Utilization of Mirror Visual Feedback for Upper Limb Function in Poststroke Patients: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Study Selection
2.3.1. Inclusion Criteria
- Participants: Only studies involving stroke patients are considered eligible for inclusion. The participants’ characteristics, such as age, gender, and stroke severity, are taken into account.
- Intervention: Only interventional studies that evaluate the use of MVF for upper limb rehabilitation are included. MVF therapy involves the use of mirrors to provide visual feedback to stroke patients during rehabilitation exercises.
- Outcomes: All outcome variables related to cognition are included in the review. This could include measures of cognitive function, such as attention, memory, executive function, and language. If three or more identical outcome variables are reported across studies, they are synthesized for quantitative analysis.
- Type of studies: Only published randomized controlled trials (RCTs) are included.
2.3.2. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
- Random sequence generation: The method used to generate the random sequence allocation was assessed to determine whether it was conducted adequately and with minimal risk of bias.
- Allocation concealment: The process of concealing the allocation sequence from the researchers or participants was evaluated to assess whether it effectively prevented selection bias.
- Blinding of participants and personnel: The extent to which participants and personnel involved in the study were blinded to the intervention being evaluated was assessed. Blinding helps to minimize performance bias and the influence of knowledge or expectations on study outcomes.
- Blinding of outcome assessment: The assessment of outcomes by independent evaluators who are blinded to the intervention was evaluated to minimize detection bias.
- Incomplete outcome data: The extent to which data were missing or incomplete and whether this could introduce bias in the results was assessed. Additionally, the appropriateness of any statistical methods used to handle missing data was considered.
- Selective reporting: The completeness of outcome reporting was assessed to identify any potential bias due to selective reporting of outcomes.
- Other biases: Any other potential sources of bias not covered by the above domains, such as conflicts of interest or funding sources, were evaluated.
2.6. Data Synthesis and Meta-Analysis
2.7. Ethical Considerations
3. Results
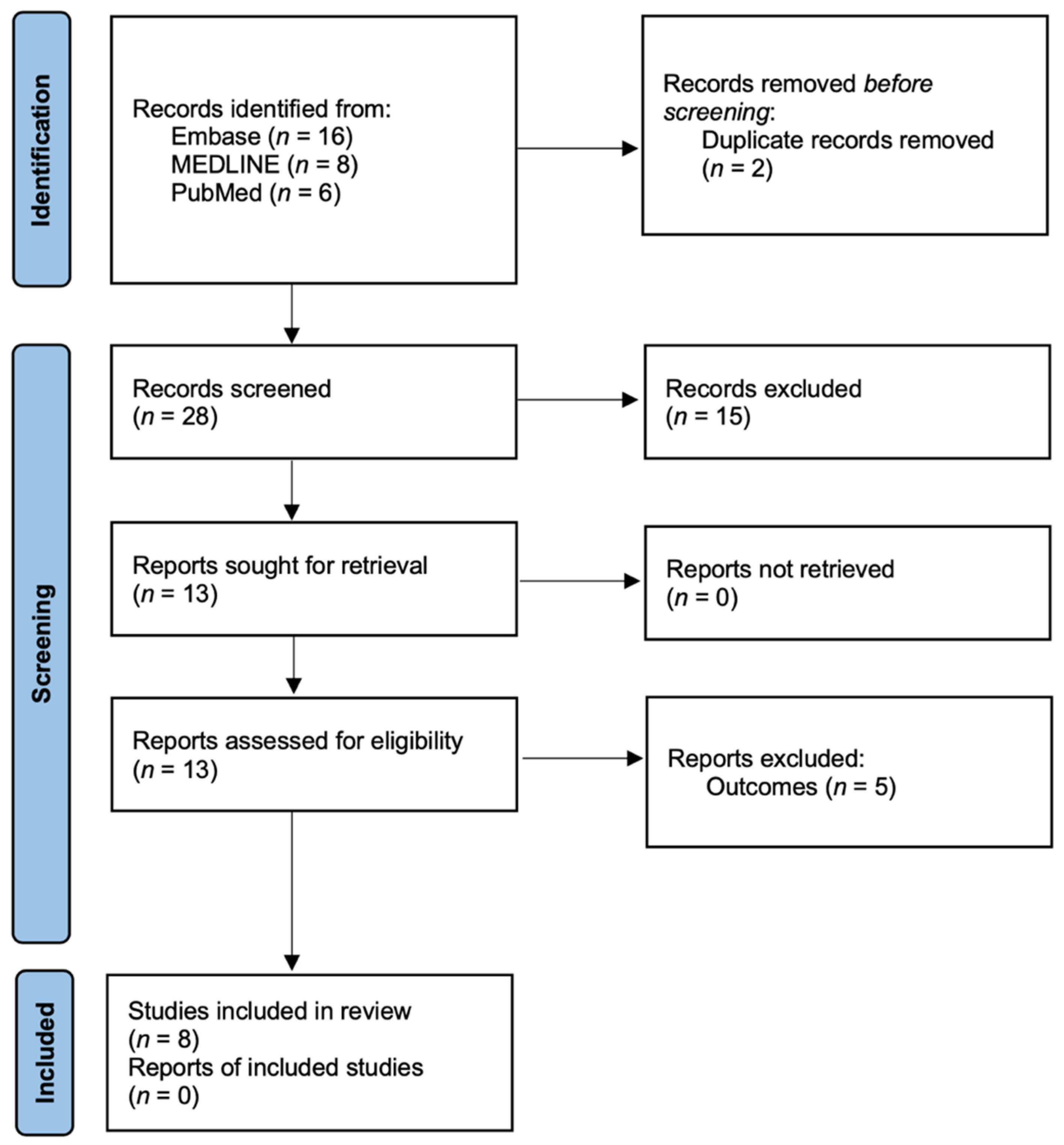
3.1. Literature Search and Characteristics of the Included Trials
3.2. Assessment of Methodological Risk of Bias
3.3. Mirror Visual Feedback in Patients with Mild Poststroke
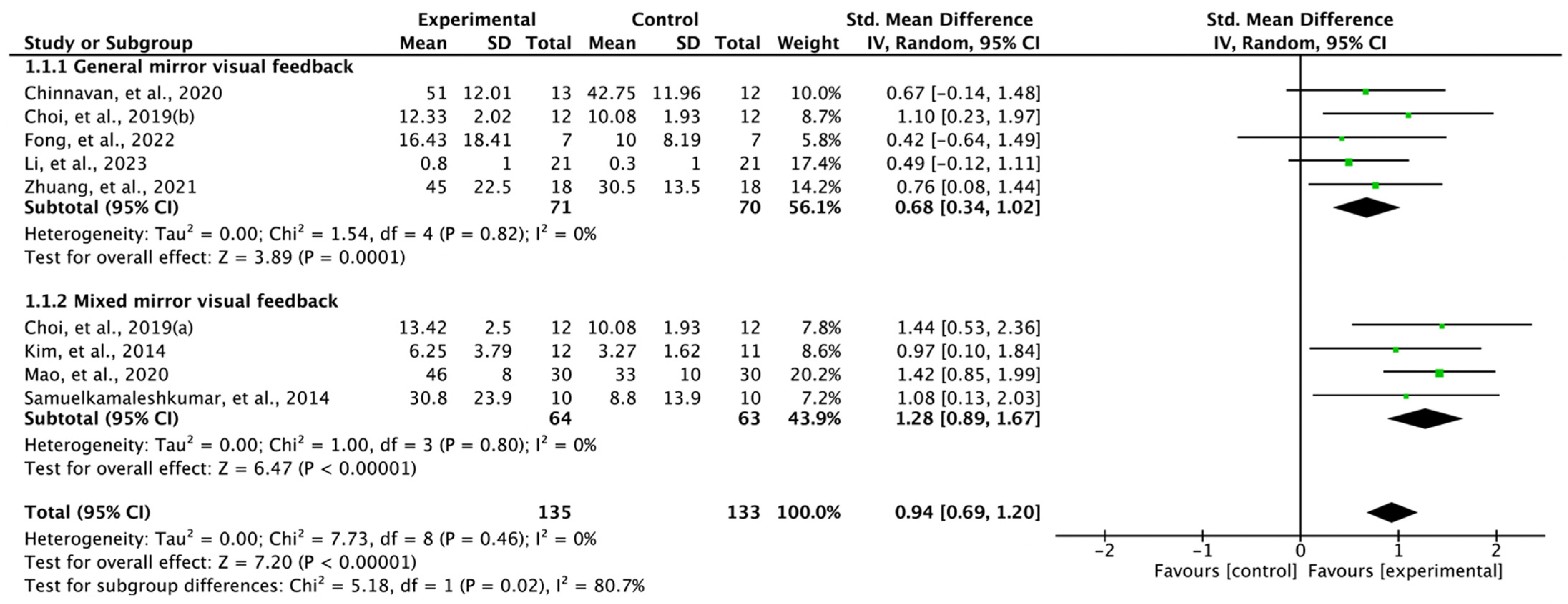
3.4. Effectiveness of Mirror Visual Feedback in Treating Poststroke Patients
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for Improving Upper Limb Function after Stroke. Cochrane Database Syst. Rev. 2014, 2014, Cd010820. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, P. Upper Limb Motor Impairment after Stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Bernardo-Filho, M.; Bemben, M.G.; Taiar, R.; Sañudo, B.; Furness, T.; Clark, B.C. Editorial: Interventional Strategies for Enhancing Quality of Life and Health Span in Older Adults. Front. Aging Neurosci. 2020, 12, 253. [Google Scholar] [CrossRef] [PubMed]
- Xue, S.; Zhou, X.; Yang, Z.H.; Si, X.K.; Sun, X. Stroke-Induced Damage on the Blood-Brain Barrier. Front. Neurol. 2023, 14, 1248970. [Google Scholar] [CrossRef]
- Lekoubou, A.; Nguyen, C.; Kwon, M.; Nyalundja, A.D.; Agrawal, A. Post-Stroke Everything. Curr. Neurol. Neurosci. Rep. 2023, 1–16. [Google Scholar] [CrossRef]
- Kuriakose, D.; Xiao, Z. Pathophysiology and Treatment of Stroke: Present Status and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 7609. [Google Scholar] [CrossRef]
- Dobkin, B.H. Strategies for Stroke Rehabilitation. Lancet Neurol. 2004, 3, 528–536. [Google Scholar] [CrossRef]
- Dobkin, B.H. The Clinical Science of Neurologic Rehabilitation; Oxford University Press: Oxford, UK, 2003; Volume 67. [Google Scholar]
- Madhoun, H.Y.; Tan, B.; Feng, Y.; Zhou, Y.; Zhou, C.; Yu, L. Task-Based Mirror Therapy Enhances the Upper Limb Motor Function in Subacute Stroke Patients: A Randomized Control Trial. Eur. J. Phys. Rehabil. Med. 2020, 56, 265–271. [Google Scholar] [CrossRef]
- Herrador Colmenero, L.; Marmol, J.M.P.; Martí-García, C.; Zaldivar, M.Q.; Haro, R.M.T.; Sánchez, A.M.C.; Aguilar-Ferrándiz, M.E. Effectiveness of Mirror Therapy, Motor Imagery, and Virtual Feedback on Phantom Limb Pain Following Amputation: A Systematic Review. Prosthet. Orthot. Int. 2018, 42, 288–298. [Google Scholar] [CrossRef]
- Kundi, M.K.; Spence, N.J. Efficacy of Mirror Therapy on Lower Limb Motor Recovery, Balance and Gait in Subacute and Chronic Stroke: A Systematic Review. Physiother. Res. Int. 2023, 28, e1997. [Google Scholar] [CrossRef]
- Fong, K.N.K.; Ting, K.H.; Zhang, X.; Yau, C.S.F.; Li, L.S.W. The Effect of Mirror Visual Feedback on Spatial Neglect for Patients after Stroke: A Preliminary Randomized Controlled Trial. Brain Sci. 2022, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Gámez Santiago, A.B.; Cáceres, C.M.M.; Hernández-Morante, J.J. Effectiveness of Intensively Applied Mirror Therapy in Older Patients with Post-Stroke Hemiplegia: A Preliminary Trial. Eur. Neurol. 2022, 85, 291–299. [Google Scholar] [CrossRef]
- İkizler May, H.; Özdolap, Ş.; Mengi, A.; Sarıkaya, S. The Effect of Mirror Therapy on Lower Extremity Motor Function and Ambulation in Post-Stroke Patients: A Prospective, Randomized-Controlled Study. Turk. J. Phys. Med. Rehabil. 2020, 66, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.D.C.B.; Silva, D.R.C.; Cortez, B.V.; Coêlho, C.; Silva, F.; de Oliveira, G.; de Sá-Caputo, D.C.; Tavares-Oliveira, A.C.; Bernardo-Filho, M.; Silva, J.M. Mirror and Vibration Therapies Effects on the Upper Limbs of Hemiparetic Patients after Stroke: A Pilot Study. Rehabil. Res. Pract. 2018, 2018, 6183654. [Google Scholar] [CrossRef] [PubMed]
- Deconinck, F.J.; Smorenburg, A.R.; Benham, A.; Ledebt, A.; Feltham, M.G.; Savelsbergh, G.J. Reflections on Mirror Therapy: A Systematic Review of the Effect of Mirror Visual Feedback on the Brain. Neurorehabil. Neural Repair 2015, 29, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.S.; Rogers-Ramachandran, D. Mirror Feedback Assisted Recovery from Hemiparesis Following Stroke. In Reply to Morkisch et al.: How to Perform Mirror Therapy after Stroke? Evidence from a Meta-Analysis. Restor. Neurol. Neurosci. 2019, 37, 437–443. [Google Scholar] [CrossRef]
- Einstad, M.S.; Saltvedt, I.; Lydersen, S.; Ursin, M.H.; Munthe-Kaas, R.; Ihle-Hansen, H.; Knapskog, A.B.; Askim, T.; Beyer, M.K.; Næss, H.; et al. Associations between Post-Stroke Motor and Cognitive Function: A Cross-Sectional Study. BMC Geriatr. 2021, 21, 103. [Google Scholar] [CrossRef]
- Yeh, T.T.; Wu, C.Y.; Hsieh, Y.W.; Chang, K.C.; Lee, L.C.; Hung, J.W.; Lin, K.C.; Teng, C.H.; Liao, Y.H. Synergistic Effects of Aerobic Exercise and Cognitive Training on Cognition, Physiological Markers, Daily Function, and Quality of Life in Stroke Survivors with Cognitive Decline: Study Protocol for a Randomized Controlled Trial. Trials 2017, 18, 405. [Google Scholar] [CrossRef]
- Cumming, T.B.; Churilov, L.; Collier, J.; Donnan, G.; Ellery, F.; Dewey, H.; Langhorne, P.; Lindley, R.I.; Moodie, M.; Thrift, A.G.; et al. Early Mobilization and Quality of Life after Stroke: Findings from Avert. Neurology 2019, 93, e717–e728. [Google Scholar] [CrossRef]
- Patel, J.J.; Hill, A.; Lee, Z.Y.; Heyland, D.K.; Stoppe, C. Critical Appraisal of a Systematic Review: A Concise Review. Crit. Care Med. 2022, 50, 1371–1379. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Cochrane Statistical Methods Group. Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot–Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Chinnavan, E.; Ragupathy, R.; Wah, Y.C. Effectiveness of Mirror Therapy on Upper Limb Motor Functions among Hemiplegic Patients. Bangladesh J. Med. Sci. 2020, 19, 208–213. [Google Scholar] [CrossRef]
- Choi, H.S.; Shin, W.S.; Bang, D.H. Mirror Therapy Using Gesture Recognition for Upper Limb Function, Neck Discomfort, and Quality of Life after Chronic Stroke: A Single-Blind Randomized Controlled Trial. Med. Sci. Monit. 2019, 25, 3271–3278. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, G.; Song, C. Effect of Functional Electrical Stimulation with Mirror Therapy on Upper Extremity Motor Function in Poststroke Patients. J. Stroke Cerebrovasc. Dis. 2014, 23, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Lin, K.C.; Chen, C.L.; Yao, G.; Ya-Ju, C.; Lee, Y.Y.; Liu, C.T.; Chen, W.S. Three Ways to Improve Arm Function in the Chronic Phase after Stroke by Robotic Priming Combined with Mirror Therapy, Arm Training, and Movement-Oriented Therapy. Arch. Phys. Med. Rehabil. 2023, 104, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Li, Y.; Tang, L.; Chen, Y.; Ni, J.; Liu, L.; Shan, C. Effects of Mirror Neuron System-Based Training on Rehabilitation of Stroke Patients. Brain Behav. 2020, 10, e01729. [Google Scholar] [CrossRef] [PubMed]
- Samuelkamaleshkumar, S.; Reethajanetsureka, S.; Pauljebaraj, P.; Benshamir, B.; Padankatti, S.M.; David, J.A. Mirror Therapy Enhances Motor Performance in the Paretic Upper Limb after Stroke: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2014, 95, 2000–2005. [Google Scholar] [CrossRef]
- Zhuang, J.Y.; Ding, L.; Shu, B.B.; Chen, D.; Jia, J. Associated Mirror Therapy Enhances Motor Recovery of the Upper Extremity and Daily Function after Stroke: A Randomized Control Study. Neural Plast. 2021, 2021, 7266263. [Google Scholar] [CrossRef]
- Babic, A.; Pijuk, A.; Brázdilová, L.; Georgieva, Y.; Pereira, M.A.R.; Pericic, T.P.; Puljak, L. The Judgement of Biases Included in the Category “Other Bias” in Cochrane Systematic Reviews of Interventions: A Systematic Survey. BMC Med. Res. Methodol. 2019, 19, 77. [Google Scholar] [CrossRef]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Assessing Risk of Bias Due to Missing Results in a Synthesis. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 349–374. [Google Scholar]
- Zeng, W.; Guo, Y.; Wu, G.; Liu, X.; Fang, Q. Mirror Therapy for Motor Function of the Upper Extremity in Patients with Stroke: A Meta-Analysis. J. Rehabil. Med. 2018, 50, 8–15. [Google Scholar] [CrossRef]
- Morkisch, N.; Thieme, H.; Dohle, C. How to Perform Mirror Therapy after Stroke? Evidence from a Meta-Analysis. Restor. Neurol. Neurosci. 2019, 37, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Louie, D.R.; Lim, S.B.; Eng, J.J. The Efficacy of Lower Extremity Mirror Therapy for Improving Balance, Gait, and Motor Function Poststroke: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Zhou, Y.; He, H.; Lin, S.; Zhu, R.; Liu, Z.; Liu, J.; Liu, X.; Chen, S.; Zou, J.; et al. Synergistic Effect of Combined Mirror Therapy on Upper Extremity in Patients with Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 155. [Google Scholar] [CrossRef] [PubMed]
- Schick, T.; Schlake, H.P.; Kallusky, J.; Hohlfeld, G.; Steinmetz, M.; Tripp, F.; Krakow, K.; Pinter, M.; Dohle, C. Synergy Effects of Combined Multichannel Emg-Triggered Electrical Stimulation and Mirror Therapy in Subacute Stroke Patients with Severe or Very Severe Arm/Hand Paresis. Restor. Neurol. Neurosci. 2017, 35, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Amasyali, S.Y.; Yaliman, A. Comparison of the Effects of Mirror Therapy and Electromyography-Triggered Neuromuscular Stimulation on Hand Functions in Stroke Patients: A Pilot Study. Int. J. Rehabil. Res. 2016, 39, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.S.; Rogers-Ramachandran, D. Synaesthesia in Phantom Limbs Induced with Mirrors. Proc. Biol. Sci. 1996, 263, 377–386. [Google Scholar]
- Yavuzer, G.; Selles, R.; Sezer, N.; Sütbeyaz, S.; Bussmann, J.B.; Köseoğlu, F.; Atay, M.B.; Stam, H.J. Mirror Therapy Improves Hand Function in Subacute Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2008, 89, 393–398. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Fabbri-Destro, M.; Nuara, A.; Gatti, R.; Avanzini, P. The Role of Mirror Mechanism in the Recovery, Maintenance, and Acquisition of Motor Abilities. Neurosci. Biobehav. Rev. 2021, 127, 404–423. [Google Scholar] [CrossRef]
- Michielsen, M.E.; Smits, M.; Ribbers, G.M.; Stam, H.J.; van der Geest, J.N.; Bussmann, J.B.; Selles, R.W. The Neuronal Correlates of Mirror Therapy: An Fmri Study on Mirror Induced Visual Illusions in Patients with Stroke. J. Neurol. Neurosurg. Psychiatry 2011, 82, 393–398. [Google Scholar] [CrossRef]
- Wasaka, T.; Kakigi, R. The Effect of Unpredicted Visual Feedback on Activation in the Secondary Somatosensory Cortex during Movement Execution. BMC Neurosci. 2012, 13, 138. [Google Scholar] [CrossRef]
- Wasaka, T.; Kakigi, R. Conflict Caused by Visual Feedback Modulates Activation in Somatosensory Areas during Movement Execution. Neuroimage 2012, 59, 1501–1507. [Google Scholar] [CrossRef]
- Fink, G.R.; Marshall, J.C.; Halligan, P.W.; Frith, C.D.; Driver, J.; Frackowiak, R.S.; Dolan, R.J. The Neural Consequences of Conflict between Intention and the Senses. Brain 1999, 122 Pt 3, 497–512. [Google Scholar] [CrossRef]
- Kang, Y.J.; Ku, J.; Kim, H.J.; Park, H.K. Facilitation of Corticospinal Excitability According to Motor Imagery and Mirror Therapy in Healthy Subjects and Stroke Patients. Ann. Rehabil. Med. 2011, 35, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Fukumura, K.; Sugawara, K.; Tanabe, S.; Ushiba, J.; Tomita, Y. Influence of Mirror Therapy on Human Motor Cortex. Int. J. Neurosci. 2007, 117, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Funase, K.; Tabira, T.; Higashi, T.; Liang, N.; Kasai, T. Increased Corticospinal Excitability During Direct Observation of Self-Movement and Indirect Observation with a Mirror Box. Neurosci. Lett. 2007, 419, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, J.; Brunetti, M.; Steinbrink, J.; Niedeggen, M.; Dohle, C. Effect of a Mirror-Like Illusion on Activation in the Precuneus Assessed with Functional Near-Infrared Spectroscopy. J. Biomed. Opt. 2013, 18, 066001. [Google Scholar] [CrossRef]
- Fritzsch, C.; Wang, J.; Santos, L.F.D.; Mauritz, K.-H.; Brunetti, M.; Dohle, C. Different Effects of the Mirror Illusion on Motor and Somatosensory Processing. Restor. Neurol. Neurosci. 2014, 32, 269–280. [Google Scholar] [CrossRef]
- Sharma, N.; Simmons, L.H.; Jones, P.S.; Day, D.J.; Carpenter, T.A.; Pomeroy, V.M.; Warburton, E.A.; Baron, J.C. Motor Imagery after Subcortical Stroke: A Functional Magnetic Resonance Imaging Study. Stroke 2009, 40, 1315–1324. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Sample Size | Duration | Upper Limb Function | Intervention (Therapeutic Intensity) | Authors’ Conclusion |
|---|---|---|---|---|---|
| Chinnavan et al., 2020 [24] | EG = 13 CG = 12 | 6 weeks | FMA | EG = Mirror therapy (3 times a week, 45 min per session. For the first 30 min, therapy is applied to the affected upper limb, and the remaining 15 min are applied to the unaffected upper limb only) CG = Conventional therapy (Mobilization, reaching, grasping and dexterity 3 times a week, 45 min per session) | Integrating conventional therapy with mirror therapy proves beneficial for upper limb motor function recovery in hemiplegic patients. |
| Choi et al., 2019 [25] | EG1 = 12 EG2 = 12 CG = 12 | 5 weeks | MFT | EG1 = Gesture recognition mirror therapy (30 min 3 times a week 3D-motion-input-device-based mirror therapy) EG2 = Mirror therapy (30 min per session, 3 times a week general mirror therapy) CG = Control (Sham 3 times a week, 30 min per session) | Mirror therapy utilizing gesture recognition devices enhances functionality, reduces neck discomfort, and improves life quality in chronic stroke survivors. |
| Fong et al., 2022 [12] | EG = 7 CG = 7 | 3 weeks | FMA | EG = Mirror therapy (30 min task-specific training 4 times a week) CG = Sham (Sham using a covered mirror 4 times a week, 30 min per session) | Mirror visual feedback is more effective than a covered mirror in mitigating spatial neglect symptoms, without a marked advantage over bilateral transparent glass movements. |
| Kim et al., 2014 [26] | EG = 12 CG = 11 | 5 weeks | FMA subcategory; hand | Both groups received conventional rehabilitation training for 60 min per session, 5 times a week. EG = FES with MT (5 times a week, 30 min per session) CG = FES without MT (5 times a week, 30 min per session) | The application of functional electrical stimulation alongside mirror therapy in poststroke care significantly advances upper extremity motor function. |
| Li et al., 2023 [27] | EG = 21 CG = 21 | 6 weeks | ABILHAND questionnaire | Both groups offer home programs 5 times a week EG = Bilateral robotic priming combined with mirror therapy 3 times a week, 90 min per session CG = Bilateral robotic priming combined with bilateral arm training 3 times a week, 90 min per session | Enhanced motor improvement in upper limbs is evident when mirror therapy is combined with bilateral robotic priming, with effects persisting for three months. |
| Mao et al., 2020 [28] | EG = 30 CG = 30 | 8 weeks | FMA | CT; Upper limb rehabilitation training (5 times a week, 60 min per session) and Schulte Grid training (5 times a week, 30 min per session) EG = MNSP (5 times a week, 20 min per session) plus CT CG = CT | A synergy of mirror-neuron-system-based training with conventional rehabilitation practices improves motor and cognitive functions in stroke-affected upper extremities. |
| Samuelkamaleshkumar et al., 2014 [29] | EG = 10 CG = 10 | 3 weeks | FMA | 5 times a week, 6 h per session PMRP EG = Mirror therapy (5 times a week, 1 h per session) plus PMRP CG = PMRP | The employment of mirror therapy in conjunction with bilateral arm training and graded tasks yields better motor performance in stroke-induced paretic upper limbs compared with conventional therapy. |
| Zhuang et al., 2021 [30] | EG = 18 CG = 18 | 4 weeks | FMA | EG = Associated mirror therapy CG = Control | Our research indicates that associated mirror therapy is an effective strategy for facilitating motor recovery and daily functioning in individuals with stroke-affected limbs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Lee, E.; Jung, J.; Lee, S. Utilization of Mirror Visual Feedback for Upper Limb Function in Poststroke Patients: A Systematic Review and Meta-Analysis. Vision 2023, 7, 75. https://doi.org/10.3390/vision7040075
Kim H, Lee E, Jung J, Lee S. Utilization of Mirror Visual Feedback for Upper Limb Function in Poststroke Patients: A Systematic Review and Meta-Analysis. Vision. 2023; 7(4):75. https://doi.org/10.3390/vision7040075
Chicago/Turabian StyleKim, Hyunjoong, Eunsang Lee, Jihye Jung, and Seungwon Lee. 2023. "Utilization of Mirror Visual Feedback for Upper Limb Function in Poststroke Patients: A Systematic Review and Meta-Analysis" Vision 7, no. 4: 75. https://doi.org/10.3390/vision7040075
APA StyleKim, H., Lee, E., Jung, J., & Lee, S. (2023). Utilization of Mirror Visual Feedback for Upper Limb Function in Poststroke Patients: A Systematic Review and Meta-Analysis. Vision, 7(4), 75. https://doi.org/10.3390/vision7040075