Combined Branch Retinal Artery and Central Retinal Vein Occlusion: A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria for Considering Studies for This Review
2.2. Search Methods for Identifying Studies
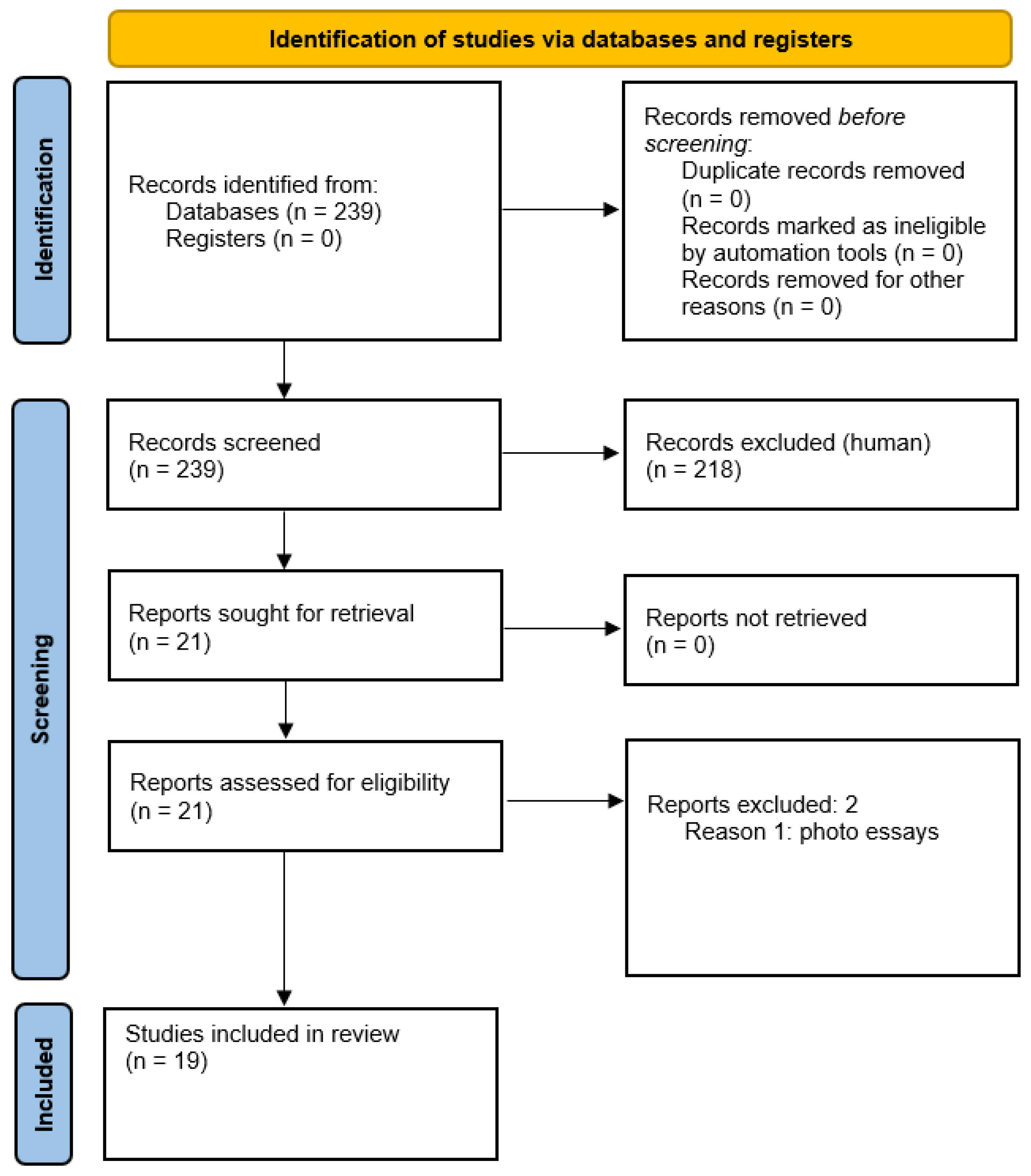
2.3. Study Selection
2.4. Data Collection and Risk of Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duker, J.S.; Cohen, M.S.; Brown, G.C.; Sergott, R.C.; McNamara, J.A. Combined branch retinal artery and central retinal vein obstruction. Retina 1990, 10, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Tavola, A.; D’Angelo, S.V.; Bandello, F.; Brancato, R.; Parlavecchia, M.; Safa, O.; D’Angelo, A. Central retinal vein and branch artery occlusion associated with inherited plasminogen deficiency and high lipoprotein(a) levels: A case report. Thromb. Res. 1995, 80, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.J. Branch retinal artery obstruction with simultaneous central retinal vein occlusion. Eye 2001, 15, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Rubio, J.E., Jr.; Charles, S. Interferon-associated combined branch retinal artery and central retinal vein obstruction. Retina 2003, 23, 546–548. [Google Scholar] [CrossRef]
- Özdek, Ş.; Yülek, F.; Gürelik, G.; Aydin, B.; Hasanreisoğlu, B. Simultaneous central retinal vein and retinal artery branch occlusions in two patients with homocysteinaemia. Eye 2004, 18, 942–945. [Google Scholar] [CrossRef] [Green Version]
- Nicolò, M.; Artioli, S.; La Mattina, G.C.; Ghiglione, D.; Calabria, G. Branch retinal artery occlusion combined with branch retinal vein occlusion in a patient with hepatitis C treated with interferon and ribavirin. Eur. J. Ophthalmol. 2005, 15, 811–814. [Google Scholar] [CrossRef] [Green Version]
- Bajaire, B.J.; Paipilla, D.F.; Arrieta, C.E.; Oudovitchenko, E. Mixed vascular occlusion in a patient with interferon-associated retinopathy. Case Rep. Ophthalmol. 2011, 2, 23–29. [Google Scholar] [CrossRef]
- Watanabe, M.; Ogasawara, S.; Takahashi, A.; Takada, J.; Tanaka, Y.; Okuwaki, Y.; Minamino, T.; Hidaka, H.; Nakazawa, T.; Shibuya, A.; et al. Branch retinal artery occlusion and central retinal vein occlusion associated with pegylated interferon plus ribavirin combination therapy for chronic hepatitis C. Cutan. Ocul. Toxicol. 2012, 31, 253–257. [Google Scholar] [CrossRef]
- Jenisch, T.; Dietrich-Ntoukas, T.; Renner, A.B.; Helbig, H.; Gamulescu, M.A. Kombinierter retinaler arteriovenöser Verschluss unter Interferon-β-Therapie [Combined retinal artery and vein occlusions associated with interferon beta therapy]. Ophthalmologe 2012, 109, 71–75. [Google Scholar] [CrossRef]
- Karapetyan, A.; Ouyang, P.; Tang, L.S.; Zeng, J.; Ying, M.D. Detection of underdiagnosed concurrent branch retinal artery occlusion in a patient with central retinal vein occlusion using spectral domain optical coherence tomography. BMC Ophthalmol. 2014, 14, 91. [Google Scholar] [CrossRef] [Green Version]
- Ozturk, T.; Takes, O.; Saatci, A.O. Dexamethasone implant (Ozurdex) in a case with unilateral simultaneous central retinal vein and branch retinal artery occlusion. Case Rep. Ophthalmol. 2015, 6, 76–81. [Google Scholar] [CrossRef]
- Parchand, S.M. Combined central retinal vein and branch retinal artery occlusion in hyperhomocysteinaemia. BMJ Case Rep. 2016, 2016, bcr2016218379. [Google Scholar] [CrossRef] [Green Version]
- Coca, M.; Tecle, N.; Made, W.; Mehta, A. Combined Central Retinal Vein and Branch Retinal Artery Occlusion Post Intense Physical Activity. Cureus 2017, 9, e1600. [Google Scholar] [CrossRef] [Green Version]
- Raval, V.; Nayak, S.; Saldanha, M.; Jalali, S.; Pappuru, R.R.; Narayanan, R.; Das, T. Combined retinal vascular occlusion: Demography, clinical features, visual outcome, systemic co-morbidities, and literature review. Indian. J. Ophthalmol. 2020, 68, 2136–2142. [Google Scholar] [CrossRef]
- Arrigo, A.; Knutsson, K.A.; Rajabjan, F.; Augustin, V.A.; Bandello, F.; Parodi, M.B. Combined central retinal vein occlusion and branch retinal artery occlusion treated with intravitreal dexamethasone implant: A case report. Eur. J. Ophthalmol. 2021, 31, NP74–NP76. [Google Scholar] [CrossRef]
- Goel, N. Concurrent branch retinal artery occlusion in central retinal vein occlusion: 3 cases reports and literature review. Saudi J. Ophthalmol. 2021, 34, 212–215. [Google Scholar] [CrossRef]
- Rosenbaum, P.S.; Srinivasan, S.; Zelefsky, J.R.; Mayers, M.; Moradi, I.E. Branch retinal artery occlusion and non-ischemic central retinal vein occlusion due to hyperhomocysteinemia in a 14-year-old child. J. Pediatr. Ophthalmol. Strabismus 2010, 47, e1–e4. [Google Scholar] [CrossRef]
- Kumar, K.; Dan, S.; Sinha, T.K.; Bhattacharya, D. Severe Vaso-Occlusive Retinopathy in Systemic Lupus Erythematosus: A Case Series. Cureus 2021, 13, e13019. [Google Scholar] [CrossRef]
- Panigrahi, P.K.; Navyasree, C.; Srija, Y.N. Combined central retinal vein occlusion with branch retinal artery occlusion in a leukaemic patient with COVID-19. Clin. Exp. Optom. 2022, 1–2. [Google Scholar] [CrossRef]
- Richards, R.P. Simultaneous occlusion of the central retinal artery and vein. Trans. Am. Ophthalmol. Soc. 1979, 77, 191–209. [Google Scholar]
- McLeod, D.; Ring, C.P. Cilioretinal infarction after retinal vein occlusion. Br. J. Ophthalmol. 1976, 60, 419–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayreh, S.S.; Fraterrigo, L.; Jonas, J. Central retinal vein occlusion associated with cilioretinal artery occlusion. Retina 2008, 28, 581–594. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S. Combined branch retinal artery and vein occlusion in hyperhomocysteinemia. JAMA Ophthalmol. 2014, 132, 1255. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Saurabh, K.; Roy, R. Combined central retinal vein occlusion and branch retinal artery occlusion. Indian J. Ophthalmol. 2018, 66, 1862–1863. [Google Scholar] [CrossRef]
- Hayreh, S.S.; Podhajsky, P.A.; Zimmerman, M.B. Branch retinal artery occlusion—Natural history of visual outcome. Ophthalmology 2009, 116, 1188–1195. [Google Scholar] [CrossRef] [Green Version]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G.S. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology 2020, 127, P259–P287. [Google Scholar] [CrossRef] [Green Version]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G.S. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology 2020, 127, P288–P320. [Google Scholar] [CrossRef] [Green Version]
- Rahimy, E.; Sarraf, D.; Dollin, M.L.; Pitcher, J.D.; Ho, A.C. Paracentral acute middle maculopathy in nonischemic central retinal vein occlusion. Am. J. Ophthalmol. 2014, 158, 372–380.e1. [Google Scholar] [CrossRef]
- Rentiya, Z.S.; Wells, M.; Bae, J.; Chen, K.J.; Chao, A.N.; Turgeon, N.; Shah, S.M.; Hanout, M. Interferon-α-induced retinopathy in chronic hepatitis C treatment: Summary, considerations, and recommendations. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 447–452. [Google Scholar] [CrossRef]
- Haller, J.A.; Bandello, F.; Belfort, R., Jr.; Blumenkranz, M.S.; Gillies, M.; Heier, J.; Loewenstein, A.; Yoon, Y.H.; Jiao, J.; Li, X.Y.; et al. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology 2011, 118, 2453–2460. [Google Scholar] [CrossRef]


{kind=link}
| Patient | Gender/Age (Years) | Eye & Arterial Branch | CRVO | Visual Acuity at Onset | Final Visual Outcome | Vascular Risk Factors | Therapy |
|---|---|---|---|---|---|---|---|
| 1 (Duker et al. 1990, US) [1] | F/24 | L.E.; infero-temporal | Nonischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/30 [0.66 D.E.] (7 months) * | No | Systemic steroids |
| 2 (Duker et al. 1990, US) [1] | M/42 | R.E.; supero-temporal | Nonischemic | 20/70 [0.29 D.E.] | 20/25 [0.8 D.E.] (2 months) * | No | No therapy |
| 3 (Duker et al. 1990, US) [1] | M/20 | R.E.; supero-temporal | Nonischemic | 20/20 [1 D.E.] | 20/20 [1 D.E.] (3 months) * | No | No therapy |
| 4 (Duker et al. 1990, US) [1] | M/62 | L.E.; supero-temporal | Nonischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/40 [0.5 D.E.] (6 years) * | Yes | Aspirin and carbonic anydrase inhibitor |
| 5 (Duker et al. 1990, US) [1] | M/65 | L.E.; infero-temporal | Nonischemic | 20/20 [1 D.E.] | 20/20 [1 D.E.] (not reported) * | No | Aspirin |
| 6 (Duker et al. 1990, US) [1] | F/53 | R.E.; infero-temporal | Ischemic | 20/20,000 (H.M.) [0.001 D.E.] | 20/2000 (C.F.) [0.01 D.E.] (4 years) * | Yes | Aspirin and dipyridimole |
| 7 (Duker et al. 1990, US) [1] | M/85 | R.E.; supero-temporal | Ischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/2000 (C.F.) [0.01 D.E.] (2 years) * | No | No therapy |
| 8 (Tavola et al. 1995, Italy) [2] | F/45 | R.E.; supero-temporal | Ischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/2000 (C.F.) [0.01 D.E.] (3 months) * | Yes | Warfarin |
| 9 (Singh 2001, UK) [3] | F/28 | R.E.; supero-temporal | Nonischemic | 20/60 [0.33 D.E.] | 20/125 [0.16 D.E.] (9 months) * | No | No therapy |
| 10 (Rubio & Charles 2003, US) [4] | M/51 | L.E.; infero-temporal | Nonischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/20000 (H.M.) [0.001 D.E.] (not reported) * | Yes | Aspirin and topical timolol |
| 11 (Özdek et al. 2004, Turkey) [5] | M/38 | R.E.; infero-temporal | Nonischemic | 20/60 [0.33 D.E.] | 20/20 [1 D.E.] (6 months) * | Yes | Mannitol infusion, acetazolamide, folic acid |
| 12 (Özdek et al. 2004, Turkey) [5] | M/25 | R.E.; infero-temporal | Nonischemic | 20/50 [0.4 D.E.] | 20/25 [0.8 D.E.] (5 months) * | Yes | Mannitol infusion, acetazolamide, folic acid |
| 13 (Nicolò et al. 2005, Itay) [6] | M/29 | L.E.; infero-temporal | Ischemic | 20/320 [0.06 D.E.] | 20/320 [0.06 D.E.] (not reported) * | Yes | No therapy |
| 14 (Rosenbaum et al. 2010, US) [17] | F/14 | L.E.; infero-temporal | Nonischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/50 [0.4 D.E.] (4 weeks) * | Yes | Vitamin B6 supplementation |
| 15 (Bajare et al. 2011, Colombia) [7] | F/45 | L.E.; supero-temporal | Ischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/20000 (H.M.) [0.001 D.E.] (3 years) * | Yes | Intravitreal bevacizumab |
| 16 (Watanabe et al. 2012, Japan) [8] | M/62 | R.E.; supero-temporal | Nonischemic | 20/400 [0.05 D.E.] | 20/400 [0.05 D.E.] (16 months) * | Yes | Eye-drops for IOP reduction |
| 17 (Jenisch et al. 2012, Germany) [9] | F/44 | R.E.; infero-temporal | Nonischemic | 20/500 [0.04 D.E.] | 20/25 [0.8 D.E.] (6 weeks) * | Yes | Aspirin |
| 18 (Karapetyan et al. 2014, China) [10] | F/51 | R.E.; supero-temporal | Nonischemic | 20/320 [0.06 D.E.] | 20/60 [0.33 D.E.] (4 weeks) * | No | Periocular triamcinolone acetonide |
| 19 (Ozturk et al. 2015, Turkey) [11] | M/30 | R.E.; supero-temporal | Nonischemic | 20/20,000 (H.M.) [0.001 D.E.] | 20/25 [0.8 D.E.] (6 months) * | Yes | Mannitol infusion, ant. chamber paracentesis, Ozurdex® |
| 20 (Parchand 2016, India) [12] | F/30 | R.E.; supero-temporal | Nonischemic | 20/80 [0.25 D.E.] | 20/40 [0.5 D.E.] (6 months) * | Yes | Folic acid, pyridoxine |
| 21 (Coca et al. 2017, US) [13] | M/47 | R.E.; infero-temporal | Nonischemic | 20/20 [1 D.E.] | 20/20 [1 D.E.] (1 month) * | No | Topical timolol |
| 22 (Raval et al. 2020, India) [14] | M/52 | L.E.; infero-temporal | Ischemic | 20/2000 (C.F.) [0.01 D.E.] | 20/20000 (H.M.) [0.001 D.E.] (9 months) * | Yes | Intravitreal bevacizumab, panretinal photocoagulation |
| 23 (Arrigo et al. 2021, Italy) [15] | M/51 | L.E.; infero-temporal | Ischemic | 20/40 [0.5 D.E.] | 20/20 [1 D.E.] (2 years) * | No | Ozurdex® |
| 24 (Goel 2021, India) [16] | F/52 | R.E.; supero-temporal | Nonischemic | 20/60 [0.33 D.E.] | 20/40 [0.5 D.E.] (6 weeks) * | No | No therapy |
| 25 (Goel 2021, India) [16] | F/48 | R.E.; supero-temporal | Nonischemic | 20/40 [0.5 D.E.] | Not reported | No | No therapy |
| 26 (Goel 2021, India) [16] | F/45 | R.E.; supero-temporal | Nonischemic | 20/60 [0.33 D.E.] | Not reported | No | No therapy |
| 27 (Kumar et al. 2021, India) [18] | F/51 | R.E.; infero-temporal | Ischemic | 20/40 [0.5 D.E.] | 20/60 [0.33 D.E.] (6 months) * | Yes | Systemic steroids, LMWH, intravitreal ranimizumab |
| 28 (Kumar et al. 2021, India) [18] | M/34 | L.E.; infero-temporal | Nonischemic | 20/20,000 (H.M.) [0.001 D.E.] | 20/20000 (H.M.) [0.001 D.E.] (6 months) * | Yes | Systemic steroids, LMWH, intravitreal ranimizumab |
| 29 (Panigrahi et al. 2022, India) [19] | F/23 | R.E.; superotemporal | Nonischemic | 20/30 [0.66 D.E.] | Not reported | Yes | Systemic anticoagulants |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinna, A.; Zinellu, A.; Serra, R.; Boscia, G.; Ronchi, L.; Dore, S. Combined Branch Retinal Artery and Central Retinal Vein Occlusion: A Systematic Review. Vision 2023, 7, 51. https://doi.org/10.3390/vision7030051
Pinna A, Zinellu A, Serra R, Boscia G, Ronchi L, Dore S. Combined Branch Retinal Artery and Central Retinal Vein Occlusion: A Systematic Review. Vision. 2023; 7(3):51. https://doi.org/10.3390/vision7030051
Chicago/Turabian StylePinna, Antonio, Angelo Zinellu, Rita Serra, Giacomo Boscia, Lorenza Ronchi, and Stefano Dore. 2023. "Combined Branch Retinal Artery and Central Retinal Vein Occlusion: A Systematic Review" Vision 7, no. 3: 51. https://doi.org/10.3390/vision7030051
APA StylePinna, A., Zinellu, A., Serra, R., Boscia, G., Ronchi, L., & Dore, S. (2023). Combined Branch Retinal Artery and Central Retinal Vein Occlusion: A Systematic Review. Vision, 7(3), 51. https://doi.org/10.3390/vision7030051