Efficacy of Perceptual Learning-Based Vision Training as an Adjuvant to Occlusion Therapy in the Management of Amblyopia: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Subjects until 17 years old with moderate or severe amblyopia.
- Anisometropic amblyopia (differences in sphere between eyes of more than 1.0 D and in cylinder of more than 1.5 D) or strabismic amblyopia (any angle of deviation).
- No active ocular or systemic disease.
- No previous ocular surgery.
2.2. Clinical Protocol
2.3. Perceptual Learning Software
- -
- Follow the letter: Orientation identification with a moving Landolt C of increasing resolution.
- -
- Letter jump: Orientation identification with a jumping Landolt C of increasing resolution that appears in different parts of the screen.
- -
- Find the target: Letter discrimination using a reference letter or symbol that must be found by the patient among many crowded letters or symbols.
- -
- Concentration: Optotype or symbol identification in a list of stimuli after its previous presentation during a short period of time.
- -
- Capture the target: Identification of an optotype or symbol among a list of optotypes and symbols that are moving constantly across the screen.
- -
- Space ball: Eye-hand coordination exercise in which a space ball must be kept on the field of the game with a moving stimulus (a planet or similar) and 4 paddles, one of each side of the screen. The patient should move a paddle to bounce the ball away from the side. The patient will use the mouse to move the bars (up, down, right, and left of the screen) to hit the ball and prevent it from exiting from the screen.
- -
- Chipmunk chase: Orientation discrimination with Snellen Es presented by 3 squirrels (Figure 1).
- -
- Penguin peek: Orientation discrimination in several penguins holding a card with stimuli (Forms, E or C). For each penguin, there will be another penguin holding a card with the stimulus partner. Using the mouse, the patient will click on a penguin and then on another penguin that the stimulus partner is holding.
- -
- Skiing: Eye-hand coordination with a mouse; the patient must pass between a pair of moving poles a small penguin that can be moved across the screen.
- -
- Traffic jam: Orientation discrimination of Landolt C optotypes printed on the roof of several crowded colored and noisy cars (Figure 2).
- -
- Laser ball: Orientation discrimination of a Landolt C of increasing resolution. The patient will use the mouse to move the laser ball to the end of the screen and find the stimulus in the upper half of the screen that matches that of the laser ball. The patient will move the mouse directly under the corresponding stimulus, and then will press the mouse button to launch the laser ball.
2.4. Data Analysis
3. Results
3.1. Description of the Sample
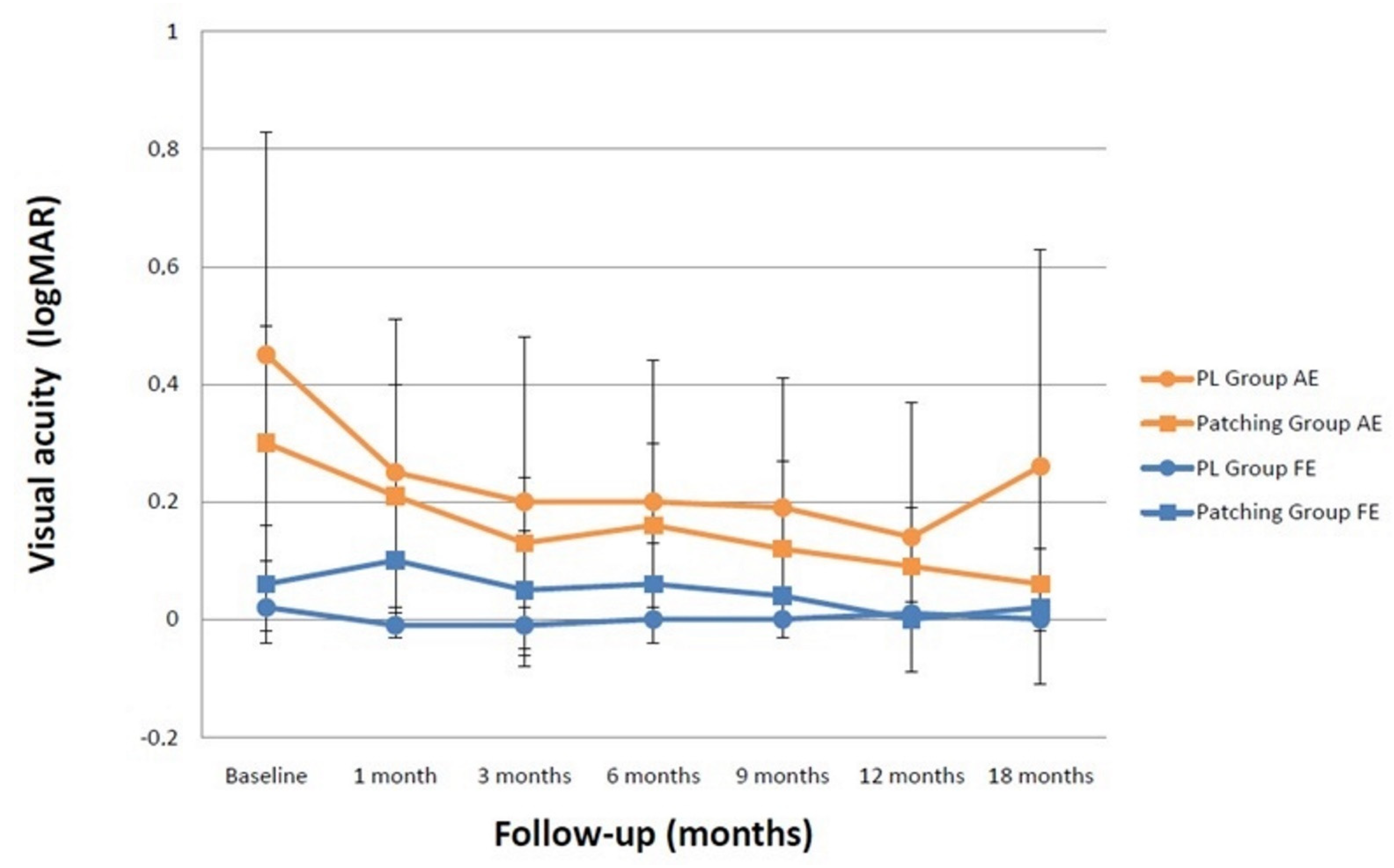
3.2. Changes in Visual Acuity
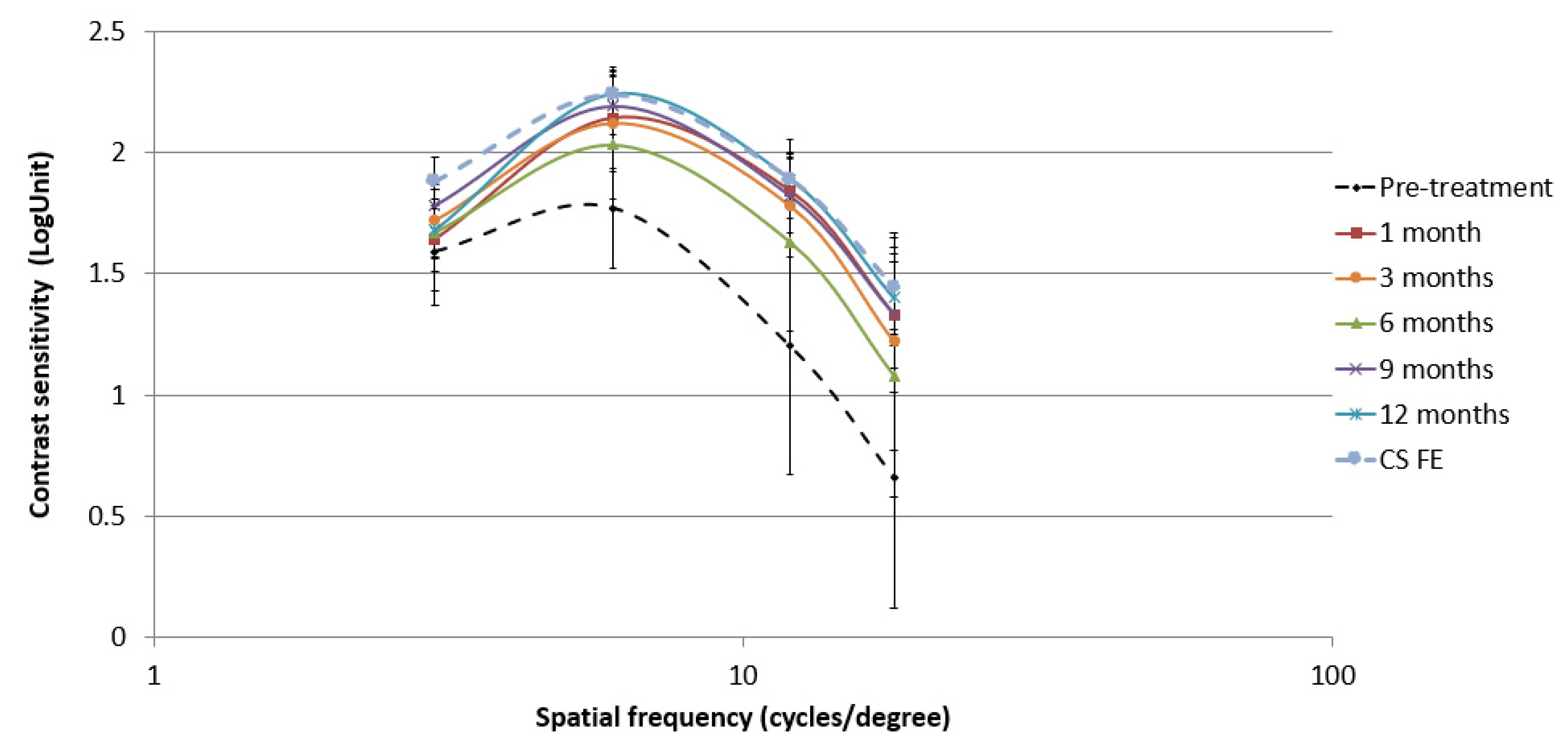
3.3. Changes in Contrast Sensitivity in the Perceptual Learning Group and Correlation with Visual Acuity Outcomes
3.4. Compliance and Duration of Perceptual Learning Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Webber, A.L.; Wood, J. Amblyopia: Prevalence, natural history, functional effects and treatment. Clin. Exp. Optom. 2005, 88, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Barrett, B.T.; Bradley, A.; McGraw, P.V. Understanding the neural basis of amblyopia. Neuroscientist 2004, 10, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Webber, A. The functional impact of amblyopia. Clin. Exp. Optom. 2018, 101, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J. Compliance and patching and atropine amblyopia treatments. Vis. Res. 2015, 114, 31–40. [Google Scholar] [CrossRef]
- Narasimhan, S.; Harrison, E.R.; Giaschi, D.E. Quantitative measurement of interocular suppression in children with amblyopia. Vis. Res. 2012, 66, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hess, R.F.; Thompson, B.; Baker, D.H. Binocular vision in amblyopia: Structure, suppression and plasticity. Ophthalmic Physiol. Opt. 2014, 34, 146–162. [Google Scholar] [CrossRef] [Green Version]
- Kraus, C.L.; Culican, S.M. New advances in amblyopia therapy I: Binocular therapies and pharmacologic augmentation. Br. J. Ophthalmol. 2018, 102, 1492–1496. [Google Scholar] [CrossRef] [Green Version]
- Dye, M.W.G.; Green, C.S.; Bavelier, D. The development of attention skills in action video game players. Neuropsychologia 2009, 47, 1780–1789. [Google Scholar] [CrossRef] [Green Version]
- Levi, D.M.; Li, R.W. Perceptual learning as a potential treatment for amblyopia: A mini-review. Vis. Res. 2009, 49, 2535–2549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dosher, B.; Lu, Z.L. Visual perceptual learning and models. Annu. Rev. Vis. Sci. 2017, 3, 343–363. [Google Scholar] [CrossRef]
- Barollo, M.; Contemori, G.; Battaglini, L.; Pavan, A.; Casco, C. Perceptual learning improves contrast sensitivity, visual acuity, and foveal crowding in amblyopia. Restor. Neurol. Neurosci. 2017, 35, 483–496. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Yang, X.; Liao, M.; Zhang, N.; Liu, L. Internet-based perceptual learning in treating amblyopia. Eur. J. Ophthalmol. 2013, 23, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Avram, E.; Stănilă, A. Treating anisometric amblyopia with HTS Amblyopia iNet Software--preliminary results. Oftalmologia 2013, 57, 32–37. [Google Scholar]
- Gambacorta, C.; Nahum, M.; Vedamurthy, I.; Bayliss, J.; Jordan, J.; Bavelier, D.; Levi, D.M. An action video game for the treatment of amblyopia in children: A feasibility study. Vis. Res. 2018, 148, 1–14. [Google Scholar] [CrossRef]
- Birch, E.E.; Li, S.L.; Jost, R.M.; Morale, S.E.; De La Cruz, A.; Stager, D., Jr.; Dao, L.; Stager, D.R., Sr. Binocular iPad treatment for amblyopia in preschool children. J. AAPOS 2015, 19, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Žiak, P.; Holm, A.; Halička, J.; Mojžiš, P.; Piñero, D.P. Amblyopia treatment of adults with dichoptic training using the virtual reality oculus rift head mounted display: Preliminary results. BMC Ophthalmol. 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Coco-Martin, M.B.; Piñero, D.P.; Leal-Vega, L.; Hernández-Rodríguez, C.J.; Adiego, J.; Molina-Martín, A.; de Fez, D.; Arenillas, J.F. The potential of virtual reality for inducing neuroplasticity in children with amblyopia. J. Ophthalmol. 2020, 2020, 7067846. [Google Scholar] [CrossRef] [PubMed]
- Campana, G.; Camilleri, R.; Pavan, A.; Veronese, A.; Lo Giudice, G. Improving visual functions in adult amblyopia with combined perceptual training and transcranial random noise stimulation (tRNS): A pilot study. Front. Psychol. 2014, 5, 1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moret, B.; Camilleri, R.; Pavan, A.; Lo Giudice, G.; Veronese, A.; Rizzo, R.; Campana, G. Differential effects of high-frequency transcranial random noise stimulation (hf-tRNS) on contrast sensitivity and visual acuity when combined with a short perceptual training in adults with amblyopia. Neuropsychologia 2018, 114, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Totsuka, S.; Handa, T.; Ishikawa, H.; Shoji, N. Improvement of adherence with Occlu-Pad therapy for pediatric patients with amblyopia. BioMed Res. Int. 2018, 2018, 2394562. [Google Scholar] [CrossRef] [Green Version]
- Polat, U.; Ma-Naim, T.; Spierer, A. Treatment of children with amblyopia by perceptual learning. Vis. Res. 2009, 49, 2599–2603. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, P.G.; Bhalchandra, P.C.; Nalgirkar, A.R.; Tathe, S.R. Improvement of visual acuity in residual meridional amblyopia by astigmatic axis video games. Indian J. Ophthalmol. 2018, 66, 1156–1160. [Google Scholar] [CrossRef]
- Kuruca, S.; Niyaz, L.; Yucel, O.E.; Erkan, N.D. Results of CAM therapy in amblyopic patients. Vestn. Oftalmol. 2015, 131, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Polat, U.; Ma-Naim, T.; Belkin, M.; Sagi, D. Improving vision in adult amblyopia by perceptual learning. Proc. Natl. Acad. Sci. USA 2004, 101, 6692–6697. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Li, J.; Liu, J.; Cai, X.; Yuan, J.; Deng, D.; Yu, M. Monocular perceptual learning of contrast detection facilitates binocular combination in adults with anisometropic amblyopia. Sci. Rep. 2016, 6, 20187. [Google Scholar] [CrossRef] [Green Version]
- Xi, J.; Jia, W.L.; Feng, L.X.; Lu, Z.L.; Huang, C.B. Perceptual learning improves stereoacuity in amblyopia. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2384–2391. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Rodríguez, C.J.; Piñero, D.P.; Molina-Martín, A.; Morales-Quezada, L.; de Fez, D.; Leal-Vega, L.; Arenillas, J.F.; Coco-Martín, M.B. Stimuli characteristics and psychophysical requirements for visual training in amblyopia: A narrative review. J. Clin. Med. 2020, 9, 3985. [Google Scholar] [CrossRef] [PubMed]
- Kiorpes, L.; Daw, N. Cortical correlates of amblyopia. Vis. Neurosci. 2018, 35, E016. [Google Scholar] [CrossRef]
- Hernández-Rodríguez, C.J.; Piñero, D.P. Active vision therapy for anisometropic amblyopia in children: A systematic review. J. Ophthalmol. 2020, 2020, 4282316. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Zhai, L.; Jiang, Q.; Qin, W.; Li, Q.; Yin, X.; Guo, M. Tract-based spatial statistics analysis of white matter changes in children with anisometropic amblyopia. Neurosci. Lett. 2015, 597, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Crewther, S.G.; Liang, M.; Laycock, R.; Yu, T.; Alexander, B.; Crewther, D.P.; Wang, J.; Yin, Z. Impaired activation of visual attention network for motion salience is accompanied by reduced functional connectivity between frontal eye fields and visual cortex in strabismic amblyopia. Front. Hum. Neurosci. 2017, 11, 195. [Google Scholar] [CrossRef] [Green Version]
- Buckle, M.; Billington, C.; Shah, P.; Ferris, J.D. Treatment outcomes for amblyopia using PEDIG amblyopia protocols: A retrospective study of 877 cases. J. AAPOS 2019, 23, 98.e1–98.e4. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.M.; Levi, D.M. Treatment of amblyopia as a function of age. Vis. Neurosci. 2018, 35, E015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Maniglia, M.; Velez, F.; Demer, J.L.; Seitz, A.R.; Pineles, S. Short-term Perceptual Learning Game Does Not Improve Patching-Resistant Amblyopia in Older Children. J. Pediatr. Ophthalmol. Strabismus 2020, 57, 176–184. [Google Scholar] [CrossRef]
- Jia, W.; Lan, F.; Xin, Z.; Lu, Z.L.; Huang, C.B.; Zhao, W.; Li, M. The effects of monocular training on binocular functions in anisometropic amblyopia. Vis. Res. 2018, 152, 74–83. [Google Scholar] [CrossRef]
- Liu, S.; Zou, L.; Wen, W.; Wang, S.; Liu, G.; Li, Y.; Yang, G.; Chang, X.; Liu, H.; Liao, R. Binocular treatment in adult amblyopia is based on parvocellular or magnocellular pathway. Eur. J. Ophthalmol. 2020, 30, 658–667. [Google Scholar]
- Karmarkar, U.R.; Dan, Y. Experience-dependent plasticity in adult visual cortex. Neuron 2006, 52, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, T.; Sasaki, Y. Perceptual learning: Toward a comprehensive theory. Annu. Rev. Psychol. 2015, 66, 197–221. [Google Scholar] [CrossRef] [Green Version]
- Maniglia, M.; Seitz, A.R. Towards a whole brain model of Perceptual Learning. Curr. Opin. Behav. Sci. 2018, 20, 47–55. [Google Scholar] [CrossRef]
- Rosa, A.M.; Silva, M.F.; Ferreira, S.; Murta, J.; Castelo-Branco, M. Plasticity in the human visual cortex: An ophthalmology-based perspective. BioMed Res. Int. 2013, 2013, 568354. [Google Scholar] [CrossRef]
- Golla, H.; Ignashchenkova, A.; Haarmeier, T.; Thier, P. Improvement of visual acuity by spatial cueing: A comparative study in human and non-human primates. Vis. Res. 2004, 44, 1589–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwata, Y.; Handa, T.; Ishikawa, H.; Goseki, T.; Shoji, N. Evaluation of the Effects of the Occlu-Pad for the Management of Anisometropic Amblyopia in Children. Curr. Eye Res. 2018, 43, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Handa, T.; Ishikawa, H.; Goseki, T.; Shoji, N. Comparison between Amblyopia Treatment with Glasses Only and Combination of Glasses and Open-Type Binocular “Occlu-Pad” Device. BioMed Res. Int. 2018, 2018, 2459696. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PL Group Perceptual Learning Group (n= 14) | Patching Group Patching Group (n = 13) | p-Value | |
|---|---|---|---|
| Age (mean ± SD years) | 9.7 ± 1.4 | 5.0 ± 0.4 | 0.006 * |
| Gender (male/female) | 6 M/8 F | 6 M/7 F | 0.863 |
| Type of amblyopia | 7 aniso/7 strab | 7 aniso/6 strab | 0.842 |
| Patching regimen (mean ± SD hours) | 4.1 ± 1.2 | 4.8 ± 0.5 | 0.440 |
| Previous treatment | Yes 12/No 2 | Yes 3/No 10 | 0.001 * |
| Amblyopic eye | |||
| Sphere (mean ± SD) (D) | +4.98 ± 2.75 | +4.61 ± 2.66 | 0.752 |
| Cylinder (mean ± SD) (D) | −1.51 ± 1.19 | −1.12 ± 1.27 | 0.338 |
| Fellow eye | |||
| Sphere (mean ± SD) (D) | +2.10 ± 2.14 | +3.34 ± 2.92 | 0.342 |
| Cylinder (mean ± SD) (D) | −0.25 ± 0.47 | −0.60 ± 0.78 | 0.228 |
| LogMAR VA FE | |||||||||||||
| Baseline | 1 month | 3 months | 6 months | 9 months | 12 months | 18 months | |||||||
| PL Patching | 0.02 ± 0.04 | −0.01 ± 0.02 | 0.066 b | −0.01 ± 0.05 | 0.180 c | 0.00 ± 0.00 | 0.317 d | 0.00 ± 0.01 | 0.317 e | 0.01 ± 0.02 | 0.317 f | 0.0 ± 0.01 | 0.317 g |
| 0.06 ± 0.10 | 0.10 ± 0.10 | 0.180 b | 0.05 ± 0.10 | 0.317 c | 0.06 ± 0.07 | 0.317 d | 0.04 ± 0.07 | 0.655 e | 0.00 ± 0.01 | 0.317 f | 0.02 ± 0.04 | 0.999 g | |
| p-value | 0.519 | 0.043 *,a | 0.234 a | 0.083 a | 0.129 a | 0.639 a | 0.648 a | ||||||
| LogMAR VA AE | |||||||||||||
| Baseline | 1 month | 3 months | 6 months | 9 months | 12 months | 18 months | |||||||
| PL Patching | 0.45 ± 0.38 | 0.25 ± 0.26 | 0.001 b,* | 0.20 ± 0.28 | 0.063 c | 0.20 ± 0.24 | 0.262 d | 0.19 ± 0.22 | 0.063 e | 0.19 ± 0.23 | 0.273 f | 0.26 ± 0.37 | 0.109 g |
| 0.30 ± 0.20 | 0.21 ± 0.19 | 0.018 b,* | 0.13 ± 0.11 | 0.655 c | 0.16 ± 0.14 | 0.317 d | 0.12 ± 0.15 | 0.655 e | 0.09 ± 0.10 | 0.180 f | 0.06 ± 0.06 | 0.285 g | |
| p-value | 0.350 a | 0.877 a | 0.924 a | 0.840 a | 0.679 a | 0.755 a | 0.368 a | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Rodríguez, C.J.; Fukumitsu, H.; Ruiz-Fortes, P.; Soto-Negro, R.; Merino-Suárez, M.; Piñero, D.P. Efficacy of Perceptual Learning-Based Vision Training as an Adjuvant to Occlusion Therapy in the Management of Amblyopia: A Pilot Study. Vision 2021, 5, 15. https://doi.org/10.3390/vision5010015
Hernández-Rodríguez CJ, Fukumitsu H, Ruiz-Fortes P, Soto-Negro R, Merino-Suárez M, Piñero DP. Efficacy of Perceptual Learning-Based Vision Training as an Adjuvant to Occlusion Therapy in the Management of Amblyopia: A Pilot Study. Vision. 2021; 5(1):15. https://doi.org/10.3390/vision5010015
Chicago/Turabian StyleHernández-Rodríguez, Carlos Javier, Hideki Fukumitsu, Pedro Ruiz-Fortes, Roberto Soto-Negro, María Merino-Suárez, and David P. Piñero. 2021. "Efficacy of Perceptual Learning-Based Vision Training as an Adjuvant to Occlusion Therapy in the Management of Amblyopia: A Pilot Study" Vision 5, no. 1: 15. https://doi.org/10.3390/vision5010015
APA StyleHernández-Rodríguez, C. J., Fukumitsu, H., Ruiz-Fortes, P., Soto-Negro, R., Merino-Suárez, M., & Piñero, D. P. (2021). Efficacy of Perceptual Learning-Based Vision Training as an Adjuvant to Occlusion Therapy in the Management of Amblyopia: A Pilot Study. Vision, 5(1), 15. https://doi.org/10.3390/vision5010015