
MicroRNAs in Gingival Crevicular Fluid: An Observational Case-Control Study of Differential Expression in Periodontitis
 ,
,
Abstract
:1. Introduction
2. Results
2.1. Description of Patients
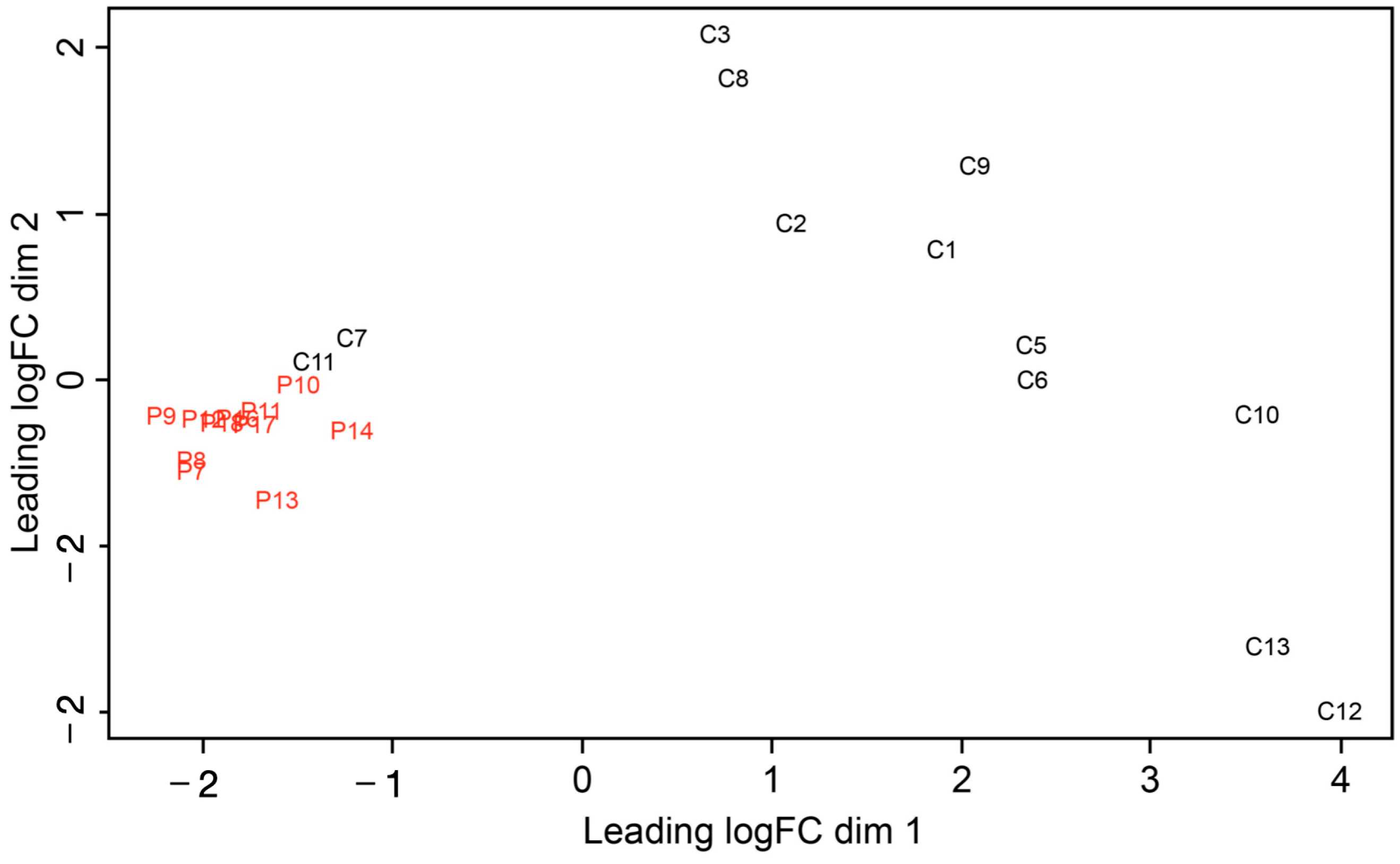
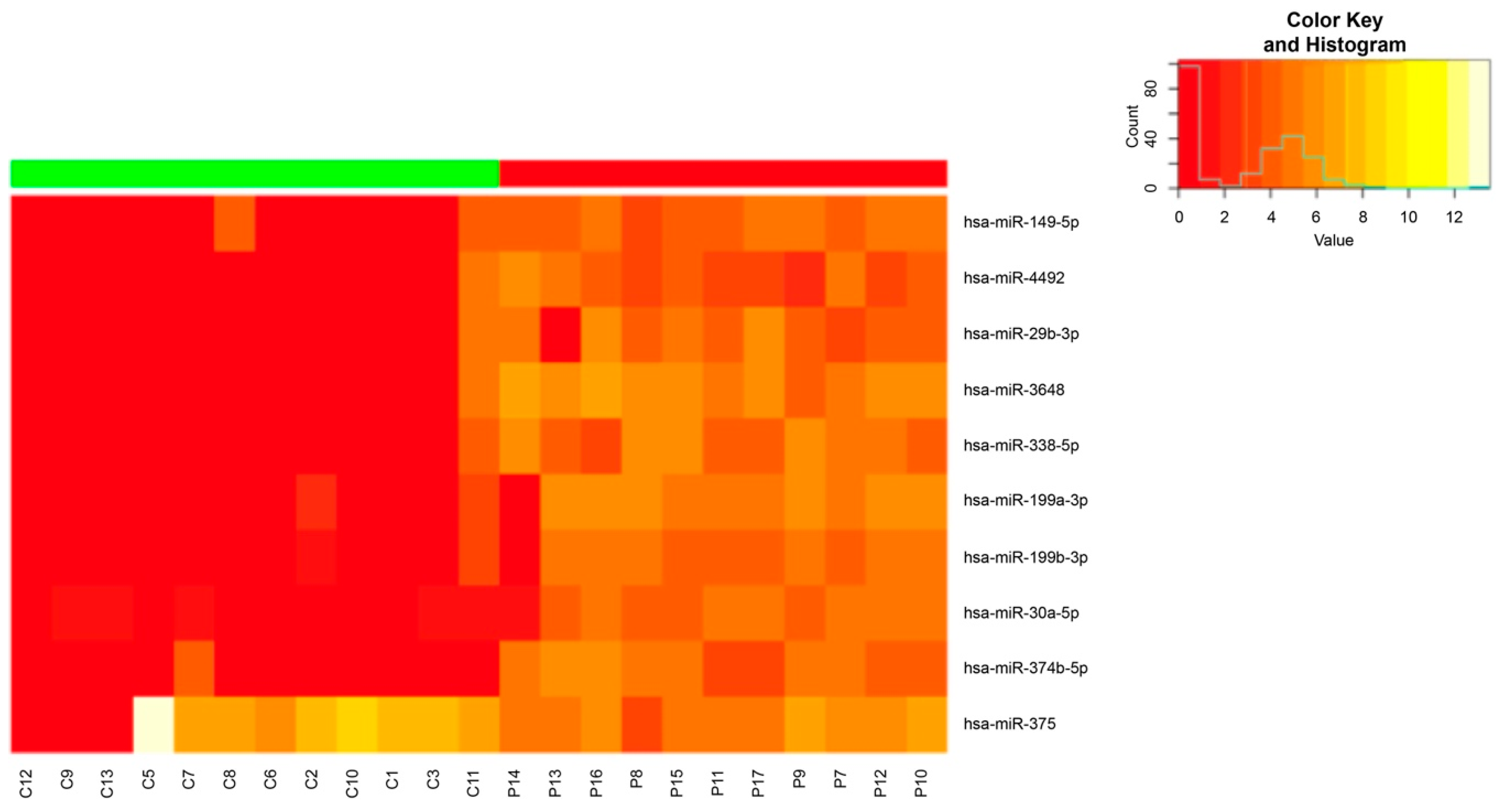
2.2. miRNA Expression Analysis in Patients with Advanced Chronic Periodontitis
2.3. Selection of Reliable miRNAs to Define Periodontitis and Its Etiopathogenesis
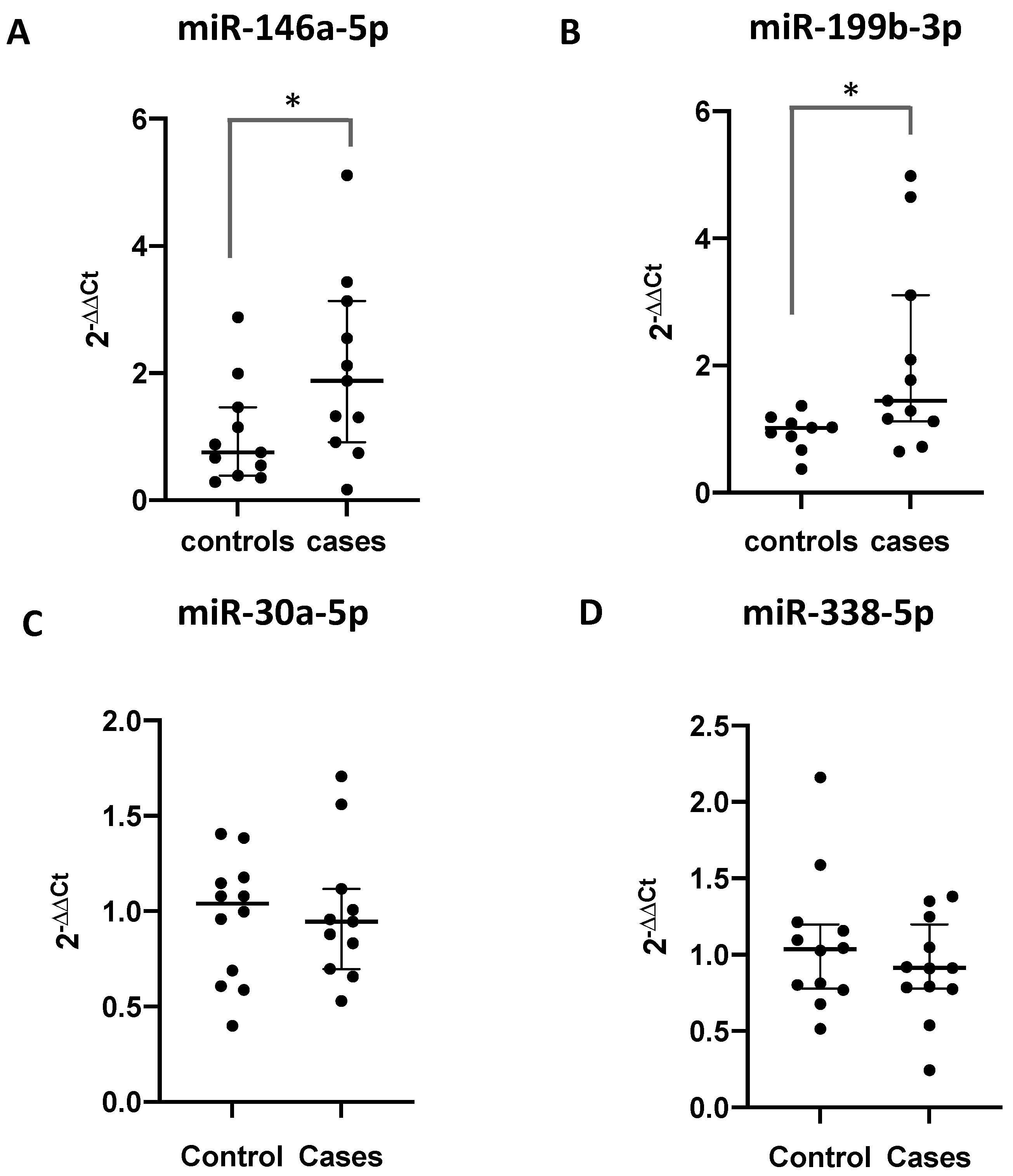
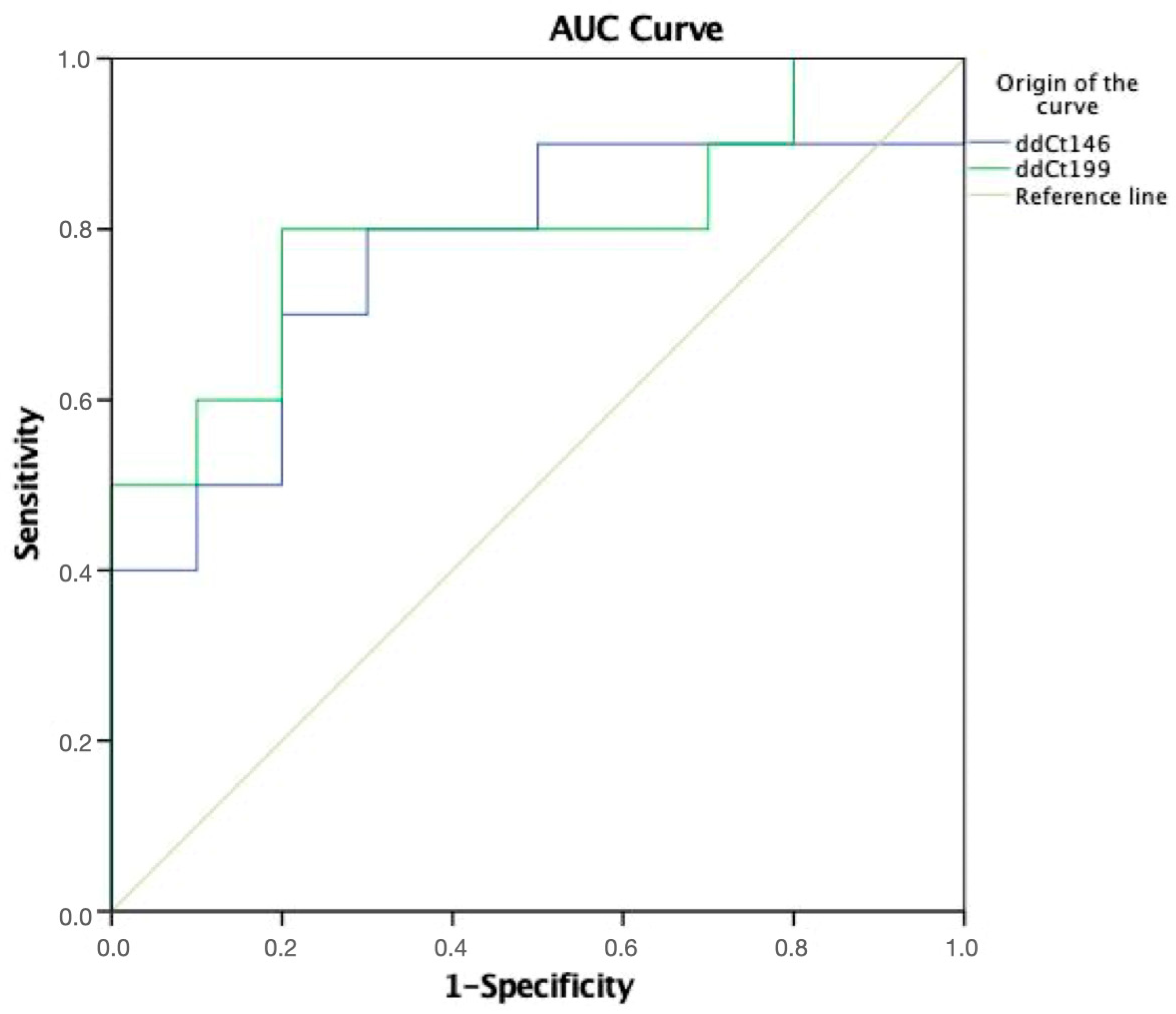
2.4. Validation of Differentially Expressed miRNAs via RT-qPCR


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| miRNA | AUC | 95% CI | p Value | Cut-Off Value | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| 146a-5p | 0.74 | 0.53–0.96 | 0.05 | 1.22 | 72.7 | 72.7 |
| 199b-3p | 0.78 | 0.57–0.99 | 0.09 | 1.11 | 80.0 | 72.7 |
2.5. Analysis of the Correlation between GCF Volume and Expression Levels of the Validated miRNAs
3. Discussion
4. Materials and Methods
4.1. Clinical Records
4.2. GCF Sample Collection and Small RNA Extraction and Quantification
4.3. Small RNA-Seq and Analysis
4.3.1. Library Preparation and Next-Generation Sequencing
4.3.2. Differential Expression Analysis between Advanced Chronic Periodontitis Patients and Healthy Subjects
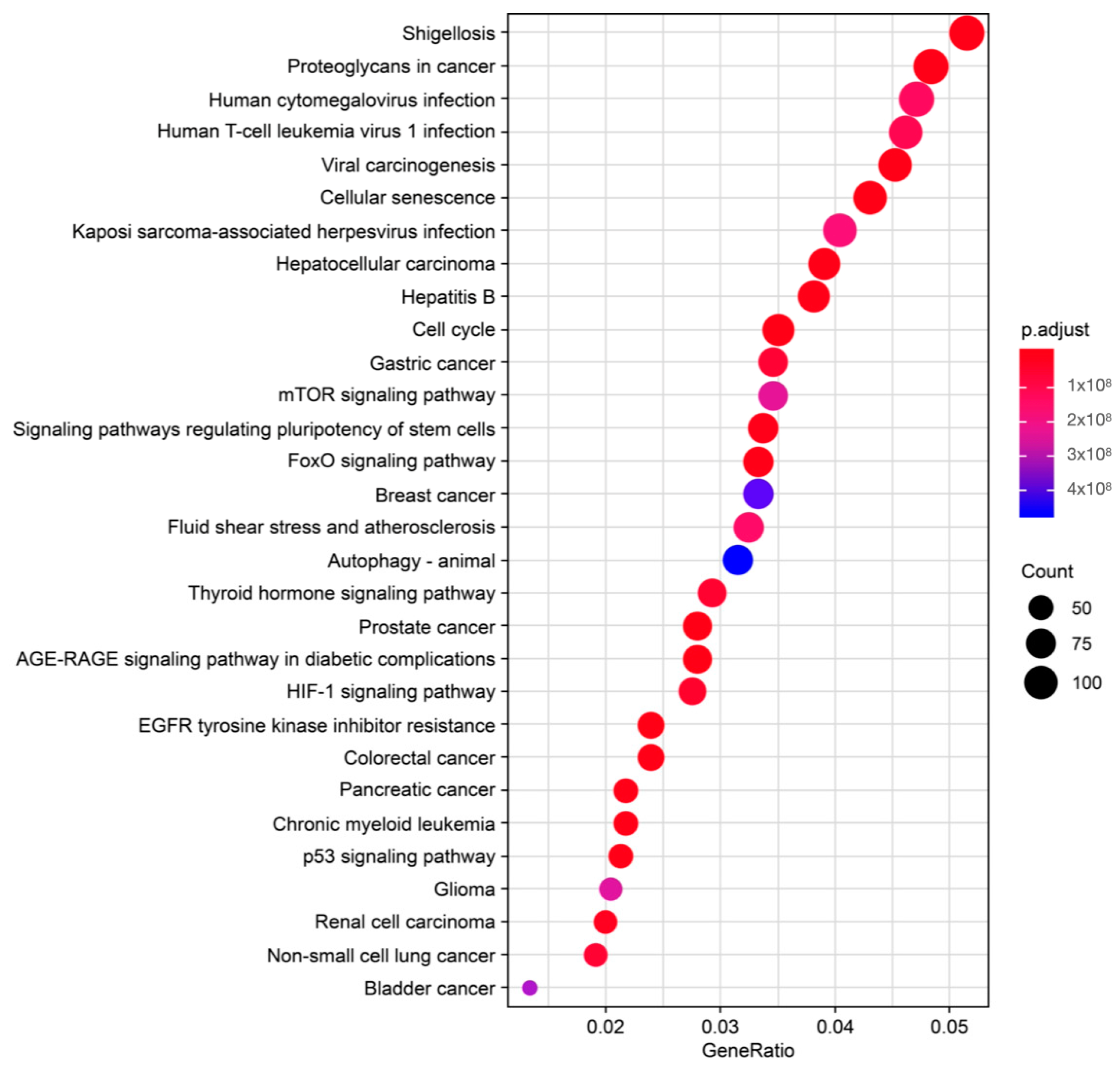
4.4. Prediction of miRNA Targets and Overrepresentation Analysis (ORA)
4.5. miRNA Validation Using Quantitative Reverse Transcription Polymerase Chain Reaction (RT-qPCR) in CSF Samples
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2016, 15, 30–44. [Google Scholar] [CrossRef]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2000 2015, 69, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, G.; Hart, T.C. A Critical Assessment of Interleukin-1 (IL-1) Genotyping When Used in a Genetic Susceptibility Test for Severe Chronic Periodontitis. J. Periodontol. 2002, 73, 231–247. [Google Scholar] [CrossRef]
- Santonocito, S.; Polizzi, A.; Palazzo, G.; Indelicato, F.; Isola, G. Dietary factors affecting the prevalence and impact of periodontal disease. Clin. Cosm. Investig. Dent. 2021, 13, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Santonocito, S.; Giudice, A.; Polizzi, A.; Troiano, G.; Merlo, E.M.; Sclafani, R.; Grosso, G.; Isola, G. A Cross-Talk between Diet and the Oral Microbiome: Balance of Nutrition on Inflammation and Immune System’s Response during Periodontitis. Nutrients 2022, 14, 2426. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Genco, R. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef]
- Linden, G.J.; Lyons, A.; Scannapieco, F.A.; Sharma, P.; Dietrich, T.; Ferro, C.J.; Cockwell, P.; Chapple, I.L.C.C.; Chapple, I.L.C.C.; Genco, R.; et al. Periodontal systemic associations: Review of the evidence. J. Clin. Periodontol. 2013, 40, 8–19. [Google Scholar] [CrossRef]
- Sharma, P.; Dietrich, T.; Ferro, C.J.; Cockwell, P.; Chapple, I.L.C. Association between periodontitis and mortality in stages 3–5 chronic kidney disease: NHANES III and linked mortality study. J. Clin. Periodontol. 2016, 43, 104–113. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Van Dyke, T.E. Periodontitis and atherosclerotic cardiovascular disease: Consensus report of the Joint EFP/AAPWorkshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S24–S29. [Google Scholar] [CrossRef]
- Stoecklin-Wasmer, C.; Guarnieri, P.; Celenti, R.; Demmer, R.T.; Kebschull, M.; Papapanou, P.N. MicroRNAs and Their Target Genes in Gingival Tissues. J. Dent. Res. 2012, 91, 934–940. [Google Scholar] [CrossRef]
- Thomson, D.W.; Bracken, C.P.; Goodall, G.J. Experimental strategies for microRNA target identification. Nucleic Acids Res. 2011, 39, 6845–6853. [Google Scholar] [CrossRef] [PubMed]
- Baek, D.; Villén, J.; Shin, C.; Camargo, F.D.; Gygi, S.P.; Bartel, D.P. The impact of microRNAs on protein output. Nature 2008, 455, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Shu, R.; Jiang, S.; Liu, D.; Zhang, X. Comparison of microRNA profiles of human periodontal diseased and healthy gingival tissues. Int. J. Oral. Sci. 2011, 3, 125–134. [Google Scholar] [CrossRef]
- García-Giménez, J.L.; Seco-Cervera, M.; Tollefsbol, T.O.; Romá-Mateo, C.; Peiró-Chova, L.; Lapunzina, P.; Pallardó, F.V. Epigenetic biomarkers: Current strategies and future challenges for their use in the clinical laboratory. Crit. Rev. Clin. Lab. Sci. 2017, 54, 529–550. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of microRNA biogenesis, mechanisms of actions, and circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Karimi, M.; Johansson, S.; Axelsson, J.; Suliman, M.; Lindholm, B.; Heimb?rger, O.; Barany, P.; Alvestrand, A.; Nordfors, L.; et al. Impact of inflammation on epigenetic DNA methylation ? a novel risk factor for cardiovascular disease? J. Intern. Med. 2007, 261, 488–499. [Google Scholar] [CrossRef]
- Ogata, Y.; Matsui, S.; Kato, A.; Zhou, L.; Nakayama, Y.; Takai, H. MicroRNA expression in inflamed and noninflamed gingival tissues from Japanese patients. J. Oral Sci. 2014, 56, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Volinia, S.; Calin, G.A.; Liu, C.-G.; Ambs, S.; Cimmino, A.; Petrocca, F.; Visone, R.; Iorio, M.; Roldo, C.; Ferracin, M.; et al. A microRNA expression signature of human solid tumors defines cancer gene targets. Proc. Natl. Acad. Sci. USA 2006, 103, 2257–2261. [Google Scholar] [CrossRef]
- De Oliveira, N.F.P.; Andia, D.C.; Planello, A.C.; Pasetto, S.; Marques, M.R.; Nociti, F.H.; Line, S.R.P.; De Souza, A.P. TLR2 and TLR4 gene promoter methylation status during chronic periodontitis. J. Clin. Periodontol. 2011, 38, 975–983. [Google Scholar] [CrossRef]
- Loo, W.T.Y.; Jin, L.; Cheung, M.N.B.; Wang, M.; Chow, L.W.C. Epigenetic change in E-cadherin and COX-2 to predict chronic periodontitis. J. Transl. Med. 2010, 8, 110. [Google Scholar] [CrossRef]
- Schaefer, A.S.; Richter, G.M.; Nothnagel, M.; Laine, M.L.; Rühling, A.; Schäfer, C.; Cordes, N.; Noack, B.; Folwaczny, M.; Glas, J.; et al. A 3′UTR transition within DEFB1 is associated with chronic and aggressive periodontitis. Genes Immun. 2010, 11, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.J.; He, L.; Yuan, M.; Tsang, W.W.N.; Hao, L.; Wang, M.; Chow, L.W.C.; Cheung, M.N.B.; Liu, Q.; Ng, E.L.Y.; et al. Epigenetic changes of TIMP-3, GSTP-1 and 14-3-3 sigma genes as indication of status of chronic inflammation and cancer. Int. J. Biol. Markers 2014, 29, e208–e214. [Google Scholar] [CrossRef]
- Zhang, S.; Barros, S.P.; Moretti, A.J.; Yu, N.; Zhou, J.; Preisser, J.S.; Niculescu, M.D.; Offenbacher, S. Epigenetic regulation of TNFA expression in periodontal disease. J. Periodontol. 2013, 84, 1606–1616. [Google Scholar] [CrossRef]
- Almiñana-Pastor, P.J.; Boronat-Catalá, M.; Micó-Martinez, P.; Bellot-Arcís, C.; Lopez-Roldan, A.; Alpiste-Illueca, F.M. Epigenetics and periodontics: A systematic review. Med. Oral Patol. Oral Cirugía Bucal 2019, 24, e659. [Google Scholar] [CrossRef] [PubMed]
- de Camargo Pereira, G.; Guimarães, G.N.; Planello, A.C.; Santamaria, M.P.; de Souza, A.P.; Line, S.R.; Marques, M.R. Porphyromonas gingivalis LPS stimulation downregulates DNMT1, DNMT3a, and JMJD3 gene expression levels in human HaCaT keratinocytes. Clin. Oral Investig. 2013, 17, 1279–1285. [Google Scholar] [CrossRef]
- Li, H.; Deng, Y.; Sun, K.; Yang, H.; Liu, J.; Wang, M.; Zhang, Z.; Lin, J. Structural basis of kindlin-mediated integrin recognition and activation. Proc. Natl. Acad. Sci. USA 2017, 114, 9349–9354. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Leidinger, P.; Bauer, A.; ElSharawy, A.; Haas, J.; Backes, C.; Wendschlag, A.; Giese, N.; Tjaden, C.; Ott, K.; et al. Toward the blood-borne miRNome of human diseases. Nat. Methods 2011, 8, 841–843. [Google Scholar] [CrossRef]
- Xie, Y.; Shu, R.; Jiang, S.; Song, Z.; Guo, Q.; Dong, J.; Lin, Z. miRNA-146 negatively regulates the production of pro-inflammatory cytokines via NF-κB signalling in human gingival fibroblasts. J. Inflamm. 2014, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- De Souza, A.P.; Planello, A.C.; Marques, M.R.; De Carvalho, D.D.; Line, S.R.P. High-throughput DNA analysis shows the importance of methylation in the control of immune inflammatory gene transcription in chronic periodontitis. Clin. Epigenetics 2014, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Uitto, V.-J. Gingival crevice fluid—An introduction. Periodontology 2000 2003, 31, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef]
- Păunică, I.; Giurgiu, M.; Dumitriu, A.S.; Păunică, S.; Pantea Stoian, A.M.; Martu, M.A.; Serafinceanu, C. The Bidirectional Relationship between Periodontal Disease and Diabetes Mellitus—A Review. Diagnostics 2023, 13, 681. [Google Scholar] [CrossRef]
- Xu, S.; Song, M.; Xiong, Y.; Liu, X.; He, Y.; Qin, Z. The association between periodontal disease and the risk of myocardial infarction: A pooled analysis of observational studies. BMC Cardiovasc. Disord. 2017, 17, 50. [Google Scholar] [CrossRef]
- Blaizot, A.; Vergnes, J.N.; Nuwwareh, S.; Amar, J.; Sixou, M. Periodontal diseases and cardiovascular events:meta-analysis of observational studies. Int. Dent. J. 2008, 58, 342–348. [Google Scholar] [CrossRef]
- Radović, N.; Nikolić Jakoba, N.; Petrović, N.; Milosavljević, A.; Brković, B.; Roganović, J. MicroRNA-146a and microRNA-155 as novel crevicular fluid biomarkers for periodontitis in non-diabetic and type 2 diabetic patients. J. Clin. Periodontol. 2018, 45, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Motedayyen, H.; Ghotloo, S.; Saffari, M.; Sattari, M.; Amid, R. Evaluation of MicroRNA-146a and Its Targets in Gingival Tissues of Patients With Chronic Periodontitis. J. Periodontol. 2015, 86, 1380–1385. [Google Scholar] [CrossRef]
- Griffiths, G.S. Formation, collection and significance of gingival crevice fluid. Periodontology 2000 2003, 31, 32–42. [Google Scholar] [CrossRef]
- Dolz, S.; Górriz, D.; Tembl, J.I.; Sánchez, D.; Fortea, G.; Parkhutik, V.; Lago, A. Circulating MicroRNAs as novel biomarkers of stenosis progression in asymptomatic carotid stenosis. Stroke 2017, 48, 10–16. [Google Scholar] [CrossRef]
- Zhu, L.; Xu, H.; Lv, W.; He, Z.; Ye, P.; Wang, Y.; Hu, J. miR-199b-5p Regulates Immune-Mediated Allograft Rejection after Lung Transplantation Through the GSK3β and NF-κB Pathways. Inflammation 2018, 41, 1524–1535. [Google Scholar] [CrossRef]
- Kadkhodazadeh, M.; Jafari, A.R.; Amid, R.; Ebadian, A.R.; Alipour, M.M.; Mollaverdi, F.; Lafzi, A. MiR146a and MiR499 gene polymorphisms in Iranian periodontitis and peri-implantitis patients. J. Long Term Eff. Med. Implant. 2013, 23, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Roldán, A.L.; Giménez, J.L.G.; Illueca, F.A. Impact of periodontal treatment on the RANKL/OPG ratio in crevicular fluid. PLoS ONE 2020, 15, e0227757. [Google Scholar] [CrossRef]
- Saito, A.; Horie, M.; Ejiri, K.; Aoki, A.; Katagiri, S.; Maekawa, S.; Suzuki, S.; Kong, S.; Yamauchi, T.; Yamaguchi, Y.; et al. MicroRNA profiling in gingival crevicular fluid of periodontitis—A pilot study. FEBS Open Bio 2017, 7, 981–994. [Google Scholar] [CrossRef] [PubMed]
- Rovas, A.; Puriene, A.; Snipaitiene, K.; Punceviciene, E.; Buragaite-Staponkiene, B.; Matuleviciute, R.; Butrimiene, I.; Jarmalaite, S. Analysis of periodontitis-associated miRNAs in gingival tissue, gingival crevicular fluid, saliva and blood plasma. Arch. Oral Biol. 2021, 126, 105125. [Google Scholar] [CrossRef]
- Rovas, A.; Puriene, A.; Snipaitiene, K.; Punceviciene, E.; Buragaite-Staponkiene, B.; Matuleviciute, R.; Butrimiene, I.; Jarmalaite, S. Gingival crevicular fluid microRNA associations with periodontitis. J. Oral Sci. 2022, 64, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Costantini, E.; Sinjari, B.; Di Giovanni, P.; Aielli, L.; Caputi, S.; Muraro, R.; Murmura, G.; Reale, M. TNFα, IL-6, miR-103a-3p, miR-423-5p, miR-23a-3p, miR-15a-5p and miR-223-3p in the crevicular fluid of periodontopathic patients correlate with each other and at different stages of the disease. Sci. Rep. 2023, 13, 126. [Google Scholar] [CrossRef]
- Zhu, J.; Zhong, Z. The expression and clinical significance of miR-30b-3p and miR-125b-1-3p in patients with periodontitis. BMC Oral Health 2022, 22, 325. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Santonocito, S.; Distefano, A.; Polizzi, A.; Vaccaro, M.; Raciti, G.; Alibrandi, A.; Li Volti, G. Impact of periodontitis on gingival crevicular fluid miRNAs profiles associated with cardiovascular disease risk. J. Periodontal Res. 2023, 58, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef] [PubMed]
- Micó-Martínez, P.; García-Giménez, J.L.; Seco-Cervera, M.; López-Roldán, A.; Almiñana-Pastor, P.J.; Alpiste-Illueca, F.; Pallardó, F.V. MiR-1226 detection in GCF as potential biomarker of chronic periodontitis: A pilot study. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e308–e314. [Google Scholar] [CrossRef]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced plaque formation by the chloromethyl analogue of victamine C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar] [PubMed]
- Liao, Y.; Smyth, G.K.; Shi, W. The Subread aligner: Fast, accurate and scalable read mapping by seed-and-vote. Nucleic Acids Res. 2013, 41, e108. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Smyth, G.K.; Shi, W. FeatureCounts: An efficient general purpose program for assigning sequence reads to genomic features. Bioinformatics 2014, 30, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.D.; Oshlack, A. A scaling normalization method for differential expresion analysis of RNA-seq data. Genome Biol. 2010, 11, R25. [Google Scholar] [CrossRef]
- Robinson, M.D.; Smyth, G.K. Small-sample estimation of negative binomial dispersion, with applications to SAGE data. Biostatistics 2008, 9, 321–332. [Google Scholar] [CrossRef]
- Robinson, M.D.; Smyth, G.K. Moderated statistical tests for assessing differences in tag abundance. Bioinformatics 2007, 23, 2881–2887. [Google Scholar] [CrossRef]
- Anders, S.; Huber, W. Differential expression analysis for sequence count data. Genome Biol. 2010, 11, R106. [Google Scholar] [CrossRef]
- Lun, A.T.L.; Mccarthy, D.J.; Marioni, J.C. A step-by-step workflow for low-level analysis of single-cell RNA-seq data with Bioconductor. F1000Research 2016, 5, 2122. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Vlachos, I.S.; Zagganas, K.; Paraskevopoulou, M.D.; Georgakilas, G.; Karagkouni, D.; Vergoulis, T.; Dalamagas, T.; Hatzigeorgiou, A.G. DIANA-miRPath v3.0: Deciphering microRNA function with experimental support. Nucleic Acids Res. 2015, 43, W460–W466. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]




| Variable | Healthy Subjects | CP Patients | p Value |
|---|---|---|---|
| CAL | 2.92 (CI 2.66–3.17) (SD ± 0.40) | 5.06 (CI 4.60–5.52) (SD ± 0.68) | p < 0.0001 |
| Mean PD | 2.29 (CI 2.14–2.44) (SD ± 0.23) | 4.04 (CI 3.76–4.31) (SD ± 0.41) | p < 0.0001 |
| Mean PI | 2.03 (CI 1.70–2.36) (SD ± 0.52) | 3.32 (CI 2.85–3.61) (SD ± 0.56) | p < 0.0001 |
| BOP percentage | 13.90% (CI 5.09–22.72) (SD ± 13.87) | 80.19% (CI 67.5–92.8) (SD ± 18.83) | p < 0.0001 |
| GCF Volume Tooth 1 | GCF Volume Tooth 2 | GCF Volume Tooth 3 | |||
|---|---|---|---|---|---|
| Rho Spearman | 2-ΔΔCt miR-146a-5p | Correlation coefficient | 0.483 * | 0.514 * | 0.561 ** |
| Sig. (bilateral) | 0.027 | 0.017 | 0.008 | ||
| n | 21 | 21 | 21 | ||
| 2-ΔΔCt miR-199b-3p | Correlation coefficient | 0.615 ** | 0.686 ** | 0.717 ** | |
| Sig. (bilateral) | 0.004 | 0.001 | 0.000 | ||
| n | 20 | 20 | 20 | ||
| 2-ΔΔCt miR-30a-5p | Correlation coefficient | 0.114 | 0.116 | 0.166 | |
| Sig. (bilateral) | 0.624 | 0.616 | 0.471 | ||
| n | 21 | 21 | 21 | ||
| 2-ΔΔCt miR-338-5p | Correlation coefficient | −0.001 | 0.024 | −0.072 | |
| Sig. (bilateral) | 0.996 | 0.914 | 0.744 | ||
| n | 23 | 23 | 23 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almiñana-Pastor, P.J.; Alpiste-Illueca, F.M.; Micó-Martinez, P.; García-Giménez, J.L.; García-López, E.; López-Roldán, A. MicroRNAs in Gingival Crevicular Fluid: An Observational Case-Control Study of Differential Expression in Periodontitis. Non-Coding RNA 2023, 9, 73. https://doi.org/10.3390/ncrna9060073
Almiñana-Pastor PJ, Alpiste-Illueca FM, Micó-Martinez P, García-Giménez JL, García-López E, López-Roldán A. MicroRNAs in Gingival Crevicular Fluid: An Observational Case-Control Study of Differential Expression in Periodontitis. Non-Coding RNA. 2023; 9(6):73. https://doi.org/10.3390/ncrna9060073
Chicago/Turabian StyleAlmiñana-Pastor, Pedro J., Francisco M. Alpiste-Illueca, Pablo Micó-Martinez, Jose Luis García-Giménez, Eva García-López, and Andrés López-Roldán. 2023. "MicroRNAs in Gingival Crevicular Fluid: An Observational Case-Control Study of Differential Expression in Periodontitis" Non-Coding RNA 9, no. 6: 73. https://doi.org/10.3390/ncrna9060073
APA StyleAlmiñana-Pastor, P. J., Alpiste-Illueca, F. M., Micó-Martinez, P., García-Giménez, J. L., García-López, E., & López-Roldán, A. (2023). MicroRNAs in Gingival Crevicular Fluid: An Observational Case-Control Study of Differential Expression in Periodontitis. Non-Coding RNA, 9(6), 73. https://doi.org/10.3390/ncrna9060073