rockville, MD, USA, 2018. [Google Scholar]
- Iversen, M.; Burton, C.M.; Vand, S.; Skovfoged, L.; Carlsen, J.; Milman, N.; Andersen, C.B.; Rasmussen, M.; Tvede, M. Aspergillus infection in lung transplant patients: Incidence and prognosis. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 879–886. [Google Scholar] [CrossRef]
- Hosseini-Moghaddam, S.M.; Ouédraogo, A.; Naylor, K.L.; Bota, S.E.; Husain, S.; Nash, D.M.; Paterson, J.M. Incidence and outcomes of invasive fungal infection among solid organ transplant recipients: A population-based cohort study. Transpl. Infect. Dis. 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Doligalski, C.T.; Benedict, K.; Cleveland, A.A.; Park, B.; Derado, G.; Pappas, P.G.; Baddley, J.W.; Zaas, D.W.; Harris, M.T.; Alexander, B.D. Epidemiology of invasive mold infections in lung transplant recipients. Am. J. Transplant. 2014, 14, 1328–1333. [Google Scholar] [CrossRef]
- Herrera, S.; Davoudi, S.; Farooq, A.; Tikkanen, J.; Foroutan, F.; Kumar, D.; Humar, A.; Rotstein, C.; Singer, L.G.; Keshavjee, S.; et al. Late Onset Invasive Pulmonary Aspergillosis in Lung Transplant Recipients in the Setting of a Targeted Prophylaxis/Preemptive Antifungal Therapy Strategy. Transplantation 2020, 104, 2575–2581. [Google Scholar] [CrossRef]
- Arthurs, S.K.; Eid, A.J.; Deziel, P.J.; Marshall, W.F.; Cassivi, S.D.; Walker, R.C.; Razonable, R.R. The impact of invasive fungal diseases on survival after lung transplantation. Clin. Transplant. 2010, 24, 341–348. [Google Scholar] [CrossRef]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Lto, J.; et al. Invasive fungal infections among organ transplant recipients: Results of the transplant-associated infection surveillance network (Transnet). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.W.; Maziarz, E.K.; Arnold, C.J.; Johnson, M.D.; Workman, A.D.; Reynolds, J.M.; Perfect, J.R.; Alexander, B.D. Invasive Fungal Infection after Lung Transplantation: Epidemiology in the Setting of Antifungal Prophylaxis. Clin. Infect. Dis. 2020, 70, 30–39. [Google Scholar] [CrossRef]
- Van Delden, C.; Stampf, S.; Hirsch, H.H.; Manuel, O.; Meylan, P.; Cusini, A.; Hirzel, C.; Khanna, N.; Weisser, M.; Garzoni, C.; et al. Burden and Timeline of Infectious Diseases in the First Year After Solid Organ Transplantation in the Swiss Transplant Cohort Study. Clin. Infect. Dis. 2020, 71, e159–e169. [Google Scholar] [CrossRef] [Green Version]
- Koo, S.; Kubiak, D.W.; Issa, N.C.; Dietzek, A.; Boukedes, S.; Camp, P.C.; Goldberg, H.J.; Baden, L.R.; Fuhlbrigge, A.L.; Marty, F.M. A targeted peritransplant antifungal strategy for the prevention of invasive fungal disease after lung transplantation: A sequential cohort analysis. Transplantation 2012, 94, 281–286. [Google Scholar] [CrossRef]
- Silveira, F.P.; Kwak, E.J.; Paterson, D.L.; Pilewski, J.M.; McCurry, K.R.; Husain, S. Post-transplant Colonization with Non-Aspergillus Molds and Risk of Development of Invasive Fungal Disease in Lung Transplant Recipients. J. Hearth Lung Transplant. 2008, 27, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, R.; Vazquez-Guillamet, M.C.; Suarez, J.; Mooney, J.; Montoya, J.G.; Dhillon, G.S. Invasive mold infections in lung and heart-lung transplant recipients: Stanford University experience. Transpl. Infect. Dis. 2015, 17, 259–266. [Google Scholar] [CrossRef]
- Husain, S.; Paterson, D.L.; Studer, S.; Pilewski, J.; Crespo, M.; Zaldonis, D.; Shutt, K.; Pakstis, D.L.; Zeevi, A.; Johnson, B.; et al. Voriconazole prophylaxis in lung transplant recipients. Am. J. Transplant. 2006, 6, 3008–3016. [Google Scholar] [CrossRef]
- Husni, R.N.; Gordon, S.M.; Longworth, D.L.; Arroliga, A.; Stillwell, P.C.; Avery, R.K.; Maurer, J.R.; Mehta, A.; Kirby, T. Cytomegalovirus infection is a risk factor for invasive aspergillosis in lung transplant recipients. Clin. Infect. Dis. 1998, 26, 753–755. [Google Scholar] [CrossRef] [Green Version]
- Cahill, B.C.; Hibbs, J.R.; Savik, K.; Juni, B.A.; Dosland, B.M.; Edin-Stibbe, C.; Hertz, M.I. Aspergillus airway colonization and invasive disease after lung transplantation. Chest 1997, 112, 1160–1164. [Google Scholar] [CrossRef]
- Aguilar, C.A.; Hamandi, B.; Fegbeutel, C.; Silveira, F.P.; Verschuuren, E.A.; Ussetti, P.; Chin-Hong, P.V.; Sole, A.; Holmes-Liew, C.; Billaud, E.M.; et al. Clinical risk factors for invasive aspergillosis in lung transplant recipients: Results of an international cohort study. J. Hearth Lung Transplant. 2018, 37, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Gavalda, J.; Len, O.; San Juan, R.; Aguado, J.M.; Fortun, J.; Lumbreras, C.; Moreno, A.; Munoz, P.; Blanes, M.; Ramos, A.; et al. Risk factors for invasive aspergillosis in solid-organ transplant recipients: A case-control study. Clin. Infect. Dis. 2005, 41, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camargo, J.F.; Husain, S. Immune correlates of protection in human invasive aspergillosis. Clin. Infect. Dis. 2014, 59, 569–577. [Google Scholar] [CrossRef] [Green Version]
- Husain, S.; Sole, A.; Alexander, B.D.; Aslam, S.; Avery, R.; Benden, C.; Billaud, E.M.; Chambers, D.; Danziger-Isakov, L.; Fedson, S.; et al. The 2015 International Society for Heart and Lung Transplantation Guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: Executive summary. J. Hearth Lung Transplant. 2016, 35, 261–282. [Google Scholar] [CrossRef] [Green Version]
- Solé, A.; Morant, P.; Salavert, M.; Pemán, J.; Morales, P.; Pastor, A.; Lozano, C.; Vicente, R.; Ramos, F.; Blasco, E.; et al. Aspergillus infections in lung transplant recipients: Risk factors and outcome. Clin. Microbiol. Infect. 2005, 11, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luong, M.L.; Chaparro, C.; Stephenson, A.; Rotstein, C.; Singer, L.G.; Waters, V.; Azad, S.; Keshavjee, S.; Tullis, E.; Husain, S. Pretransplant aspergillus colonization of cystic fibrosis patients and the incidence of post-lung transplant invasive aspergillosis. Transplantation 2014, 97, 351–357. [Google Scholar] [CrossRef]
- Nunley, D.R.; Ohori, N.P.; Grgurich, W.F.; Iacono, A.T.; Williams, P.A.; Keenan, R.J.; Dauber, J.H. Pulmonary aspergillosis in cystic fibrosis lung transplant recipients. Chest 1998, 114, 1321–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmi, M.; Love, R.B.; Welter, D.; Cornwell, R.D.; Meyer, K.C. Aspergillus infection in lung transplant recipients with cystic fibrosis: Risk factors and outcomes comparison to other types of transplant recipients. Chest 2003, 123, 800–808. [Google Scholar] [CrossRef]
- Hoenigl, M.; Prattes, J.; Spiess, B.; Wagner, J.; Prueller, F.; Raggam, R.B.; Posch, V.; Duettmann, W.; Hoenigl, K.; Wölfler, A.; et al. Performance of galactomannan, beta-d-glucan, aspergillus lateral-flow device, conventional culture, and pcr tests with bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis. J. Clin. Microbiol. 2014, 52, 2039–2045. [Google Scholar] [CrossRef] [Green Version]
- Geltner, C.; Lass-Flörl, C. Invasive pulmonary Aspergillosis in organ transplants—Focus on lung transplants. Respir. Investig. 2016, 54, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Avni, T.; Levy, I.; Sprecher, H.; Yahav, D.; Leibovici, L.; Paul, M. Diagnostic accuracy of PCR alone compared to galactomannan in bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis: A systematic review. J. Clin. Microbiol. 2012, 50, 3652–3658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, C.D.; Fine, J.P.; Safdar, N. Diagnosis of invasive aspergillosis using a galactomannan assay: A meta-analysis. Clin. Infect. Dis. 2006, 42, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Husain, S.; Clancy, C.J.; Nguyen, M.H.; Swartzentruber, S.; Leather, H.; LeMonte, A.M.; Durkin, M.M.; Knox, K.S.; Hage, C.A.; Bentsen, C.; et al. Performance characteristics of the platelia Aspergillus enzyme immunoassay for detection of Aspergillus galactomannan antigen in bronchoalveolar lavage fluid. Clin. Vaccine Immunol. 2008, 15, 1760–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husain, S.; Paterson, D.L.; Studer, S.M.; Crespo, M.; Pilewski, J.; Durkin, M.; Wheat, J.L.; Johnson, B.; McLaughlin, L.; Bentsen, C.; et al. Aspergillus galactomannan antigen in the bronchoalveolar lavage fluid for the diagnosis of invasive aspergillosis in lung transplant recipients. Transplantation 2007, 83, 1330–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenks, J.D.; Prattes, J.; Frank, J.; Spiess, B.; Mehta, S.R.; Boch, T.; Buchheidt, D.; Hoenigl, M. Performance of the Bronchoalveolar Lavage Fluid Aspergillus Galactomannan Lateral Flow Assay With Cube Reader for Diagnosis of Invasive Pulmonary Aspergillosis: A Multicenter Cohort Study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Alexander, B.D.; Smith, P.B.; Davis, R.D.; Perfect, J.R.; Reller, L.B. The (1, 3)β-D-glucan test as an aid to early diagnosis of invasive fungal infections following lung transplantation. J. Clin. Microbiol. 2010, 48, 4083–4088. [Google Scholar] [CrossRef] [Green Version]
- Bhaskaran, A.; Kabbani, D.; Singer, L.G.; Prochnow, T.; Bhimji, A.; Rotstein, C.; Finkelman, M.A.; Keshavjee, S.; Husain, S. (1, 3) β-D-Glucan in bronchoalveolar lavage of lung transplant recipients for the diagnosis of invasive pulmonary aspergillosis. Med. Mycol. 2017, 55, 173–179. [Google Scholar] [CrossRef]
- Pennington, K.M.; Dykhoff, H.J.; Yao, X.; Sangaralingham, L.R.; Shah, N.D.; Peters, S.G.; Barreto, J.N.; Razonable, R.R.; Kennedy, C.C. The Impact of Antifungal Prophylaxis in Lung Transplant Recipients. Ann. Am. Thorac. Soc. 2020. [Google Scholar] [CrossRef]
- Neoh, C.F.; Snell, G.I.; Kotsimbos, T.; Levvey, B.; Morrissey, C.O.; Slavin, M.A.; Stewart, K.; Kong, D.C.M. Antifungal prophylaxis in lung transplantation-a world-wide survey. Am. J. Transplant. 2011, 11, 361–366. [Google Scholar] [CrossRef]
- He, S.Y.; Makhzoumi, Z.H.; Singer, J.P.; Chin-Hong, P.V.; Arron, S.T. Practice variation in Aspergillus prophylaxis and treatment among lung transplant centers: A national survey. Transpl. Infect. Dis. 2015, 17, 14–20. [Google Scholar] [CrossRef]
- Husain, S.; Zaldonis, D.; Kusne, S.; Kwak, E.J.; Paterson, D.L.; McCurry, K.R. Variation in antifungal prophylaxis strategies in lung transplantation. Transpl. Infect. Dis. 2006, 8, 213–218. [Google Scholar] [CrossRef]
- Samanta, P.; Clancy, C.J.; Marini, R.V.; Rivosecchi, R.M.; McCreary, E.K.; Shields, R.K.; Falcione, B.A.; Viehman, A.; Sacha, L.; Kwak, E.J.; et al. Isavuconazole Is as Effective as and Better Tolerated Than Voriconazole for Antifungal Prophylaxis in Lung Transplant Recipients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pennington, K.M.; Razonable, R.R.; Peters, S.; Scott, J.P.; Wylam, M.; Daly, R.C.; Kennedy, C.C. Why do lung transplant patients discontinue triazole prophylaxis? Transpl. Infect. Dis. 2019, 21. [Google Scholar] [CrossRef]
- Husain, S.; Camargo, J.F. Invasive Aspergillosis in solid-organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, S.M.; Drew, R.H.; Whitehouse, J.D.; Tapson, V.F.; Duane Davis, R.; McConnell, R.R.; Kanj, S.S.; Perfect, J.R. Safety of aerosolized amphotericin B lipid complex in lung transplant recipients. Transplantation 2001, 72, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Shitrit, D.; Ollech, J.E.; Ollech, A.; Bakal, I.; Saute, M.; Sahar, G.; Kramer, M.R. Itraconazole prophylaxis in lung transplant recipients receiving tacrolimus (FK 506): Efficacy and drug interaction. J. Hearth Lung Transplant. 2005, 24, 2148–2152. [Google Scholar] [CrossRef]
- Lowry, C.M.; Marty, F.M.; Vargas, S.O.; Lee, J.T.; Fiumara, K.; Deykin, A.; Baden, L.R. Safety of aerosolized liposomal versus deoxycholate amphotericin B formulations for prevention of invasive fungal infections following lung transplantation: A retrospective study. Transpl. Infect. Dis. 2007, 9, 121–125. [Google Scholar] [CrossRef]
- Borro, J.M.; Solé, A.; de la Torre, M.; Pastor, A.; Fernandez, R.; Saura, A.; Delgado, M.; Monte, E.; Gonzalez, D. Efficiency and Safety of Inhaled Amphotericin B Lipid Complex (Abelcet) in the Prophylaxis of Invasive Fungal Infections Following Lung Transplantation. Transplant. Proc. 2008, 40, 3090–3093. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D., Jr.; Ball, A.M.; Mansour, H.M.; Martin, C.A.; Flynn, J.D. Fungal infection in heart-lung transplant recipients receiving single-agent prophylaxis with itraconazole. Exp. Clin. Transplant. 2011, 9, 399–404. [Google Scholar]
- Mitsani, D.; Nguyen, M.H.; Shields, R.K.; Toyoda, Y.; Kwak, E.J.; Silveira, F.P.; Pilewski, J.M.; Crespo, M.M.; Bermudez, C.; Bhama, J.K.; et al. Prospective, observational study of voriconazole therapeutic drug monitoring among lung transplant recipients receiving prophylaxis: Factors impacting levels of and associations between serum troughs, efficacy, and toxicity. Antimicrob. Agents Chemother. 2012, 56, 2371–2377. [Google Scholar] [CrossRef] [Green Version]
- Kato, K.; Nagao, M.; Nakano, S.; Yunoki, T.; Hotta, G.; Yamamoto, M.; Matsumura, Y.; Ito, Y.; Takakura, S.; Chen, F.; et al. Itraconazole prophylaxis for invasive Aspergillus infection in lung transplantation. Transpl. Infect. Dis. 2014, 16, 340–343. [Google Scholar] [CrossRef] [Green Version]
- Chong, P.P.; Kennedy, C.C.; Hathcock, M.A.; Kremers, W.K.; Razonable, R.R. Epidemiology of invasive fungal infections in lung transplant recipients on long-term azole antifungal prophylaxis. Clin. Transplant. 2015, 29, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Peghin, M.; Monforte, V.; Martin-Gomez, M.T.; Ruiz-Camps, I.; Berastegui, C.; Saez, B.; Riera, J.; Ussetti, P.; Solé, J.; Gavaldá, J.; et al. 10 years of prophylaxis with nebulized liposomal amphotericin B and the changing epidemiology of Aspergillus spp. infection in lung transplantation. Transpl. Int. 2016, 29, 51–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stelzer, D.; Weber, A.; Ihle, F.; Matthes, S.; Ceelen, F.; Zimmermann, G.; Kneidinger, N.; Schramm, R.; Winter, H.; Zoller, M.; et al. Posaconazole liquid vs tablet formulation in lung transplant recipients. Mycoses 2018, 61, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Lemström, K.; Suojaranta-Ylinen, R.; Martelius, T.; Harjula, A.; Sipponen, J.; Halme, M.; Piilonen, A.; Salmenkivi, K.; Anttila, V.J.; et al. Control of early aspergillus mortality after lung transplantation: Outcome and risk factors. Transplant. Proc. 2010, 42, 4459–4464. [Google Scholar] [CrossRef]
- Neoh, C.F.; Snell, G.I.; Levvey, B.; Kotsimbos, T.; Morrissey, C.O.; Slavin, M.A.; Stewart, K.; Kong, D.C.M. Preemptive treatment with voriconazole in lung transplant recipients. Transpl. Infect. Dis. 2013, 15, 344–353. [Google Scholar] [CrossRef]
- Hamacher, J.; Spiliopoulos, A.; Kurt, A.M.; Nicod, L.P. Pre-emptive therapy with azoles in lung transplant patients. Eur. Respir. J. 1999, 13, 180–186. [Google Scholar] [CrossRef]
- Pinney, M.F.; Rosenberg, A.F.; Hampp, C.; Schain, D.; Akindipe, O.; Baz, M. Invasive fungal infections in lung transplant recipients not receiving routine systemic antifungal prophylaxis: 12-Year experience at a University Lung Transplant Center. Pharmacotherapy 2011, 31, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Calvo, V.; Borro, J.M.; Morales, P.; Morcillo, A.; Viccnte, R.; Tarrazona, V. Antifungal prophylaxis during the early postoperative period of lung transplantation. Chest 1999, 115, 1301–1304. [Google Scholar] [CrossRef] [PubMed]
- Monforte, V.; Roman, A.; Gavalda, J.; Bravo, C.; Tenorio, L.; Ferrer, A.; Maestre, J.; Morell, F. Nebulized amphotericin B prophylaxis for Aspergillus infection in lung transplantation: Study of risk factors. J. Hearth Lung Transplant. 2001, 20, 1274–1281. [Google Scholar] [CrossRef]
- Minari, A.; Husni, R.; Avery, R.K.; Longworth, D.L.; DeCamp, M.; Bertin, M.; Schilz, R.; Smedira, N.; Haug, M.T.; Mehta, A.; et al. The incidence of invasive aspergillosis among solid organ transplant recipients and implications for prophylaxis in lung transplants. Transpl. Infect. Dis. 2002, 4, 195–200. [Google Scholar] [CrossRef]
- Tofte, N.; Jensen, C.; Tvede, M.; Andersen, C.B.; Carlsen, J.; Iversen, M. Use of prophylactic voriconazole for three months after lung transplantation does not reduce infection with Aspergillus: A retrospective study of 147 patients. Scand. J. Infect. Dis. 2012, 44, 835–841. [Google Scholar] [CrossRef]
- Mattner, F.; Chaberny, I.F.; Weissbrodt, H.; Fischer, S.; Gastmeier, P.; Haubitz, B.; Gottlieb, J.; Mattner, L.; Strueber, M. Surveillance invasiver Fadenpilzmykosen in lungentransplantierten Patienten: Effekt antimykotischer Prophylaxe mit Itraconazol und Voriconazol. Surveillance of invasive mold infections in lung transplant recipients: Effect of antimycotic prophylaxis with itraconazole and voriconazole. Mycoses 2005, 48, 51–55. [Google Scholar] [CrossRef]
- Drew, R.H.; Ashley, E.D.; Benjamin, D.K.; Davis, R.D.; Palmer, S.M.; Perfect, J.R. Comparative safety of amphotericin B lipid complex and amphotericin B deoxycholate as aerosolized antifungal prophylaxis in lung-transplant recipients. Transplantation 2004, 77, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Cadena, J.; Levine, D.J.; Angel, L.F.; Maxwell, P.R.; Brady, R.; Sanchez, J.F.; Michalek, J.E.; Levine, S.M.; Restrepo, M.I. Antifungal prophylaxis with voriconazole or itraconazole in lung transplant recipients: Hepatotoxicity and effectiveness. Am. J. Transplant. 2009, 9, 2085–2091. [Google Scholar] [CrossRef] [PubMed]
- Monforte, V.; Ussetti, P.; Gavaldà, J.; Bravo, C.; Laporta, R.; Len, O.; García-Gallo, C.L.; Tenorio, L.; Solé, J.; Román, A. Feasibility, tolerability, and outcomes of nebulized liposomal amphotericin B for Aspergillus infection prevention in lung transplantation. J. Hearth Lung Transplant. 2010, 29, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Pennington, K.M.; Baqir, M.; Erwin, P.J.; Razonable, R.R.; Murad, M.H.; Kennedy, C.C. Antifungal prophylaxis in lung transplant recipients: A systematic review and meta-analysis. Transpl. Infect. Dis. 2020, 22. [Google Scholar] [CrossRef]
- Bhaskaran, A.; Mumtaz, K.; Husain, S. Anti-aspergillus prophylaxis in lung transplantation: A systematic review and meta-analysis. Curr. Infect. Dis. Rep. 2013, 15, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Pilarczyk, K.; Haake, N.; Heckmann, J.; Carstens, H.; Haneya, A.; Cremer, J.; Jakob, H.; Pizanis, N.; Kamler, M. Is universal antifungal prophylaxis mandatory in adults after lung transplantation? A review and meta-analysis of observational studies. Clin. Transplant. 2016, 30, 1522–1531. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Years | N | Strategy | Antifungal | Duration of Prophylaxis, m | Duration of Follow-up, m | IFD | IA | Colonization (Aspergillus/mold) | Mortality |
|---|---|---|---|---|---|---|---|---|---|---|
| Non-comparative studies | ||||||||||
| Hamacher 1999 | 1993–1997 | 31 | Preemptive + targeted ^ | Itraconazole | 4.2, mean | 19.4, mean | 3 (9.6%) | 2 (6.4%) | 8 (25.8%) | |
| Palmer 2001 | 1997–1998 | 51 | Universal | nABLC | 2 | 12 ~ | 6 | 0 | ||
| Shitrit 2005 | 1994–2004 | 40 | Universal | Itraconazole | 6 | 12 | 2 (5%) | 2 (5%) | 11 (27.5%) | |
| Lowry 2007 | 2002–2004 | 38 | Universal | nAmBd/nLAmB | 0.25, median | NS | 1 (2.6%) | 1 (2.6%) | 0 | |
| Borro 2008 | 2005–2007 | 60 | Universal | nABLC + fluconazole | nABLC-3m fluconazole-3w | 6 | 0 | 0 | 1 (0.15%) | |
| Eriksson 2010 | 2002–2010 | 76 | Universal + targeted # | Universal-nAmBd/nABLB Targeted-caspofungin | Universal-till anastomosis heals Targeted-not specified | 31.2, median | 3 (3.9%) | 3 (3.9%) | 12 (15.7%) | 11 (14.5%) |
| Hayes 2011 | 2001–2005 | 41 | Universal | Itraconazole | 12, median | Varied, at least 12 | 8 (19.5%) | 6 (14.6%) | 32% @ 3y | |
| Pinney 2011 | 1994–2006 | 242 | None | 34, median | 22 (9%) | 11 (4.5%) | 44% @ 3y | |||
| Mitsani 2012 | 2009 | 93 | Universal | Voriconazole | At least 3 | NS | 10 (10.7%) | 1 (1%) | 6 (6.4%) | |
| Neoh 2013 | NS | 62 | Preemptive | Voriconazole | 3, median | 12 | 1 (1.6%) | 1 (1.6%) | 16 (25.8%) | |
| Kato 2014 | 2008–2012 | 30 | Universal | Itraconazole ~ | Variable, at least 12 | 60 ~ | 5 (16.6%) | 5 (16.6%) | ||
| Chong 2015 | 2002–2011 | 91 | Universal | Voriconazole/itraconazole @ | At least 12 (most lifelong) | Variable, at least 12 | 15 (16.5%) | 10 (10.9%) | 27 (29.6%) | 15.3% @ 1y 49.4% @ 3y |
| Peghin 2016 | 2003–2013 | 412 | Universal | nLAmB | Lifelong | 30.7, mean | 22 (5.3%) | 22 (5.3%) | 61 (14.8%) | |
| Stelzer 2018 | 2014–2016 | 9 | Universal | Posaconazole | At least 6 | 15, median | 0 | 0 | 2 (22.2%) | |
| Baker 2020 | 2007–2014 | 815 | Targeted * | Universal-nABLC Targeted-mold-active azole/micafungin/nABLC | Universal-till discharge Targeted-variable | 3 | 156 (19.1%) | 42 (5.1%) | ||
| Comparative studies | ||||||||||
| Calvo 1999 | 1990–1997 | 52 | Universal | nAmBd + fluconazole | Till discharge 1.4, mean | During hospitalization | 0 | 0 | ||
| 13 | None | 3 (23%) | NS | |||||||
| Monforte 2001 | 1990–1997 | 44 | Universal | nAmB | Lifelong | 14, mean | 10 (22.7%) | 10 (22.7%) | 12 (21.8%, combined) | 23 (41.8%, combined) |
| 11 | None | 8 (72.7%) | 8 (72.7%) | |||||||
| Minari 2002 | 1990–1999 | 81 | Universal | nAmBd + itraconazole | nAmBd-post-transplant itraconazole- lifelong? | variable | 4 (4.9%) | 4 | ||
| 88 | None | 16 (18.1%) | 16 | |||||||
| Drew 2004 RCT | 1999–2002 | 49 | Universal | nAmBd | 7w | 2 | 7 (14.2%) | 1 (2%) | ||
| 51 | Universal | nABLC | 7w | 6 (11.7) | 1 (2%) | |||||
| Matter 2005 | 2002–2003 | 18 | Targeted $ | Voriconazole | 6w | During hospitalization | 1 (5.6%) | 1 | ||
| 101 | Universal | Itraconazole | NS | 6 (5.9%) | 6 | |||||
| Husain 2006 | 2001–2004 | 65 | Universal | Voriconazole | ≥4 | 12 | 3 (4.6%) | 1 (1.5%) | 16 (24%) | 2 (3%) |
| 30 | Universal + preemptive & | Fluconazole-universal Itraconazole ± nAmBd- preemptive | 3–6 | 14 (46.6%) | 7 (23.3%) | 12 (40%) | 5 (16%) | |||
| Cadena 2009 | 2003–2006 | 32 | Universal | Itraconazole | ≥3 | 12 | 4 (12.5%) | 4 | 11(34.3%) | 4 (12.5%) |
| 35 | Universal | nAmBd + voriconazole | ≥3 (nAmBd-2w) | 1 (2.8%) | 0 | 9 (25.7%) | 7 (20%) | |||
| Monforte 2010 | 2000–2001 | 49 | Universal | nAmBd | Lifelong | 12 | 2 (4.1%) | 2 (4.1%) | 1 (2%) | |
| 2003–2005 | 104 | Universal | nLAmB | Lifelong | 2 (1.9%) | 2 (1.9%) | 5 (4.8%) | |||
| Koo 2012 | 2003–2010 | 82 | Universal | nAmBd/nLAmB | During hospitalization | 12 | 29 (35.3%) | 8 | 13 (16%) | |
| 83 | Universal + targeted % | nAmb + micafungin ± tailored antifungal | nAmB-during hospitalization micafungin- 10d tailored antifungal- 3–6 | 10 (12%) | 2 | 9 (11%) | ||||
| Tofte 2012 | 2002–2006 | 57 | Universal | Voriconazole | 3 | Up to 60 | 11 (19.2%) | 11 (19.2%) | 12 (21%) | 7% @ 1y 21% @ 3y |
| 82 | None | 8 (10%) | 8 (10%) | 23 (28%) | 29% @ 1y 43% @ 3y | |||||
| Aguilar 2018 | 2005–2008 | 471 | universal | Mostly nAmB or itraconazole | Variable | 48, median | 36 (7.6%) | 36 (7.6%) | ||
| 429 | Targeted/preemptive | Variable | Variable | 43 (10%) | 43 (10%) | |||||
| Samanta 2020 | 2013–2015 | 144 | Universal | Isavuconazole (+nAmB 100%) | 3.4, median | At least 12 | 10 (6.9%) | 3 (2%) | 19 (6%) | 14 (10%) |
| 156 | Universal | Voriconazole (+nAmB 41%) | 3.1, median | 13 (8.3%) | 7 (4.4%) | 5 (3%) | 18 (12%) | |||
| Pennington 2020 | 2002–2017 | 232 | Universal + targeted | Variable | Variable | 12 | 14.94% (adjusted) | 8.36% (adjusted) | ||
| 232 | none | 22.37% (adjusted) | 19.49% (adjusted) | |||||||
| Drug | Short-Term Toxicity | Long-Term Toxicity |
|---|---|---|
| Nebulized Amphotericin B | Respiratory-cough, shortness of breath, bronchospasm | Damage to surfactant causing deterioration in pulmonary function (suspected) |
| GI-nausea, vomiting | ||
| Azoles Itraconazole | AKI secondary to cyclodextrin in IV formulation (suspected) | Neurologic-peripheral neuropathy |
| DDI-CYP3A4 (inhibitor + substrate), Pgp (inhibitor) | ||
| GI-nausea, vomiting (most) | ||
| Hepatotoxicity | ||
| Prolongation of QT interval | ||
| Voriconazole | AKI secondary to cyclodextrin in IV formulation (suspected) | Periostitis |
| DDI-CYP2C19 (inhibitor + substrate), CYP3A4 (inhibitor + substrate) | Peripheral neuropathy | |
| Neurologic-visual disturbances, hallucinations | Alopecia | |
| GI-nausea, vomiting, diarrhea | Squamous cell carcinoma of the skin | |
| Hepatotoxicity (most) | ||
| Skin-rash, photosensitivity, perioral excoriations | ||
| Prolongation of QT interval | ||
| Posaconazole | AKI secondary to cyclodextrin in IV formulation (suspected) | Not reported |
| DDI-CYP3A4 (inhibitor) | ||
| GI-nausea, vomiting | ||
| Hepatotoxicity | ||
| Prolongation of QT interval | ||
| Isavuconazole | DDI-CYP3A4 (inhibitor + substrate) | Not reported |
| Hepatotoxicity | ||
| Shortening of QT interval |
| Pros | Cons | |
|---|---|---|
| Universal prophylaxis | Easy to implement | Increased antifungal consumption Drives resistance Increased toxicity Increased drug–drug interactions |
| Preemptive treatment | Lower antifungal drug consumption | Requires resources (surveillance bronchoscopies, short turnaround time for galactomannan results) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bitterman, R.; Marinelli, T.; Husain, S. Strategies for the Prevention of Invasive Fungal Infections after Lung Transplant. J. Fungi 2021, 7, 122. https://doi.org/10.3390/jof7020122
Bitterman R, Marinelli T, Husain S. Strategies for the Prevention of Invasive Fungal Infections after Lung Transplant. Journal of Fungi. 2021; 7(2):122. https://doi.org/10.3390/jof7020122
Chicago/Turabian StyleBitterman, Roni, Tina Marinelli, and Shahid Husain. 2021. "Strategies for the Prevention of Invasive Fungal Infections after Lung Transplant" Journal of Fungi 7, no. 2: 122. https://doi.org/10.3390/jof7020122
APA StyleBitterman, R., Marinelli, T., & Husain, S. (2021). Strategies for the Prevention of Invasive Fungal Infections after Lung Transplant. Journal of Fungi, 7(2), 122. https://doi.org/10.3390/jof7020122