
Emergence of Clonally-Related South Asian Clade I Clinical Isolates of Candida auris in a Greek COVID-19 Intensive Care Unit

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting, Definition of Cases, Demographic and Clinical Characteristics of C. auris Cases
2.2. Culture, Identification of the Isolates, Antimicrobial Susceptibility Testing and Environmental Screening
2.3. Sequencing and Phylogenetic Analysis of C. auris Isolates
3. Results
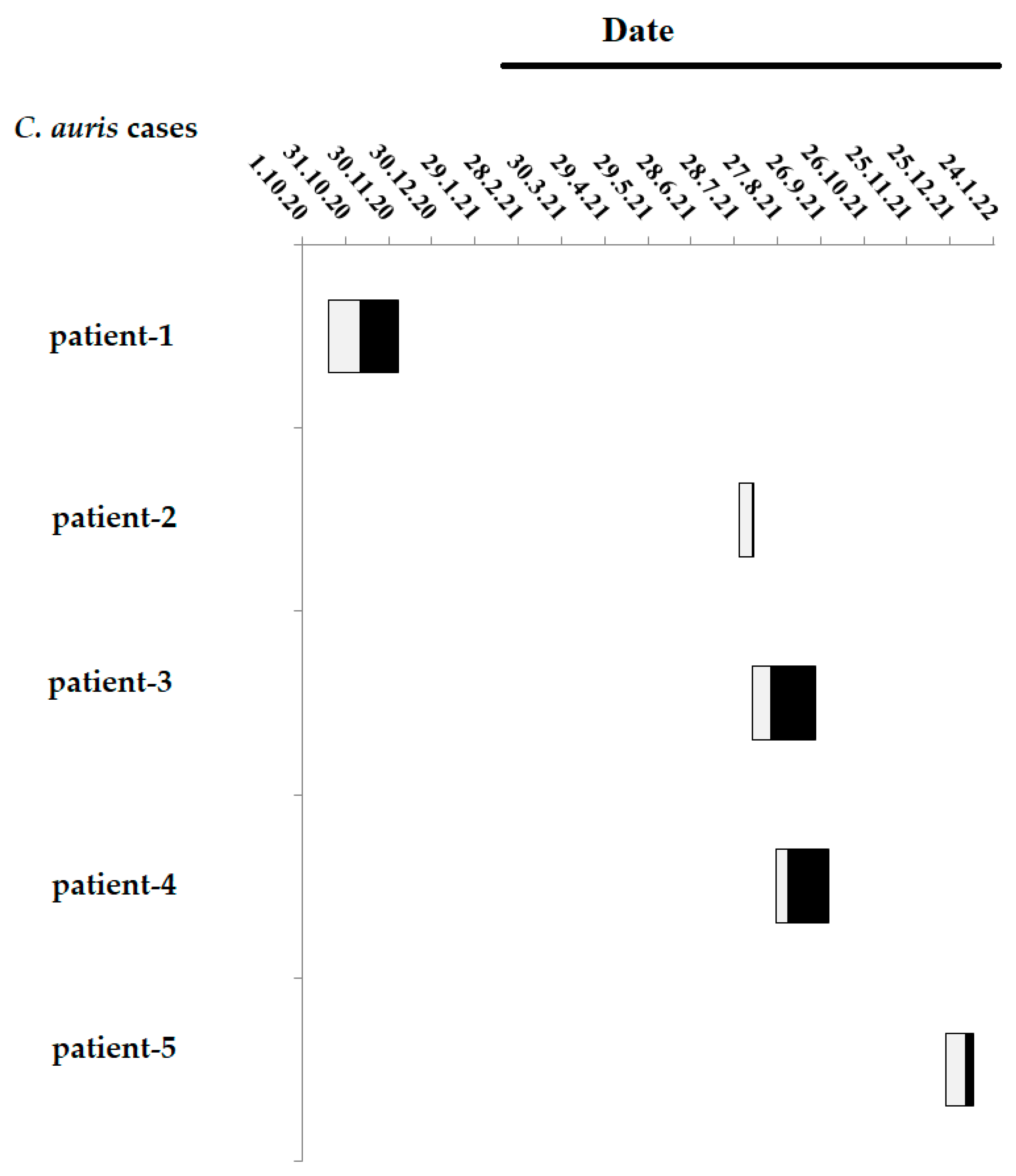
3.1. Timeline of the Five C. auris Cases in the ICU
3.2. Antifungal Susceptibility Testing
3.3. Molecular Typing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pfaller, M.; Diekema, D.J.; Turnidge, J.D.; Castanheira, M.; Jones, R.N. Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species from 1997–2016. Open Forum. Infect. Dis. 2019, 6, 79–94. [Google Scholar] [CrossRef]
- Lockhart, S.R. Current Epidemiology of Candida Infection. Clin. Microbiol. Newsl. 2014, 36, 131–136. [Google Scholar] [CrossRef]
- Chi, H.-W.; Yang, Y.-S.; Shang, S.-T.; Chen, K.-H.; Yeh, K.-M.; Chang, F.-Y.; Lin, J.-C. Candida Albicans versus Non-Albicans Bloodstream Infections: The Comparison of Risk Factors and Outcome. J. Microbiol. Immunol. Infect 2011, 44, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida Auris Sp. Nov., a Novel Ascomycetous Yeast Isolated from the External Ear Canal of an Impatient in a Japanese Hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef]
- Lee, W.G.; Shin, J.H.; Uh, Y. First Three Reported Cases of Nosocomial Fungemia Caused by Candida Auris. J. Clin. Microbiol. 2011, 49, 3139–3142. [Google Scholar] [CrossRef] [PubMed]
- U.S.A. Centers for Disease Control and Prevention (CDC). Candida Auris: A Drug-Resistant Germ That Spreads in Healthcare Facilities. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-drug-resistant.html#:~:text=auris%20has%20caused%20outbreaks%20in,on%20surfaces%20for%20several%20weeks (accessed on 4 February 2022).
- Cortegiani, A.; Misseri, G.; Fasciana, T.; Giammanco, A.A.G.; Chowdhary, A. Epidemiology, Clinical Characteristics, Resistance, and Treatment of Infections by Candida Auris. J. Intensive Care 2018, 6, 69. [Google Scholar] [CrossRef]
- Spruijtenburg, B.; Badali, H.; Abastabar, M.; Mirhendi, H.; Khodavaisy, S.; Sharifisooraki, J.; Taghizadeh Armaki, M.; de Groot, T.; Meis, J.F. Confirmation of fifth Candida auris clade by whole genome sequencing. Emerg. Microbes Infect. 2022, 11, 2405–2411. [Google Scholar] [CrossRef]
- Cendejas-Bueno, E.; Kolecka, A.; Alastruey-Izquierdo, A.; Theelen, B.; Groenewald, M.; Kostrzewa, M.; Cuenca-Estrella, M.; Gómez-López, A.; Boekhout, T. Reclassification of the Candida haemulonii complex as Candida haemulonii (C. haemulonii group I), C. duobushaemulonii sp. nov. (C. haemulonii group II), and C. haemulonii var. vulnera var. nov.: Three multiresistant human pathogenic yeasts. J. Clin. Microbiol. 2012, 50, 3641–3651. [Google Scholar] [CrossRef]
- Kathuria, S.; Singh, P.K.; Sharma, C. Multidrug-Resistant Candida Auris Misidentified as Candida Haemulonii: Characterization by Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry and DNA Sequencing and Its Antifungal Susceptibility Profile Variability by Vitek 2, CLSI Broth Microdilution, and Etest Method. J. Clin. Microbiol. 2015, 53, 1823–1830. [Google Scholar]
- Borman, A.M.; Szekely, A.; Johnson, E.M. Comparative Pathogenicity of United Kingdom Isolates of the Emerging Pathogen Candida Auris and Other Key Pathogenic Candida Species. mSphere 2016, 1, e00189-16. [Google Scholar] [CrossRef]
- Kim, T.H.; Kweon, O.J.; Kim, H.R.; Lee, M.K. Identification of uncommon Candida species using commercial identification system. J. Microbiol. Biotechnol. 2016, 26, 2206–2213. [Google Scholar] [CrossRef] [PubMed]
- Kordalewska, M.; Zhao, Y.; Lockhart, S.R.; Chowdhary, A.; Berrio, I.; Perlin, D.S. Rapid and Accurate Molecular Identification of the Emerging Multidrug-Resistant Pathogen Candida Auris. J. Clin. Microbiol. 2017, 55, 2445–2452. [Google Scholar] [CrossRef]
- Day, A.M.; McNiff, M.M.; Silva Dantas, A.; Gow, N.A.R.; Quinn, J. Hog1 Regulates Stress Tolerance and Virulence in the Emerging Fungal Pathogen Candida Auris. mSphere 2018, 3, e00506-18. [Google Scholar] [CrossRef]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida Auris on a Plastic Health Care Surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef]
- Cadnum, J.L.; Shaikh, A.A.; Piedrahita, C.T. Effectiveness of Disinfectants against Candida Auris and Other Candida Species. Infect. Control. Hosp. Epidemiol. 2017, 38, 1240–1243. [Google Scholar] [CrossRef]
- Kean, R.; Ramage, G. Combined Antifungal Resistance and Biofilm Tolerance: The Global Threat of Candida Auris. mSphere 2019, 4, e00458-19. [Google Scholar] [CrossRef]
- Frías-De-León, M.G.; Hernàndez-Castro, R.; Vite-Garín, T.; Srens, R.; Bonifaz, A.; Castaňő-Olivares, L.; Acosta-Altamirano, G.; Martinez-Herrera, E. Antifungal resistance in Candida auris: Molecular determinants. Antibiotics 2020, 9, 568. [Google Scholar] [CrossRef]
- Stathi, A.; Loukou, I.; Kirikou, H.; Petrocheilou, A.; Moustaki, M.; Velegraki, A.; Zachariadou, L. Isolation of Candida Auris from Cystic Fibrosis Patient, Greece, April 2019. Eur. Surveill. 2019, 24, 1900400. [Google Scholar]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST) Breakpoint Tables for Interpretation of MICs for Antifungal Agents Version 10.0. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/AFST_BP_v10.0_200204_updatd_links_200924.pdf (accessed on 4 February 2022).
- U.S.A. Centers for Disease Control and Prevention (CDC). Candida auris Antifungal Susceptibility Testing and Interpretation. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html (accessed on 9 December 2022).
- Prakash, A.; Sharma, C.; Singh, A.; Kumar Singh, P.; Kumar, A.; Hagen, F.; Govender, N.P.; Colombo, A.L.; Meis, J.F.; Chowdhary, A. Evidence of Genotypic Diversity among Candida Auris Isolates by Multilocus Sequence Typing, Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry and Amplified Fragment Length Polymorphism. Clin. Microbiol. Infect 2016, 22, 277.e1–e9. [Google Scholar] [CrossRef]
- Kumar, M.; Shukla, P.K. Use of PCR Targeting of Internal Transcribed Spacer Regions and Single-Stranded Conformation Polymorphism Analysis of Sequence Variation in Different Regions of rRNA Genes in Fungi for Rapid Diagnosis of Mycotic Keratitis. J. Clin. Microbiol. 2005, 43, 662–668. [Google Scholar] [CrossRef] [PubMed]
- de Groot, T.; Puts, Y.; Berrio, I.; Chowdhary, A.; Meis, J.F. Development of Candida Auris Short Tandem Repeat Typing and Its Application to a Global Collection of Isolates. mBio 2020, 11, e02971-19. [Google Scholar] [CrossRef]
- Edgar, R.C. MUSCLE: Multiple Sequence Alignment with High Accuracy and High Throughput. Nucleic Acids Res. 2004, 32, 1792–1797. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, G.; Lohman, D.J.; Meier, R. Sequence Matrix: Concatenation Software for the Fast Assembly of Multi-Gene Datasets with Character Set and Codon Information. Cladistics 2011, 27, 171–180. [Google Scholar] [CrossRef]
- Tamura, K.; Stecher, G.; Kumar, S. MEGA11: Molecular Evolutionary Genetics Analysis Version 11. Mol. Biol. Evol. 2021, 38, 3022–3027. [Google Scholar] [CrossRef] [PubMed]
- Villanueva-Lozano, H.; Treviño-Rangel, R.J.; González, G.M.; Ramírez-Elizondo, M.T.; Lara-Medrano, R.; Aleman-Bocanegra, M.C.; Guajardo-Lara, C.E.; Gaona-Chávez, N.; Castilleja-Leal, F.; Torre-Amione, G.; et al. Outbreak of Candida auris infection in a COVID-19 hospital in Mexico. Clin. Microbiol. Infect. 2021, 27, 813–816. [Google Scholar] [CrossRef]
- Di Pilato, V.; Codda, G.; Ball, L.; Giacobbe, D.R.; Willison, E.; Mikulska, M.; Magnasco, L.; Crea, F.; Vena, A.; Pelosi, P.; et al. Molecular epidemiological investigation of a nosocomial cluster of C. auris: Evidence of recent emergence in Italy and ease of transmission during the COVID-19 pandemic. J. Fungi 2021, 7, 140. [Google Scholar] [CrossRef] [PubMed]
- Allaw, F.; Kara Zahreddine, N.; Ibrahim, A.; Tannous, J.; Taleb, H.; Bizri, A.R.; Dbaibo, G.; Kanj, S.S. First Candida auris outbreak during a COVID-19 pandemic in a tertiary-care center in Lebanon. Pathogens 2021, 10, 157. [Google Scholar] [CrossRef]
- Prestel, C.; Anderson, E.; Forsberg, K.; Lyman, M.; de Perio, M.A.; Kuhar, D.; Edwards, K.; Rivera, M.; Shugart, A.; Walters, M.; et al. Candida auris outbreak in a COVID-19 specialty care unit-Florida, July–August 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Somers, E.C.; Eschenauer, G.A.; Troost, J.P.; Golob, J.L.; Gandhi, T.N.; Wang, L.; Zhou, N.; Petty, L.A.; Baang, J.H.; Dillman, N.O.; et al. Tocilizumab for treatment of mechanically ventilated patients with COVID-19. Clin. Infect. Dis. 2020, 73, e445–e454. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Ostrowsky, B.; Greenko, J.; Adams, E.; Quinn, M.; O'Brien, B.; Chaturvedi, V.; Berkow, E.; Vallabhaneni, S.; Forsberg, K.; Chaturvedi, S.; et al. Candida auris Isolates Resistant to Three Classes of Antifungal Medications—New York, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 10, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Voss, A.; Meis, J.F. Multidrug-Resistant Candida Auris: “New Kid on the Block” in Hospital-Associated Infections? J. Hosp. Infect. 2016, 94, 209–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, A.; Sharma, A. The lurking scourge of multidrug resistant Candida auris in times of COVID-19 pandemic. J. Glob. Antimicrob. Resist. 2020, 22, 175–176. [Google Scholar] [CrossRef]
- Allert, S.; Schulz, D.; Kämmer, P.; Großmann, P.; Wolf, T.; Schäuble, S.; Panagiotou, G.; Brunke, S.; Hube, B. From Environmental Adaptation to Host Survival: Attributes That Mediate Pathogenicity of Candida Auris. Virulence 2022, 13, 191–194. [Google Scholar] [CrossRef]
- Magobo, R.; Mhlanga, M.; Corcoran, C.; Govender, N.P. Multilocus sequence typing of azole-resistant Candida auris strains, South Africa. S. Afr. J Infect. Dis. 2020, 35, 116. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clin. Infect. Dis. 2017, 15, 134–140. [Google Scholar] [CrossRef]
- Sharma, C.; Kumar, N.; Pandey, R.; Meis, J.F.; Chowdhary, A. Whole genome sequencing of emerging multidrug resistant Candida auris isolates in India demonstrates low genetic variation. New Microbes New Infect. 2016, 13, 77–82. [Google Scholar] [CrossRef]
- Rhodes, J.; Fisher, M.C. Global epidemiology of emerging Candida auris. Curr. Opin. Microbiol. 2019, 52, 84–89. [Google Scholar] [CrossRef]
- Welsh, R.M.; Misas, E.; Forsberg, K.; Lyman, M.; Chow, N.A. Candida auris Whole-Genome Sequence Benchmark Dataset for Phylogenomic Pipelines. J. Fungi 2021, 16, 214. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Abbasi, A.F.; Prakash, S.; Mangat, J.; Hosein, Z.; Haider, N.; Chan, J. Candida auris: An Overview of the Emerging Drug-Resistant Fungal Infection. Infect. Chemother. 2022, 54, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Desoubeaux, G.; Coste, A.T.; Imbert, C.; Hennequin, C. Overview about Candida auris: What's up 12 years after its first description? J. Mycol. Med. 2022, 32, 101248. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, A.; Monnet Dominique, L.; Plachouras, D.; Candida auris survey collaborative group. Increasing Number of Cases and Outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Eur. Surveill. 2022, 27, pii=2200846. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| C. auris Cases | COVID-19 Status | Admission Date | Gender | Co-Morbidities | Age | Apache II Score | ICU Day at C. auris Isolation | LOS (Days) | ICU Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Patient-1 | Negative | 19 October 2020 | Male | paraplegia, diabetes mellitus | 42 | 17 | 22 | 49 | Death |
| Patient-2 | Positive | 1 August 2021 | Female | metastatic adenocarcinoma of rectum (nephrostomy, ureterostomy) | 57 | 23 | 9 | 10 | Survival |
| Patient-3 | Positive | 10 August 2021 | Female | diabetes mellitus, arterial hypertension, asthma | 72 | 18 | 13 | 44 | Survival |
| Patient-4 | Positive | 26 August 2021 | Male | diabetes mellitus, arterial hypertension, painless jaundice (recently placed stent in the common bile) | 78 | 12 | 9 | 37 | Death |
| Patient-5 | Positive | 22 December 2021 | Female | rheumatoid arthritis, renal resection (adenocarcinoma 6 years ago), Hashimoto thyroiditis | 64 | 15 | 14 | 20 | Death |
| C. auris Cases | Date of Isolation of | Source of Specimen | MIC (μg/mL) of Antifungal Agents | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AMPHB 1 | 5-FLUC | FLU 1 | VOR | POS | MICF | AND | ITR | |||
| Patient-1 | 30 November 2020 | Deep hip decubitus Ulcer/urine | 1 | <0.0625 | >256 | >8 | >8 | 0.12 | 0.12 | 2 |
| Patient-2 | 23 August 2021 | Urine | 1 | 0.12 | >128 | >8 | 0.5 | 0.5 | 0.5 | 1 |
| Patient-3 | 1 September 2021 | Urine | 2 | <0.0625 | >128 | 8 | 0.25 | 0.12 | 0.12 | 0.5 |
| Patient-4 | 13 September 2021 | Blood/ Urine | 2 | 0.12 | >128 | 0.5 | 0.25 | 0.12 | 0.12 | 0.25 |
| Patient-5 | 13 January 2022 | Bronchial aspirate | 2 | 0.12 | >128 | 0.12 | 0.12 | 0.25 | 0.25 | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsiari, M.; Mavroidi, A.; Kesesidis, N.; Palla, E.; Zourla, K.; Ntorlis, K.; Konstantinidis, K.; Laskou, M.; Strigklis, K.; Sakkalis, A.; et al. Emergence of Clonally-Related South Asian Clade I Clinical Isolates of Candida auris in a Greek COVID-19 Intensive Care Unit. J. Fungi 2023, 9, 243. https://doi.org/10.3390/jof9020243
Katsiari M, Mavroidi A, Kesesidis N, Palla E, Zourla K, Ntorlis K, Konstantinidis K, Laskou M, Strigklis K, Sakkalis A, et al. Emergence of Clonally-Related South Asian Clade I Clinical Isolates of Candida auris in a Greek COVID-19 Intensive Care Unit. Journal of Fungi. 2023; 9(2):243. https://doi.org/10.3390/jof9020243
Chicago/Turabian StyleKatsiari, Maria, Angeliki Mavroidi, Nikolaos Kesesidis, Eleftheria Palla, Konstantina Zourla, Kyriakos Ntorlis, Konstantinos Konstantinidis, Maria Laskou, Konstantinos Strigklis, Anastasios Sakkalis, and et al. 2023. "Emergence of Clonally-Related South Asian Clade I Clinical Isolates of Candida auris in a Greek COVID-19 Intensive Care Unit" Journal of Fungi 9, no. 2: 243. https://doi.org/10.3390/jof9020243
APA StyleKatsiari, M., Mavroidi, A., Kesesidis, N., Palla, E., Zourla, K., Ntorlis, K., Konstantinidis, K., Laskou, M., Strigklis, K., Sakkalis, A., Nikolaou, C., Platsouka, E. D., Karakasiliotis, I., Vrioni, G., & Tsakris, A. (2023). Emergence of Clonally-Related South Asian Clade I Clinical Isolates of Candida auris in a Greek COVID-19 Intensive Care Unit. Journal of Fungi, 9(2), 243. https://doi.org/10.3390/jof9020243