
Epidemiologic Aspects of Mycetoma in Africa
Abstract
:1. Introduction
2. Etiological Mycetoma Agents in Africa
3. Agents of Mycetoma in the Environment
4. Influence of Climate and Environmental Factors in the African Endemic Zone for Mycetoma
5. Mode of Contamination
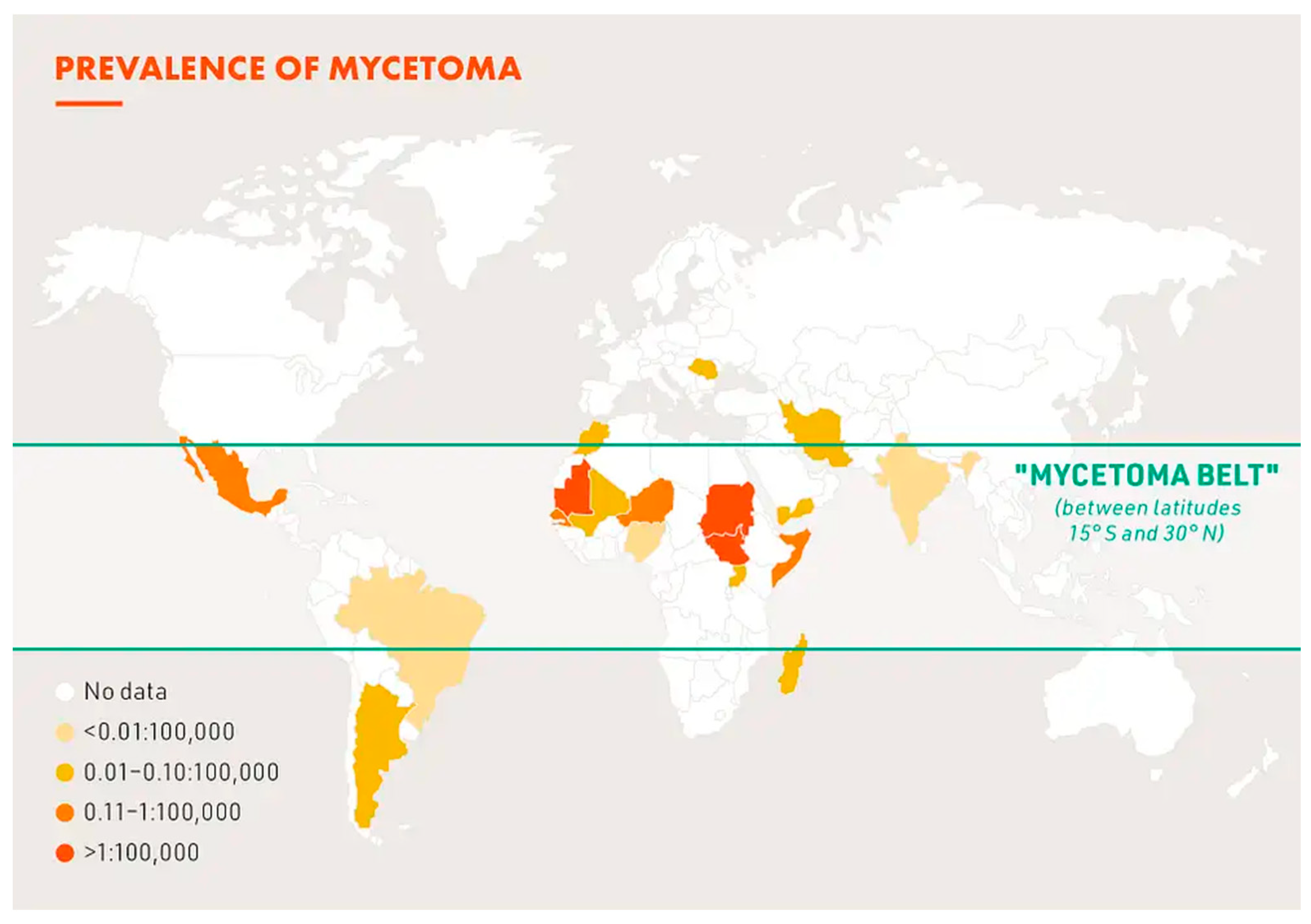
6. Geographical Distribution of Mycetoma in Africa
7. Prevalence and Incidence
8. Host of Mycetoma
9. Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Emery, D.; Denning, D.W. The global distribution of actinomycetoma and eumycetoma. PLoS Negl. Trop. Dis. 2020, 14, e0008397. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A.; Ali, Y.; Bakhert, S.M.; Mohamed, N.S.; Ahmed, E.S.; Fahal, A.H. Eumycetoma medical treatment: Past, current practice, latest advances and perspectives. Microbiol. Res. 2021, 12, 899–906. [Google Scholar] [CrossRef]
- van de Sande, W.; Fahal, A.; Ahmed, S.A.; Serrano, J.A.; Bonifaz, A.; Zijstra, E. Closing the mycetoma knowledge gap. Med. Mycol. 2018, 56, S153–S164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Sande, W.W.J. Global burden of human mycetoma: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2013, 7, e2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desnos-Ollivier, M.; Bretagne, S.; Dromer, F.; Lortholary, O. Molecular identification of black- grain mycetoma agents. J. Clin. Microbiol. 2006, 44, 3117–3523. [Google Scholar] [CrossRef] [Green Version]
- Siddig, E.E.; Verbon, A.; Bakhaert, S.; Fahal, H. The developed molecular identification tools for mycetoma causative agents: An update. Acta Trop. 2022, 225, 106205. [Google Scholar] [CrossRef] [PubMed]
- de Hoog, G.S.; van Diepeningen, A.D.; Maghoub, E.-S.; van de Sande, W.W. New species of Madurella, causative agents of black grain mycetoma. J. Clin. Microbiol. 2012, 50, 988–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, E.A.; Nour, B.Y.M.; Abakar, A.D.; Hamid, S.; Mohamadani, A.A.; Daffalla, M.; Mahmoud, M.; Altayb, H.N.; Desnos-Ollivier, M.; de Hoog, S.; et al. The genus Madurella: Molecular identification and epidemiology in Sudan. PLoS Negl. Trop. Dis. 2020, 14, e0008420. [Google Scholar] [CrossRef] [PubMed]
- Mhmoud, N.A.; Ahmed, S.A.; Fahal, A.H.; de Hoog, S.G.; Gerrits van den Ende, A.H.G.; van de Sande, W.W.J. Pleurostomophora ochracea, a novel agent of human mycetoma with yellow grains. J. Clin. Microbiol. 2012, 50, 2987–2994. [Google Scholar] [CrossRef] [Green Version]
- Bousquet, A.; Souraud, J.B.; Mérens, A.; Garcia-Hermoso, D.; Fougerousse, A.C. Photo quiz: A 25-year-old male with chronic firm mass of the foot. J. Clin. Microbiol. 2017, 55, 1977. [Google Scholar] [CrossRef]
- Mhmoud, N.A.; Santona, A.; Fiamma, M.; Siddig, E.E.; Deligios, M.; Beckhiet, S.M.; Rubino, S.; Fahal, A.H. Chaetimium atrobrunneum causing human mycetoma: The first report. PLoS Negl. Trop. Dis. 2019, 13, e0007276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mhoud, N.A.; Siddig, E.E.; Nyuykongi, B.; Bakhiet, S.M.; van de Sande, W.W.J.; Fahal, A.H. Mycetoma caused by Microascus gracilis: A novel agent of human eumycetoma in Sudan. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 426–430. [Google Scholar] [CrossRef]
- Quintana, E.T.; Wierzbicka, K.; Mackiewicz, P.; Osman, A.; Fahal, A.H.; Hamid, M.E.; Zakrzewska-Czerwinska, J.; Maldonado, L.A.; Goodfellow, M. Streptomyces sudanensis sp. nov; a new pathogen isolated from patients with actinomycetoma. Antonie Van Leeuvenhoek 2008, 93, 305–313. [Google Scholar] [CrossRef]
- Siddig, E.E.; Ahmed, H.T.; Hassan, R.; Saad, E.S.A.; Mhoud, N.A.; Bakhiet, S.M.; van de Sande, W.W.J.; Fahal, A.H. Human mycetoma caused by Actinomadura mexicana in Sudan: The first report. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Berot, V.; Ousser, A.F.; Sougakoff, W.; Lecso, G.; Monsel, G.; Caumes, E. A patient from Mali with Actinomadura bangladeshensis-induced foot mycetoma: A diagnostic challenge. Travel. Med. Infect. Dis. 2019, 31, 101452. [Google Scholar] [CrossRef] [PubMed]
- Segretain, G.; Mariat, F. Recherche sur la présence d’agents de mycétomes dans le sol et sur les épineux du Sénégal et de la Mauritanie. Bull. Soc. Path Exot. 1968, 61, 194–202. [Google Scholar] [PubMed]
- Ahmed, A.; Adelman, D.; Fahal, A.; Verbrugh, H.; van Belkum, A.; de Hoog, S. Environmental occurrence of Madurella mycetomatis, the major agent of eumycetoma in Sudan. J. Clin. Microbiol. 2002, 40, 1031–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashizume, H.; Taga, S.; Sakata, M.K.; Hussein, M.; Taha, M.; Siddig, E.E.; Minamoto, T.; Fahal, A.H.; Kaneko, S. Detection of multiple mycetoma pathogens using fungal metabarcoding analysis of soil DNA in an endemic area of Sudan. PLoS Negl. Trop. Dis. 2011, 16, e0010274. [Google Scholar] [CrossRef] [PubMed]
- de Hoog, G.S.; Ahmed, S.A.; Najafzadeh, M.J.; Sulton, D.A.; Keisari, M.S.; Fahal, A.H.; Eberhardt, U.; Verkley, G.J.; Xin, L.; Stielow, B.; et al. Phylogenetic findings suggest possible new habitat and routes of infection of human mycetoma. PLoS Negl. Trop. Dis. 2013, 7, e2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey, M.; Baylet, R.; Camain, R. Données actuelles sur les mycétomes. A propos de 214 cas africains. Ann. Dermatol. Syph 1962, 89, 511–527. [Google Scholar]
- Ndiaye, B.; Develoux, M.; Dieng, M.T.; Kane, A.; Ndir, O.; Raphenon, G.; Huerre, M. Actual presentation of mycetoma in Senegal. About 109 cases. J. Mycol. Med. 2000, 10, 140–144. [Google Scholar]
- Sow, D.; Ndiaye, M.; Sarr, L.; Kante, M.D.; Ly, F.; Dioussé, P.; Faye, B.T.; Gaye, A.M.; Sokhna, C.; Ranque, S.; et al. Mycetoma epidemiology, diagnosis management, and outcome in three hospital centers in Senegal from 2008 to 2018. PLoS ONE 2020, 15, e0231871. [Google Scholar] [CrossRef] [PubMed]
- Mahe, A.; Develoux, M.; Lienhardt, C.; Keita, S.; Bobin, P. Mycetoma in Mali: Causative agents and geographic distribution. Am. J. Trop. Med. Hyg. 1996, 54, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Develoux, M.; Audoin, J.; Treguer, J.; Vetter, J.M.; Warter, A.; Cenac, A. Mycetoma in the Republic of Niger: Clinical features and epidemiology. Am. J. Trop. Med. Hyg. 1988, 38, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Samy, A.M.; van de Sande, W.W.J.; Fahal, A.H.; Peterson, A.T. Mapping the potential risk of mycetoma infection in Sudan and South Sudan using ecological niche modeling. PLoS Negl. Trop. Dis. 2014, 8, e3250. [Google Scholar] [CrossRef] [Green Version]
- Hassan, R.; Simpson, H.; Cano, J.; Bakhiet, S.; Ganawa, E.; Argow, D.; Newport, M.J.; Deribe, K.; Fahal, A.H. Modelling the spatial distribution of mycetoma in Sudan. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Ganawa, E.T.S.; Bushara, M.A.; Musa, A.E.A.; Bakhiet, S.M.; Fahal, A.H. Mycetoma spatial geographical distribution in the Eastern Sennar locality, Sennar State, Sudan. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Cardenas-de la Garza, J.A.; Welsh, O.; Cuellar-Barboza, A.; Suarez-Sanchez, K.P.; Cruz-Gomez, L.G.; De la Cruz-Valadez, E.; Ocampo-Candiani, J.; Vera-Cabrera, L. Climate, soil type, and geographical distribution of actinomycetoma cases in Northeast Mexico: A cross-sectional study. PLoS ONE 2020, 15, e0232556. [Google Scholar] [CrossRef] [PubMed]
- Fahal, A.; Mahgoub, E.S.; El Hassan, A.M.; Abdel-Rahman, M.E. Mycetoma in the Sudan: An update from the mycetoma research center, University of Khartoum, Sudan. PLoS Trop. Negl. Dis. 2015, 9, e0003679. [Google Scholar] [CrossRef] [PubMed]
- Fahal, A.H.; Mahgoub, E.S.; El Hassan, A.M.; Abdel-Raham, M.E.; Aishambaty, Y.; Hashim, A.; Hago, A.; Zijlstra, E. A new model for management of mycetoma in the Sudan. PLoS Negl. Trop. Dis. 2014, 8, e3271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Sande, W.W.J.; Maghoub, E.S.; Fahal, A.H.; Goodfellow, M.; Welsh, O.; Zijlstra, E. The mycetoma knowledge gap: Identification of research priorities. PLoS Negl. Trop. Dis. 2014, 8, e2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azrag, R.S.; Bakhier, S.M.; Mhmoud, N.A.; Almalick, A.M.; Mohmaed, A.H.; Fahal, A.H. A possible role for ticks in the transmission of Madurella mycetomatis in a mycetoma-endemic village in Sudan. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.S.; Newport, M.J.; Bakhiet, S.M.; Ibrahim, M.E.; Fahal, A.H. Host genetic susceptibility to mycetoma. PLoS Negl. Trop. Dis. 2020, 14, e0008053. [Google Scholar] [CrossRef] [PubMed]
- Kébé, M.; Ba, O.; Abderahmane, M.A.M.; Baba, N.D.M.; Bell, M.; Fahal, A. A study of 87 mycetoma patients seen at three health facilities in Nouakchott, Mauritania. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 315–319. [Google Scholar] [CrossRef]
- Traore, T.; Toure, L.; Diassara, M.; Niang, M.; Ballo, E.S.; Coulibaly, B.; Hans-Moevi, A. Medico-surgical treatment in the Somine Dolo hospital of Mopti (Mali). Med. Trop. Santé 2021, 1, mtsi.2021.170. [Google Scholar]
- Oladele, R.O.; Ly, F.; Sow, D.; Akinkugbe, A.O.; Ocansey, B.K.; Fahal, A.H.; van de Sande, W.W.J. Mycetoma in West Africa. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 328–336. [Google Scholar] [CrossRef]
- Destombes, P.; Ravisse, P.; Nazimoff, O. Bilan des mycoses profondes établi en vingt années d’histopathologie à l’institut Pasteur de Brazzaville. Bull. Soc. Pathol. Exot. 1970, 63, 315–324. [Google Scholar]
- de L’Escalopier, N.; Choufani, C.; Grosset, A.; de Lesquen, H.; Murison, J.C.; Bertani, A.; Mathieu, L. Traitement chirurgical des mycétomes au Tchad: Expérience de l’antenne médico-chirurgicale françase déployée à N’Djamena. Med. Santé Trop. 2019, 29, 164–169. [Google Scholar]
- Destombes, P.; Du Tour, J.; Marquet, J.; Mariat, F.; Segretain, G. les mycétomes en Côte française des Somalis. Bull. Soc. Pathol. Exot. 1958, 51, 575–581. [Google Scholar]
- Destombes, P.; Mariat, F.; Rosati, L.; Segretain, G. Les mycétomes en Somalie, conclusions d’une enquête menée de 1959 to 1964. Act. Trop. 1977, 34, 355–373. [Google Scholar]
- Abate, D.A.; Ayele, M.H.; Mohammed, A.B. Subcutaneous mycoses in Ethiopia: A retrospective study in a single dermatologic center. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1468–1470. [Google Scholar] [CrossRef] [PubMed]
- Tilahun Zewdu, F.; Getahun Abdela, S.; Takarinda, K.C.; Kamau, E.M.; Van Griensven, J.; Van Hentsen, S. Mycetoma patients in Ethiopia: Case series from Boru Meda Hospital. J. Infect. Dev. Ctires 2022, 16, 41S–44S. [Google Scholar] [CrossRef] [PubMed]
- Schibli, A.; Goldenberger, D.; Krieg, A.; Hirschmann, A.; Bruder, E.; Osthoff, M. Painless swelling of the forefoot and recurrent subcutneous abcess of the lower leg. Two distinct presentations illustrating the spectrum of eumycetoma in a non-endemic country. PLoS Negl. Trop. Dis. 2017, 11, e0005360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasciana, T.; Coloba, C.; Cervo, A.; Di Carlo, P.; Scarlata, F.; Mascarella, C.; Giammanco, A.; Cascio, A. Madura foot: An imported case of a non-common diagnosis. Infez. Med. 2018, 26, 167–170. [Google Scholar] [PubMed]
- Cazzato, G.; Colagrande, A.; Cimmino, A.; Lospalutti, L.; Demarco, A.; Foti, C.; Romita, P.; Arrezzo, F.; Loizzi, V.; Parente, P.; et al. Skin mycetoma in a 11-year-old African boy: Case presentation with emphasis in histopathological features and differential diagnosis. Dermatopathology 2021, 8, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Bitan, O.; Wiener-Well, Y.; Segal, R.; Schwartz, E. Mycetoma (Madura foot) in Israel: Recent cases and systematic review of the literature. Am. J. Trop. Med. Hyg. 2017, 96, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Adoubrym, K.D.; Koffi, K.E.; Trah, E.; Doucoure, B.; Kouadio-Yapo, C.G.; Ouhon, J.; Assoumou, A.; Ferly-Therizol, F.; Diomande, M.I.J.; Honde, M.; et al. Native mycetoma of Côte d’ivoire epidemiological and etiological features of confirmed cases. J. Mycol. Med. 2009, 19, 71–76. [Google Scholar]
- Darre, T.; Bayiki, S.; Mouhari-Toure, A.; Tchaou, M.; Dorkeno, A.M.; Doh, K.; Walla, A.; Amegbor, K.; Pitché, V.P.; Napo-Koura, G. Mycetoma in the Togolese: An update from a single-center experience. Mycopathologia 2018, 183, 961–965. [Google Scholar] [CrossRef]
- Vanbreuseghem, R. Epidemiology and therapeutic of Madura foot in the Belgian Congo. Bull. Soc. Pathol. Exot. 1958, 51, 593–814. [Google Scholar]
- Kwizera, R.; Bongonim, F.; Meya, D.B.; Dening, D.W.; Fahal, A.H.; Lukande, R. Mycetoma in Uganda: A neglected tropical disease. PLoS Negl. Trop. Dis. 2020, 14, e0008240. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Boyles, T.H.; Kenyon, C.R.; Hoving, J.C.; Brown, G.D.; Denning, D.W. The estimated burden of fungal disease in South Africa. S. Afr. Med. J. 2019, 109, 885–889. [Google Scholar] [CrossRef] [Green Version]
- Coulanges, P.; Vicens, R.; Rakotonirina-Randriambeloma, P.J. Mycetoma in Madagascar (a propos of 142 cases seen in the laboratory of Anatomical Pathology of the Pasteur Institute of Madagascar from 1954 to 1984). Arch. Inst. Pasteur. Madagascar. 1987, 53, 37–42. [Google Scholar]
- Zait, H.; Madani, K.; Abed-Benamara, M.; Achir, I.; Hamrioui, B. Mycetoma in Algeria. About two new cases. Review of cases reported between 1995 and 2005. J. Mycol. Med. 2008, 18, 116–122. [Google Scholar] [CrossRef]
- Elgallali, N.; El Euch, D.; Cheikhrouhou, R.; Belhadj, S.; Chelly, I.; Chaker, E.; Ben Osman, A. Mycetoma in Tunisia: A 15 case-series. Med. Trop. 2010, 70, 269–273. [Google Scholar]
- Marc, S.; Meziane, M.; Hamada, S.; Hassam, B.; Benzekri, L. Clinical and epidemiological features of mycetoma in Morocco. Med. Mal. Infect. 2011, 41, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.A.; Deribe, K.; Fahal, A.H.; Newport, M.; Bakkhiet, S. A scoping review of the mycetoma profile in Egypt, revisiting the global endemicity map. Trans. R. Soc. Trop. Med. Hyg. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Hassan, R.; Deribe, K.; Fahal, A.H.; Newport, M.; Bakkhiet, S. Clinical, epidemiological characteristics of mycetoma in Eastern Sennar locality, Sennar State, Sudan. PLoS Negl. Trop. Dis. 2021, 15, e0009847. [Google Scholar] [CrossRef] [PubMed]
- van de Sande, W.W.J.; Fahal, A.H.; Tavako, M.; Van Belkum, A. Polymorphisms in catechol-O-methyltransferase and cytochrome p450 subfamily 19 genes predispose towards Madurella mycetomatis-induced mycetoma susceptibility. Med. Mycol. 2010, 48, 959–968. [Google Scholar] [CrossRef] [Green Version]
- Hassan, R.; Deribe, K.; Simpson, H.; Bremner, S.; Elhadi, O.; Alnour, M.; Fahal, A.H.; Neport, M.; Bakhiet, S. Individual risk factors of mycetoma occurrence in Eastern Sennar localities, Sennar State, Sudan: A case -controlled study. Trop. Med. Infect. Dis. 2022, 7, 174. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Eumycetoma | |
|---|---|
| Black grain | |
| Madurella fahalii | [5] |
| Madurella tropicana | [8] |
| Curvularia pseudolunata | [10] |
| Sphaerulina rhododendricola | [8] |
| Chaetomium atrobrunneum | [11] |
| White grain | |
| Microascus gracilis | [12] |
| Yellow grain | |
| Pleurostomophora ochracea | [9] |
| Actinomycetoma | |
| White or yellow grain | |
| Streptomyces sudanensis | [13] |
| Actinomadura bangladeshensis | [15] |
| Actinomadura mexicana | [14] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Develoux, M. Epidemiologic Aspects of Mycetoma in Africa. J. Fungi 2022, 8, 1258. https://doi.org/10.3390/jof8121258
Develoux M. Epidemiologic Aspects of Mycetoma in Africa. Journal of Fungi. 2022; 8(12):1258. https://doi.org/10.3390/jof8121258
Chicago/Turabian StyleDeveloux, Michel. 2022. "Epidemiologic Aspects of Mycetoma in Africa" Journal of Fungi 8, no. 12: 1258. https://doi.org/10.3390/jof8121258
APA StyleDeveloux, M. (2022). Epidemiologic Aspects of Mycetoma in Africa. Journal of Fungi, 8(12), 1258. https://doi.org/10.3390/jof8121258