
Severe Odontogenic Infections during Pregnancy and Related Adverse Outcomes. Case Report and Systematic Literature Review

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Case
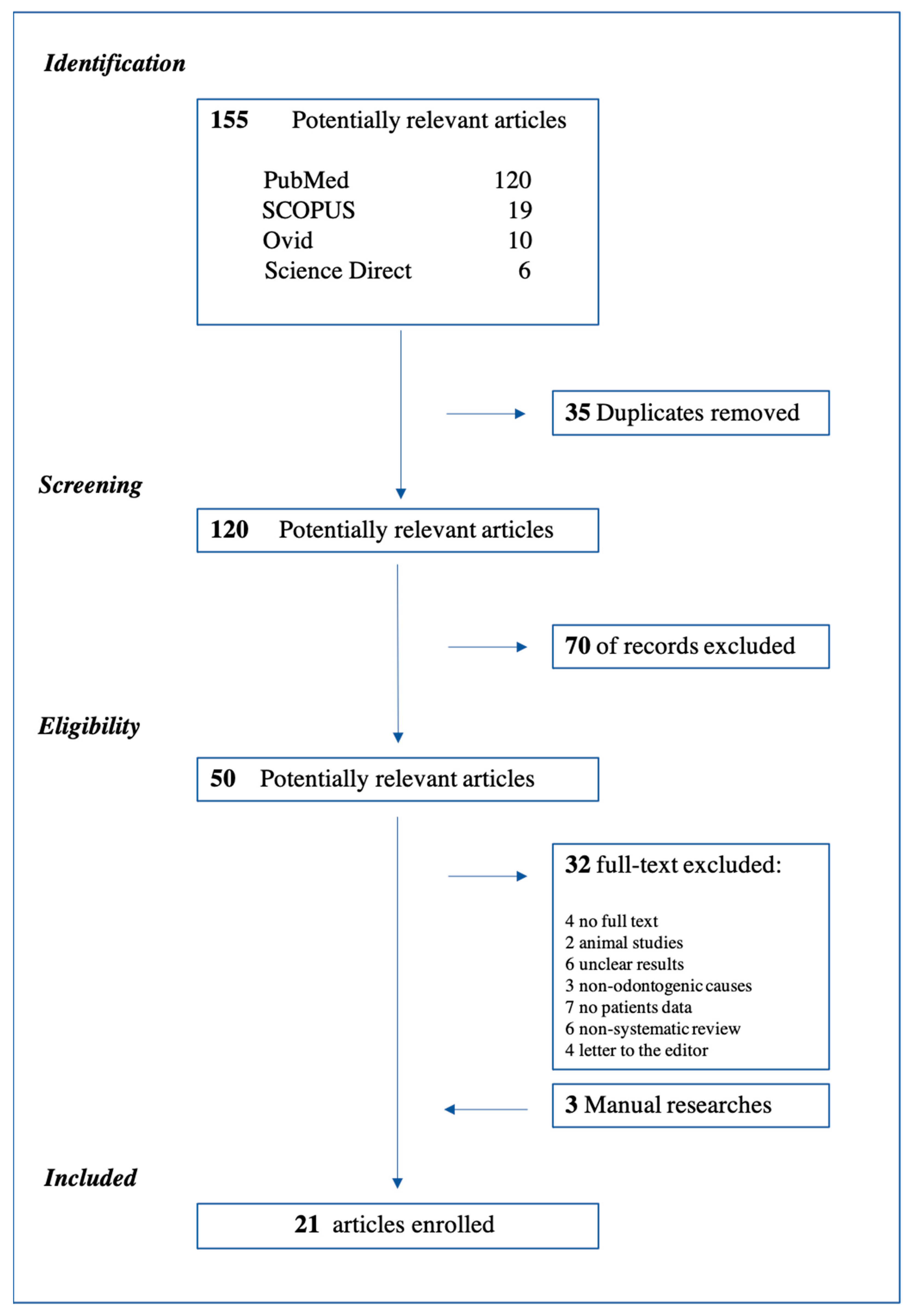
2.2. Systematic Literature Review
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weise, H.; Naros, A.; Weise, C.; Reinert, S.; Hoefert, S. Severe odontogenic infections with septic progress—A constant and increasing challenge: A retrospective analysis. BMC Oral Health 2019, 19, 173. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.; Cheng, A.; Kunchur, R.; Lam, S.; Sambrook, P.; Goss, A. Management of severe odontogenic infections in pregnancy. Aust. Dent. J. 2012, 57, 498–503. [Google Scholar] [CrossRef] [Green Version]
- Omeje, U.; Omeje, I.; Agbara, R. Severe Cervicofacial Cellulitis in Pregnancy—A Review of 18 Cases. Iran. J. Otorhinolaryngol. 2020, 32, 93–100. [Google Scholar] [CrossRef]
- Nuriel-Ohayon, M.; Neuman, H.; Koren, O. Microbial Changes during Pregnancy, Birth, and Infancy. Front. Microbiol. 2016, 7, 1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amar, S.; Chung, K.M. Influence of hormonal variation on the periodontium in women. Periodontology 2000 1994, 6, 79–87. [Google Scholar] [CrossRef]
- Villa, A.; Abati, S.; Pileri, P.; Calabrese, S.; Capobianco, G.; Strohmenger, L.; Ottolenghi, L.; Cetin, I.; Campus, G.G. Oral health and oral diseases in pregnancy: A multicentre survey of Italian postpartum women. Aust. Dent. J. 2013, 58, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Dalla Torre, D.; Burtscher, D.; Höfer, D.; Kloss, F.R. Odontogenic deep neck space infection as life-threatening condition in pregnancy. Aust. Dent. J. 2014, 59, 375–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doumbia-Singare, K.; Timbo, S.K.; Keita, M.; Mohamed, A.A.; Guindo, B.; Soumaoro, S. Cellulite cervico-faciale au cours de la grossesse. À propos d’une série de 10 cas au Mali [Cervico-facial cellulitis during pregnancy: About a series of 10 cases in Mali]. Bull. Soc. Pathol. Exot. 2014, 107, 312–316. [Google Scholar] [CrossRef]
- Osunde, O.; Bassey, G.; Ver-Or, N. Management of Ludwig’s Angina in Pregnancy: A Review of 10 Cases. Ann. Med. Health Sci. Res. 2014, 4, 361–364. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The University of Adelaide: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Fayek, S.; Isaac, P.; Shah, J. Awake fibre optic intubation in a 38-week pregnant patient with submandibular abscess. Int. J. Obstet. Anesth. 1994, 3, 103–105. [Google Scholar] [CrossRef]
- Martin, F.; Viviand, X.; Desbriere, R.; Boubli, L.; Martin, C. Faut-il monitorer le rythme cardiaque foetal au cours d’une anesthésie générale? [Do we have to monitor foetal heart rate during general anesthesia?]. Ann. Françaises d’Anesthésie Réanimation 2004, 23, 1179–1181. [Google Scholar] [CrossRef]
- Abramowicz, S.; Abramowicz, J.S.; Dolwick, M.F. Severe life threatening maxillofacial infection in pregnancy presented as Ludwig’s angina. Infect. Dis. Obstet. Gynecol. 2006, 2006, 051931. [Google Scholar] [CrossRef] [Green Version]
- Niederhauser, A.; Kirkwood, D.; Magann, E.F.; Mullin, P.M.; Morrison, J.C. Ludwig’s angina in pregnancy. J. Matern. Neonatal Med. 2006, 19, 119–120. [Google Scholar] [CrossRef]
- Soltero, R.; Mercado-Alvarado, J. Successful conservative management of Ludwig’s angina in advanced pregnancy. Bol. Asoc. Med. Puerto Rico 2009, 101, 42–43. [Google Scholar]
- Rana, A.S.; Lall, S.; Kala, G.; Tyagi, A. A rare case of simultaneous surgery of an odontogenic space infection and delivery by caesarean section in a pregnant patient. J. Maxillofac. Oral Surg. 2009, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Rajeev, S.; Panda, N.B.; Batra, Y.K. Anaesthetic management of Ludwig’s angina in pregnancy. Int. J. Obstet. Anesth. 2009, 18, 96–97. [Google Scholar] [CrossRef]
- Moorhead, K.; Guiahi, M. Pregnancy complicated by Ludwig’s angina requiring delivery. Infect. Dis. Obstet. Gynecol. 2010, 2010, 158264. [Google Scholar] [CrossRef] [Green Version]
- Hobson, D.T.G.; Imudia, A.N.; Soto, E.; Awonuga, A.O. Pregnancy complicated by recurrent brain abscess after extraction of an infected tooth. Obstet. Gynecol. 2011, 118 Pt 2, 467–470. [Google Scholar] [CrossRef]
- Çelebi, N.; Kütük, M.; Tas, M.; Soylu, E.; Etöz, O.; Alkan, A. Acute fetal distress following tooth extraction and abscess drainage in a pregnant patient with maxillofacial infection. Aust. Dent. J. 2013, 58, 117–119. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S.; Sharma, S.; Maru, L. Poor dental hygiene in pregnancy leading to submandibular cellulitis and intrauterine fetal demise: Case report and literature review. Int. J. Prev. Med. 2013, 4, 603–606. [Google Scholar] [PubMed]
- Kamath, A.T.; Bhagania, M.K.; Balakrishna, R.; Sevagur, G.K.; Amar, R. Ludwig’s Angina in Pregnancy Necessitating Pre Mature Delivery. J. Maxillofac. Oral Surg. 2012, 14 (Suppl. 1), 186–189. [Google Scholar] [CrossRef] [Green Version]
- Tocaciu, S.; Robinson, B.W.; Sambrook, P.J. Severe odontogenic infection in pregnancy: A timely reminder. Aust. Dent. J. 2017, 62, 98–101. [Google Scholar] [CrossRef] [Green Version]
- Pereira, R.D.S.; Gomes-Ferreira, P.H.S.; Bonardi, J.P.; Da Silva, J.R.; Latini, G.L.; Hochuli-Vieira, E. Dental Infection and Pregnancy: The Lack of Treatment by the Dental Professional Evolving to a Complex Maxillofacial Infection. J. Craniofacial Surg. 2017, 28, e748–e750. [Google Scholar] [CrossRef]
- Rahman, T.; Ahmed, S.; Rahman, S. Decompression of Ludwig’s angina in a pregnant patient under bilateral superficial cervical plexus block. J. Perioper. Pract. 2019, 27, 1750458919834195. [Google Scholar] [CrossRef]
- Ali, E.A.M.; Eltayeb, A.S.; Osman, M.A.K. Delay in the Referral of Pregnant Patients with Fascial Spaces Infection: A Cross-Sectional Observational Study from Khartoum Teaching Dental Hospital, Sudan. J. Maxillofac. Oral Surg. 2020, 19, 298–301. [Google Scholar] [CrossRef]
- Romero, B.C.; Chiquito, C.S.; Elejalde, L.E.; Bernardoni, C.B. Relationship between periodontal disease in pregnant women and the nutritional condition of their newborns. J. Periodontol. 2002, 73, 1177–1183. [Google Scholar] [CrossRef]
- Borgo, P.V.; Rodrigues, V.A.A.; Feitosa, A.C.R.; Xavier, K.C.B.; Avila-Campos, M.J. Association between periodontal condition and subgingival microbiota in women during pregnancy: A longitudinal study. J. Appl. Oral Sci. 2014, 22, 528–533. [Google Scholar] [CrossRef]
- Kurien, S.; Kattimani, V.S.; Sriram, R.R.; Sriram, S.K.; Bhupathi, A.; Bodduru, R.R.; Patil, N.N. Management of pregnant patient in dentistry. J. Int. Oral Health 2013, 5, 88–97. [Google Scholar]
- Freeman, R.K.; Vallières, E.; Verrier, E.D.; Karmy-Jones, R.; Wood, D.E. Descending necrotizing mediastinitis: An analysis of the effects of serial surgical debridement on patient mortality. J. Thorac. Cardiovasc. Surg. 2000, 119, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Giglio, J.A.; Lanni, S.M.; Laskin, D.M.; Giglio, N.W. Oral health care for the pregnant patient. J. Can. Dent. Assoc. 2009, 75, 43–48. [Google Scholar]
- Flynn, T.R.; Susarla, S.M. Oral and maxillofacial surgery for the pregnant patient. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 207–221. [Google Scholar] [CrossRef]
- Official Source Ministero della Salute Ministero Della Salute, Raccomandazioni per la Promozione della Salute Orale in Età Perinatale. Recommendations for the Promotion of Oral Health in Perinatal Age. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2317_allegato.pdf (accessed on 10 April 2021).
- Mylonas, I. Antibiotic chemotherapy during pregnancy and lactation period: Aspects for consideration. Arch. Gynecol. Obstet. 2011, 283, 7–18. [Google Scholar] [CrossRef]
- Strafford, K.E.; Shellhaas, C.; Hade, E. Provider and patient perceptions about dental care during pregnancy. J. Matern. Neonatal Med. 2008, 21, 63–71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year, Country of Origin | Title | Journal | Age | Gestation Week | Diagnosis | Risk of Bias * | |
|---|---|---|---|---|---|---|---|
| 1 | Fayek SS et al. [11] 1994, Saudi Arabia | Awake fibre optic intubation in a 38-week pregnant patient with submandibular abscess. | Int J. Obstet Anesth. | 32 | 38 weeks | submandibular abscess | G |
| 2 | Martin F. et al. [12] 2004, France | Do we have to monitor foetal heart rate during general anesthesia? | Ann Fr Anesth Rian | 29 | 36 weeks | submandibular abscess | F |
| 3 | Abramowicz et al. [13] 2006, USA | Severe life-threatening maxillofacial infection in pregnancy presented as Ludwig’s angina. | Infect Dis Obstet Gynecol. | 24 | 29 weeks | Ludwig’s angina | G |
| 4 | Niederhauser A. et al. [14] 2006, USA | Ludwig’s angina in pregnancy. | J. Matern Fetal Neonatal Med. | 24 | twin gestation at 22 weeks | bilateral Ludwig’s angina | G |
| 5 | Soltero R. et al. [15] 2009, Puerto Rico | Successful conservative management of Ludwig’s angina in advanced pregnancy. | Bol Asoc Med P R. | 20 | 32 weeks | Ludwig’s angina | F |
| 6 | Rana AS. et al. [16] 2009, India | A rare case of simultaneous surgery of an odontogenic space infection and delivery by caesarean section in a pregnant patient. | J. Maxillofac Oral Surg. | 34 | full term pregnant | DNI | G |
| 7 | Rajeev S. et al. [17] 2008, India | Anaesthetic management of Ludwig’s angina in pregnancy. | Int J. Obstet Anesth | 26 | 32 weeks | Ludwig’s angina | G |
| 8 | Moorhead K. et al. [18] 2010, USA | Pregnancy Complicated by Ludwig’s Angina Requiring Delivery. | Infect Dis Obstet Gynecol. | 24 | 33 weeks | Ludwig’s Angina + septis and ARDS | G |
| 9 | Hobson DT. et al. [19] 2011, USA | Pregnancy complicated by recurrent brain abscess after extraction of an infected tooth. | Obstet Gynecol. | 35 | 22 weeks | acute meningoencephalitis and left pterygoids muscles abscess and brain abscess | G |
| 10 | Çelebi N. et al. [20] 2013, Turkey | Acute fetal distress following tooth extraction and abscess drainage in a pregnant patient with maxillofacial infection. | Aust Dent J. | 28 | 36 weeks | submandibular abscess | G |
| 11 | Mukherjee S. et al. [21] 2013, India | Poor Dental Hygiene in Pregnancy Leading to Submandibular Cellulitis and Intrauterine Fetal Demise: Case Report and Literature Review. | Int J. Prev Med | 38 | 34 weeks | bilateral submandibular cellulitis and necrosis | F |
| 12 | Dalla Torre D. et al. [7] 2014, Austria | Odontogenic deep neck space infection as life-threatening condition in pregnancy. | Aust Dent J. | 25 | 28 weeks | DNI mediastinitis and sepsis | F |
| 13 | Kamath AT. et al. [22] 2015, India | Ludwig’s Angina in Pregnancy Necessitating Pre Mature Delivery. | J. Maxillofac Oral Surg. | 24 | 32 weeks | Ludwig’s angina DNI mediastinitis and sepsis | F |
| 14 | Tocaciu S. et al. [23] 2017, Australia | Severe odontogenic infection in pregnancy: a timely reminder. | Aust Dent J. | 29 | 17 weeks | odontogenic infection + DNI | F |
| 15 | Pereira RDS. et al. [24] 2017, Brazil | Dental Infection and Pregnancy: The Lack of Treatment by the Dental Professional Evolving to a Complex Maxillofacial Infection. | J. Craniofac Surg. | 30 | 32 weeks | odontogenic infection + DNI | G |
| 16 | Rahman T. et al. [25] 2019, India | Decompression of Ludwig’s angina in a pregnant patient under bilateral superficial cervical plexus block. | J. Perioper Pract | 25 | 28 weeks | Ludwing’s Angina | G |
| Author, Year, Country of Origin | Title | Journal | Patients Included | Age | Gestation Week | Diagnosis | Risk of Bias * | |
|---|---|---|---|---|---|---|---|---|
| 17 | Wong D et al. [2] 2012, Hong Kong | Management of severe odontogenic infections in pregnancy. | Aust Dent J. | 5 | 33; 32; 22; 26; 29 | 33; 35; 8; 10; 30 weeks | dental abscess | F |
| 18 | Doumbia-Singare K. et al. [8] 2014, Mali | Cervico-facial cellulitis during pregnancy: about a series of 10 cases in Mali. | Bull Soc Pathol Exot. | 10 | 23 (range 16–31) | 1 first trimester; 6 second and 3 third trimester | odontogenic infection + DNI | F |
| 19 | Osunde O et al. [9] 2014, Nigeria | Management of Ludwig’s Angina in Pregnancy: A Review of 10 Cases. | Ann Med Health Sci Res. | 10 | 29.5 years SD ± 5.3 | third trimester | Ludwing’s angina | G |
| 20 | Ali EAM. et al. [26] 2019, Sudan | Delay in the Referral of Pregnant Patients with Fascial Spaces Infection: A Cross-Sectional Observational Study from Khartoum Teaching Dental Hospital, Sudan. | J. Maxillofac. Oral Surg. | 10 | 26.5 years SD ± 6.3 | 6 third trimester; 4 second trimester | 7 submandibular abscess; 1 submental abscess; 2 Ludwig’s angina | F |
| 21 | Omeje KU. et al. [3] 2020, Nigeria | Severe Cervicofacial Cellulitis in Pregnancy—A Review of 18 Cases. | Iran J. Otorhinolaryngol. | 18 | 29 years SD ± 7.1 | 12 third trimester; 4 second; 2 in the first trimester | Cervicofacial cellulitis | F |
| Author, Year, Country of Origin | Odontogenic Cause | Intervention | Anaesthesia | Adverse Outcomes | |
|---|---|---|---|---|---|
| 1 | Fayek SS et al. [11] 1994, Saudi Arabia | right second molar tooth in the lower jaw | drainage + extraction | GA | fetal distress and C-section 38 weeks |
| 2 | Martin F. et al. [12] 2004, France | dental abscess NR | drainage | GA | foetal distress and C-section 36 weeks |
| 3 | Abramowicz et al. [13] 2006, USA | lower left third molar | awake tracheostomy + drainage + extraction | GA | maternal ICU post op (6 days) |
| 4 | Niederhauser A. et al. [14] 2006, USA | multiple periapical abscesses | bilateral drainage + multiple extractions | GA | maternal ICU post op (1 day) |
| 5 | Soltero R. et al. [15] 2009, Puerto Rico | recurrence of a periapical abscess | drainage + extraction | LA | no complications |
| 6 | Rana AS. et al. [16] 2009, India | lower right third molar | tracheostomy +drainage + delay extraction | GA | C-section 34 weeks simultaneously with the surgical procedure |
| 7 | Rajeev S. et al. [17] 2008, India | right second molar | drainage | GA | normal delivery 37 weeks of a 1700-g baby |
| 8 | Moorhead K. et al. [18] 2010, USA | tooth abscess NR | tracheotomy + drainage + extraction of five of teeth | GA | preterm C-section; infant weighing 2120 grams: mather and baby needed ICU |
| 9 | Hobson DT. et al. [19] 2011, USA | left maxillary third molar | drainage of left pterygoid abscess + multiple partial lobectomies | GA | C-section at 39 weeks; maternal neurologic deficits, which included Broca’s aphasia and apraxia with right hemiplegia |
| 10 | Çelebi N. et al. [20] 2013, Turkey | lower left third molar | drainage + extraction | LA | 8 h later foetal distress: C-section, baby needed ICU (12 days) |
| 11 | Mukherjee S. et al. [21] 2013, India | second or third mandibular molar | drainage | GA | fetal death normal delivery 34 weeks and maternal necrotizing fasciitis |
| 12 | Dalla Torre D. et al. [7] 2014, Austria | first and second lower left molars | drainage + extraction | GA | mathernal sepsis and ARDS, intrauterine death of the foetus and C-section at 28 weeks |
| 13 | Kamath AT. et al. [22] 2015, India | lower first molar and right upper second molar | bilateral drainage + dentals extraction and second neck and mediastinum drainage | GA | foetal distress C-section 32 weeks preterm delivery |
| 14 | Tocaciu S. et al. [23] 2017, Australia | lower left third molar | drainage + extraction | GA | maternal ICU post op (3 days) |
| 15 | Pereira RDS. et al. [24] 2017, Brazil | lower left third molar | drainage + delay extraction | LA | no complications |
| 16 | Rahman T. et al. [25] 2019, India | lower left second molar | drainage + extraction. | LA + superficial cervical plexus block | no complications |
| Author, Year, Country of Origin | Odontogenic Cause | Intervention | Anaesthesia | Adverse Outcomes | |
|---|---|---|---|---|---|
| 17 | Wong D et al. [2] 2012, Hong Kong | 5 dental abscess | 4 drainage + 2 contemporary extractions, 1 spontaneus drainage | 2 GA; 1 LA; LA+IV sedation | 2 patients required post op ICU, 1 C-section (patient has previous C-sections); 1 planned abortion. |
| 18 | Doumbia-Singare K. et al. [8] 2014, Mali | 5 third molar tooth; 5 premolar tooth | 8 drainage 2 medical treatment only | LA | 1 premature birth, 4 fetus deaths, 2 maternal deaths caused by sepsis |
| 19 | Osunde O et al. [9] 2014, Nigeria | 8 odontogenic infection; 2 unknown | drainage | LA | 3 fetal deaths, 2 maternal deaths, of which only one death occurred in hospital. |
| 20 | Ali EAM. et al. [26] 2019, Sudan | 5 lower third molar; 4 lower first molars; 1 lower canine | drainage and extractions | LA | 2 patients with necrotizing fasciitis |
| 21 | Omeje KU. et al. [3] 2020, Nigeria | odontogenic infection | drainage + 8 extractions, 10 delay extractions | LA | NR |
| Sample Characteristics | N. | |
|---|---|---|
| Age (Mean +/− SD) | 27.72 years +/− 5.3 | 69 |
| Gestational age | First trimester | 7.3% |
| Second trimester | 24.6% | |
| Third trimester | 68.1% | |
| Nationality | African countries (Nigeria, Sudan, Mali) | 69.5% |
| India | 7.2% | |
| Hong Kong | 7.2% | |
| USA | 5.7% | |
| Odontogenic cause | Third molar | 23% |
| First molar | 8.7% | |
| Second molars | 7.3% | |
| Premolars | 7.3% | |
| Surgical treatment | ||
| Extraoral surgical drainage with extraction | 63% | |
| Extraoral surgical drainage + delay extraction | 17% | |
| General anesthesia | 21.2% | |
| Local anesthesia | 78.8% | |
| Odontogenic complications | ||
| Cervicofacial cellulitis | 30% | |
| Ludwig’s angina | 27.5% | |
| Abscesses (submandibular and submental) | 23.2% | |
| Deep neck infection (DNI) | 21.7% | |
| Mediastinitis | 2.3% | |
| Adverse outcomes | ||
| Fetal deaths | 13% | |
| Fetal distress | 5.8% | |
| Baby needs of ICU | 2.9% | |
| Preterm birth | 4.3% | |
| Low birth weight | 2.9% | |
| Maternal deaths | 5.8% | |
| Mother need of ICU | 8.7% | |
| Infection-related C-section | 13% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pucci, R.; Cassoni, A.; Di Carlo, D.; Della Monaca, M.; Romeo, U.; Valentini, V. Severe Odontogenic Infections during Pregnancy and Related Adverse Outcomes. Case Report and Systematic Literature Review. Trop. Med. Infect. Dis. 2021, 6, 106. https://doi.org/10.3390/tropicalmed6020106
Pucci R, Cassoni A, Di Carlo D, Della Monaca M, Romeo U, Valentini V. Severe Odontogenic Infections during Pregnancy and Related Adverse Outcomes. Case Report and Systematic Literature Review. Tropical Medicine and Infectious Disease. 2021; 6(2):106. https://doi.org/10.3390/tropicalmed6020106
Chicago/Turabian StylePucci, Resi, Andrea Cassoni, Daniele Di Carlo, Marco Della Monaca, Umberto Romeo, and Valentino Valentini. 2021. "Severe Odontogenic Infections during Pregnancy and Related Adverse Outcomes. Case Report and Systematic Literature Review" Tropical Medicine and Infectious Disease 6, no. 2: 106. https://doi.org/10.3390/tropicalmed6020106
APA StylePucci, R., Cassoni, A., Di Carlo, D., Della Monaca, M., Romeo, U., & Valentini, V. (2021). Severe Odontogenic Infections during Pregnancy and Related Adverse Outcomes. Case Report and Systematic Literature Review. Tropical Medicine and Infectious Disease, 6(2), 106. https://doi.org/10.3390/tropicalmed6020106