
Implementing a Rural Natural Experiment: A Protocol for Evaluating the Impacts of Food Coops on Food Consumption, Resident’s Health and Community Vitality


 , ,
, ,
Abstract
:1. Introduction
- Objective 1:
- Evaluate the effects of the food cooperative on food consumption, residents’ health, and community vitality;
- Objective 2:
- Document the mobilization of community actors before and after the implementation of the food cooperative;
- Objective 3:
- Evaluate the effects of the intervention on food accessibility, use of the food cooperative, and food supply in the local environment;
- Objective 4:
- Analyze the socioeconomic and community contexts of the implementation of a food cooperative;
- Objective 5:
- Implement an integrated knowledge translation process (iKT) to improve practices throughout the project.
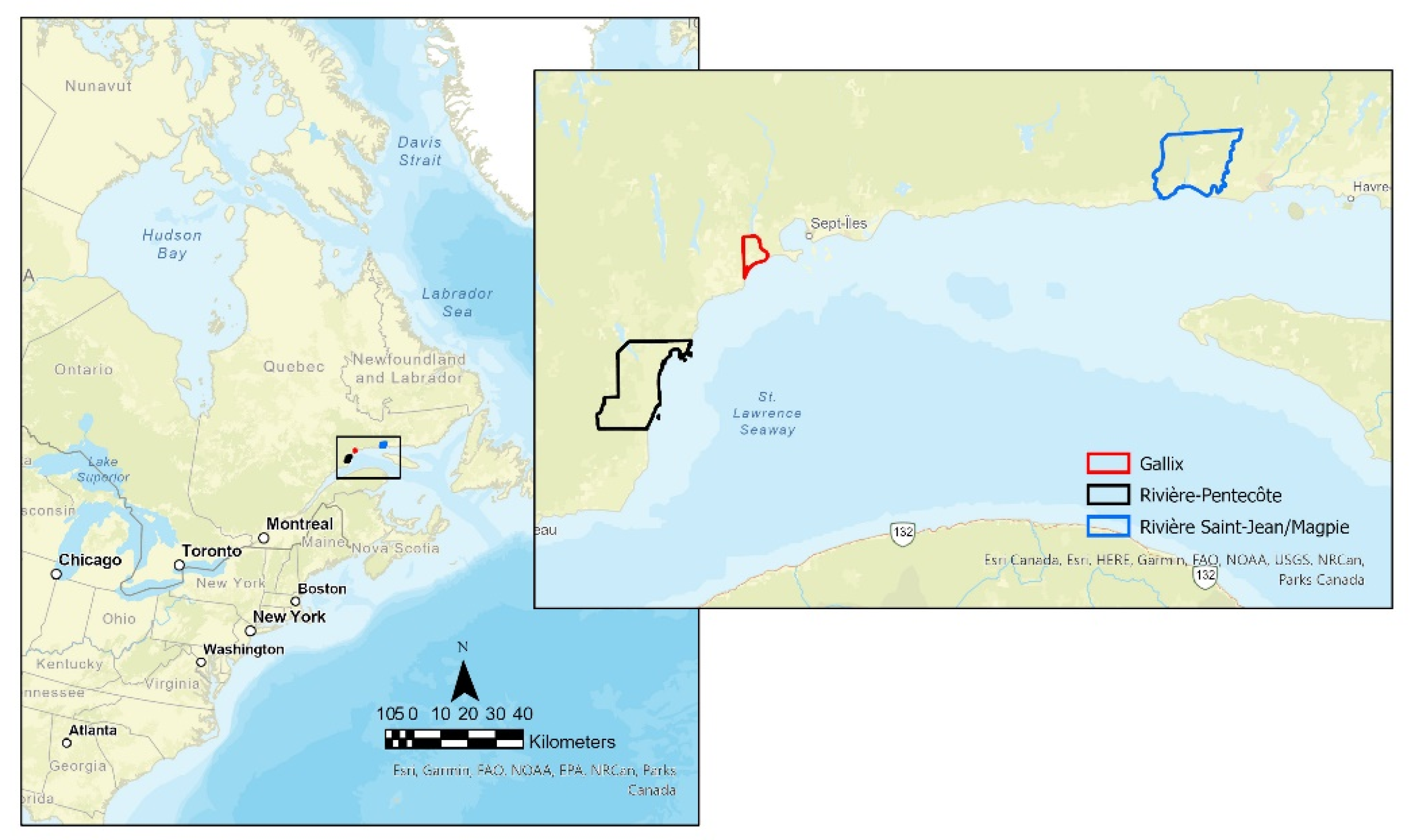
2. Experimental Design
2.1. Rivière-Pentecôte
2.2. Gallix
2.3. Rivière Saint-Jean and Magpie
- Prepare data collection tools;
- Interview key informants (n = 2–3/community) from the selected communities and other organizations involved in the implementation of food cooperatives (n = 3–4) before the implementation of the coops (T0) using semi-structured interviews. The key informants from the selected communities will be interviewed again in T1 or T2 to further understand the process of community mobilization;
- Collect information on the socio-economic characteristics and food environment of the selected communities;
- Integrated knowledge translation process (iKT).
3. Procedure
3.1. Quantitative Data
3.1.1. Study Population
3.1.2. Sample Size Calculation
3.1.3. Recruitment and Retention of Participants
- Community engagement: This will be facilitated by our iKT approach which includes communication with municipal and public health authorities and the region’s healthy living collaborative structures as research stakeholders.
- Increase awareness, knowledge, and understanding of the research: At the beginning of data collection (T0), a campaign to promote the research to citizens will be conducted through local and social media and at popular community locations (e.g., community centers, churches, post offices, gas stations). The objective is to recruit participants, explain the purpose of the research and the process, and the role of local and regional authorities in the project. This campaign will also enhance the profile of the project and research team [70].
- Social and financial supports for participants: Regular contact with participants through reminder letters and greeting cards will also be part of the retention strategies. Several studies have shown that financial incentives can improve the recruitment and retention of survey participants, particularly among socioeconomically disadvantaged populations. We, therefore, plan to use this strategy to facilitate recruitment and to increase the retention of participants [67,73,74]. The value of financial retribution to participants will be gradual and as follows: T0: $25, T1: $30, T2: $35. By adopting these strategies and based on the results of various studies, we foresee a retention rate of 70% at T1 and 50% at T2 [67,68].
3.1.4. Dependent, Independent, and Covariables
Primary Dependent Variable
Secondary Dependent Variables
- Community vitality and well-being will be measured using a combination of three measures of community vitality [80,81,82] and well-being. The final scale resulted in 19 questions on community resilience, citizen participation, community pride, and sustainable development. Questions will be answered on three or five-point Likert scales. A reliability analysis will be performed on the scale using lambda-6 [83];
- Weight and height: one question on weight and one question on height will be used to calculate participants’ BMI.
Independent Respondent Variables
- Adult household food insecurity: The Household Food Security Survey Module (HFSSM) focuses on self-reports of uncertain, insufficient, or inadequate food access, availability, and utilization due to limited financial resources, and any compromised eating patterns and food consumption that may result. The HFSSM contains 18 questions about the food security situation in the household over the previous 12 months. Each question specifies a lack of money or the ability to afford food as the reason for the condition or behavior. The questions range in severity from worrying about running out of food, to children not eating for a whole day. Only questions that are specific to the experiences of adults in the household or the household in general (Adult Scale) will be used in this study [87].
Independent Community Variables
Covariables
3.1.5. Data Protection and Management
3.2. Qualitative Data
3.2.1. Recruitment of Key Informants
3.2.2. Interview Guide
3.3. Analytical Strategies
3.3.1. Quantitative Analysis
3.3.2. Qualitative Analysis
3.4. Integrated Knowledge Translation Process (iKT)
4. Limits
5. Expected Results
- Draw up portraits of their community’s food environment (presence of food deserts, level of physical accessibility, food insecurity, community vitality);
- Take stock of socio-economic characteristics, food consumption, and food insecurity of the communities;
- Evaluate the effects of the implementation of their food cooperative;
- Illustrate, through examples from the communities, the mobilization process, the conditions for success, and the pitfalls to be anticipated when implementing a food cooperative.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Garriguet, D. Canadians’ Eating. Health Rep. 2007, 18, 17. [Google Scholar] [PubMed]
- Garriguet, D. Diet Quality in Canada. Health Rep. 2009, 20, 41. [Google Scholar]
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WH; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Blouin, C.; Vandal, N.; Martel, S.; Barry, A.D.; Hamel, D.; Lo, E.; Jen, Y. Les Conséquences Économiques Associées à l’obésité et à l’embonpoint Au Québec: Les Coûts Liés à l’hospitalisation et Aux Consultations Médicales; Fardeau du poids corporel; Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2015; ISBN 978-2-550-72043-0. [Google Scholar]
- Lieffers, J.R.L.; Ekwaru, J.P.; Ohinmaa, A.; Veugelers, P.J. The Economic Burden of Not Meeting Food Recommendations in Canada: The Cost of Doing Nothing. PLoS ONE 2018, 13, e0196333. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IOM). An Integrated Framework for Assessing the Value of Community-Based Prevention; The National Academy of Sciences: Washington, DC, USA, 2012. [Google Scholar]
- Plante, C.; Rochette, L.; Blanchet, C. Les Apports et Les Sources Alimentaires de Sucre, de Sodium et de Gras Saturés Chez Les Québécois; Regard sur l’alimentation des Québécois; Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2019; ISBN 978-2-550-83521-9. [Google Scholar]
- Plante, C.; Blanchet, C.; Rochette, L. La consommation des Autres Aliments et des Boissons Chez les Québécois; Collection: Regard sur l’alimentation des Québécois; Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2020; p. 28. [Google Scholar]
- EC-FAO Food Security Programme; Agriculture and Economic Development Analysis Division. Introduction Aux Concepts de la Sécurité Alimentaire—Guide Pratique; FAO: Rome, Italy, 2008. [Google Scholar]
- Doyon, M.; Élie-Leonard, J.; Arsenault-Hétu, C. La sécurisation alimentaire en milieu rural: Le cas de trois initiatives agricoles innovantes. Rev. Organ. Territ. 2020, 29, 105–115. [Google Scholar] [CrossRef]
- Raine, K.D. Determinants of Healthy Eating in Canada: An Overview and Synthesis. Can. J. Public Health Rev. Can. Santee Publique 2005, 96, S8–S14. [Google Scholar] [CrossRef]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [Green Version]
- Giskes, K.; Lenthe, F.; van Avendano-Pabon, M.; Brug, J. A Systematic Review of Environmental Factors and Obesogenic Dietary Intakes among Adults: Are We Getting Closer to Understanding Obesogenic Environments? Obes. Rev. 2011, 12, e95–e106. [Google Scholar] [CrossRef]
- World Cancer Research Fund Our Policy Framework to Promote Healthy Diets & Reduce Obesity. Available online: https://www.wcrf.org/int/policy/nourishing/our-policy-framework-promote-healthy-diets-reduce-obesity (accessed on 2 March 2019).
- Lake, A.; Townshend, T. Obesogenic Environments: Exploring the Built and Food Environments. J. R. Soc. Promot. Health 2006, 126, 262–267. [Google Scholar] [CrossRef]
- Kirk, S.F.L.; Penney, T.L.; McHugh, T.-L.F. Characterizing the Obesogenic Environment: The State of the Evidence with Directions for Future Research. Obes. Rev. 2010, 11, 109–117. [Google Scholar] [CrossRef]
- Santé Canada. Mesure de L’environnement Alimentaire Au Canada; Gouvernement du Canada: Ottawa, ON, Canada, 2013; p. 98.
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Healthy Nutrition Environments: Concepts and Measures. Sect. Sci. Health Promot. 2005, 19, 330–333. [Google Scholar] [CrossRef]
- Minaker, L.M.; Shuh, A.; Olstad, D.L.; Engler-Stringer, R.; Black, J.L.; Mah, C.L. Retail Food Environments Research in Canada: A Scoping Review. Can. J. Public Health Rev. Can. St. Publique 2016, 107, 5344. [Google Scholar] [CrossRef] [PubMed]
- Black, C.; Moon, G.; Baird, J. Dietary Inequalities: What Is the Evidence for the Effect of the Neighbourhood Food Environment? Health Place 2014, 27, 229–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papas, M.A.; Alberg, A.J.; Ewing, R.; Helzlsouer, K.J.; Gary, T.L.; Klassen, A.C. The Built Environment and Obesity. Epidemiol. Rev. 2007, 29, 129–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood Environments: Disparities in Access to Healthy Foods in the U.S. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Mercille, G.; Braën, C.; Perez, E.; Boyer, G.; Rehany, E.; Potvin, L. L’associations Entre La Présence de Ressources de Proximité de l’environnement Alimentaire et La Santé; Chaire de Recherche du Canada Approches Communautaires et Inégalités de Santé: Montréal, QC, Canada, 2018; p. 4. [Google Scholar]
- Keener, D.; Goodman, K.; Lowry, A.; Zaro, S.; Kettel Khan, L. Recommended Community Strategies and Measurements to Prevent Obesity in the United States; Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, Canada, 2009.
- WHO. WHO European Action Plan for Food and Nutrition Policy 2007–2012; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- CDC. CDC—Zoning to Encourage Healthy Eating—Winnable Battles—Public Health Law. Available online: http://www.cdc.gov/phlp/winnable/zoning_obesity.html (accessed on 7 February 2014).
- Sadler, R.C.; Gilliland, J.; Arku, G. A Food Retail-Based Intervention on Food Security and Consumption. Int. J. Environ. Res. Public. Health 2013, 10, 3325–3346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummins, S.; Flint, E.; Matthews, S.A. New Neighborhood Grocery Store Increased Awareness Of Food Access But Did Not Alter Dietary Habits Or Obesity. Health Aff. 2014, 33, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubowitz, T.; Ghosh-Dastidar, M.; Cohen, D.A.; Beckman, R.; Steiner, E.D.; Hunter, G.P.; Flórez, K.R.; Huang, C.; Vaughan, C.A.; Sloan, J.C.; et al. Diet And Perceptions Change With Supermarket Introduction in A Food Desert, But Not Because of Supermarket Use. Health Aff. 2015, 34, 1858–1868. [Google Scholar] [CrossRef] [Green Version]
- Rogus, S.; Athens, J.; Cantor, J.; Elbel, B. Measuring Micro-Level Effects of a New Supermarket: Do Residents Within 0.5 Mile Have Improved Dietary Behaviors? J. Acad. Nutr. Diet. 2017, 118, 1037–1046. [Google Scholar] [CrossRef]
- Elbel, B.; Moran, A.; Dixon, L.B.; Kiszko, K.; Cantor, J.; Abrams, C.; Mijanovich, T. Assessment of a Government-Subsidized Supermarket in a High-Need Area on Household Food Availability and Children’s Dietary Intakes. Public Health Nutr. 2015, 18, 2881–2890. [Google Scholar] [CrossRef]
- Abusabha, R.; Namjoshi, D.; Klein, A. Increasing Access and Affordability of Produce Improves Perceived Consumption of Vegetables in Low-Income Seniors. J. Am. Diet. Assoc. 2011, 111, 1549–1555. [Google Scholar] [CrossRef]
- Evans, A.E.; Jennings, R.; Smiley, A.W.; Medina, J.L.; Sharma, S.V.; Rutledge, R.; Stigler, M.H.; Hoelscher, D.M. Introduction of Farm Stands in Low-Income Communities Increases Fruit and Vegetable among Community Residents. Health Place 2012, 18, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Ruelas, V.; Iverson, E.; Kiekel, P.; Peters, A. The Role of Farmers’ Markets in Two Low Income, Urban Communities. J. Community Health 2012, 37, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Gorham, G.; Dulin-Keita, A.; Risica, P.M.; Mello, J.; Papandonatos, G.; Nunn, A.; Gorham, S.; Roberson, M.; Gans, K.M. Effectiveness of Fresh to You, a Discount Fresh Fruit and Vegetable Market in Low-Income Neighborhoods, on Children’s Fruit and Vegetable Consumption, Rhode Island, 2010–2011. Prev. Chronic. Dis. 2015, 12, 140583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leone, L.A.; Haynes-Maslow, L.; Ammerman, A.S. Veggie Van Pilot Study: Impact of a Mobile Produce Market for Underserved Communities on Fruit and Vegetable Access and Intake. J. Hunger Environ. Nutr. 2017, 12, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, R.C.; Raskind, I.G.; Harris, D.M.; Gazmararian, J.A.; Kramer, M.; Haardörfer, R.; Kegler, M.C. The Dietary Impact of Introducing New Retailers of Fruits and Vegetables into a Community: Results from a Systematic Review. Public Health Nutr. 2018, 21, 981–991. [Google Scholar] [CrossRef] [Green Version]
- Hartmann-Boyce, J.; Bianchi, F.; Piernas, C.; Riches, S.P.; Frie, K.; Nourse, R.; Jebb, S.A. Grocery Store Interventions to Change Food Purchasing Behaviors: A Systematic Review of Randomized Controlled Trials. Am. J. Clin. Nutr. 2018, 107, 1004–1016. [Google Scholar] [CrossRef]
- Mah, C.L.; Minaker, L.M.; Jameson, K.; Rappaport, L.; Taylor, K.; Graham, M.; Moody, N.; Cook, B. An Introduction to the Healthy Corner Store Intervention Model in Canada. Can. J. Public Health 2017, 108, 320–324. [Google Scholar] [CrossRef]
- Table intersectorielle régionale en Saines habitudes de vie COSMOSS du Bas-Saint-Laurent (TIR-SHV). Favoriser La Saine Alimentation Grâce Aux Outils d’aménagement Du Territoire; COSMOSS: Bas-Saint-Laurent, QC, Canada, 2018; p. 11. [Google Scholar]
- Mah, C.L.; Cook, B.; Rideout, K.; Minaker, L.M. Policy Options for Healthier Retail Food Environments in City-Regions. Can. J. Public Health 2016, 107, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Abeykoon, A.H.; Engler-Stringer, R.; Muhajarine, N. Health-Related Outcomes of New Grocery Store Interventions: A Systematic Review. Public Health Nutr. 2017, 20, 2236–2248. [Google Scholar] [CrossRef]
- Engler-Stringer, R.; Muhajarine, N.; Ridalls, T.; Abonyi, S.; Vatanparast, H.; Whiting, S.; Walker, R. The Good Food Junction: A Community-Based Food Store Intervention to Address Nutritional Health Inequities. JMIR Res. Protoc. 2016, 5, e52. [Google Scholar] [CrossRef]
- Fuller, D.; Engler-Stringer, R.; Muhajarine, N. Examining Food Purchasing Patterns from Sales Data at a Full-Service Grocery Store Intervention in a Former Food Desert. Prev. Med. Rep. 2015, 2, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, D.; Engler-Stringer, R.; Muhajarine, N. Retail Food Environments Research: Promising Future with More Work to Be Done. Can. J. Public Health 2016, 107, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Arterburn, D.; Zane, J.; Aggarwal, A.; Gupta, S.; Hurvitz, P.M.; Moudon, A.V.; Bobb, J.; Cook, A.; Lozano, P.; et al. The Moving to Health (M2H) Approach to Natural Experiment Research: A Paradigm Shift for Studies on Built Environment and Health. SSM Popul. Health 2019, 7, 100345. [Google Scholar] [CrossRef] [PubMed]
- Leatherdale, S.T. Natural Experiment Methodology for Research: A Review of How Different Methods Can Support Real-World Research. Int. J. Soc. Res. Methodol. 2019, 22, 19–35. [Google Scholar] [CrossRef]
- Robitaille, É.; Bergeron, P.; Laguë, J. Accessibilité Géographique Aux Commerces Alimentaires Au Québec: Analyse de Situation et Perspectives d’interventions; Institut National de Santé Publique du Québec: Québec, QC, Canada, 2013. [Google Scholar]
- Ramirez, A.S.; Diaz Rios, L.K.; Valdez, Z.; Estrada, E.; Ruiz, A. Bringing Produce to the People: Implementing a Social Marketing Food Access Intervention in Rural Food Deserts. J. Nutr. Educ. Behav. 2017, 49, 166–174.e1. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and Access to Healthy Food in the United States: A Review of Food Deserts Literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef]
- Cadieux, É.; Corbeil, D.; Payette, J. Accessibilité Géographique Aux Commerces d’alimentation: Outil Pour Comprendre et Utiliser La Cartographie Des Unités Résidentielles Répondant Aux Critères de Désert Alimentaire; DSpublique Lanaudière: Joliette, QC, Canada, 2017; p. 4.
- Robichaud, M.-P. Coopératives de Services Marchands de Proximité; CQCM: Lévis, QC, Canada, 2017; p. 15. [Google Scholar]
- Lebel, A. L’identification Des Déserts Alimentaires En Milieu Rural; CISSS de Chaudière-Appalaches, Université Laval: Québec, QC, Canada, 2015; p. 10. [Google Scholar]
- Guise, J.-M.; Chang, C.; Butler, M.; Viswanathan, M.; Tugwell, P. AHRQ Series on Complex Intervention Systematic Reviews-Paper 1: An Introduction to a Series of Articles That Provide Guidance and Tools for Reviews of Complex Interventions. J. Clin. Epidemiol. 2017, 90, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Morestin, F.; Castonguay, J. Construire Le Modèle Logique d’une Politique Publique Favorable à La Santé: Pourquoi et Comment?: Note Documentaire; Pour des connaissances en matière de politiques publiques favorables à la santé; Centre de Collaboration Nationale sur les Politiques Publiques et la Santé, Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2013; ISBN 978-2-550-70851-3. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2002; ISBN 978-0-7619-1971-1. [Google Scholar]
- McDermott, F. Researching Groupwork: Outsider and Insider Perspectives. Groupwork 2005, 15, 90–108. [Google Scholar] [CrossRef]
- Evans, A.; Banks, K.; Jennings, R.; Nehme, E.; Nemec, C.; Sharma, S.; Hussaini, A.; Yaroch, A. Increasing Access to Healthful Foods: A Qualitative Study with Residents of Low-Income Communities. Int. J. Behav. Nutr. Phys. Act. 2015, 12 (Suppl. 1), S5. [Google Scholar] [CrossRef] [Green Version]
- Petticrew, M.; Cummins, S.; Ferrell, C.; Findlay, A.; Higgins, C.; Hoy, C.; Kearns, A.; Sparks, L. Natural Experiments: An Underused Tool for Public Health? Public Health 2005, 119, 751–757. [Google Scholar] [CrossRef]
- FCAQ. FCAQ—Fédération Des Coopératives d’alimentation Du Québec. Available online: http://www.fcaq.coop/ (accessed on 23 February 2019).
- Statistique Canada Profil Du Recensement, Recensement de 2016. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/index.cfm?Lang=F (accessed on 18 February 2022).
- Kestens, Y.; Winters, M.; Fuller, D.; Bell, S.; Berscheid, J.; Brondeel, R.; Cantinotti, M.; Datta, G.; Gauvin, L.; Gough, M.; et al. INTERACT: A Comprehensive Approach to Assess Urban Form Interventions through Natural Experiments. BMC Public Health 2019, 19, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaix, B.; Kestens, Y.; Perchoux, C.; Karusisi, N.; Merlo, J.; Labadi, K. An Interactive Mapping Tool to Assess Individual Mobility Patterns in Neighborhood Studies. Am. J. Prev. Med. 2012, 43, 440–450. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Oxfordshire, UK, 2013. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMillan, F.; George, E.S.; Feng, X.; Merom, D.; Bennie, A.; Cook, A.; Sanders, T.; Dwyer, G.; Pang, B.; Guagliano, J.M.; et al. Do Natural Experiments of Changes in Neighborhood Built Environment Impact Physical Activity and Diet? A Systematic Review. Int. J. Environ. Res. Public. Health 2018, 15, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, L.; Barnason, S.; Do, V. Review Strategies to Recruit and Retain Rural Patient Participating Self-Management Behavioral Trials. Online J. Rural Res. Policy 2015, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Flynn, A.; Tremblay, P.F.; Rehm, J.; Wells, S. A Modified Random Walk Door-to-Door Recruitment Strategy for Collecting Social and Biological Data Relating to Mental Health, Substance Use, Addiction, and Violence Problems in a Canadian Community. Int. J. Alcohol Drug Res. 2013, 2, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Huppé, V.; Lévesque, B.; Tourigny, A.; Robitaille, É. Mon Habitat, plus Qu’un Simple Toit: Évaluer Les Caractéristiques de l’environnement Bâti En Lien Avec La Santé; Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2018; ISBN 978-2-550-81995-0. [Google Scholar]
- Dubowitz, T.; Ncube, C.; Leuschner, K.; Tharp-Gilliam, S. A Natural Experiment Opportunity in Two Low-Income Urban Food Desert Communities: Research Design, Community Engagement Methods, and Baseline Results. Health Educ. Behav. 2015, 42, 87S–96S. [Google Scholar] [CrossRef] [Green Version]
- Wages, J.G.; Jackson, S.F.; Bradshaw, M.H.; Chang, M.; Estabrooks, P.A. Different Strategies Contribute to Community Physical Activity Program Participation in Rural versus Metropolitan Settings. Am. J. Health Promot. 2010, 25, 36–39. [Google Scholar] [CrossRef]
- Booker, C.L.; Harding, S.; Benzeval, M. A Systematic Review of the Effect of Retention Methods in Population-Based Cohort Studies. BMC Public Health 2011, 11, 249. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, L.; Schwirian, P.; Groner, J. Recruitment and Retention Strategies in Clinical Studies with Low-Income and Minority Populations: Progress from 2004–2014. Contemp. Clin. Trials 2015, 45, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Gouvernement du Canada, S.C. Enquête sur la Santé dans les Collectivités Canadiennes—Composante Annuelle (ESCC). Available online: http://www23.statcan.gc.ca/imdb/p2SV_f.pl?Function=getSurvey&SDDS=3226 (accessed on 24 May 2017).
- Lafrenière, J.; Harrison, S.; Laurin, D.; Brisson, C.; Talbot, D.; Couture, P.; Lemieux, S.; Lamarche, B. Development and Validation of a Brief Diet Quality Assessment Tool in the French-Speaking Adults from Quebec. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 61. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, E.M.; Kobayashi, M.M.; DuBow, W.M.; Wytinck, S.M. Perceived Access to Fruits and Vegetables Associated with Increased Consumption. Public Health Nutr. 2009, 12, 1743–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dibsdall, L.A.; Lambert, N.; Bobbin, R.F.; Frewer, L.J. Low-Income Consumers’ Attitudes and Behaviour towards Access, Availability and Motivation to Eat Fruit and Vegetables. Public Health Nutr. 2003, 6, 159–168. [Google Scholar] [CrossRef]
- Carbonneau, E.; Robitaille, J.; Lamarche, B.; Corneau, L.; Lemieux, S. Development and Validation of the Perceived Food Environment Questionnaire in a French-Canadian Population. Public Health Nutr. 2017, 20, 1914–1920. [Google Scholar] [CrossRef] [Green Version]
- Baldwin, C.; Vincent, P.; Anderson, J.; Rawstorne, P. Measuring Well-Being: Trial of the Neighbourhood Thriving Scale for Social Well-Being Among Pro-Social Individuals. Int. J. Community Well-Being 2020, 3, 361–390. [Google Scholar] [CrossRef]
- Sirgy, M.J.; Widgery, R.N.; Lee, D.-J.; Yu, G.B. Developing a Measure of Community Well-Being Based on Perceptions of Impact in Various Life Domains. Soc. Indic. Res. 2010, 96, 295–311. [Google Scholar] [CrossRef]
- Stolte, M.; Metcalfe, B. Beyond Economic Survival: 97 Ways Small Communities Can Thrive. A Guide to Community Vitality. Available online: http://www.meansofexchange.com/reportdownloads/Beyond-Economic-Survival.pdf (accessed on 20 December 2021).
- Bourque, J.; Doucet, D.; LeBlanc, J.; Dupuis, J.; Nadeau, J. L’alpha de Cronbach est l’un des pires estimateurs de la consistance interne: Une étude de simulation. Rev. Sci. L’éducation 2019, 45, 78–99. [Google Scholar] [CrossRef] [Green Version]
- Widener, M.J.; Minaker, L.M.; Reid, J.L.; Patterson, Z.; Ahmadi, T.K.; Hammond, D. Activity Space-Based Measures of the Food Environment and Their Relationships to Food Purchasing Behaviours for Young Urban Adults in Canada. Public Health Nutr. 2018, 21, 2103–2116. [Google Scholar] [CrossRef] [Green Version]
- Chaput, S.; Mercille, G.; Drouin, L.; Kestens, Y. Promoting Access to Fresh Fruits and Vegetables through a Local Market Intervention at a Subway Station. Public Health Nutr. 2018, 21, 3258–3270. [Google Scholar] [CrossRef]
- Drisdelle, C.; Kestens, Y.; Hamelin, A.M.; Mercille, G. Disparities in Access to Healthy Diets: How Food Security and Food Shopping Behaviors Relate to Fruit and Vegetable Intake. J. Acad. Nutr. Diet. 2020, 120, 1847–1858. [Google Scholar] [CrossRef] [PubMed]
- Canada, H. The Household Food Security Survey Module (HFSSM). Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-community-health-survey-cchs/household-food-insecurity-canada-overview/household-food-security-survey-module-hfssm-health-nutrition-surveys-health-canada.html (accessed on 20 December 2021).
- Jalbert-Arsenault, É.; Robitaille, É.; Paquette, M.-C. Development, Reliability and Use of a Food Environment Assessment Tool in Supermarkets of Four Neighbourhoods in Montréal, Canada. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2017, 37, 293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamache, P.; Hamel, D. Les Défis de la Mise à Jour de L’indice de Défavorisation Avec les Données du Recensement de 2011 et de l’Enquête Nationale Auprès des Ménages (ENM); Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2017; ISBN 978-2-550-77343-6. [Google Scholar]
- Government of Canada, S.C. 2021 Census Questionnaires. Available online: https://www12.statcan.gc.ca/census-recensement/2021/ref/questionnaire/index-eng.cfm (accessed on 20 December 2021).
- Government of Canada, S.C. Canadian Community Health Survey—Annual Component (CCHS). Available online: https://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=3226 (accessed on 20 December 2021).
- Billion, C. Rôle Des Acteurs Du Commerce et de La Distribution Dans Les Processus de Gouvernance Alimentaire Territoriale. Ph.D. Thesis, Université Clermont Auvergne, Clermont-Ferrand, France, 2018. [Google Scholar]
- Mayer, V.L. Perspectives of Urban Corner Store Owners and Managers on Community Health Problems and Solutions. Prev. Chronic. Dis. 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Fortier, J. Proposition d’un Cadre de Référence En Concertation. Doctoral Dissertation, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada, 2002. [Google Scholar]
- Maher, M. Terminologie 101: Analyse Selon L’intention de Traiter Dans les ECR|Infirmiere Canadienne. Available online: https://www.canadian-nurse.com/fr/articles/issues/2015/avril-2015/analyse-selon-lintention-de-traiter-dans-les-ecr (accessed on 3 March 2019).
- Elbel, B.; Mijanovich, T.; Kiszko, K.; Abrams, C.; Cantor, J.; Dixon, L.B. The Introduction of a Supermarket via Tax-Credits in a Low-Income Area: The Influence on Purchasing and Consumption. Am. J. Health Promot. 2017, 31, 59–66. [Google Scholar] [CrossRef]
- Richardson, A.S.; Ghosh-Dastidar, M.; Beckman, R.; Flórez, K.R.; DeSantis, A.; Collins, R.L.; Dubowitz, T. Can the Introduction of a Full-Service Supermarket in a Food Desert Improve Residents’ Economic Status and Health? Ann. Epidemiol. 2017, 27, 771–776. [Google Scholar] [CrossRef]
- Bennett, W.L.; Cheskin, L.J.; Wilson, R.F.; Zhang, A.; Tseng, E.; Shogbesan, O.; Knapp, E.A.; Stuart, E.A.; Bass, E.B.; Kharrazi, H. Methods for Evaluating Natural Experiments in Obesity: Systematic Evidence Review; AHRQ Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2017.
- Cole, S.R.; Chu, H.; Greenland, S. Multiple-Imputation for Measurement-Error Correction. Int. J. Epidemiol. 2006, 35, 1074–1081. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple Imputation for Missing Data in Epidemiological and Clinical Research: Potential and Pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Lemire, N.; Laurendeau, M.-C.; Souffez, K. Animer un Processus de Transfert des Connaissances: Bilan des Connaissances et Outil D’animation; Institut National de Santé Publique du Québec: Montréal, QC, Canada, 2009; ISBN 978-2-550-57546-7. [Google Scholar]
- Kirkpatrick, S.I.; Reedy, J.; Butler, E.N.; Dodd, K.W.; Subar, A.F.; Thompson, F.E.; McKinnon, R.A. Dietary Assessment in Food Environment Research: A Systematic Review. Am. J. Prev. Med. 2014, 46, 94–102. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.M.; Haslam, R.L.; Burrows, T.L.; Duncanson, K.R.; Ashton, L.M.; Rollo, M.E.; Shrewsbury, V.A.; Schumacher, T.L.; Collins, C.E. Issues in Measuring and Interpreting Diet and Its Contribution to Obesity. Curr. Obes. Rep. 2019, 8, 53–65. [Google Scholar] [CrossRef]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social Desirability Bias in Dietary Self-Report May Compromise the Validity of Dietary Intake Measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Methods | Measurement Tools (F = Validated in French) |
|---|---|---|
| Dependent variables | ||
| Fruit and vegetable consumption | Surveys * | Fruit and vegetable module (CCHS) (F) |
| Food quality consumption | Surveys * | Brief food quality assessment tool (F) |
| Perception of the food environment | Surveys * | Nine questions each measured five-point scale (F) |
| Community vitality | Surveys * | Combination of three vitality and well-being scales |
| Body mass index (BMI) | Surveys * | Self-reported weight and size (F) |
| Independent variables | ||
| Household food insecurity | Surveys * | Household Food Security Survey Module (F) |
| Attendance and food shopping locations | Surveys * | Interactive mapping tool to measure shopping locations. |
| Characteristics of the community’s food environment | GIS † | MAPAQ food business files (distance to nearest food retailer, distance to principal food retailer as identifier by participant, density of fast-food outlets) |
| Socioeconomic characteristics of communities | GIS † | INSPQ Deprivation Index and Vitality Index |
| Covariables | ||
| Sociodemographic characteristics of individuals | Surveys * | Canadian Community Health Survey (CCHS) (F) and Census Canada (F), (age, income, education, marital and family status) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robitaille, É.; Paquette, M.-C.; Durette, G.; Bergeron, A.; Dubé, M.; Doyon, M.; Mercille, G.; Lemire, M.; Lo, E. Implementing a Rural Natural Experiment: A Protocol for Evaluating the Impacts of Food Coops on Food Consumption, Resident’s Health and Community Vitality. Methods Protoc. 2022, 5, 33. https://doi.org/10.3390/mps5020033
Robitaille É, Paquette M-C, Durette G, Bergeron A, Dubé M, Doyon M, Mercille G, Lemire M, Lo E. Implementing a Rural Natural Experiment: A Protocol for Evaluating the Impacts of Food Coops on Food Consumption, Resident’s Health and Community Vitality. Methods and Protocols. 2022; 5(2):33. https://doi.org/10.3390/mps5020033
Chicago/Turabian StyleRobitaille, Éric, Marie-Claude Paquette, Gabrielle Durette, Amélie Bergeron, Marianne Dubé, Mélanie Doyon, Geneviève Mercille, Marc Lemire, and Ernest Lo. 2022. "Implementing a Rural Natural Experiment: A Protocol for Evaluating the Impacts of Food Coops on Food Consumption, Resident’s Health and Community Vitality" Methods and Protocols 5, no. 2: 33. https://doi.org/10.3390/mps5020033
APA StyleRobitaille, É., Paquette, M. -C., Durette, G., Bergeron, A., Dubé, M., Doyon, M., Mercille, G., Lemire, M., & Lo, E. (2022). Implementing a Rural Natural Experiment: A Protocol for Evaluating the Impacts of Food Coops on Food Consumption, Resident’s Health and Community Vitality. Methods and Protocols, 5(2), 33. https://doi.org/10.3390/mps5020033