

Alginate Hydrogel Formulation with Ketorolac for the Treatment of Pain Related Sialolithiasis

 ,
,  ,
, 
 , ,
, ,  and
and
Abstract
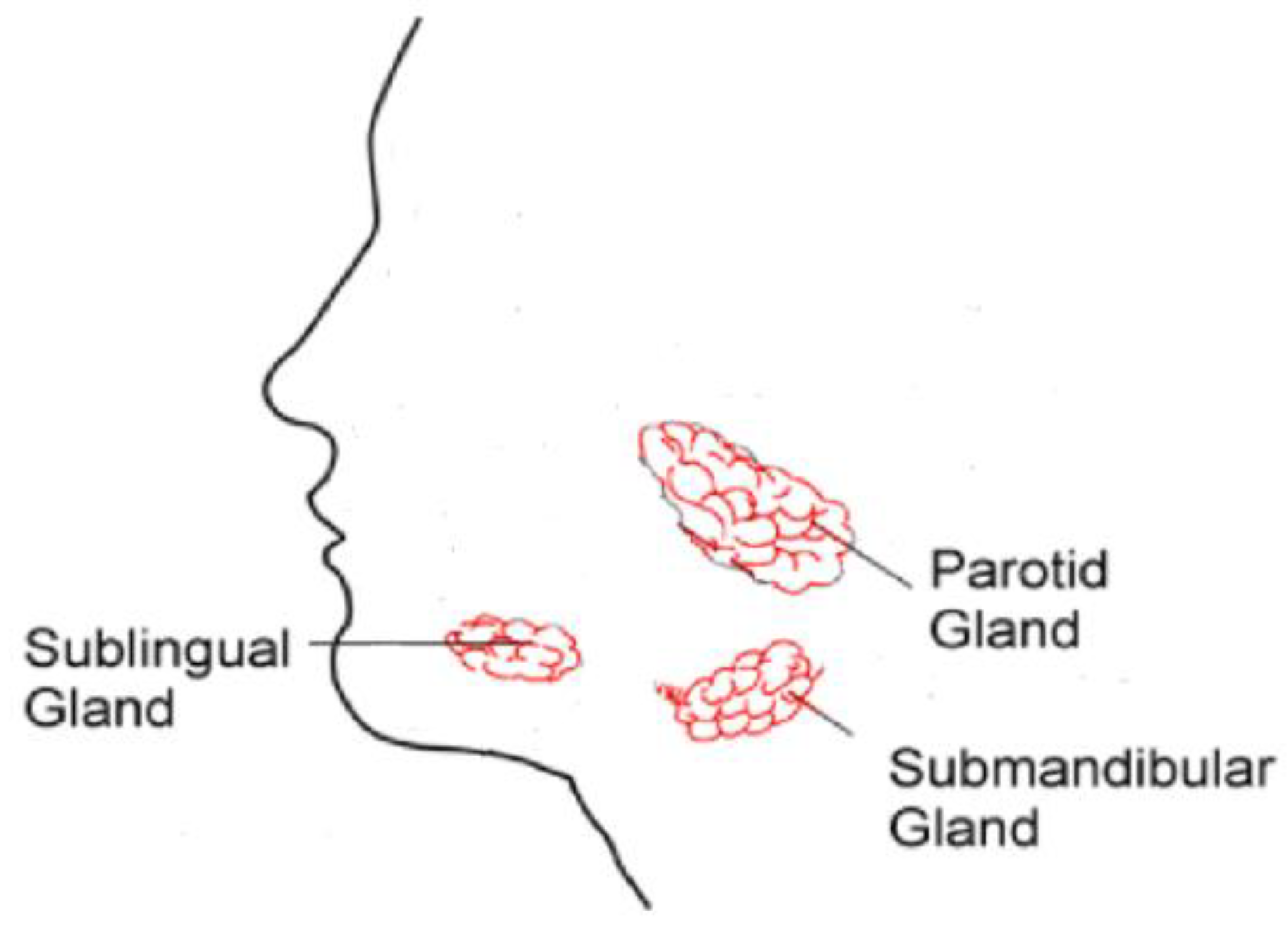
:1. Introduction
2. Results and Discussion
2.1. Formulation of the Alginate Gel with Ketorolac
2.2. Physicochemical Characterization of Kerotolac Hydrogel
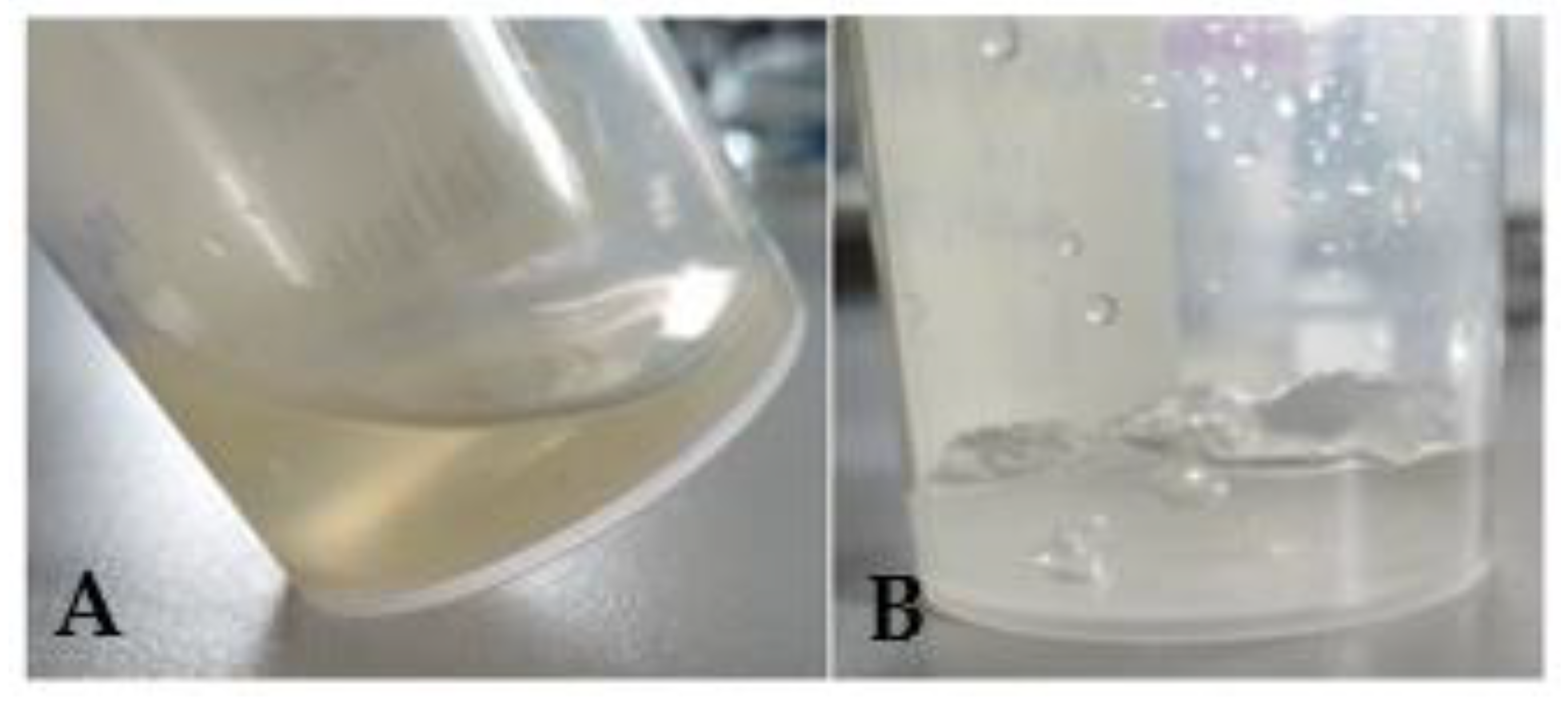
2.2.1. Appearance Evaluation and Sensory Properties
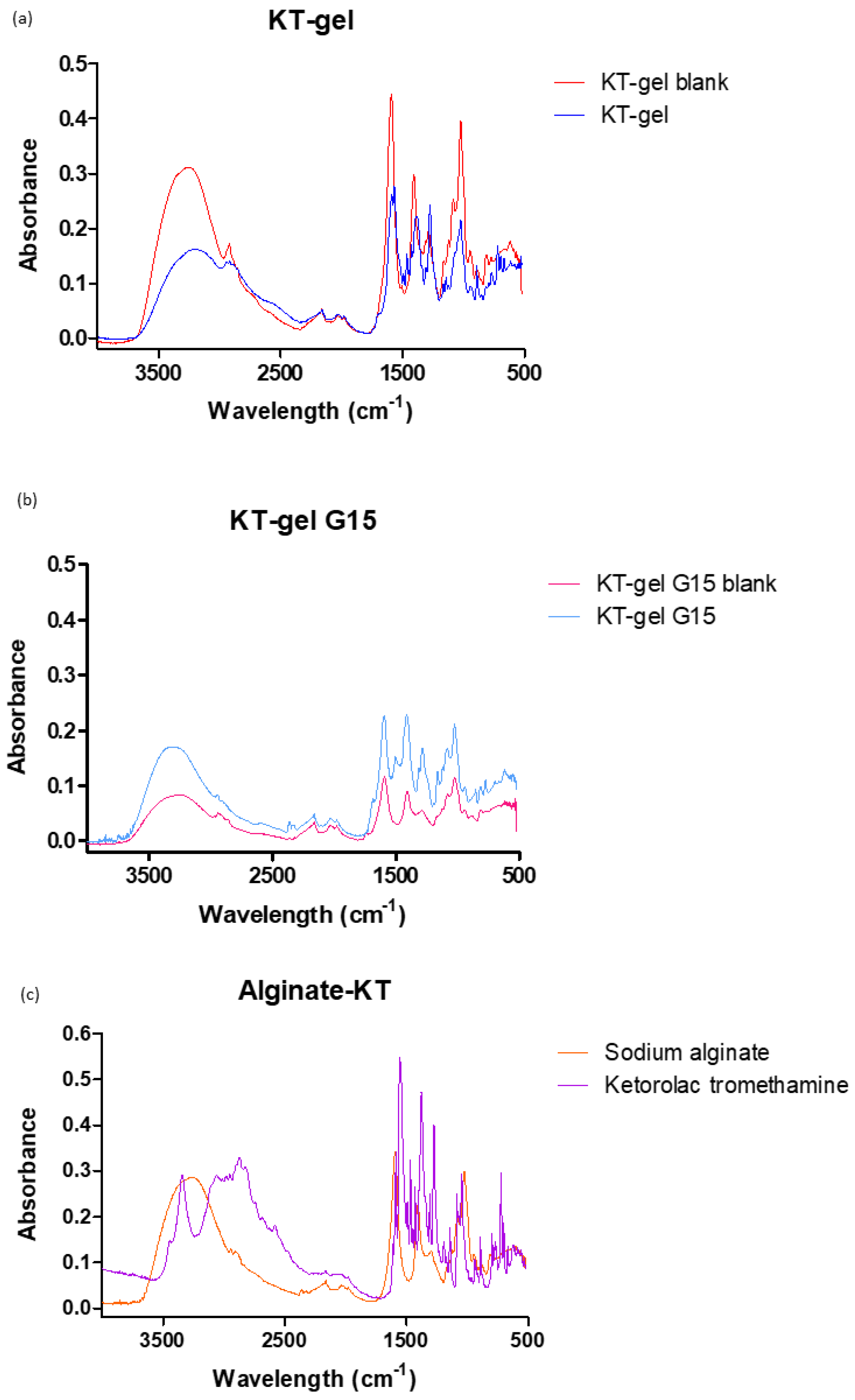
2.2.2. FT-IR
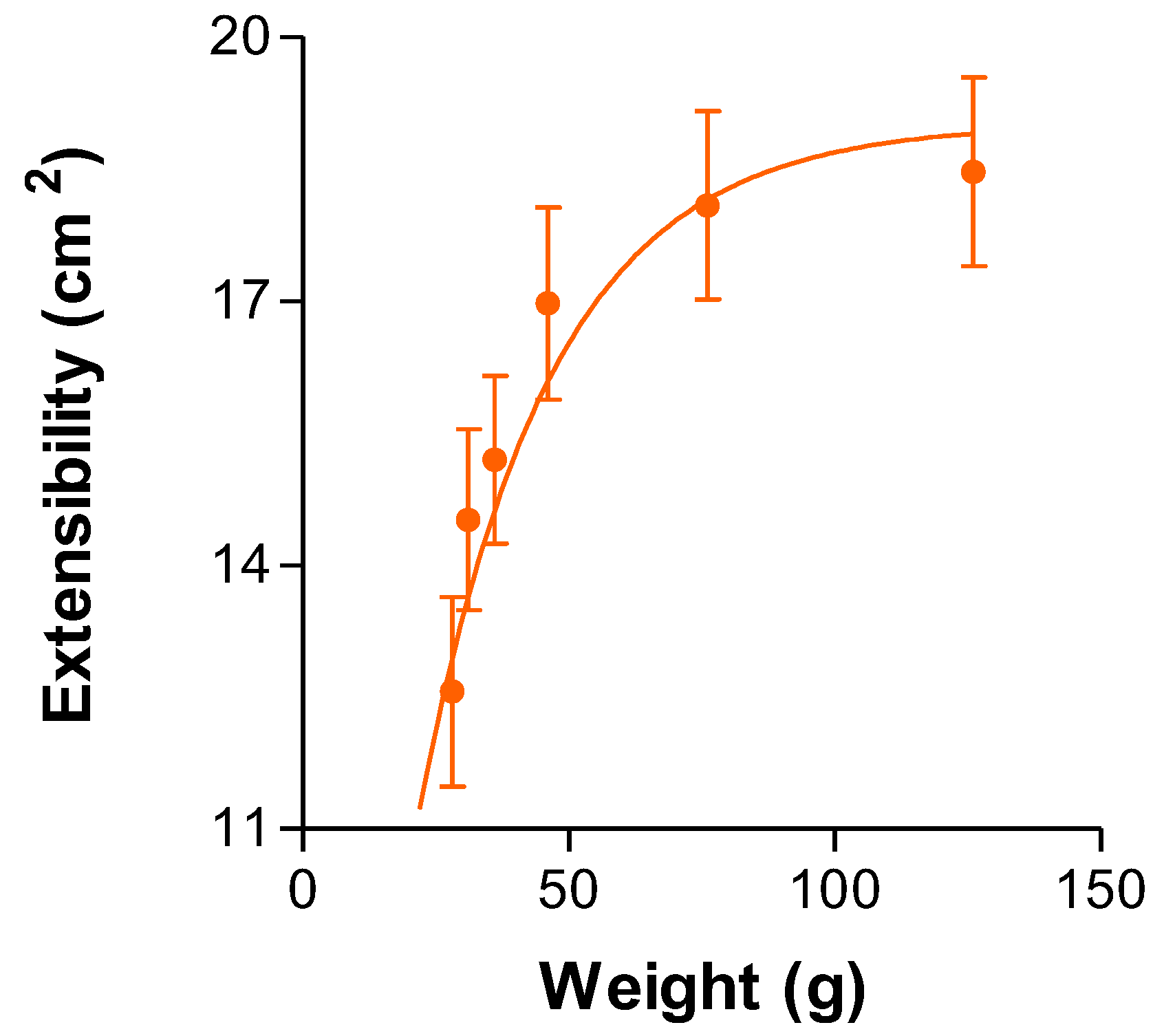
2.2.3. Extensibility
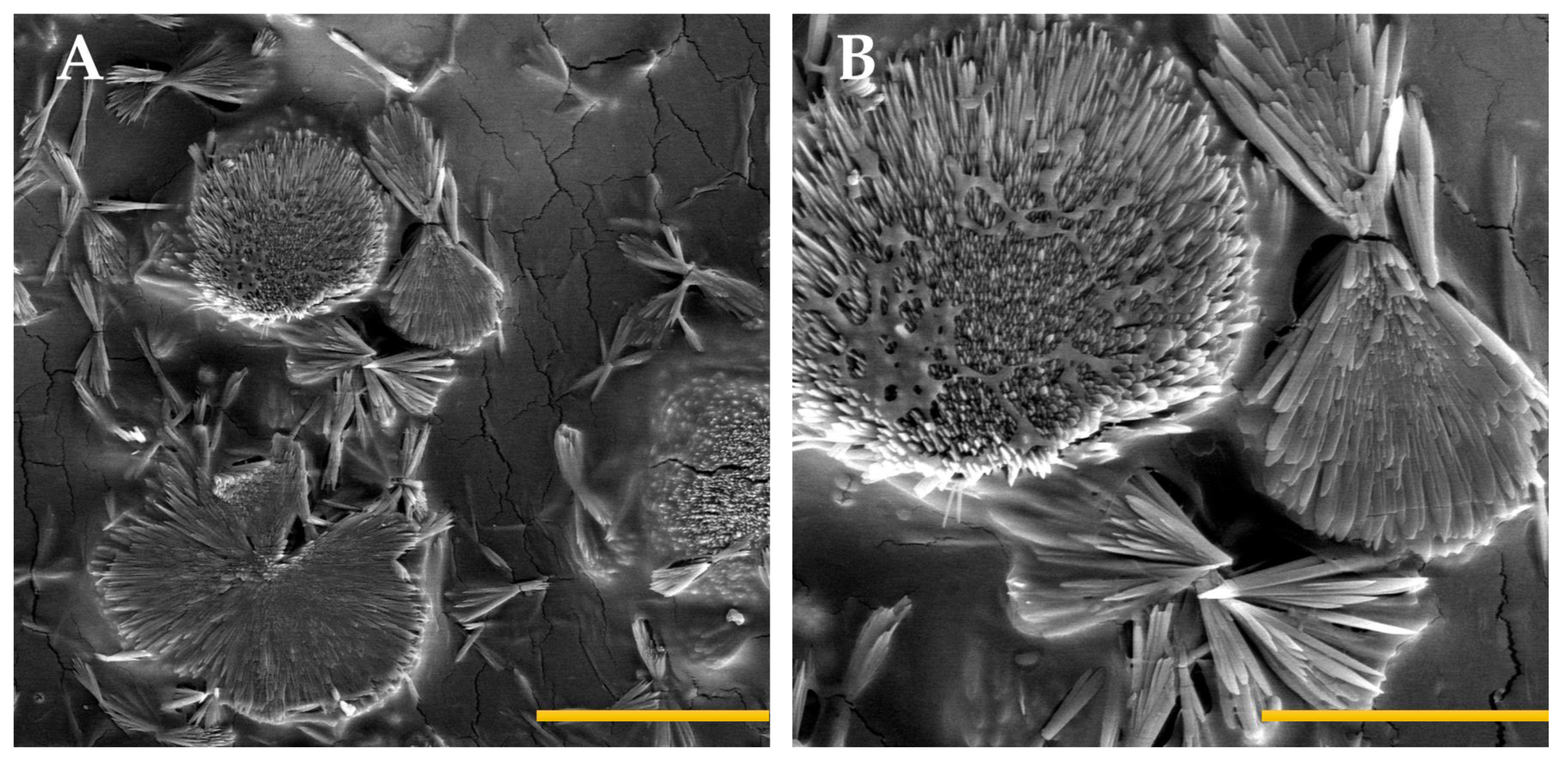
2.2.4. Morphological Studies
2.2.5. Determination of the Gel Porosity
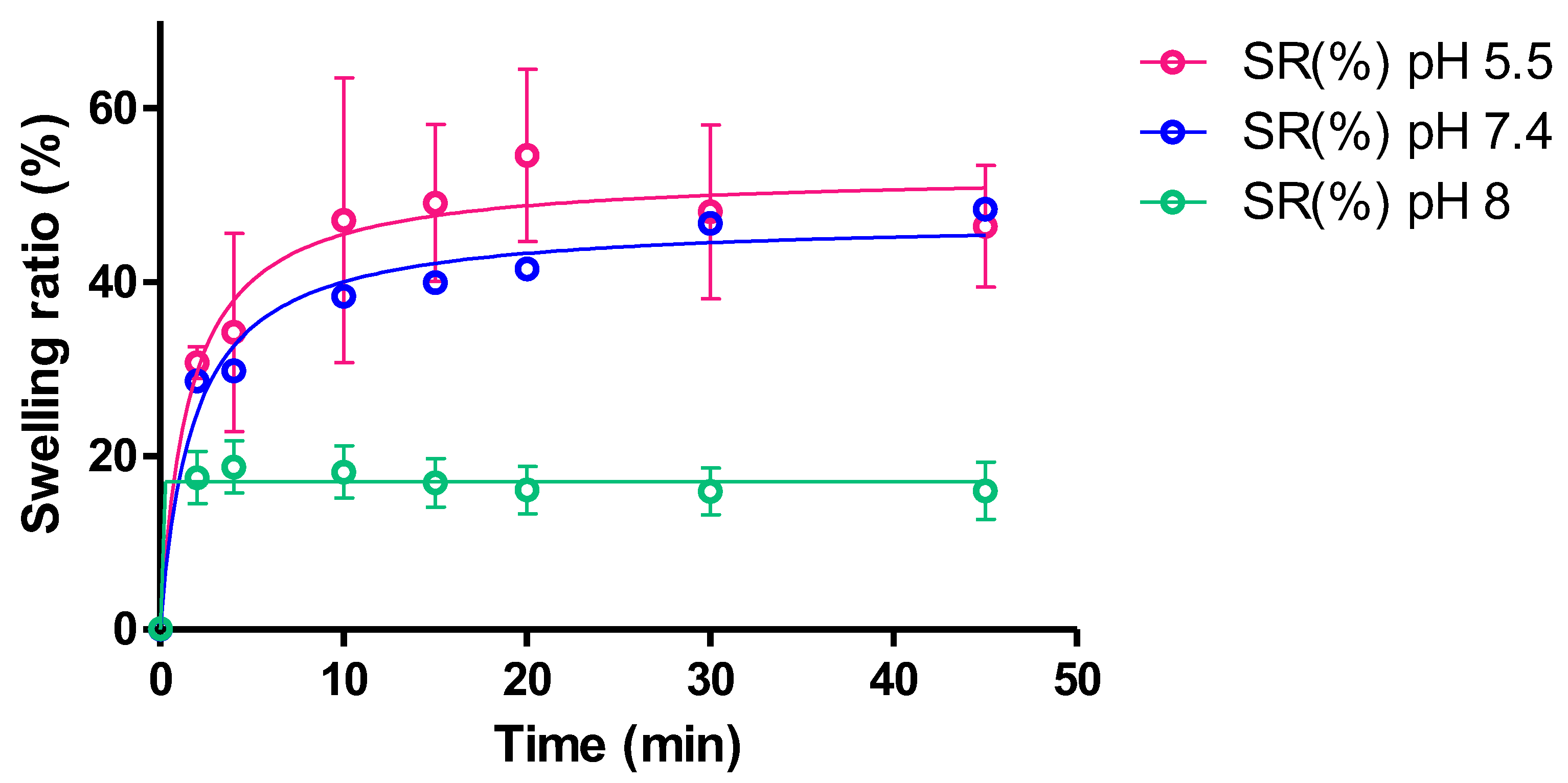
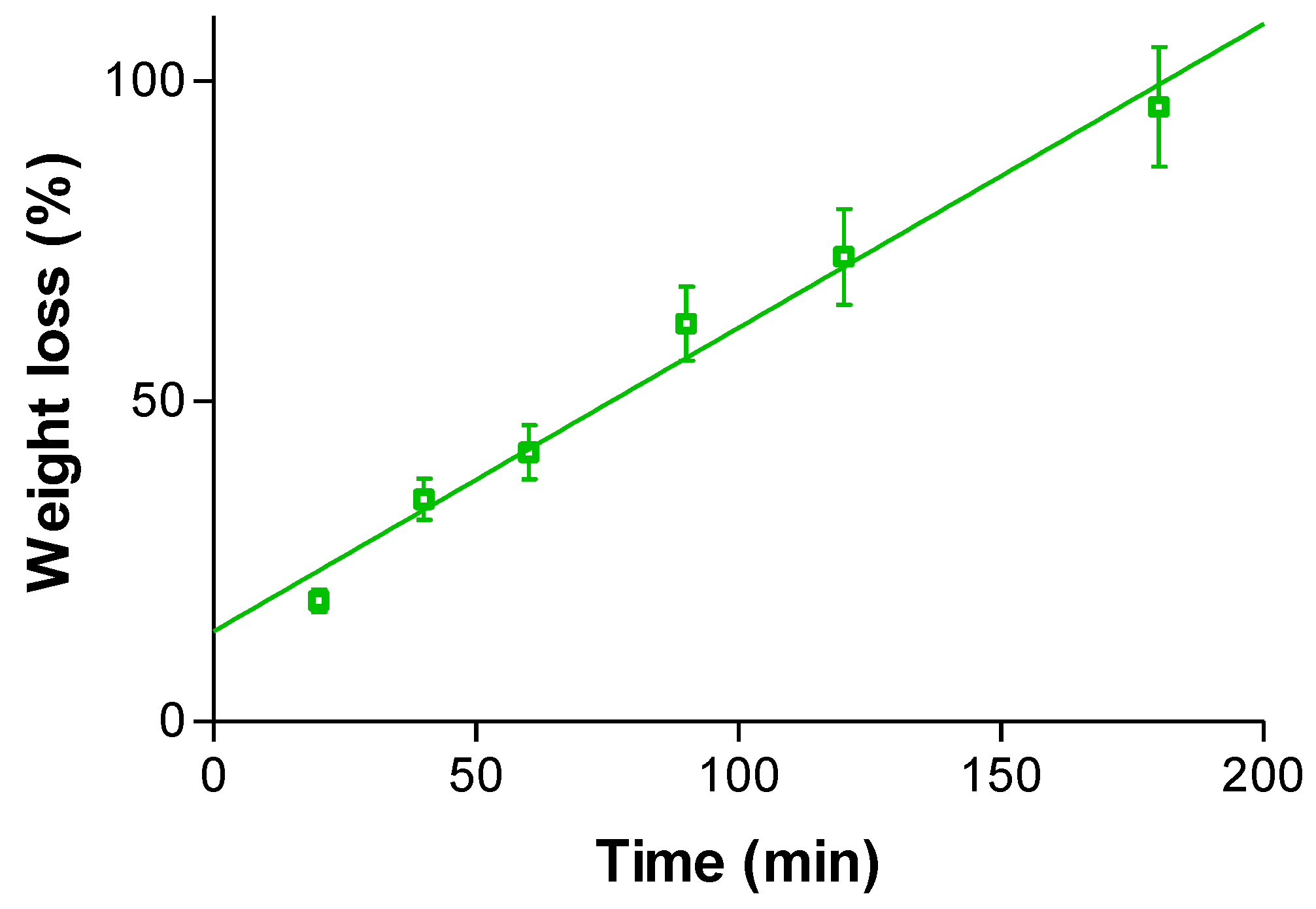
2.2.6. Swelling and Degradation Tests
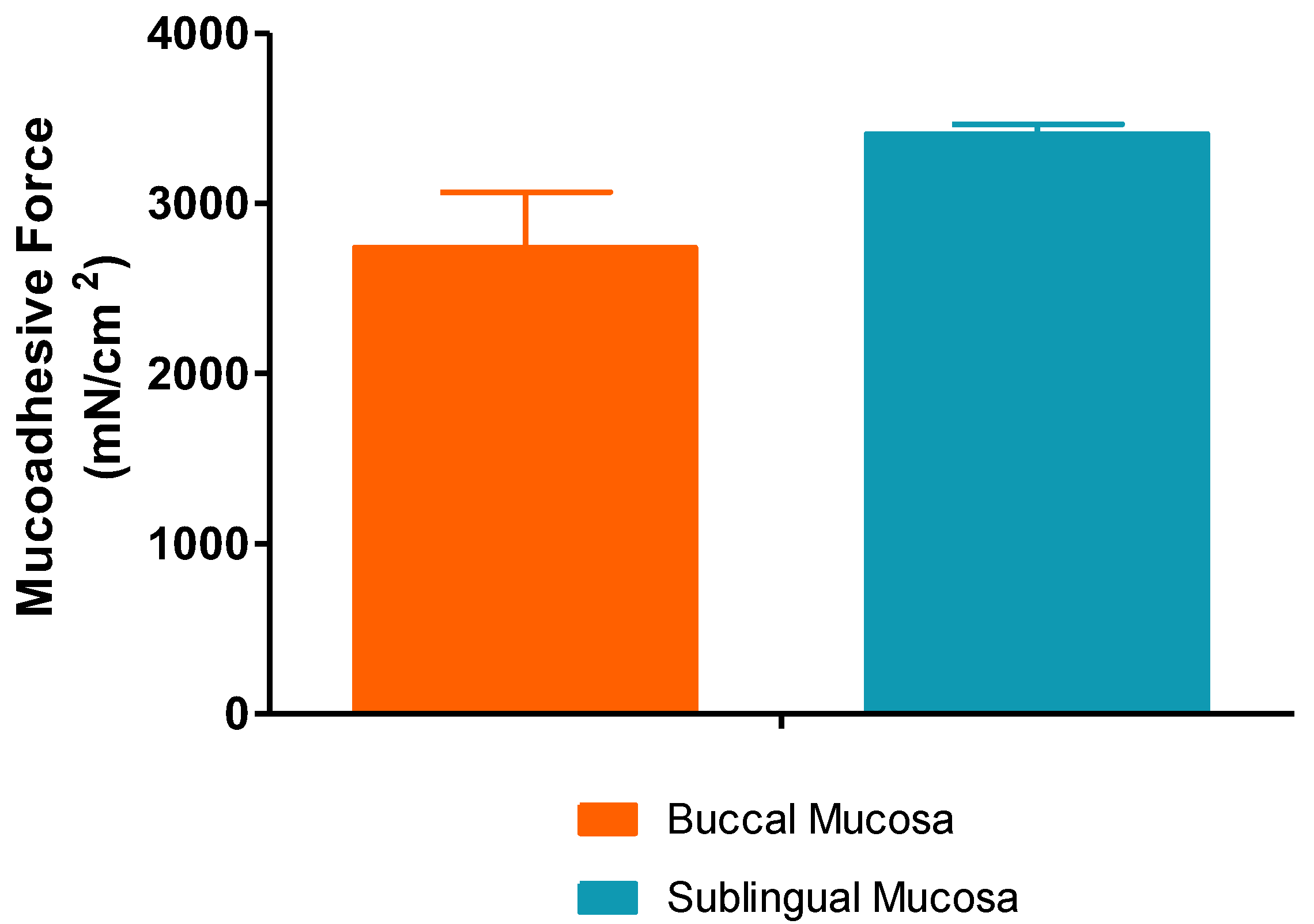
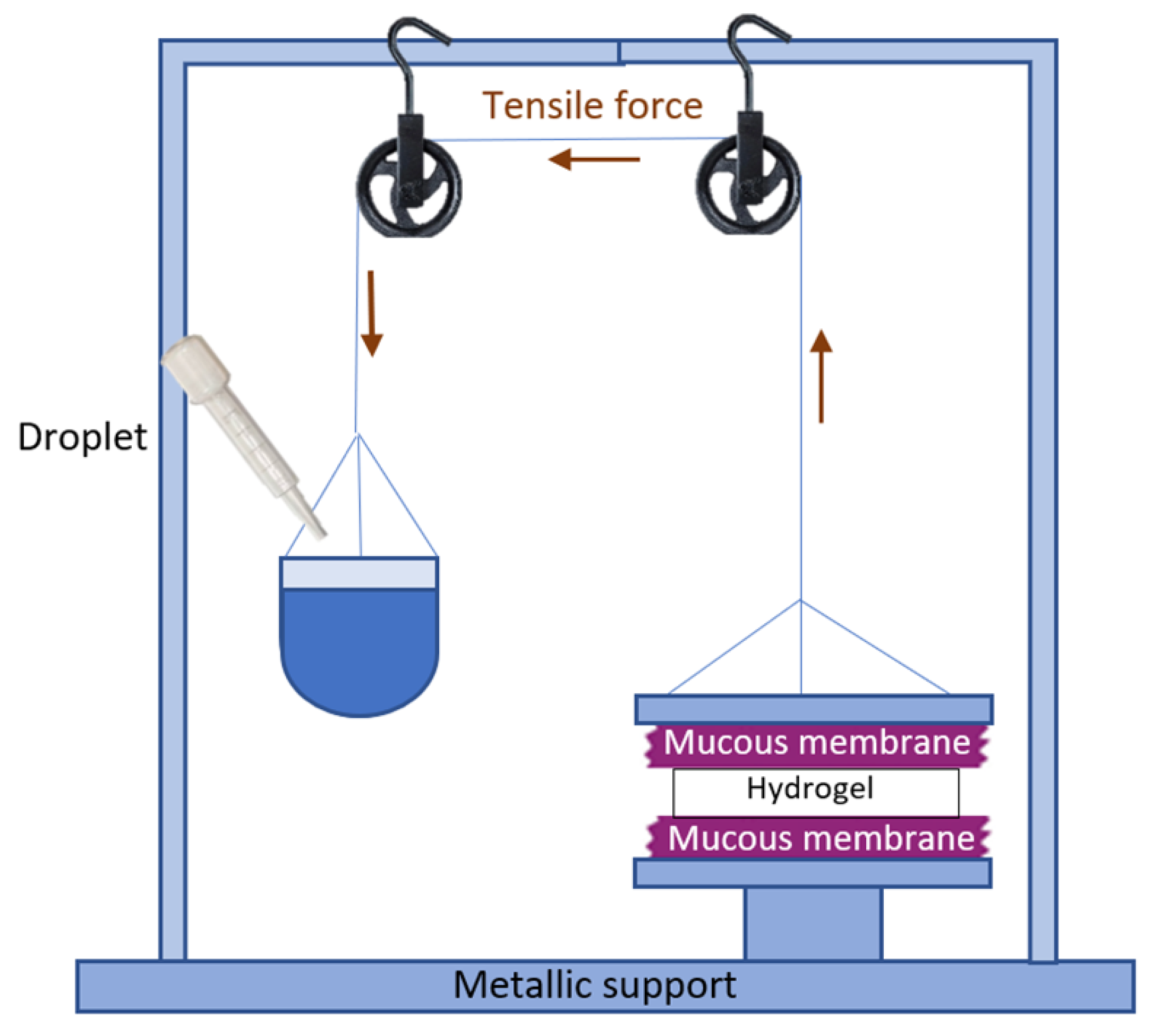
2.2.7. Ex Vivo Mucoadhesion Study
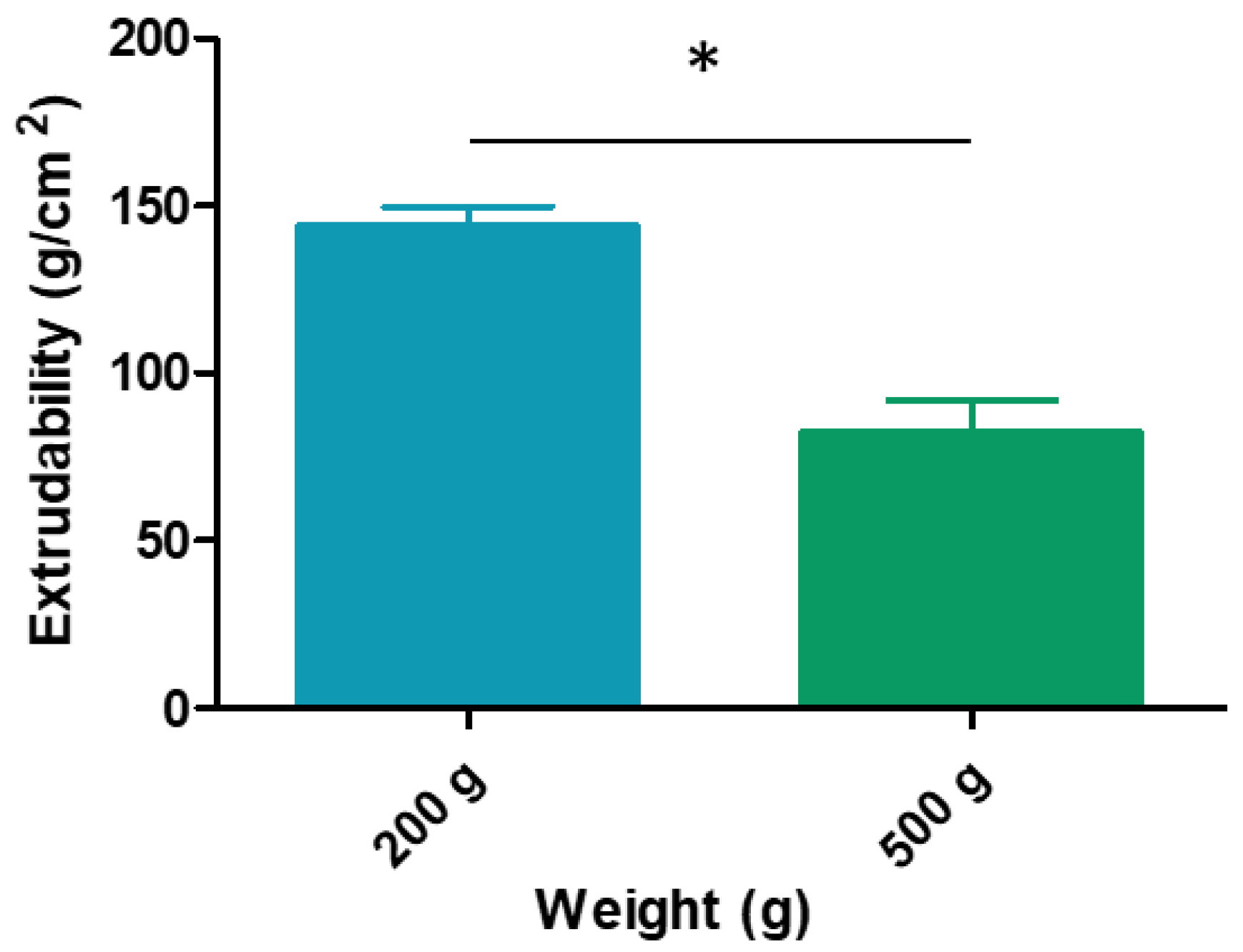
2.2.8. Syringeability/Extrudability Study
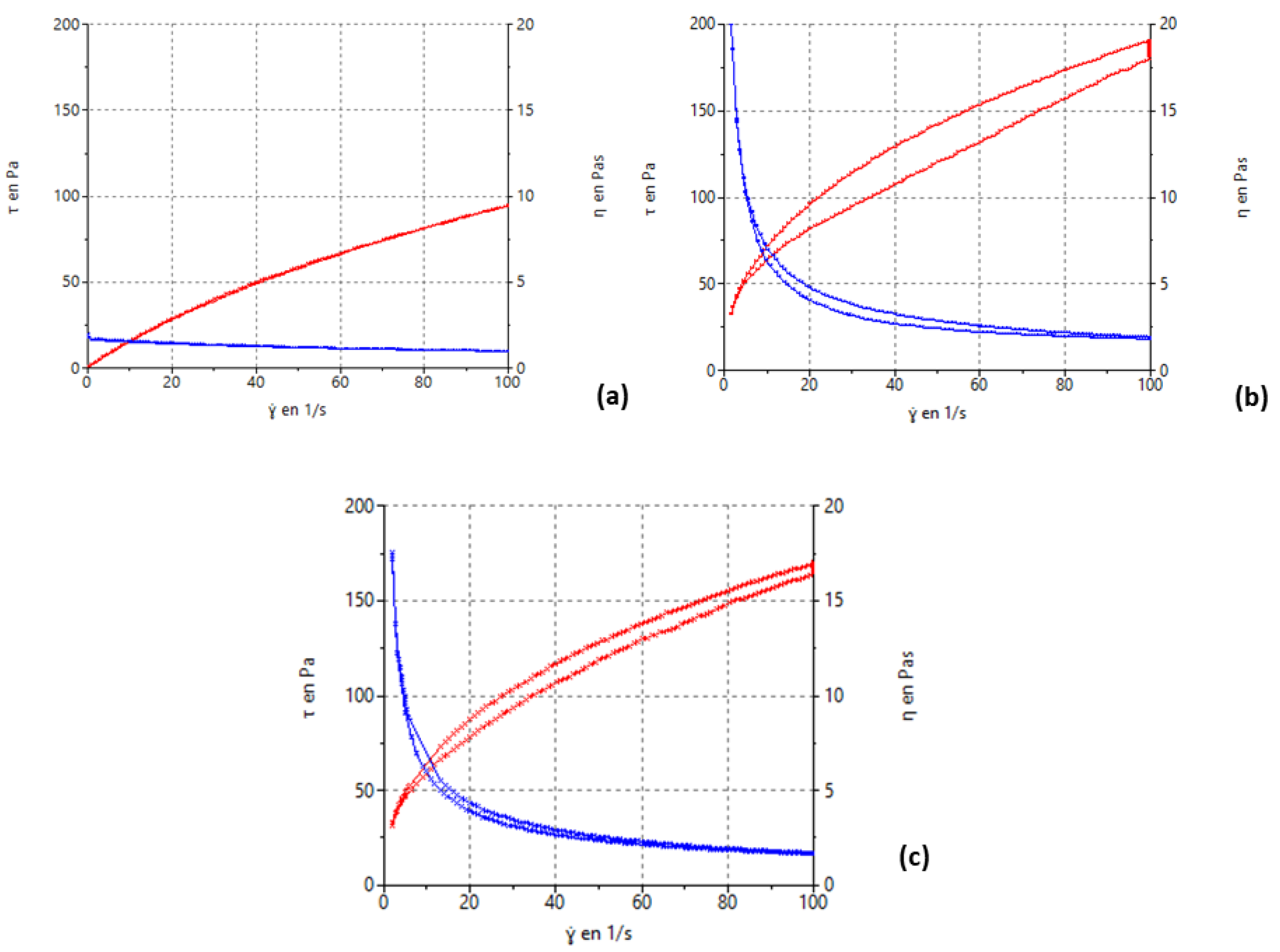
2.2.9. Rheological Analysis
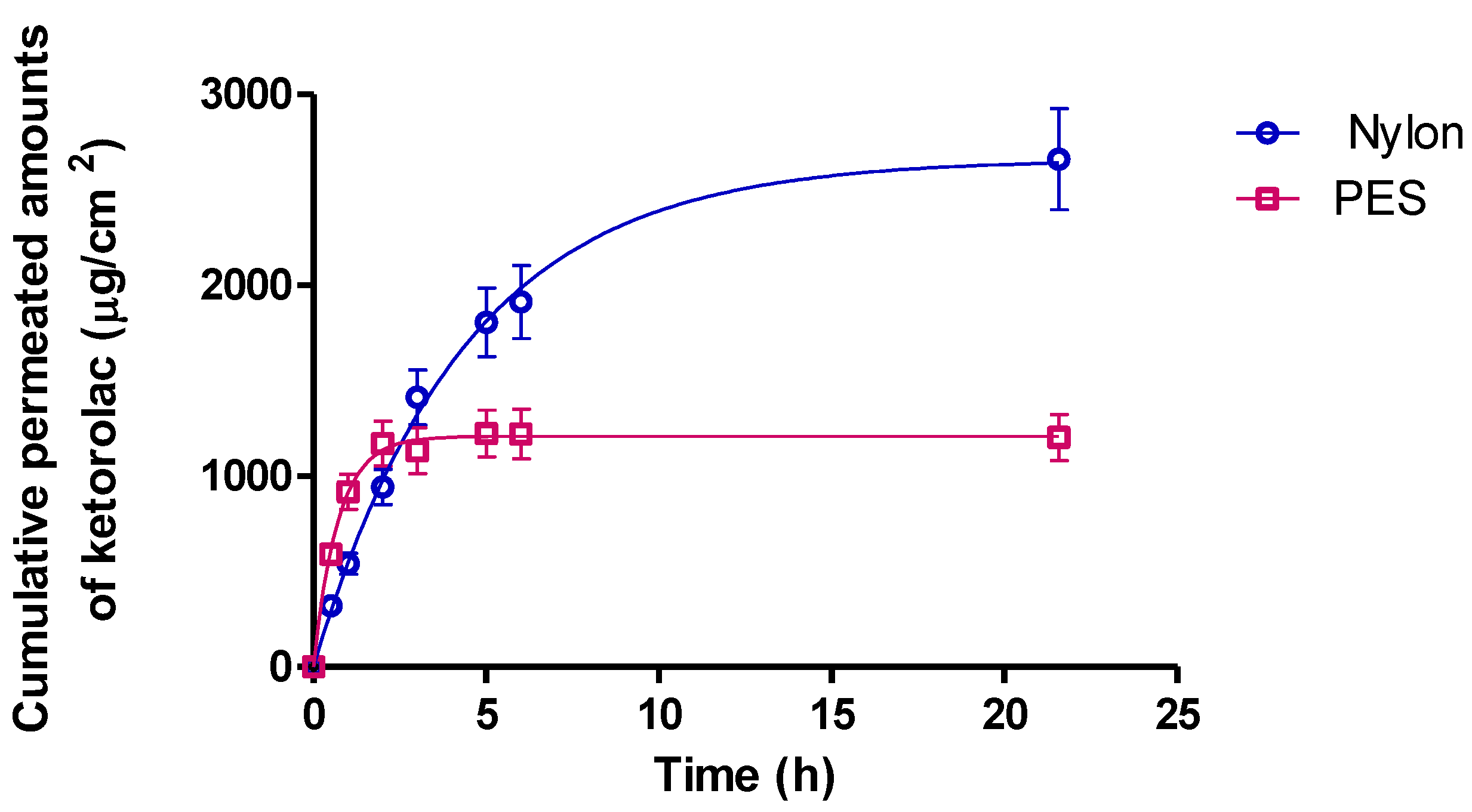
2.3. In Vitro Release Study
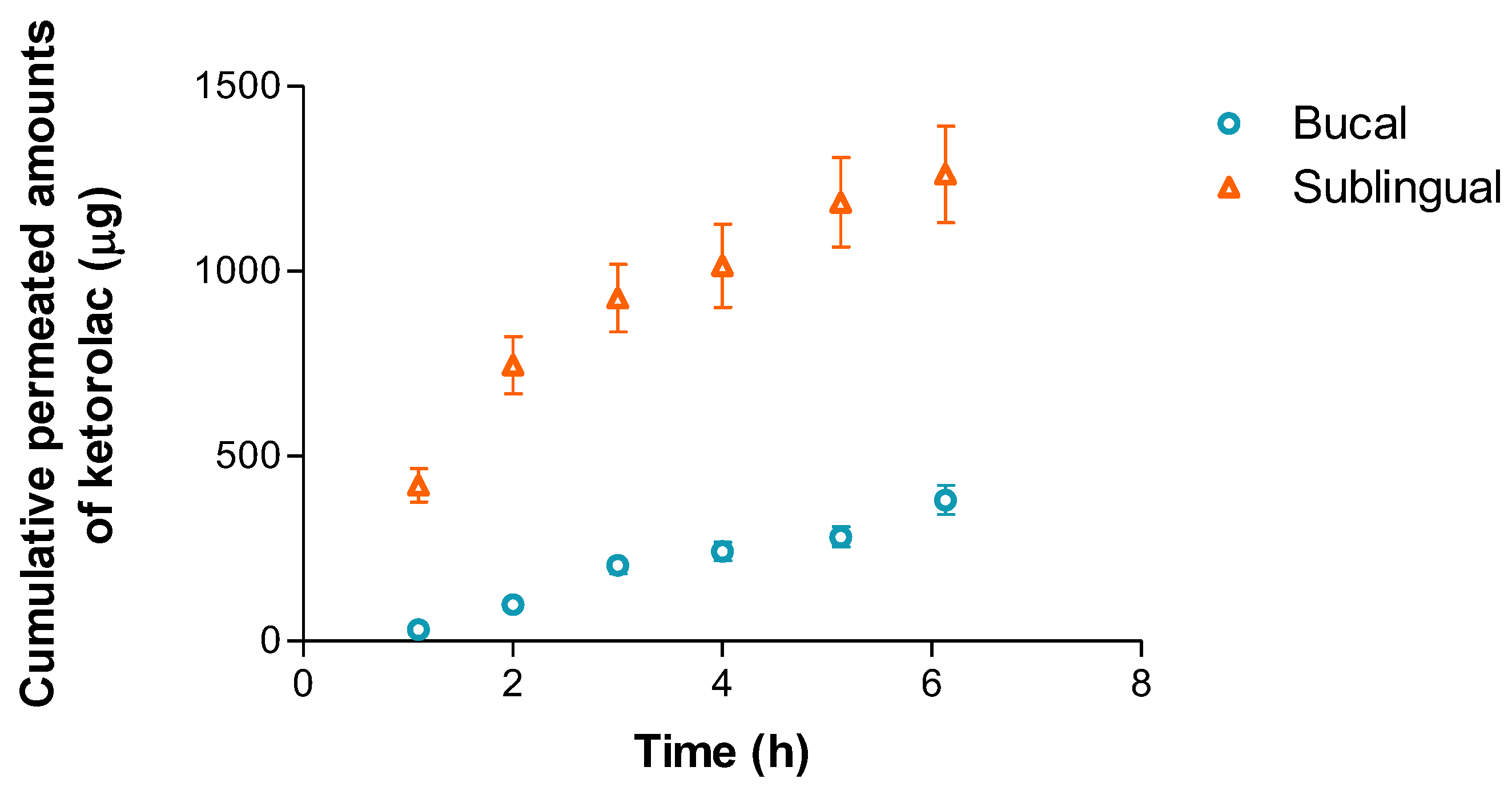
2.4. Ex Vivo Permeation through Buccal and Sublingual Mucosa
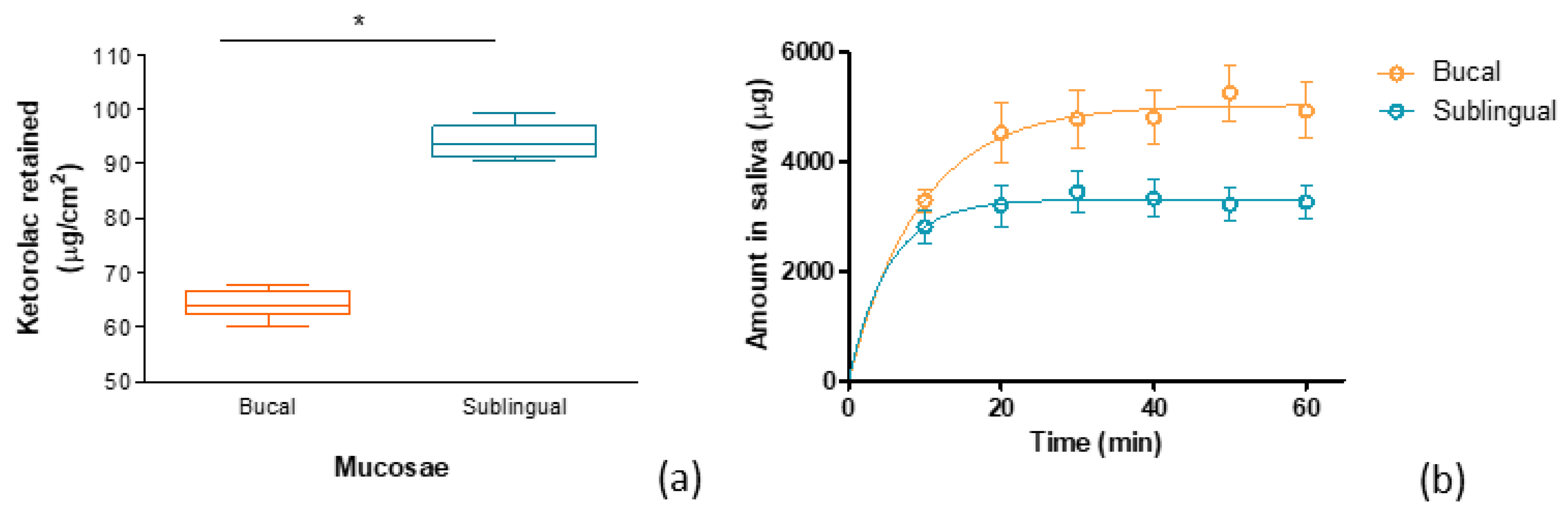
2.5. Evaluation of the Drug Amount Released and Retained in the Buccal/Sublingual Mucosa under an Artificial Saliva Flow
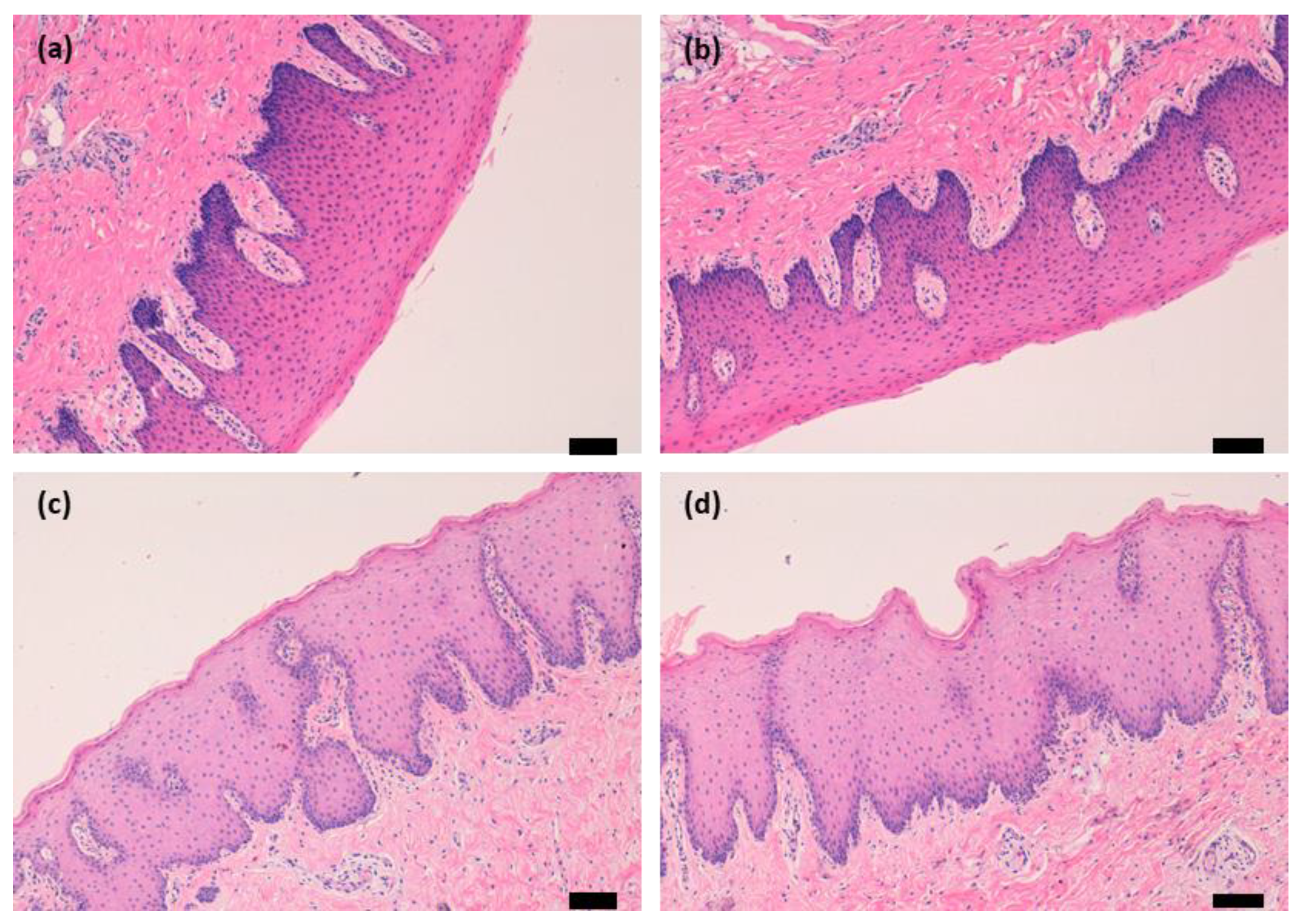
2.6. Mucosa Histology Evaluation
3. Conclusions
4. Materials and Methods
4.1. Material
4.2. Tissues and Experimental Animals for Ex Vivo Assays
4.3. Formulation of the Alginate Gel with Ketorolac
4.4. Physicochemical Characterization of Kerotolac Hydrogel
4.4.1. FT-IR
4.4.2. Extensibility
4.4.3. Morphological Studies
4.4.4. Determination of the Gel Porosity
4.4.5. Swelling and Degradation Tests
4.4.6. Ex Vivo Mucoadhesion Study
4.4.7. Syringeability/Extrudability Study
4.4.8. Rheological Analysis
4.5. In Vitro Release Study
4.6. Ex Vivo Permeation through Buccal/Sublingual Mucosa
4.7. Evaluation of the Drug Amount Released and Retained in the Buccal/Sublingual Mucosa under an Artificial Saliva Flow
4.8. Mucosa Histology Evaluation
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torres Lagares, D.; Barranco Piedra, S.; Serrera Figallo, M.Á.; Hita Iglesias, P.; Martínez-Sahuquillo Márquez, A.; Gutiérrez Pérez, J.L. Sialolitiasis Parotídea Del Conducto de Stensen. Med. Oral Patol. Oral Y Cirugía Bucal 2006, 11, 80–84. [Google Scholar]
- Hupp, J.; Tucker, M.; Ellis, E. Contemporary Oral and Maxillofacial Surgery, 7th ed.; Peterson, L.J., Ellis, E., Hupp, J.R., Tucker, M.R., Eds.; Mosby: Sant Louis, MI, USA, 2018; ISBN 9780323552226. [Google Scholar]
- Thong, H.K.; Mohamad Mahbob, H.; Sabir Husin Athar, P.P.; Tengku Kamalden, T.M.I. Recurrent Submandibular Sialolithiasis in a Child. Cureus 2020, 12, e12163. [Google Scholar] [CrossRef] [PubMed]
- Orlian, A.I.; Schaefer, M.; Golub, J. Multiple Bilateral Sialoliths of the Submandibular Ducts. N. Y. State Dent. J. 1998, 64, 42–43. [Google Scholar] [PubMed]
- Koch, M.; Mantsopoulos, K.; Müller, S.; Sievert, M.; Iro, H. Treatment of Sialolithiasis: What Has Changed? An Update of the Treatment Algorithms and a Review of the Literature. J. Clin. Med. 2022, 11, 231. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Echazú, M.I.; Olivetti, C.E.; Anesini, C.; Perez, C.J.; Alvarez, G.S.; Desimone, M.F. Development and Evaluation of Thymol-Chitosan Hydrogels with Antimicrobial-Antioxidant Activity for Oral Local Delivery. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 81, 588–596. [Google Scholar] [CrossRef]
- Parhi, R. Cross-Linked Hydrogel for Pharmaceutical Applications: A Review. Adv. Pharm. Bull. 2017, 7, 515–530. [Google Scholar] [CrossRef]
- Lu, L.; Yuan, S.; Wang, J.; Shen, Y.; Deng, S.; Xie, L.; Yang, Q. The Formation Mechanism of Hydrogels. Curr. Stem Cell Res. Ther. 2018, 13, 490–496. [Google Scholar] [CrossRef]
- Goh, C.H.; Heng, P.W.S.; Chan, L.W. Alginates as a Useful Natural Polymer for Microencapsulation and Therapeutic Applications. Carbohydr. Polym. 2012, 88, 1–12. [Google Scholar] [CrossRef]
- Chaturvedi, K.; Ganguly, K.; More, U.A.; Reddy, K.R.; Dugge, T.; Naik, B.; Taminabhavi, T.M.; Noolvi, M.N. Sodium Alginate in Drug Delivery and Biomedical Areas. In Natural Polysaccharides in Drug Delivery and Biomedical Application; Hasnain, M.S., Nayak, A.K., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 59–100. ISBN 9780128170557. [Google Scholar]
- Park, K.; Robinson, J.R. Bioadhesive Polymers as Platforms for Oral-Controlled Drug Delivery: Method to Study Bioadhesion. Int. J. Pharm. 1984, 19, 107–127. [Google Scholar] [CrossRef]
- Chickering, D.E.; Mathiowitz, E. Bioadhesive Microspheres: I. A Novel Electrobalance-Based Method to Study Adhesive Interactions between Individual Microspheres and Intestinal Mucosa. J. Control. Release 1995, 34, 251–261. [Google Scholar] [CrossRef]
- Hasnain, M.S.; Jameel, E.; Mohanta, B.; Dhara, A.K.; Alkahtani, S.; Nayak, A.K. Alginates: Sources, Structure, and Properties. In Alginates in Drug Delivery; Academic Press: Cambridge, MA, USA, 2020; pp. 1–17. ISBN 9780128176412. [Google Scholar]
- Trindade, P.A.K.; Giglio, F.P.M.; Colombini-Ishikiriama, B.L.; Calvo, A.M.; Modena, K.C.S.; Ribeiro, D.A.; Dionísio, T.J.; Brozoski, D.T.; Lauris, J.R.P.; Faria, F.A.C.; et al. Sublingual Ketorolac and Sublingual Piroxicam Are Equally Effective for Postoperative Pain, Trismus, and Swelling Management in Lower Third Molar Removal. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 27–34. [Google Scholar] [CrossRef]
- Penniston, S.G.; Hargreaves, K.M. Evaluation of Periapical Injection of Ketorolac for Management of Endodontic Pain. J. Endod. 1996, 22, 55–59. [Google Scholar] [CrossRef]
- Rogers, M.J.; Johnson, B.R.; Remeikis, N.A.; Begole, E.A. Comparison of Effect of Intracanal Use of Ketorolac Tromethamine and Dexamethasone with Oral Ibuprofen on Post Treatment Endodontic Pain. J. Endod. 1999, 25, 381–384. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information PubChem Compound Summary for CID 84003, Ketorolac Tromethamine. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Ketorolac-tromethamine (accessed on 5 March 2023).
- National Center for Biotechnology Information PubChem Compound Summary for CID 133126842 Sodium Alginate. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/133126842 (accessed on 5 March 2023).
- Ghannam, M.G.; Singh, P. Anatomy, Head and Neck, Salivary Glands; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- LLS Health Technical Team How Sensory Properties Are Driving Topical Drug Product Development. Available online: https://www.lubrizol.com/Health/Blog/2020/12/How-Sensory-Properties-are-Driving-Topical-Drug-Product-Development (accessed on 17 February 2023).
- Li, J.; Suo, Z.; Vlassak, J.J. Stiff, Strong, and Tough Hydrogels with Good Chemical Stability. J. Mater. Chem. B 2014, 2, 6708–6713. [Google Scholar] [CrossRef] [PubMed]
- Baus, R.A.; Zahir-Jouzdani, F.; Dünnhaupt, S.; Atyabi, F.; Bernkop-Schnürch, A. Mucoadhesive Hydrogels for Buccal Drug Delivery: In Vitro-In Vivo Correlation Study. Eur. J. Pharm. Biopharm. 2019, 142, 498–505. [Google Scholar] [CrossRef] [PubMed]
- El Moussaoui, S.; Fernández-Campos, F.; Alonso, C.; Limón, D.; Halbaut, L.; Garduño-Ramirez, M.L.; Calpena, A.C.; Mallandrich, M. Topical Mucoadhesive Alginate-Based Hydrogel Loading Ketorolac for Pain Management after Pharmacotherapy, Ablation, or Surgical Removal in Condyloma Acuminata. Gels 2021, 7, 8. [Google Scholar] [CrossRef]
- Foudazi, R.; Zowada, R.; Manas-Zloczower, I.; Feke, D.L. Porous Hydrogels: Present Challenges and Future Opportunities. Langmuir 2023, 39, 2092–2111. [Google Scholar] [CrossRef] [PubMed]
- Roberge, C.L.; Kingsley, D.M.; Cornely, L.R.; Spain, C.J.; Fortin, A.G.; Corr, D.T. Viscoelastic Properties of Bioprinted Alginate Microbeads Compared to Their Bulk Hydrogel Analogs. J. Biomech. Eng. 2022, 145, 031002. [Google Scholar] [CrossRef]
- Nindiyasari, F.; Fernández-Díaz, L.; Griesshaber, E.; Astilleros, J.M.; Sánchez-Pastor, N.; Schmahl, W.W. Influence of Gelatin Hydrogel Porosity on the Crystallization of CaCO3. Cryst. Growth Des. 2014, 14, 1531–1542. [Google Scholar] [CrossRef]
- Choi, N.W.; Kim, J.; Chapin, S.C.; Duong, T.; Donohue, E.; Pandey, P.; Broom, W.; Hill, W.A.; Doyle, P.S. Multiplexed Detection of MRNA Using Porosity-Tuned Hydrogel Microparticles. Anal. Chem. 2012, 84, 9370–9378. [Google Scholar] [CrossRef]
- Da Silva, M.A.; Bierhalz, A.C.K.; Kieckbusch, T.G. Alginate and Pectin Composite Films Crosslinked with Ca2+ Ions: Effect of the Plasticizer Concentration. Carbohydr. Polym. 2009, 77, 736–742. [Google Scholar] [CrossRef]
- El Moussaoui, S.; Mallandrich, M.; Garrós, N.; Calpena, A.C.; Lagunas, M.J.R.; Fernández-Campos, F. Hpv Lesions and Other Issues in the Oral Cavity Treatment and Removal without Pain. Int. J. Mol. Sci. 2021, 22, 11158. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.F.; Liu, F.; Brown, M.B. Advances in Oral Transmucosal Drug Delivery. J. Control. Release 2011, 153, 106–116. [Google Scholar] [CrossRef]
- Moles-Aranda, C.; Calpena-Campmany, A.; Halbaut-Bellowa, L.; Díaz-Tomé, V.; Otero-Espinar, F.; Morales-Molina, J.; Clares-Naveros, B. Novel Polymeric Formulation for Removal of Gastrointestinal Polyps by Digestive Endoscopy. Pharmaceutics 2020, 12, 322. [Google Scholar] [CrossRef]
- Mallandrich, M.; Fernández-Campos, F.; Clares, B.; Halbaut, L.; Alonso, C.; Coderch, L.; Garduño-Ramírez, M.L.; Andrade, B.; del Pozo, A.; Lane, M.E.; et al. Developing Transdermal Applications of Ketorolac Tromethamine Entrapped in Stimuli Sensitive Block Copolymer Hydrogels. Pharm. Res. 2017, 34, 1728–1740. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, S.; Ferrara, A.; Larach, S.; Williamson, P. Intraoperative Use of Toradol® Facilitates Outpatient Hemorrhoidectomy. Dis. Colon Rectum 1994, 37, 793–799. [Google Scholar] [CrossRef]
- Limón, D.; Jiménez-Newman, C.; Calpena, A.C.; González-Campo, A.; Amabilino, D.B.; Pérez-García, L. Microscale Coiling in Bis-Imidazolium Supramolecular Hydrogel Fibres Induced by the Release of a Cationic Serine Protease Inhibitor. Chem. Commun. 2017, 53, 4509–4512. [Google Scholar] [CrossRef]
- Lau, W.M.; Ng, K.W. Finite and Infinite Dosing. In Percutaneous Penetration Enhancers Drug Penetration into/through the Skin; Dragicevic, N., Maibach, H.I., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 35–44. [Google Scholar]
- PubChem Database Ketorolac|C15H13NO3—PubChem. Available online: https://Pubchem.Ncbi.Nlm.Nih.Gov/Compound/3826 (accessed on 20 November 2021).
- PubChem Database Ketorolac Tromethamine|C19H24N2O6—PubChem. Available online: https://Pubchem.Ncbi.Nlm.Nih.Gov/Compound/Ketorolac-Tromethamine (accessed on 20 November 2021).
- TORADOL (Ketorolac Tromethamine Tablets); Roche Laboratories Inc.: Branchburg, NJ, USA, 2008; pp. 1–27.
- Harris, D.; Robinson, J.R. Drug Delivery via the Mucous Membranes of the Oral Cavity. J. Pharm. Sci. 1992, 81, 1–10. [Google Scholar] [CrossRef]
- Cordero, J.A.; Alarcon, L.; Escribano, E.; Obach, R.; Domenech, J. A Comparative Study of the Transdermal Penetration of a Series of Nonsteroidal Antiinflammatory Drugs. J. Pharm. Sci. 1997, 86, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Miranda, M.; Cardoso, C.; Vitorino, C. Quality and Equivalence of Topical Products: A Critical Appraisal. Eur. J. Pharm. Sci. 2020, 148, 105082. [Google Scholar] [CrossRef]
- Li, W.-Z.; Zhao, N.; Zhou, Y.-Q.; Yang, L.-B.; Wang, X.-N.; Hao, B.-H.; Peng, K.; Zhang, C.-F. Post-Expansile Hydrogel Foam Aerosol of PG-Liposomes: A Novel Delivery System for Vaginal Drug Delivery Applications. Eur. J. Pharm. Sci. 2012, 47, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Mei, L.; Chen, J.; Yu, S.; Huang, Y.; Xie, Y.; Wang, H.; Pan, X.; Wu, C. Expansible Thermal Gelling Foam Aerosol for Vaginal Drug Delivery. Drug Deliv. 2017, 24, 1325–1337. [Google Scholar] [CrossRef]
- Yang, T.-T.; Cheng, Y.-Z.; Qin, M.; Wang, Y.-H.; Yu, H.-L.; Wang, A.-L.; Zhang, W.-F. Thermosensitive Chitosan Hydrogels Containing Polymeric Microspheres for Vaginal Drug Delivery. Biomed. Res. Int. 2017, 2017, 3564060. [Google Scholar] [CrossRef]
- Costa, P.; Sousa Lobo, J.M. Modeling and Comparison of Dissolution Profiles. Eur. J. Pharm. Sci. 2001, 13, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Park, E.K.; Song, K.W. Rheological Evaluation of Petroleum Jelly as a Base Material in Ointment and Cream Formulations: Steady Shear Flow Behavior. Arch. Pharm. Res. 2010, 33, 141–150. [Google Scholar] [CrossRef]
- Marques, M.R.C.; Loebenberg, R.; Almukainzi, M. Simulated Biological Fluids with Possible Application in Dissolution Testing. Dissolut. Technol. 2011, 18, 15–28. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A Review of Saliva: Normal Composition, Flow, and Function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Gómez-Segura, L.; Parra, A.; Calpena, A.C.; Gimeno, Á.; Boix-Montañes, A. Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study. Vet. Sci. 2020, 7, 152. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Alginate [%] | CaCl2 [mM] | Gelation [Yes/No] | Physical Stability [Yes/No] | Viscosity | pH |
|---|---|---|---|---|---|---|
| G1 | 0.5 | 4 | No | - | - | - |
| G2 | 0.5 | 8 | No | - | - | - |
| G3 | 0.5 | 10 | No | - | - | - |
| G4 | 0.5 | 12 | No | - | - | - |
| G7 | 1 | 4 | No | - | - | - |
| G8 | 1 | 8 | Yes | No | - | - |
| G9 | 1 | 10 | Yes | No | - | - |
| G10 | 1 | 12 | Yes | No | - | - |
| G13 | 2 | 4 | No | - | - | - |
| G14 | 2 | 8 | Yes | Yes | Fluid | 6.90 |
| G15 | 2 | 10 | Yes | Yes | Soft | 6.99 |
| G16 | 2 | 12 | Yes | Yes | Thick | 7.72 |
| Swelling Ratio (Mean ± SD) | |||
|---|---|---|---|
| Parameters | pH 5.5 | pH 7.4 | pH 8.0 |
| Bmax (%) | 52.57± | 47.17± | 17.02± |
| Kd (min) | 1.55± | 1.79 | |
| R2 | 0.787 | 0.972 | 0.84 |
| Formulation | Rheological Behaviour and Model | Viscosity at 100 s−1 [Pa·s] | |
|---|---|---|---|
| Stretch Ramp-Up | Stretch Ramp-Down | ||
| KT G15 gel previous reticulation | Pseudoplastic (Cross, r = 1.0000) | Pseudoplastic (Cross, r = 1.0000) | 0.94 ± 1.5 |
| KT G15 gel | Pseudoplastic (Cross, r = 0.9999) | Pseudoplastic (Cross, r = 1.0000) | 1.88 ± 24.5 |
| KT G15 gel extruded | Pseudoplastic (Cross, r = 0.9999) | Pseudoplastic (Cross, r = 1.0000) | 1.68 ± 13.9 |
| Kinetic Models | Nylon |
|---|---|
| Hyperbolic | 0.9721 |
| First-order | 0.9973 |
| Higuchi | 0.897 |
| Parameters | Values ± SD |
|---|---|
| Ymax (µg/cm2) | 2666 ± 25 |
| K (h−1) | 0.225 ± 0.027 |
| Half Life (h) | 3.08 |
| R2 | 0.997 |
| Buccal | Sublingual | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameters | Units | Median | Min | Max | Median | Min | Max | p-Value |
| J | µg/h | 92.89 | 82.35 | 100.67 | 264.8 | 214.62 | 316.09 | p < 0.0001 |
| J/SUP | µg/h/cm2 | 145.14 | 128.67 | 157.3 | 413.75 | 335.34 | 493.89 | p < 0.0001 |
| Kp | cm/h | 0.0143 | 0.0129 | 0.0157 | 0.0414 | 0.0335 | 0.0494 | p < 0.0001 |
| Q6 | µg/cm2 | 547.32 | 534.73 | 637.8 | 1863.14 | 1652.41 | 2354.12 | p < 0.0001 |
| Css 1 cm2 | µg/mL | 0.078 | 0.07 | 0.085 | 0.225 | 0.182 | 0.268 | p < 0.0001 |
| Css 2 cm2 | µg/mL | 0.155 | 0.14 | 0.171 | 0.45 | 0.365 | 0.537 | p < 0.0001 |
| Formulation | G1 | G2 | G3 | G4 | G5 | G6 | G7 | G8 | G9 | G10 | G11 | G12 | G13 | G14 | G15 | G16 | G17 | G18 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alginate [%] | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 |
| CaCl2 [mM] | 4 | 8 | 10 | 12 | 25 | 50 | 4 | 8 | 10 | 12 | 25 | 50 | 4 | 8 | 10 | 12 | 25 | 50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, C.; Ramos-Yacasi, G.; Mallandrich, M.; Colom-Codina, H.; Suñer-Carbó, J.; Pérez-González, N.; Calpena, A.C.; Fernández-Campos, F. Alginate Hydrogel Formulation with Ketorolac for the Treatment of Pain Related Sialolithiasis. Gels 2023, 9, 415. https://doi.org/10.3390/gels9050415
Silva C, Ramos-Yacasi G, Mallandrich M, Colom-Codina H, Suñer-Carbó J, Pérez-González N, Calpena AC, Fernández-Campos F. Alginate Hydrogel Formulation with Ketorolac for the Treatment of Pain Related Sialolithiasis. Gels. 2023; 9(5):415. https://doi.org/10.3390/gels9050415
Chicago/Turabian StyleSilva, Cristina, Gladys Ramos-Yacasi, Mireia Mallandrich, Helena Colom-Codina, Joaquim Suñer-Carbó, Noelia Pérez-González, Ana Cristina Calpena, and Francisco Fernández-Campos. 2023. "Alginate Hydrogel Formulation with Ketorolac for the Treatment of Pain Related Sialolithiasis" Gels 9, no. 5: 415. https://doi.org/10.3390/gels9050415
APA StyleSilva, C., Ramos-Yacasi, G., Mallandrich, M., Colom-Codina, H., Suñer-Carbó, J., Pérez-González, N., Calpena, A. C., & Fernández-Campos, F. (2023). Alginate Hydrogel Formulation with Ketorolac for the Treatment of Pain Related Sialolithiasis. Gels, 9(5), 415. https://doi.org/10.3390/gels9050415