


Social Media Devices’ Influence on User Neck Pain during the COVID-19 Pandemic: Collaborating Vertebral-GLCM Extracted Features with a Decision Tree

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
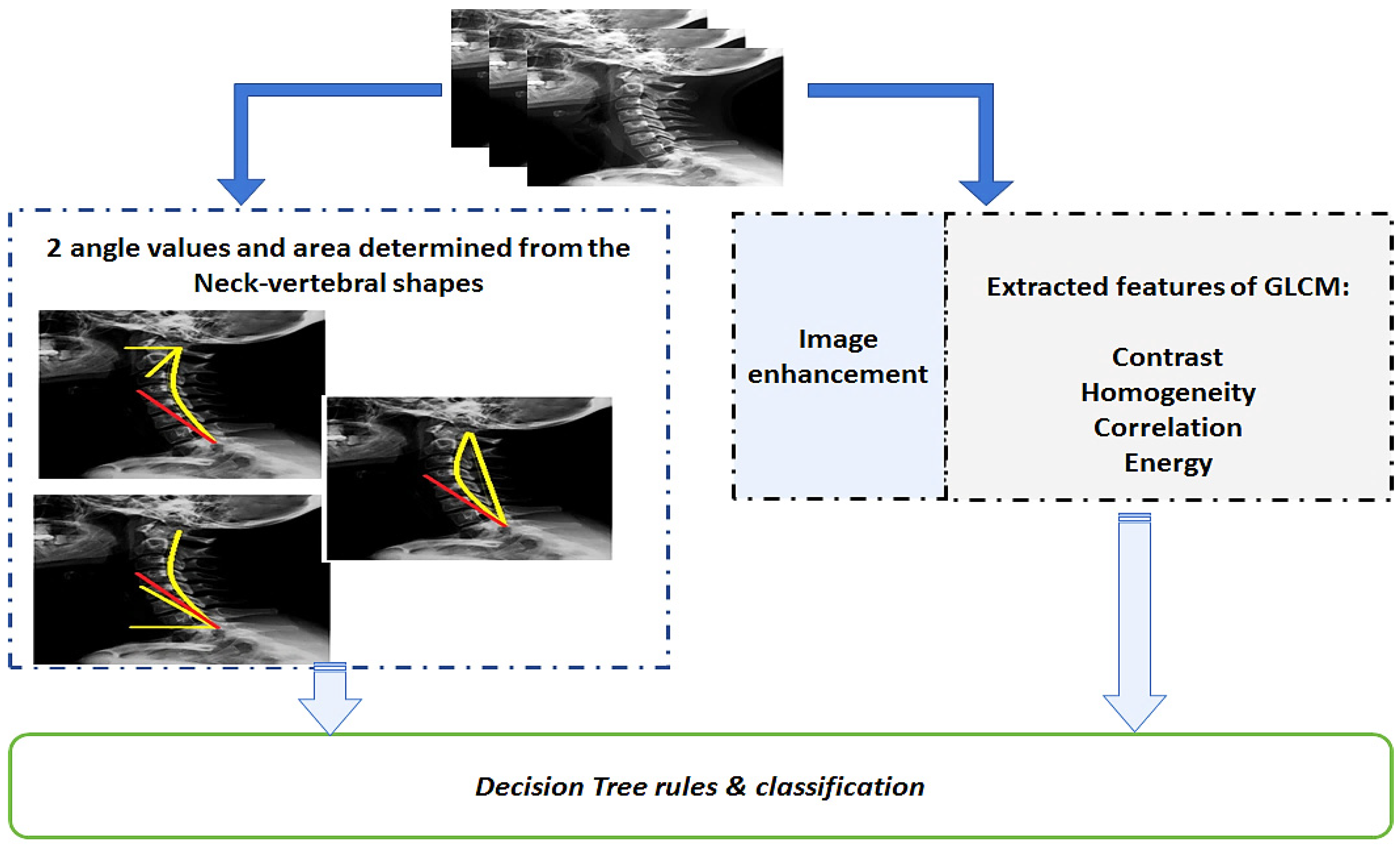
- The extracted features from X-ray retrospective images using the gray level co-occurrence matrix (GLCM);
- The two angles measured, and the related area controlled by these angles according to the inclination of the neck vertebrae for normal and abnormal cases (i.e., patients with perceived neck pain);
- Information about the SM-usage period in hours correlated with the users’ ages. Nine inputs or information were provided to the decision tree (DT) to predict the conditions that may lead to muscle fatigue or produce neck pain;
- The DT classifier (provided by the Weka package, University of Waikato, New Zealand) can reduce the bias (noise) produced by unbalanced samples. The final phase of this framework is a new, predictive mathematical model utilizing a gene-expression programming (GEP) tool to define the class (normal or abnormal) to which each patient belongs using a MATLAB-based, graphical user interface to support the orthopedic doctor.
Related Works
2. Materials and Methods
2.1. Data Collection and Study Design
2.2. Ethical Approval
2.3. Inclusion and Exclusion Criteria
- (i)
- To restore balance in the training set and avoid the creation of bias in the first place, it is possible to under-sample the large class or to over-sample the small class [37];
- (ii)
- Alternately, one can change the costs (shift matrix) associated with misclassification in order to prevent any bias [37];
- (iii)
- A further precaution is to replace precision with so-called balanced accuracy [37].
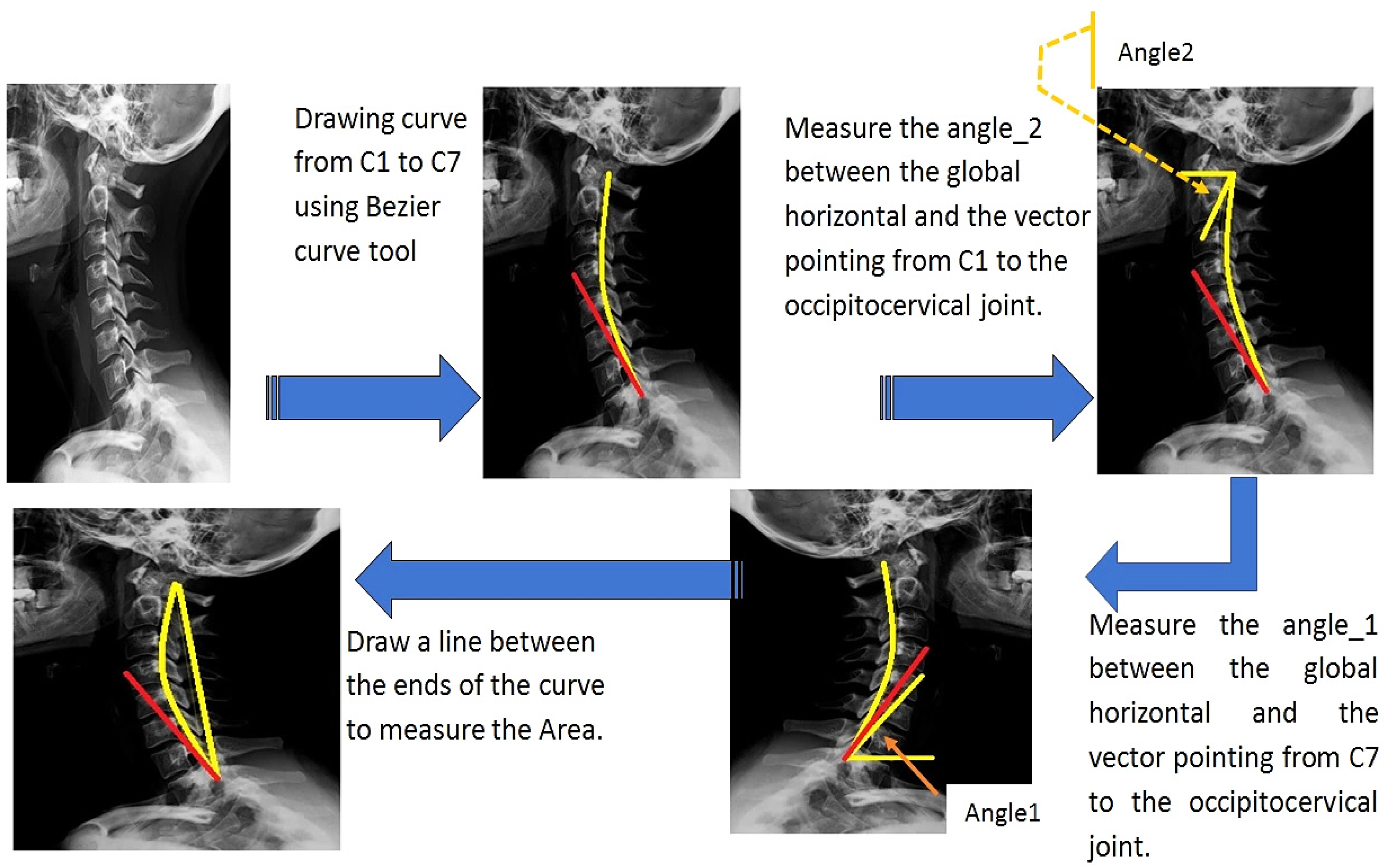
2.4. Angles and Area Measurement
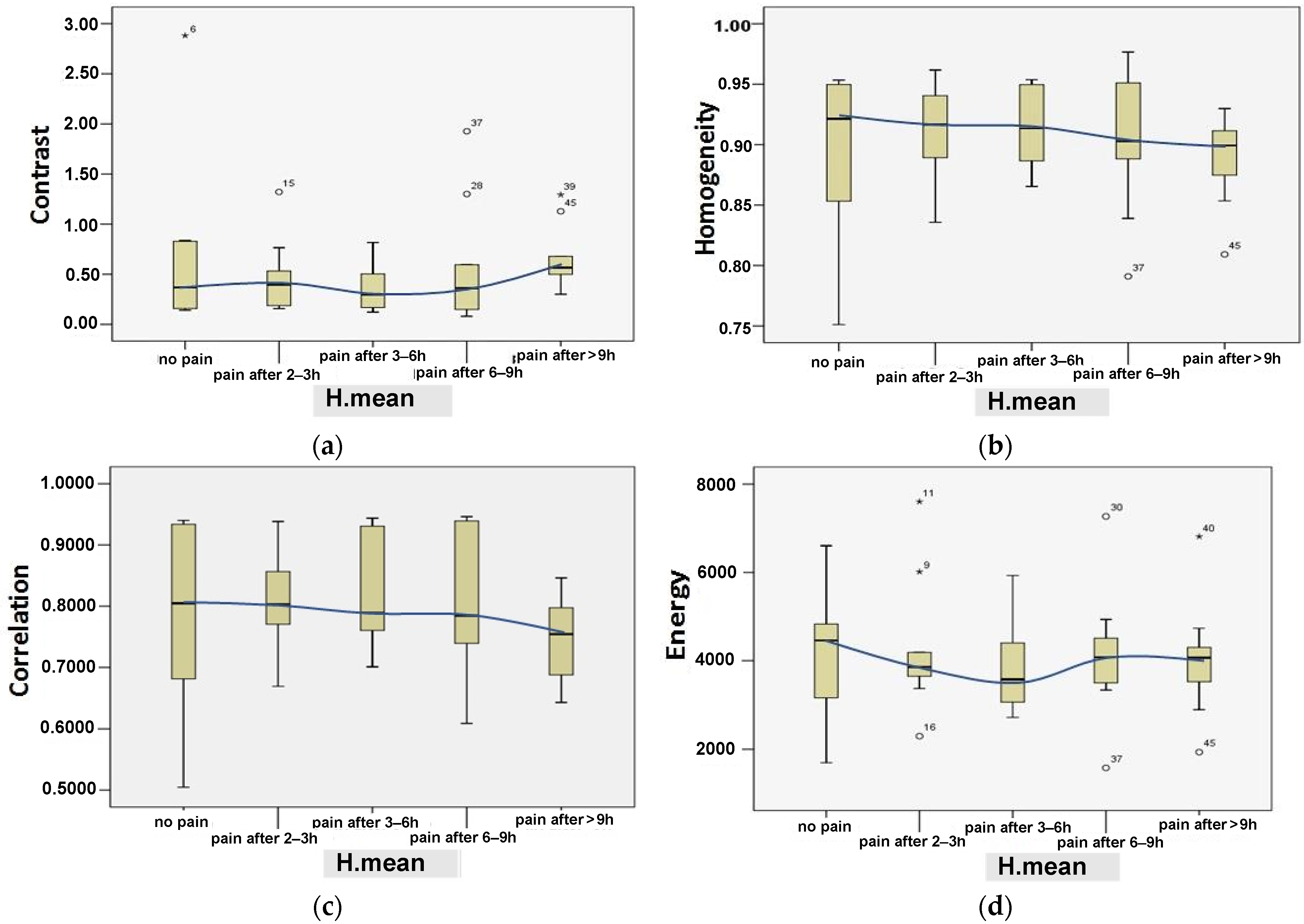
2.5. Features Extraction from the Gray Level Co-Occurrence Matrix
- (i)
- Contrast: the separation between the brightest and darkest image area; namely, the difference between the highest and lowest values of the adjacent set of pixels.
- (ii)
- Homogeneity: the closeness of the distribution of elements in the GLCM to the GLCM diagonal. It is defined as:
- (iii)
- Correlation: the linear dependency of gray levels on those of neighboring pixels. This indicates that there is a predictable and linear relationship between two neighboring pixels within the window, expressed by the regression equation. The correlation can be represented mathematically as:
- (iv) Energy: computed as the square root of an angular second moment:
- (1)
- Adjusting the contrast and brightness of the image; cropping to specify the position of the neck;
- (2)
- Magnification of the image and freehand selection of the vertebrae;
- (3)
- Smoothing many times and improving the image sharpness;
- (4)
- Finding the edges of the vertebrae using the image edge detection method;
- (5)
- Adjusting the brightness and contrast of the image (0–108 pixels);
- (6)
- Applying the fast Fourier transform (FFT) bandpass filter to remove low and high spatial frequencies responsible for image blurring [42]. This filter has been designed to smooth variations of the X-ray image (bright or dark patches) with sizes larger than 40 pixels and to strongly attenuate insignificant spots smaller than 3 pixels. Note that these values are half the spatial frequencies of the actual cutoff frequency. The cutoff frequency is very soft, so the bandpass filter will also significantly attenuate the spatial frequencies in the center of the bandpass unless the difference between the two values is greater than a factor of five or so. It can also suppress the horizontal or vertical stripes created by scanning an image line by line with a direction tolerance of 5%;
- (7)
- Further adjusting to the brightness and contrast of the image;
- (8)
- Resizing the image size to 256 × 256 pixels and completing a gray-scale conversion;
- (9)
- Applying the GLCM method using Matlab software (version. R2022a, MathWorks, Inc., Natick, MA, US) to extract contrast, homogeneity, correlation, and energy parameters.
2.6. Descriptive Variables
2.7. Decision Trees
2.8. Mathematical Predictive Model for the Neck Pain Diagnosis
3. Results
3.1. Results of Statistical Validation for the Objectively Calculated Parameters
3.2. Results of Using the Decision Tree Method
- −
- TP: true positive represents a case or patient with neck pain (abnormal) detected correctly;
- −
- FP: false positive represents a case or patient without neck pain (normal) detected as abnormal (perceived neck pain);
- −
- TN: true negative represents a case or patient without neck pain (normal) detected correctly;
- −
- FN: false negative represents a case or patient with neck pain (abnormal) detected as normal (no perceived neck pain).
3.3. Results from the Developed Graphical GEP Predictive Model
- −
- TP = 8, when the patient condition (as reported in the questionnaire) is normal (i.e., no perceived pain, value 1) and the predicted class is normal (namely, H value ≥ 0.5);
- −
- TN = 34, when the patient condition (as reported in the questionnaire) is abnormal (i.e., perceived neck pain) and the predicted class is also abnormal (i.e., H value < 0.5);
- −
- FP = 4, when the patient condition (as reported in the questionnaire) is abnormal (i.e., perceived neck pain) and the predicted class (by the GEP prediction model) is normal (namely, H value ≥ 0.5);
- −
- FN = 0; when the patient condition (as reported in the questionnaire) is normal (i.e., no perceived pain, value 1) and the predicted class is abnormal (H value < 0.5).
3.4. Further Comorbidities
4. Discussion
- (1)
- New quantitative parameters have been proposed for studying or evaluating the effect of SM devices on their users’ neck muscles;
- (2)
- The ability to use the DT rules increases the prediction of neck pain;
- (3)
- The geometric measures of neck postures may increase the pain prediction;
- (4)
- (5)
- This research activity was approached objectively rather than subjectively. The number of input parameters received from retrospective X-ray images was seven (angle_1, angle_2, area, contrast, homogeneity, correlation, and energy), while the remaining parameters (age and H.mean—just two) were gathered through patient questionnaire (survey) forms. In percentage terms, compared to the total number of parameters considered (nine), they correspond to 77.7% and 22.2%, respectively.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Acronym | Meaning and Definition |
| Angle_1 | The neck-flexion angle between the global horizontal and the vector pointing from C7 vertebra to the occipito-cervical joint. |
| Angle_2 | The neck-flexion angle between the global horizontal and the vector pointing from C1 vertebra to the occipito-cervical joint. |
| C1, C7 | Neck vertebrae |
| C4.5 | DT algorithm named C4.5 |
| DT | Decision tree |
| E | Entropy |
| FFT | Fast Fourier transform |
| FN | False negative |
| FP | False positive |
| GLCM | Gray-level co-occurrence matrix (GLCM) |
| IG | Information gain |
| ML | Machine learning |
| NDI | Neck disability index |
| NP | Neck pain |
| RMSE | Root mean square error |
| ROC | Receiver operating characteristic |
| SM | Social media |
| Std. Error | Standard error |
| STDev | Standard deviation |
| TN | True negative |
| TP | True positive |
| VAS | Visual analogue scale |
| WHO | World health organization |
References
- Daily Social Media Usage Worldwide 2012–2022, Published by S. Dixon. March 2022. Available online: https://www.statista.com/statistics/433871/daily-social-media-usage-worldwide/#statisticContainer (accessed on 4 April 2022).
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Smith, L. Computer-Related Musculoskeletal Dysfunction among Adolescent School Learners in the Cape Metropolitan Regionle, Stellenbosch University. 2007. Available online: https://scholar.sun.ac.za/handle/10019.1/1545 (accessed on 1 September 2021).
- Kubin, E.; Von Sikorski, C. The role of (social) media in political polarization: A systematic review. Ann. Int. Commun. Assoc. 2021, 45, 188–206. [Google Scholar] [CrossRef]
- Kamper, S.J.; Henschke, N.; Hestbaek, L.; Dunn, K.M.; Williams, C.M. Musculoskeletal pain in children and adolescents. Braz. J. Phys. Ther. 2016, 20, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Simon, L.S. Relieving Pain In America: A Blueprint For Transforming Prevention, Care, Education, and Research. J. Pain Palliat. Care Pharmacother. 2012, 26, 197–198. [Google Scholar] [CrossRef]
- De Fazio, R.; Carrasco, M.; Giannoccaro, N.I.; Velázquez, R.; Visconti, P. Wearable devices and IoT applications for symptom detection, infection tracking, and diffusion containment of the COVID-19 pandemic: A survey. Front. Inf. Technol. Electron. Eng. 2021, 22, 1413–1442. [Google Scholar] [CrossRef]
- De Fazio, R.; Sponziello, A.; Cafagna, D.; Velazquez, R.; Visconti, P. An overview on technologies and devices against Covid-19 pandemic diffusion: Virus detection and monitoring solutions. Int. J. Smart Sens. Intell. Syst. 2021, 14, 1–28. [Google Scholar] [CrossRef]
- Yang, H.; Wang, J.J.; Tng, G.Y.Q.; Yang, S. Effects of social media and smartphone use on body esteem in female adolescents: Testing a cognitive and affective model. Children 2020, 7, 148. [Google Scholar] [CrossRef]
- Naslund, J.A.; Bondre, A.; Torous, J.; Aschbrenner, K.A. Social Media and Mental Health: Benefits, Risks, and Opportunities for Research and Practice. J. Technol. Behav. Sci. 2020, 5, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, R.J.; Mandrekar, J.; Ward, A.; Aase, L.A.; Lanier, W.L.; Farris, K.T.; Gerber, T.C. Effect of Promotion via Social Media on Access of Articles in an Academic Medical Journal: A Randomized Controlled Trial. Acad. Med. 2019, 94, 1546–1553. [Google Scholar] [CrossRef] [Green Version]
- Pereira, A.; Miller, T.; Huang, Y.M.; Odell, D.; Rempel, D. Holding a tablet computer with one hand: Effect of tablet design features on biomechanics and subjective usability among users with small hands. Ergonomics 2013, 56, 1363–1375. [Google Scholar] [CrossRef]
- Farra, N.; El-Sayed, B.; Moacdieh, N.; Hajj, H.; Hajj, Z.; Haidar, R. A mobile sensing and imaging system for real-time monitoring of spine health. J. Med. Imaging Health Inform. 2011, 1, 238–245. [Google Scholar] [CrossRef]
- Al Otaibi, B.D.; Alamri, R.D.; Alzahrani, M.A.; Albalawi, R.M.; Alzhrani, K.A.; Alzahrani, K.T. Neck Pain among Medical Students during COVID-19 Pandemic: A Questionnaire Based Study. J. Pharm. Res. Int. 2021, 33, 178–184. [Google Scholar] [CrossRef]
- Riziq, G.; Mustafa, A. The Use of Smartphones in Distance Learning/E-Learning/Online Classes and its Impact to Neck Pain in the Light of the Covid-19 Pandemic. Psychol. Educ. J. 2020, 57, 1988–1999. [Google Scholar] [CrossRef]
- Roggio, F.; Trovato, B.; Ravalli, S.; Di Rosa, M.; Maugeri, G.; Bianco, A.; Palma, A.; Muumeci, G. One year of COVID-19 pandemic in Italy: Effect of sedentary behavior on physical activity levels and musculoskeletal pain among university students. Int. J. Environ. Res. Public Health 2021, 18, 8680. [Google Scholar] [CrossRef]
- Shah, M.; Desai, R. Prevalence of Neck Pain and Back Pain in Computer Users Working from Home during COVID-19 Pandemic: A Web-Based Survey. Int. J. Health Sci. Res. 2021, 11, 26–31. [Google Scholar]
- Kakar, R.S.; Lomond, K. Can COVID-19 Lead to Another Pandemic of Back Pain? Arch. Phys. Med. Rehabil. 2020, 101, e132. [Google Scholar] [CrossRef]
- Angotti, M.; Mallow, G.M.; Wong, A.; Haldeman, S.; An, H.S.; Samartzis, D. COVID-19 and Its Impact on Back Pain. Glob. Spine J. 2022, 12, 5–7. [Google Scholar] [CrossRef]
- Chen, R.; Wang, K.; Yu, J.; Howard, D.; French, L.; Chen, Z.; Wen, C.; Xu, Z. The Spatial and Cell-Type Distribution of SARS-CoV-2 Receptor ACE2 in the Human and Mouse Brains. Front. Neurol. 2021, 11, 5–7. [Google Scholar] [CrossRef]
- KV, B.M.; Walarine, M.T. Neck Pain among Smartphone Users: An Imminent Public Health Issue during the Pandemic Time. J. Ideas Health 2020, 3, 201–204. [Google Scholar] [CrossRef]
- Dos Santos, I.N.; Pernambuco, M.L.; Da Silva, A.M.B.; Ruela, G.D.A.; De Oliveira, A.S. Association between Musculoskeletal Pain and Telework in the Context of the COVID-19 Pandemic: An Integrative Review. Rev. Bras. De Med. Do Trab. 2021, 19, 342–350. [Google Scholar] [CrossRef]
- Zyznawska, J.M.; Bartecka, W.M. Remote Working Forced by COVID-19 Pandemic and Its Influence on Neck Pain and Low Back Pain among Teachers. Med. Pr. 2021, 72, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Yaseen, Q.B.; Salah, H. The Impact of E-Learning during COVID-19 Pandemic on Students’ Body Aches in Palestine. Sci. Rep. 2021, 11, 22379. [Google Scholar] [CrossRef] [PubMed]
- Daher, A.; Halperin, O. Association between Psychological Stress and Neck Pain among College Students during the Coronavirus Disease of 2019 Pandemic: A Questionnaire-Based Cross-Sectional Study. Healthcare 2021, 9, 1526. [Google Scholar] [CrossRef] [PubMed]
- Houle, M.; Lessard, A.; Marineau-Bélanger, É.; Lardon, A.; Marchand, A.A.; Descarreaux, M.; Abboud, J. Factors Associated with Headache and Neck Pain among Telecommuters—A Five Days Follow-Up. BMC Public Health 2021, 21, 1086. [Google Scholar] [CrossRef]
- Arteaga, S.; Chevalier, J.; Coile, A.; William Hill, A.; Sali, S.; Sudhakhrisnan, S.; Kurniawan, S. Low-cost accelerometry-based posture monitoring system for stroke survivors. In Proceedings of the 10th International ACM SIGACCESS Conference on Computers and Accessibility, ASSETS 2008, Halifax, NS, Canada, 13–15 October 2008; pp. 243–244. [Google Scholar] [CrossRef]
- El-Sayed, B.; Farra, N.; Moacdieh, N.; Hajj, H.; Haidar, R.; Hajj, Z. A novel mobile wireless sensing system for realtime monitoring of posture and spine stress. In Proceedings of the 2011 1st Middle East Conference on Biomedical Engineering, Sharjah, United Arab Emirates, 21–24 February 2011. [Google Scholar] [CrossRef]
- Baek, J.; Yun, B.J. Posture monitoring system for context awareness in mobile computing. IEEE Trans. Instrum. Meas. 2010, 59, 1589–1599. [Google Scholar] [CrossRef]
- Burgess-Limerick, R.; Mon-Williams, M.; Coppard, V.L. Visual display height. Hum. Factors 2000, 42, 140–150. [Google Scholar] [CrossRef]
- Mon-Williams, M.; Burgess-Limerick, R.; Plooy, A.; Wann, J. Vertical gaze direction and postural adjustment: An extension of the Heuer model. J. Exp. Psychol. Appl. 1999, 5, 35–53. [Google Scholar] [CrossRef]
- Sommerich, C.M.; Joines, S.M.; Psihogios, J.P. Effects of computer monitor viewing angle and related factors on strain, performance, and preference outcomes. Hum. Factors 2001, 43, 39–55. [Google Scholar] [CrossRef]
- Seghers, J.; Jochem, A.; Spaepen, A. Posture, muscle activity and muscle fatigue in prolonged VDT work at different screen height settings. Ergonomics 2003, 46, 714–730. [Google Scholar] [CrossRef]
- Jaschinski, W.; Heuer, H.; Kylian, H. Preferred position of visual displays relative to the eyes: A field study of visual strain and individual differences. Ergonomics 1998, 41, 1034–1049. [Google Scholar] [CrossRef]
- Straker, L.M.; Smitha, A.J.; Bear, N.; O’Sullivan, P.B.; De Klerk, N.H. Neck/shoulder pain, habitual spinal posture and computer use in adolescents: The importance of gender. Ergonomics 2011, 54, 539–546. [Google Scholar] [CrossRef]
- Straker, L.M.; O’Sullivan, P.B.; Smith, A.; Perry, M. Computer use and habitual spinal posture in Australian adolescents. Public Health Rep. 2007, 122, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Brodersen, K.H.; Ong, C.S.; Stephan, K.E.; Buhmann, J.M. The Balanced Accuracy and Its Posterior Distribution. In Proceedings of the 2010 20th International Conference on Pattern Recognition, Istanbul, Turkey, 23–26 August 2010; pp. 3121–3124. [Google Scholar] [CrossRef]
- Package weka.classifiers.trees.j48—Weka Software, University of Waikato, New Zealand. Available online: https://weka.sourceforge.io/doc.dev/weka/classifiers/trees/j48/package-summary.html (accessed on 18 July 2022).
- Lu, M.; Liu, Y.; He, W.; Li, X. Skin Roughness Evaluation Method Based on gray level co-occurrence matrix. In Proceedings of the 2019 Chinese Control and Decision Conference (CCDC), Nanchang, China, 3–5 June 2019; IEEE: Piscataway, NJ, USA. [CrossRef]
- Bae, J.S.; Lee, S.H.; Choi, K.S.; Kim, J.O. Robust skin-roughness estimation based on co-occurrence matrix. J. Vis. Commun. Image Represent. 2017, 46, 13–22. [Google Scholar] [CrossRef]
- Giavazzi, F.; Edera, P.; Lu, P.J.; Cerbino, R. Image windowing mitigates edge effects in Differential Dynamic Microscopy. Eur. Phys. J. 2017, 40, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rha, E.Y.; Kim, J.M.; Yoo, G. Volume Measurement of Various Tissues Using the Image J Software. J. Craniofacial Surg. 2015, 26, e505–e506. [Google Scholar] [CrossRef] [PubMed]
- Pontes-Silva, A.; Avila, M.A.; Fidelis-de-Paula-Gomes, C.A.; Dibai-Filho, A.V. The Short-Form Neck Disability index has adequate measurement properties in chronic neck pain patients. Eur. Spine J. 2021, 30, 3593–3599. [Google Scholar] [CrossRef]
- Firouzi, F.; Rashidi, M.; Hashemi, S.; Kangavari, M.; Bahari, A.; Daryani, N.E.; Emam, M.M.; Naderi, N.; Shalmani, H.M.; Farnood, A.; et al. A decision tree-based approach for determining low bone mineral density in inflammatory bowel disease using WEKA software. Eur. J. Gastroenterol. Hepatol. 2007, 19, 1075–1081. [Google Scholar] [CrossRef]
- Badr, B. Implementation of Decision Trees for Embedded Systems. Ph.D. Thesis, Loughborough University, Loughborough, UK, 2014. Available online: https://repository.lboro.ac.uk/articles/thesis/Implementation_of_decision_trees_for_embedded_systems/9540221 (accessed on 1 September 2021).
- Carter, T. An Introduction to Information Theory and Entropy. 2011. Available online: http://astarte.csustan.edu/~tom/SFI-CSSS/info-theory/info-lec.pdf (accessed on 10 January 2022).
- Quinlan, J.R. Induction of Decision Trees. Mach. Learn. 1986, 1, 81–106. [Google Scholar] [CrossRef] [Green Version]
- Salzberg, S.L. C4.5: Programs for Machine Learning by J. Ross Quinlan. Morgan Kaufmann Publishers, Inc., 1993. Mach. Learn. 1994, 16, 235–240. [Google Scholar] [CrossRef] [Green Version]
- Shannon, C.E. A Mathematical Theory of Communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, C. Gene expression programming: A new adaptive algorithm for solving problems. Complex Syst. 2001, 13, 87–129. [Google Scholar] [CrossRef]
- Al-Hadidi, F.; Bsisu, I.; AlRyalat, S.A.; Al-Zu’Bi, B.; Bsisu, R.; Hamdan, M.; Kanaan, T.; Yasin, M.; Samarah, O. Association between mobile phone use and neck pain in university students: A crosssectional study using numeric rating scale for evaluation of neck pain. PLoS ONE 2019, 14, e0217231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barassi, G.; Di Simone, E.; Galasso, P.; Cristiani, S.; Supplizi, M.; Kontochristos, L.; Colarusso, S.; Visciano, C.P.; Marano, P.; Antonella, D.I.; et al. Posture and Health: Are the Biomechanical Postural Evaluation and the Postural Evaluation Questionnaire Comparable to and Predictive of the Digitized Biometrics Examination? Int. J. Environ. Res. Public Health 2021, 18, 3507. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Kim, C.-J.; Son, S.-M. Neck Pain in Adults with Forward Head Posture: Effects of Craniovertebral Angle and Cervical Range of Motion. Osong Public Health Res. Perspect. 2018, 9, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Widhiyanto, A.; Munawir, A.; Prayitno, H. The Effect of Duration of Smartphone Usage on Neck Pain. Dama Int. J. Res. (DIJR) 2017, 2, 54–61. [Google Scholar]
- Lee, H.; Lee, S.; Choi, Y.S.; Seo, Y.; Shim, E. A new posture monitoring system for preventing physical illness of smartphone users. In Proceedings of the 2013 IEEE 10th Consumer Communications and Networking Conference (CCNC), Las Vegas, NV, USA, 11–14 January 2013. [Google Scholar] [CrossRef]
- Fryman, S.; Romine, W. Measuring Smartphone Dependency and Exploration of Consequences and Comorbidities. Comput. Hum. Behav. Rep. 2021, 4, 100108. [Google Scholar] [CrossRef]
- Zafar, H.; Albarrati, A.; Alghadir, A.H.; Iqbal, Z.A. Effect of Different Head-Neck Postures on the Respiratory Function in Healthy Males. BioMed Res. Int. 2018, 2018, 4518269. [Google Scholar] [CrossRef]
- Harris, C.; Straker, L.; Pollock, C.; Smith, A.J. Children, computer exposure and musculoskeletal outcomes: The development of pathway models for school and home computer-related musculoskeletal outcomes. Ergonomics 2015, 58, 1611–1623. [Google Scholar] [CrossRef]
- Brun Sundblad, G.M.; Saartok, T. Prevalence and co-occurrence of self-rated pain and perceived health in schoolchildren: Age and gender differences. Eur. J. Pain 2007, 11, 171–180. [Google Scholar] [CrossRef]
- Fichtel, A. Psychosocial impact of headache and comorbidity with other pains among Swedish school adolescents. Headache 2002, 42, 766–775. [Google Scholar] [CrossRef] [Green Version]
- Azizur Rahman, S.; Al Marzouqi, A.; Variyath, S.; Rahman, S.; Rabbani, M.; Iqbal Ahamed, S. Effects of Social Media Use on Health and Academic Performance among Students at the University of Sharjah. In Proceedings of the IEEE 44th Annual Computers, Software, and Applications Conference (COMPSAC 2020), Madrid, Spain, 13–17 July 2020. [Google Scholar] [CrossRef]
- David, D.; Giannini, C.; Chiarelli, F.; Mohn, A. Text Neck Syndrome in Children and Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1565. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kang, H.; Shin, G. Head flexion angle while using a smartphone. Ergonomics 2015, 58, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.M.; Coleman, J.; Skoss, R.; Maslen, B.A.; Burgess-Limerick, R.; Pollock, C.M. A comparison of posture and muscle activity during tablet computer, desktop computer and paper use by young children. Ergonomics 2008, 51, 540–555. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, E.; Johnson, P.W.; Lindegård, A.; Hagberg, M. Technique, muscle activity and kinematic differences in young adults texting on mobile phones. Ergonomics 2011, 54, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.P.; Tu, C.N.; Wu, S.K.; Chien-Hsiou, L. Muscle Activity and Comfort Perception on Neck, Shoulder, and Forearm While Using a Tablet Computer at Various Tilt Angles. Int. J. Hum. Comput. Interact. 2015, 31, 769–776. [Google Scholar] [CrossRef]
- Al-Naami, B.; Fraihat, H.; Al-Nabulsi, J.; Gharaibeh, N.Y.; Visconti, P.; Al-Hinnawi, A.R. Assessment of Dual Tree Complex Wavelet Transform to improve SNR in collaboration with Neuro-Fuzzy System for Heart Sound Identification. Electronics 2022, 11, 938. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Number | Question Content | ||||
|---|---|---|---|---|---|
| 1 | Gender | ||||
| Male | Female | ||||
| 2 | Age (years) | ||||
| 16–20 | 21–30 | 31–40 | 41–50 | Above 51 | |
| 3 | Do you have diabetes? | ||||
| Yes | No | ||||
| 4 | Do you suffer from high blood pressure? | ||||
| Yes | No | ||||
| 5 | Do you browse social media? | ||||
| Yes | No | ||||
| 6 | How many hours do you spend on social media a day? | ||||
| <2 h | 2–3 h | 3–6 h | 6–9 h or more | >9 h | |
| 9 | Do you suffer from neck pain or neck tension? | ||||
| Yes | No | ||||
| 10 | What type of pain do you face when you visit doctors? The doctor can help you understand the nature and type of pain. | ||||
| Neck pain | Arthritis | Others | |||
| Pain Location | Number of Pained Patients Suffering from a Given Disease (Total Number of Patients N = 46) | Percentage of Participants Suffering from a Specific Disease Compared to the Total Number N = 46 of Participants (%) |
|---|---|---|
| Neck pain | 38 (abnormal subjects) | 82.60 |
| Shoulder pain | 9 | 19.56 |
| Back pain | 5 | 10.87 |
| Arthritis | 9 | 19.56 |
| Bone pain | 1 | 2.17 |
| Diabetic | 29 | 63.04 |
| Blood pressure | 17 | 36.95 |
| Age of the Participants (Years) | Number of Participants | Percentage with Respect to the Total Number of Participants (N = 46) |
|---|---|---|
| (20–27) | 4 | 8.70 |
| (28–35) | 21 | 45.65 |
| (36–43) | 11 | 23.91 |
| (44–51) | 8 | 17.39 |
| (52–59) | 2 | 4.35 |
| Gender | ||
| Males | 19 | 41.30 |
| Females | 27 | 58.70 |
| Subject Situation | ||
| Normal (no perceived neck pain) | 8 | 17.39 |
| Abnormal (perceived neck pain) | 38 | 82.60 |
| Neck Flexion | ||
| During the use of smartphones/handhelds, including for studying purposes (online). | 46 | 100 |
| Parameter (Unit) | N | Minimum | Maximum | Mean | Std. Deviation | |
|---|---|---|---|---|---|---|
| Statistic | Std. Error | Statistic | ||||
| Age (years) | 46 | 24.00 | 58.00 | 36.89 | 1.22 | 8.28 |
| H.mean (hour) | 46 | 0.5 | 9.0 | 2.04 | 0.21 | 1.40 |
| Angle_1 (degree) | 46 | 38.29 | 101.89 | 79.56 | 2.04 | 13.81 |
| Angle_2 (degree) | 46 | 34.24 | 74.22 | 54.19 | 1.46 | 9.87 |
| Area (mm2) | 46 | 269.00 | 1305.00 | 1007.35 | 26.29 | 178.30 |
| Contrast (pixels) | 46 | 0.08 | 2.88 | 0.55 | 0.07 | 0.52 |
| Homogeneity (pixels) | 46 | 0.75 | 0.98 | 0.90 | 0.01 | 0.05 |
| Correlation (pixels) | 46 | 0.50 | 0.95 | 0.80 | 0.02 | 0.11 |
| Energy (pixels) | 46 | 0.16 | 0.76 | 0.41 | 0.02 | 0.13 |
| Parameter | Setting |
|---|---|
| Population size (P) | 46 |
| Fitness function | ROC |
| Dependent variable (Class) | 1 |
| Independent variables | 10 |
| Number of genes | 5 |
| Function set | |
| Maximum tree depth | 10 |
| Linking function between ETs | Multiplication |
| Contributor to Class | Variable ID |
|---|---|
| Gender (male or female) | d0 |
| Patient Age | d1 |
| Time duration of social media use (H.mean) | d2 |
| Angle_1 | d3 |
| Angle_2 | d4 |
| Area | d5 |
| Contrast | d6 |
| Homogeneity | d7 |
| Correlation | d8 |
| Energy | d9 |
| Parameter | Correlation Coefficient vs. Response |
|---|---|
| Gender | −0.017 |
| Age | −0.270 |
| Time Duration of social media usage (H.mean) | −0.253 |
| Angle_1 | −0.345 |
| Angle_2 | −0.139 |
| Area | −0.369 |
| Contrast | 0.306 |
| Homogeneity | −0.258 |
| Correlation | −0.167 |
| Energy | −0.223 |
| Confusion Matrix | * Precision | * Recall | Accuracy | * F1-Score | |
|---|---|---|---|---|---|
| 13 (TP) | 1 (FN) | 0.96 | 0.94 | 94% | 0.95 |
| 0 (FP) | 2 (TN) | ||||
| Cost Matrix | Cross Validation | Percentage Split | ROC Area | Total Number of Instances | |
| 0 | 1 | 9-fold | 66% | 0.98 | 16 |
| 5 | 0 | ||||
| 1 | Social_Media_use “=1_hours” Diagnose “Normal” |
| 2 | Social_Media_use “=2_hours” Diagnose “Normal” |
| 3 | Social_Media_use “=8_10_hours” AND Age “<=27” Diagnose “Abnormal” |
| 4 | Social_Media_use “<8_10_hours” AND Age “<=27” Diagnose “Normal” |
| 5 | Social_Media_use “>2_hours and <8_10_hours” AND Age “>27” AND Contrast “<=0.1455” AND angle_1 “<=72.42” Diagnose “Normal” |
| 6 | Social_Media_use “>2_hours” AND Age “>27” AND Contrast “<=0.1455” AND angle_1 “>72.42” Diagnose “Abnormal” |
| 7 | Social_Media_use “>2_hours” AND Age “>27” AND Contrast “>0.1455” Diagnose “Abnormal” |
| Patient N. | Gender d0 | Age d1 | H.mean d2 | Angle_1 d3 | Angle_2 d4 | Area d5 | Contrast d6 | Homo-geneity d7 | Correlation d8 | Energy d9 | Input Class | GEP Model (H) | Predicted Class | Class Matching |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 29 | 3.5 | 72.42 | 41.35 | 1103 | 0.297 | 0.914 | 0.907 | 0.306 | Abnormal (0) | 0.006 | Abnormal (0) | OK (TN) |
| 2 | Male | 30 | 1.5 | 52.06 | 60.84 | 896 | 0.765 | 0.836 | 0.770 | 0.230 | Abnormal (0) | 0.028 | Abnormal (0) | OK (TN) |
| 3 | Male | 32 | 9.0 | 79.65 | 71.05 | 1012 | 1.293 | 0.854 | 0.797 | 0.407 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 4 | Male | 35 | 3.5 | 62.86 | 36.87 | 986 | 0.451 | 0.913 | 0.758 | 0.392 | Abnormal (0) | 0.004 | Abnormal (0) | OK (TN) |
| 5 | Male | 35 | 7.5 | 59.96 | 59.1 | 1279 | 0.577 | 0.881 | 0.879 | 0.382 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 6 | Male | 38 | 9.0 | 90.01 | 50.04 | 1070 | 0.550 | 0.899 | 0.846 | 0.430 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 7 | Male | 41 | 6.0 | 87.07 | 47.67 | 1009 | 1.300 | 0.839 | 0.653 | 0.399 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 8 | Male | 43 | 3.5 | 65.4 | 47.12 | 993 | 0.168 | 0.945 | 0.935 | 0.358 | Abnormal (0) | 0.028 | Abnormal (0) | OK (TN) |
| 9 | Male | 46 | 9.0 | 53.61 | 56.95 | 941 | 0.499 | 0.930 | 0.706 | 0.681 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 10 | Male | 51 | 0.5 | 70.13 | 46.61 | 939 | 0.376 | 0.899 | 0.780 | 0.386 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 11 | Male | 54 | 0.5 | 75.32 | 40.08 | 966 | 0.188 | 0.962 | 0.849 | 0.760 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 12 | Male | 58 | 0.8 | 38.29 | 38.81 | 1123 | 0.310 | 0.941 | 0.857 | 0.602 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 13 | Female | 25 | 9.0 | 89.08 | 68.77 | 1170 | 0.679 | 0.875 | 0.688 | 0.290 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 14 | Female | 27 | 9.0 | 86.97 | 52.87 | 1305 | 0.300 | 0.930 | 0.810 | 0.412 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 15 | Female | 28 | 9.0 | 77.25 | 74.22 | 1005 | 1.128 | 0.809 | 0.643 | 0.194 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 16 | Female | 28 | 8.0 | 88.87 | 71.37 | 414 | 1.926 | 0.791 | 0.609 | 0.158 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 17 | Female | 28 | 9.0 | 93.01 | 69.41 | 921 | 0.395 | 0.912 | 0.754 | 0.473 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 18 | Female | 29 | 9.0 | 93.61 | 55.29 | 1105 | 0.675 | 0.886 | 0.683 | 0.373 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 19 | Female | 30 | 7.0 | 101.89 | 68.45 | 917 | 0.149 | 0.951 | 0.934 | 0.494 | Abnormal (0) | 0.004 | Abnormal (0) | OK (TN) |
| 20 | Female | 31 | 7.0 | 84.22 | 53.13 | 1260 | 0.147 | 0.952 | 0.941 | 0.451 | Abnormal (0) | 0.003 | Abnormal (0) | OK (TN) |
| 21 | Female | 32 | 6.0 | 89.95 | 62.34 | 1094 | 0.595 | 0.893 | 0.739 | 0.350 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 22 | Female | 32 | 7.5 | 99.41 | 54.11 | 988 | 0.364 | 0.904 | 0.775 | 0.357 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 23 | Female | 32 | 9.0 | 94.01 | 58.35 | 1111 | 0.566 | 0.902 | 0.770 | 0.352 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 24 | Female | 33 | 5.6 | 91.76 | 58.65 | 1010 | 0.148 | 0.954 | 0.944 | 0.440 | Abnormal (0) | 0.016 | Abnormal (0) | OK (TN) |
| 25 | Female | 35 | 5.5 | 98.58 | 62.61 | 1064 | 0.817 | 0.866 | 0.701 | 0.272 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 26 | Female | 35 | 5.5 | 82.75 | 49.65 | 1084 | 0.503 | 0.887 | 0.761 | 0.278 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 27 | Female | 35 | 7.0 | 90.62 | 51.84 | 1116 | 0.358 | 0.902 | 0.794 | 0.333 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 28 | Female | 36 | 4.5 | 89.32 | 62.01 | 1159 | 0.247 | 0.950 | 0.789 | 0.593 | Abnormal (0) | 0.114 | Abnormal (0) | OK (TN) |
| 29 | Female | 37 | 5.5 | 89.31 | 60.28 | 1023 | 0.123 | 0.953 | 0.931 | 0.511 | Abnormal (0) | 0.093 | Abnormal (0) | OK (TN) |
| 30 | Female | 42 | 1.5 | 85.57 | 42.02 | 1080 | 0.533 | 0.889 | 0.753 | 0.385 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 31 | Female | 42 | 5.5 | 76.91 | 69.09 | 1057 | 0.605 | 0.872 | 0.778 | 0.307 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 32 | Female | 46 | 0.8 | 77.76 | 48.61 | 848 | 0.418 | 0.923 | 0.826 | 0.397 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 33 | Female | 48 | 1.5 | 90.26 | 46.14 | 1050 | 0.158 | 0.946 | 0.939 | 0.419 | Abnormal (0) | 0.001 | Abnormal (0) | OK (TN) |
| 34 | Female | 50 | 7.0 | 80.89 | 50.87 | 987 | 0.156 | 0.948 | 0.939 | 0.417 | Abnormal (0) | 0.002 | Abnormal (0) | OK (TN) |
| 35 | Male | 37 | 4.5 | 57.05 | 56.14 | 1065 | 0.142 | 0.953 | 0.931 | 0.470 | Normal (1) | 0.694 | Normal (1) | OK (TP) |
| 36 | Male | 39 | 2.5 | 60.48 | 46.15 | 1044 | 0.170 | 0.948 | 0.940 | 0.395 | Normal (1) | 1.000 | Normal (1) | OK (TP) |
| 37 | Male | 41 | 3.0 | 67.85 | 50.57 | 912 | 0.146 | 0.952 | 0.937 | 0.459 | Normal (1) | 1.000 | Normal (1) | OK (TP) |
| 38 | Male | 45 | 1.5 | 85.49 | 58.04 | 1143 | 0.265 | 0.945 | 0.846 | 0.661 | Normal (1) | 1.000 | Normal (1) | OK (TP) |
| 39 | Female | 24 | 2.5 | 79.82 | 50.52 | 1055 | 0.822 | 0.868 | 0.711 | 0.432 | Normal (1) | 0.691 | Normal (1) | OK (TP) |
| 40 | Female | 27 | 4.0 | 79.57 | 48.55 | 269 | 2.881 | 0.751 | 0.505 | 0.170 | Normal (1) | 1.000 | Normal (1) | OK (TP) |
| 41 | Female | 30 | 1.5 | 64.12 | 51.31 | 888 | 0.837 | 0.839 | 0.652 | 0.237 | Normal (1) | 0.940 | Normal (1) | OK (TP) |
| 42 | Female | 36 | 2.0 | 79.64 | 54.06 | 1067 | 0.472 | 0.898 | 0.764 | 0.497 | Normal (1) | 1.000 | Normal (1) | OK (TP) |
| 43 | Male | 35 | 7.0 | 77.17 | 52.06 | 1075 | 0.080 | 0.977 | 0.946 | 0.727 | Abnormal (0) | 0.994 | Normal (1) | Wrong (FP) |
| 44 | Male | 48 | 2.5 | 90.47 | 64.04 | 985 | 0.182 | 0.937 | 0.931 | 0.365 | Abnormal (0) | 1.000 | Normal (1) | Wrong (FP) |
| 45 | Male | 50 | 1.5 | 82.09 | 34.24 | 789 | 1.321 | 0.845 | 0.669 | 0.337 | Abnormal (0) | 1.000 | Normal (1) | Wrong (FP) |
| 46 | Female | 32 | 1.5 | 77.08 | 40.72 | 961 | 0.423 | 0.910 | 0.771 | 0.385 | Abnormal (0) | 1.000 | Normal (1) | Wrong (FP) |
| First Author, Ref. n., Year | Method Survey-Based (Subjective) or Quantitative (Objective) | Samples (Male/Female) | Evaluation Approach | Parameters # | Target of Study | |
|---|---|---|---|---|---|---|
| Machine-Learning Type | Statistics | |||||
| F. Al-Hadidi [51], 2019 | Online Questionnaire (Subjective) | 500 | None | Significant test (p < 0.001) | Two: duration, neck pain | To investigate the association between neck pain and the duration of device use, taking into consideration gender, age, and the most frequent position in which students use their devices. |
| S. A. Rahman [61], 2020 | Questionnaire (Subjective) | 300 | None | Significant test (p < 0.003) | Four: gender, age, university campus, academic year | To investigate the effects of SM use on health and academic performance of students at Sharjah University |
| D. David [62], 2021 | MRI of the cervical spine (Objective) | 1 case reported | None | None | One: neck flexion angle | To analyze the new phenomenon of the “text-neck syndrome” |
| S. Lee [63], 2014 | Three-dimensional motion capture system (Objective) | 18 | None | Significant test (p < 0.05) | One: Head flexion angle | To quantitatively assess the amount and range of head flexion of smartphone users |
| L. Straker [64], 2008 | Three-dimensional posture and muscle activity measurement (Objective) | 18 | None | Significant test (p < 0.001) | Three: working in desktop, tablet, and paper conditions and measuring the head angle | To compare the posture and muscle activity of children using a tablet computer to the posture and muscle activity of children using a desktop computer and paper technology. |
| E. Gustafsson [65], 2011 | Angle measuring system (Objective) | 56 | None | Significant test (p < 0.05) | Three: symptomatic, asymptomatic, head angle | To investigate differences in technique between young adults with and without musculoskeletal symptoms when using a mobile phone for texting, and differences in muscle activity and kinematics between different texting techniques. |
| H. Ping Chiu [66], 2015 | Angle measuring system (Objective) | 30 | Electromyography measurement | Significant test (p < 0.000) | Three: tilt angle, task type, neck muscle activity | To investigate the musculature load and comfort perception of the engaged upper extremity for three angles of viewing, and common task types performed at a computer workstation. |
| A. Widhiyanto [54], 2018 | Questionnaire (Subjective) | 979 | None | Significant test (p < 0.05) | Two: Duration, Class | To analyze the effect of duration of smartphone use on neck pain. |
| H. Lee [55], 2013 | Three-axis accelerometer (Objective) | 12 | Built-in sensors, front- faced camera, three-axis accelerometer | None | One: angle | To monitor the posture of smartphone users by built-in sensors. |
| This work | Angles measurement and X-ray images analysis (Objective) | 46 | Decision tree. Classification accuracy = 94% | Significant test | Nine: age, H.mean, angle_1, angle_2, area, contrast, homogeneity, correlation, energy | To detect neck pain by: (i) Using two angles and the area between them instead of just one angle; (ii) Applying the image statistical features (GLCM) in the same procedure; (iii) Utilizing DT algorithm; (iiii) Using a MATLAB- based GUI to help the doctor in the diagnosis of neck pain in an immediate way. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Naami, B.; Badr, B.E.A.; Rawash, Y.Z.; Owida, H.A.; De Fazio, R.; Visconti, P. Social Media Devices’ Influence on User Neck Pain during the COVID-19 Pandemic: Collaborating Vertebral-GLCM Extracted Features with a Decision Tree. J. Imaging 2023, 9, 14. https://doi.org/10.3390/jimaging9010014
Al-Naami B, Badr BEA, Rawash YZ, Owida HA, De Fazio R, Visconti P. Social Media Devices’ Influence on User Neck Pain during the COVID-19 Pandemic: Collaborating Vertebral-GLCM Extracted Features with a Decision Tree. Journal of Imaging. 2023; 9(1):14. https://doi.org/10.3390/jimaging9010014
Chicago/Turabian StyleAl-Naami, Bassam, Bashar E. A. Badr, Yahia Z. Rawash, Hamza Abu Owida, Roberto De Fazio, and Paolo Visconti. 2023. "Social Media Devices’ Influence on User Neck Pain during the COVID-19 Pandemic: Collaborating Vertebral-GLCM Extracted Features with a Decision Tree" Journal of Imaging 9, no. 1: 14. https://doi.org/10.3390/jimaging9010014
APA StyleAl-Naami, B., Badr, B. E. A., Rawash, Y. Z., Owida, H. A., De Fazio, R., & Visconti, P. (2023). Social Media Devices’ Influence on User Neck Pain during the COVID-19 Pandemic: Collaborating Vertebral-GLCM Extracted Features with a Decision Tree. Journal of Imaging, 9(1), 14. https://doi.org/10.3390/jimaging9010014