

Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
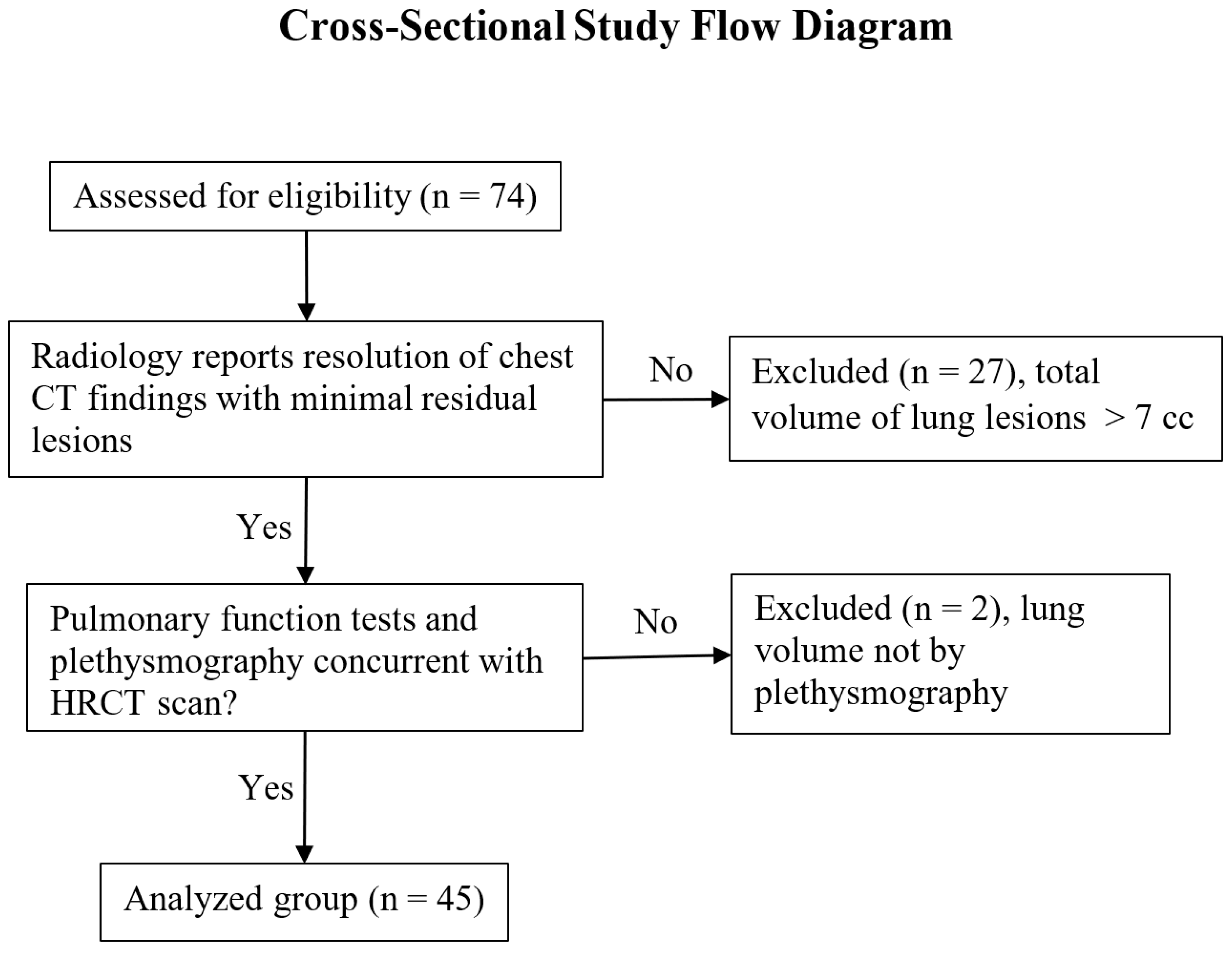
2.1. Study Population, Demographics and Pulmonary Function Tests
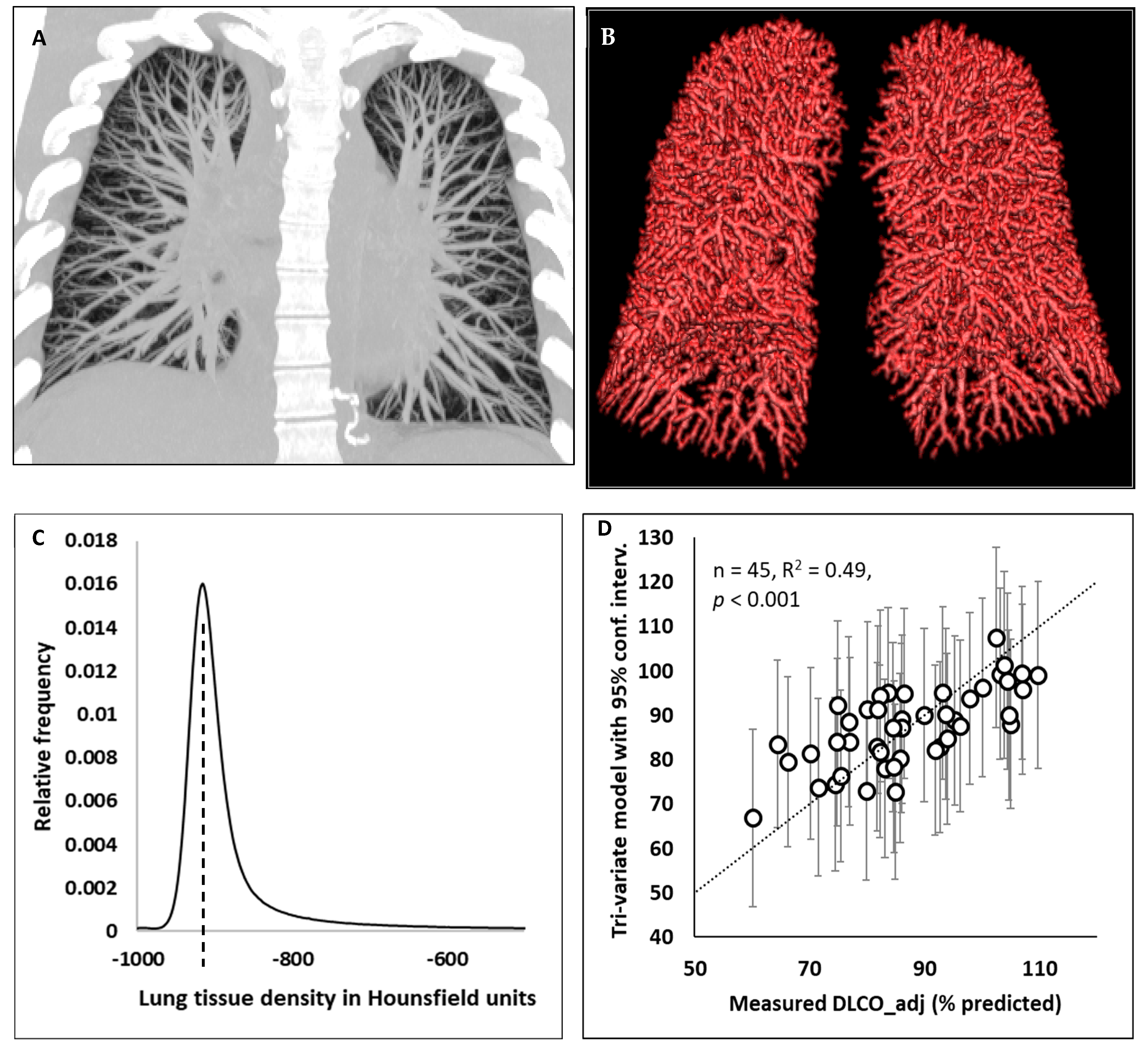
2.2. Computed Tomography Imaging Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
total non-vessel tissue volume (TissueV) = total non-vessel lung mass/(1.065 g/mL),
References
- Antoniou, K.M.; Vasarmidi, E.; Russell, A.-M.; Andrejak, C.; Crestani, B.; Delcroix, M.; Dinh-Xuan, A.T.; Poletti, V.; Sverzellati, N.; Vitacca, M.; et al. European Respiratory Society Statement on Long COVID Follow-Up. Eur. Respir. J. 2022, 60, 2102174. [Google Scholar] [CrossRef]
- Méndez, R.; Latorre, A.; González-Jiménez, P.; Feced, L.; Bouzas, L.; Yépez, K.; Ferrando, A.; Zaldívar-Olmeda, E.; Reyes, S.; Menéndez, R. Reduced Diffusion Capacity in COVID-19 Survivors. Ann. Am. Thorac. Soc. 2021, 18, 1253–1255. [Google Scholar] [CrossRef]
- Frija-Masson, J.; Debray, M.-P.; Boussouar, S.; Khalil, A.; Bancal, C.; Motiejunaite, J.; Galarza-Jimenez, M.A.; Benzaquen, H.; Penaud, D.; Laveneziana, P.; et al. Residual Ground Glass Opacities Three Months after COVID-19 Pneumonia Correlate to Alteration of Respiratory Function: The Post COVID M3 Study. Respir. Med. 2021, 184, 106435. [Google Scholar] [CrossRef]
- Huang, Y.; Tan, C.; Wu, J.; Chen, M.; Wang, Z.; Luo, L.; Zhou, X.; Liu, X.; Huang, X.; Yuan, S.; et al. Impact of Coronavirus Disease 2019 on Pulmonary Function in Early Convalescence Phase. Respir. Res. 2020, 21, 163. [Google Scholar] [CrossRef]
- Shah, A.S.; Wong, A.W.; Hague, C.J.; Murphy, D.T.; Johnston, J.C.; Ryerson, C.J.; Carlsten, C. A Prospective Study of 12-Week Respiratory Outcomes in COVID-19-Related Hospitalisations. Thorax 2021, 76, 402–404. [Google Scholar] [CrossRef]
- Faverio, P.; Luppi, F.; Rebora, P.; Busnelli, S.; Stainer, A.; Catalano, M.; Parachini, L.; Monzani, A.; Galimberti, S.; Bini, F.; et al. Six-Month Pulmonary Impairment after Severe COVID-19: A Prospective, Multicentre Follow-Up Study. Respir. Int. Rev. Thorac. Dis. 2021, 100, 1078–1087. [Google Scholar] [CrossRef]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary Recovery after COVID-19: An Observational Prospective Multicentre Trial. Eur. Respir. J. 2021, 57, 2003481. [Google Scholar] [CrossRef]
- Anastasio, F.; Barbuto, S.; Scarnecchia, E.; Cosma, P.; Fugagnoli, A.; Rossi, G.; Parravicini, M.; Parravicini, P. Medium-Term Impact of COVID-19 on Pulmonary Function, Functional Capacity and Quality of Life. Eur. Respir. J. 2021, 58, 2004015. [Google Scholar] [CrossRef]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal Pulmonary Function in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef]
- Baratella, E.; Ruaro, B.; Marrocchio, C.; Starvaggi, N.; Salton, F.; Giudici, F.; Quaia, E.; Confalonieri, M.; Cova, M.A. Interstitial Lung Disease at High Resolution CT after SARS-CoV-2-Related Acute Respiratory Distress Syndrome According to Pulmonary Segmental Anatomy. J. Clin. Med. 2021, 10, 3985. [Google Scholar] [CrossRef]
- Montesi, S.B.; Mascia, M.; Alba, G.A.; Magaletta, M.; Caravan, P.; Zhou, I. Dynamic Contrast-Enhanced Lung MRI in COVID-19 Survivors May Demonstrate Ongoing Microvascular Abnormalities. In C30. Life and Lungs after COVID: Functional Recovery and Outcomes Following SARS-CoV2 Infection; American Thoracic Society International Conference Abstracts; American Thoracic Society: New York, NY, USA, 2022; p. A3906. [Google Scholar]
- Salerno, D.; Oriaku, I.; Darnell, M.; Lanclus, M.; Backer, J.D.; Lavon, B.; Gupta, R.; Jaffe, F.; Sanchez, M.E.V.; Kim, V.; et al. Association of Abnormal Pulmonary Vasculature on CT Scan for COVID-19 Infection with Decreased Diffusion Capacity in Follow up: A Retrospective Cohort Study. PLoS ONE 2021, 16, e0257892. [Google Scholar] [CrossRef]
- Nusair, S. Abnormal Carbon Monoxide Diffusion Capacity in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 2020, 56, 2001832. [Google Scholar] [CrossRef]
- Chapman, D.G.; Badal, T.; King, G.G.; Thamrin, C. Caution in Interpretation of Abnormal Carbon Monoxide Diffusion Capacity in COVID-19 Patients. Eur. Respir. J. 2021, 57, 2003263. [Google Scholar] [CrossRef]
- Estépar, R.S.J.; Kinney, G.L.; Black-Shinn, J.L.; Bowler, R.P.; Kindlmann, G.L.; Ross, J.C.; Kikinis, R.; Han, M.K.; Come, C.E.; Diaz, A.A.; et al. Computed Tomographic Measures of Pulmonary Vascular Morphology in Smokers and Their Clinical Implications. Am. J. Respir. Crit. Care Med. 2013, 188, 231–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, R.; Tornling, G.; Forsslund, H.; Mikko, M.; Wheelock, Å.M.; Nyrén, S.; Sköld, C.M. Lung Density on High Resolution Computer Tomography (HRCT) Reflects Degree of Inflammation in Smokers. Respir. Res. 2014, 15, 23. [Google Scholar] [CrossRef] [Green Version]
- Official ERS Technical Standards: Global Lung Function Initiative Reference Values for the Carbon Monoxide Transfer Factor for Caucasians|European Respiratory Society. Available online: https://erj.ersjournals.com/content/50/3/1700010 (accessed on 10 August 2022).
- Coxson, H.O.; Mayo, J.R.; Behzad, H.; Moore, B.J.; Verburgt, L.M.; Staples, C.A.; Pare, P.D.; Hogg, J.C. Measurement of Lung Expansion with Computed Tomography and Comparison with Quantitative Histology. J. Appl. Physiol. 1995, 79, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Hedlund, L.W.; Vock, P.; Effmann, E.L. Evaluating Lung Density by Computed Tomography. Semin. Respir. Med. 1983, 5, 76–88. [Google Scholar] [CrossRef]
- Hartley, P.G.; Galvin, J.R.; Hunninghake, G.W.; Merchant, J.A.; Yagla, S.J.; Speakman, S.B.; Schwartz, D.A. High-Resolution CT-Derived Measures of Lung Density Are Valid Indexes of Interstitial Lung Disease. J. Appl. Physiol. 1994, 76, 271–277. [Google Scholar] [CrossRef]
- Ash, S.Y.; Harmouche, R.; Vallejo, D.L.L.; Villalba, J.A.; Ostridge, K.; Gunville, R.; Come, C.E.; Onieva Onieva, J.; Ross, J.C.; Hunninghake, G.M.; et al. Densitometric and Local Histogram Based Analysis of Computed Tomography Images in Patients with Idiopathic Pulmonary Fibrosis. Respir. Res. 2017, 18, 45. [Google Scholar] [CrossRef] [Green Version]
- Primack, S.L.; Remy-Jardin, M.; Remy, J.; Müller, N.L. High-Resolution CT of the Lung: Pitfalls in the Diagnosis of Infiltrative Lung Disease. Am. J. Roentgenol. 1996, 167, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Partial Correlation and Multiple Regression. Statistical Methods in Biology; Bailey, N.T.J., Ed.; Cambridge University Press: Cambridge, UK, 1995; pp. 156–171. ISBN 978-0-521-46983-8. [Google Scholar]
- Hogg, J.C.; Nepszy, S. Regional Lung Volume and Pleural Pressure Gradient Estimated from Lung Density in Dogs. J. Appl. Physiol. 1969, 27, 198–203. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Patients (n = 45) |
|---|---|
| Age, year | 45 (37, 57) |
| Sex | 23 male and 22 female |
| Vaccination status | 13 vaccinated and 32 unvaccinated |
| Disease severity in the acute phase | 34 mild, 9 moderate and 2 severe |
| Days between symptom onset and CT scan | 84 (76, 95) |
| Total volume of residual pulmonary lesions on CT (cc) | 0.02 (0, 0.8) |
| DLCO_adj (% predicted) | 86 (80, 96) |
| KCO_adj (% predicted) | 102 (91, 111) |
| FEV1 (% predicted) | 95 (84, 103) |
| FEV1/FVC (% predicted) | 96 (92, 100) |
| VA (% predicted) | 86 (80, 93) |
| Input Variables | DLCO_adj (% Predicted) | KCO_adj (% Predicted) |
|---|---|---|
| VA (% predicted) | r = 0.52, p < 0.001 | r = −0.39, p = 0.008 |
| TBV | r = 0.41, p = 0.005 | r = 0.13, p = 0.39 |
| Blood vessel volume fraction | r = 0.30, p = 0.046 | r = 0.36, p = 0.014 |
| TissueM | r = 0.29, p = 0.048 | r = −0.08, p = 0.58 |
| PDm | r = 0.21, p = 0.16 | r = 0.33, p = 0.027 |
| Total volume of residual lung lesions on CT | r = −0.21, p = 0.17 | r = −0.29, p = 0.051 |
| Age | r = −0.11, p = 0.47 | r = −0.05, p = 0.73 |
| Sex | r = 0.02, p = 0.88 | r = 0.14, p = 0.34 |
| Vaccination status | r = 0.13, p = 0.40 | r = 0.02, p = 0.91 |
| Disease severity in the acute phase | r = −0.08, p = 0.62 | r = −0.01, p = 0.94 |
| Days between symptom onset and CT date | r = −0.07, p = 0.63 | r = −0.29, p = 0.051 |
| VA (% Pred.) | Blood Vessel V.F. | PDm | Days Since Symptom Onset | All Other Input Variables | Tri-Variate Model | |
|---|---|---|---|---|---|---|
| Independent contribution to the variance of DLCO_adj (% pred.), n = 45 | 27% | 10% | 12.3% | 2.6% | <2% | 49.4% |
| Multiple linear regression model beta coefficient and p value, n = 45 | β = 0.66, p = 0.031 | β = 186, p = 0.005 | β = 0.27, p = 0.018 | β = −0.03, p = 0.17 | p > 0.25 | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, H.; Huapaya, J.A.; Kanth, S.M.; Sun, J.; Matthew, B.P.; Lee, S.C.; Do, M.; Chen, M.Y.; Malayeri, A.A.; Suffredini, A.F. Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions. J. Imaging 2023, 9, 150. https://doi.org/10.3390/jimaging9080150
Wen H, Huapaya JA, Kanth SM, Sun J, Matthew BP, Lee SC, Do M, Chen MY, Malayeri AA, Suffredini AF. Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions. Journal of Imaging. 2023; 9(8):150. https://doi.org/10.3390/jimaging9080150
Chicago/Turabian StyleWen, Han, Julio A. Huapaya, Shreya M. Kanth, Junfeng Sun, Brianna P. Matthew, Simone C. Lee, Michael Do, Marcus Y. Chen, Ashkan A. Malayeri, and Anthony F. Suffredini. 2023. "Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions" Journal of Imaging 9, no. 8: 150. https://doi.org/10.3390/jimaging9080150
APA StyleWen, H., Huapaya, J. A., Kanth, S. M., Sun, J., Matthew, B. P., Lee, S. C., Do, M., Chen, M. Y., Malayeri, A. A., & Suffredini, A. F. (2023). Quantitative CT Metrics Associated with Variability in the Diffusion Capacity of the Lung of Post-COVID-19 Patients with Minimal Residual Lung Lesions. Journal of Imaging, 9(8), 150. https://doi.org/10.3390/jimaging9080150