
Diagnostic Value of Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio, and Platelet-to-Lymphocyte Ratio in the Diagnosis of Erythema Nodosum Leprosum: A Retrospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global leprosy (Hansen disease) update, 2019: Time to step-up prevention initiatives. Wkly. Epidermiol. Rec. 2020, 95, 417–440. [Google Scholar]
- World Health Organization. Towards Zero Leprosy. Global Leprosy (Hansen’s Disease) Strategy 2021–2030; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2021.
- Bakker, M.I.; Hatta, M.; Kwenang, A.; Van Mosseveld, P.; Faber, W.R.; Klatser, P.R.; Oskam, L. Risk factors for developing leprosy—A population-based cohort study in Indonesia. Lepr. Rev. 2006, 77, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Nazario, A.P.; Ferreira, J.; Schuler-Faccini, L.; Fiegenbaum, M.; Artigalás, O.; Vianna, F.S.L. Leprosy in Southern Brazil: A twenty-year epidemiological profile. Rev. Soc. Bras. Med. Trop. 2017, 50, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, V.; Tavares, I.F.; Pignataro, P.; Machado, A.D.M.; Pacheco, F.D.S.; Dos Santos, J.B.; Da Silva, C.O.; Sarno, E.N. Neutrophils in Leprosy. Front. Immunol. 2019, 10, 495. [Google Scholar] [CrossRef] [PubMed]
- Tavares, I.F.; dos Santos, J.B.; Pacheco, F.D.S.; Gandini, M.; Mariante, R.M.; Rodrigues, T.F.; Sales, A.M.; Moraes, M.O.; Sarno, E.N.; Schmitz, V. Mycobacterium leprae induces neutrophilic degranulation and low-density neutrophil generation during erythema nodosum leprosum. Front. Med. 2021, 8, 711623. [Google Scholar] [CrossRef] [PubMed]
- Yap, F.B.; Kiung, S.T.; Yap, J.B. Quality of life in patients with erythema nodosum leprosum in Kuala Lumpur, Malaysia. Indian Dermatol. Online J. 2016, 7, 255–258. [Google Scholar] [CrossRef]
- Parker, H.A.; Forrester, L.; Kaldor, C.D.; Dickerhof, N.; Hampton, M.B. Antimicrobial activity of neutrophils against mycobacteria. Front. Immunol. 2021, 12, 782495. Available online: https://www.frontiersin.org/article/10.3389/fimmu.2021.782495 (accessed on 3 February 2022). [CrossRef]
- Kar, H.; Chauhan, A. Leprosy reactions: Pathogenesis and clinical features. In IAL Textbook of Leprosy, 2nd ed.; Kumar, B., Kar, H.K., Eds.; Jaypee Brothers Medical Publishers: New Delhi, India, 2017; p. 416. [Google Scholar]
- Gomes, L.T.; Morato-Conceição, Y.T.; Gambati, A.V.M.; Maciel-Pereira, C.M.; Fontes, C.J.F. Diagnostic value of neutrophil-to-lymphocyte ratio in patients with leprosy reactions. Heliyon 2020, 6, e03369. [Google Scholar] [CrossRef] [PubMed]
- Voorend, C.; Post, E.B. A systematic review on the epidemiological data of erythema nodosum leprosum, a type 2 leprosy reaction. PLoS Negl. Trop. Dis. 2013, 7, e2440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polycarpou, A.; Walker, S.L.; Lockwood, D.N.J. A Systematic review of immunological studies of erythema nodosum leprosum. Front. Immunol. 2017, 8, 233. [Google Scholar] [CrossRef] [Green Version]
- Fransisca, C.; Zulkarnain, I.; Ervianti, E.; Damayanti, D.; Sari, M.; Budiono, B.; Prakoeswa, C.R.S.; Alinda, M.D.; Kusumaputra, B.H.; Listiawan, M.Y. A Retrospective study: Epidemiology, onset, and duration of erythema nodosum leprosum in Surabaya, Indonesia. Berk. Ilmu Kesehat. Kulit Kelamin 2021, 33, 8–12. [Google Scholar] [CrossRef]
- Naafs, B.; Noto, S.; Schreuder, P. Mortality and morbidity in leprosy. In IAL Textbook of Leprosy, 2nd ed.; Kumar, B., Kar, H.K., Eds.; Jaypee Brothers Medical Publishers: New Delhi, India, 2017; pp. 583–586. [Google Scholar]
- Lazo-Porras, M.; Prutsky, G.J.; Barrionuevo, P.; Tapia, J.C.; Ugarte-Gil, C.; Ponce, O.J.; Acuña-Villaorduña, A.; Domecq, J.P.; De La Cruz-Luque, C.; Prokop, L.J.; et al. World health organization (WHO) antibiotic regimen against other regimens for the treatment of leprosy: A systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 62. [Google Scholar] [CrossRef]
- Sahu, S.; Sharma, K.; Sharma, M.; Narang, T.; Dogra, S.; Minz, R.W.; Chhabra, S. Neutrophil NETworking in ENL: Potential as a putative biomarker: Future insights. Front. Med. 2021, 8, 697804. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, E.P.; Oliveira, R.B.; Warwick-Davies, J.; Neto, R.B.F.; Griffln, G.E.; Shattock, R.J. T cell–monocyte contact enhances tumor necrosis factor–α production in response to Mycobacterium leprae. J. Infect. Dis. 2000, 182, 1463–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibuya, M.; Bergheme, G.; Passos, S.; Queiroz, I.; Rêgo, J.; Carvalho, L.P.; Machado, P.R. Evaluation of monocyte subsets and markers of activation in leprosy reactions. Microbes Infect. 2018, 21, 94–98. [Google Scholar] [CrossRef]
- Da Silva, D.S.; Teixeira, L.A.C.; Beghini, D.G.; Ferreira, A.T.D.S.; Pinho, M.D.B.M.; Rosa, P.S.; Ribeiro, M.R.; Freire, M.D.C.; Hacker, M.A.; Nery, J.A.D.C.; et al. Blood coagulation abnormalities in multibacillary leprosy patients. PLoS Negl. Trop. Dis. 2018, 12, e0006214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rea, T.H. Elevated platelet counts and thromboccytosis in erythema nodosum leprosum. Int. J. Lepr. Other Mycobact. Dis. 2002, 70, 167–173. [Google Scholar]
- Vilani-Moreno, F.R.; Brito-De-Souza, V.N.; Silva, S.M.U.R.; Barbosa, A.S.A.A.; Sartori, B.G.C.; Campanelli, A.P.; Barreto, J.A.; Virmond, M.D.C.L. Increased serum levels of interleukin-6 in erythema nodosum leprosum suggest its use as a biomarker. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Kalemaki, D.; Tzagkarakis, E.; Lydakis, C. Pitfalls in studies of eosinopenia and neutrophil-to-lymphocyte count ratio. Infect. Dis. 2018, 50, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic, D.; Rondovic, G.; Surbatovic, M.; Stanojevic, I.; Udovicic, I.; Andjelic, T.; Zeba, S.; Milosavljevic, S.; Stankovic, N.; Abazovic, D.; et al. Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and mean platelet volume-to-platelet count ratio as biomarkers in critically Ill and injured patients: Which ratio to choose to predict outcome and nature of bacteremia? Mediat. Inflamm. 2018, 2018, 3758068. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Kim, N.Y.; Na, S.H.; Youn, Y.H.; Shin, C.S. Reference values of neutrophil-lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio, and mean platelet volume in healthy adults in South Korea. Medicine 2018, 97, e11138. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | ENL | ||||
|---|---|---|---|---|---|
| n (%) | Absent | Present | p-Value | ||
| Gender | Males | 131 (71.97) | 115 (71.87) | 16 (72.72) | 0.986 a |
| Females | 51 (28.02) | 45 (28.12) | 6 (27.27) | ||
| Age | 18–40 | 104 (57.14) | 89 (55.62) | 15 (68.18) | 0.245 b |
| 41–59 | 63 (34.61) | 56 (35) | 7 (31.81) | ||
| ≥60 | 15 (8.24) | 15 (9.375) | 0 (0) | ||
| Treatment | New | 146 (80.21) | 136 (85) | 10 (45.45) | 0.001 b,c |
| Onset | On MDT | 5 (2.74) | 3 (1.87) | 2 (9.09) | |
| RFT/RFC | 9 (4.94) | 2 (1.25) | 7 (31.81) | ||
| Dropout | 22 (12.08) | 19 (11.87) | 3 (13.63) | ||
| Disability | 0 | 125 (68.68) | 112 (70) | 13 (59.09) | 0.236 b |
| 1 | 37 (20.32) | 30 (18.75) | 7 (31.81) | ||
| 2 | 20 (10.98) | 18 (11.25) | 2 (9.09) | ||
| Nutritional | Underweight | 32 (17.58) | 28 (17.5) | 4 (18.18) | 0.545 b |
| Status | Normal | 89 (48.90) | 76 (47.5) | 13 (59.09) | |
| Overweight | 49 (26.92) | 44 (27.5) | 5 (22.72) | ||
| Obese | 12 (6.59) | 12 (7.5) | 0 (0) | ||
| Bacterial | <3 | 146 (80.21) | 129 (80.62) | 17 (77.27) | 0.083 a |
| Index | ≥3 | 36 (19.78) | 31 (19.37) | 5 (22.72) | |
| Morphological | <5 | 160 (87.91) | 140 (87.5) | 20 (90.90) | 0.919 a |
| Index | ≥5 | 22 (12.08) | 20 (12.5) | 2 (9.09) | |
| Blood Count | ENL | Correlation | p-Value | ||
|---|---|---|---|---|---|
| Present | Absent | Coefficient | |||
| WBC a | 7,720 (4,160–30,330) | 14,820 (4,160–30,330) | 7,405 (4,380–21,980) | 0.438 c | 0.001 |
| Neutrophil a | 5,110 (2,010–26,840) | 12,355 (3,520–26,840) | 4,840 (2,010–19,540) | 0.461 c | 0.001 |
| Lymphocyte b | 1,711.97 (±629.04) | 1,526.82 (±655.57) | 1,737.43 (±623.13) | −0.105 d | 0.159 |
| Monocyte a | 590 (200–1,910) | 775 (210–1,910) | 570 (200–1,450) | 0.145 c | 0.051 |
| Thrombocyte a | 308,000 (116,000–909,000) | 375,000 (229,000–909,000) | 302,000 (116,000–721,000) | 0.263 c | 0.001 |
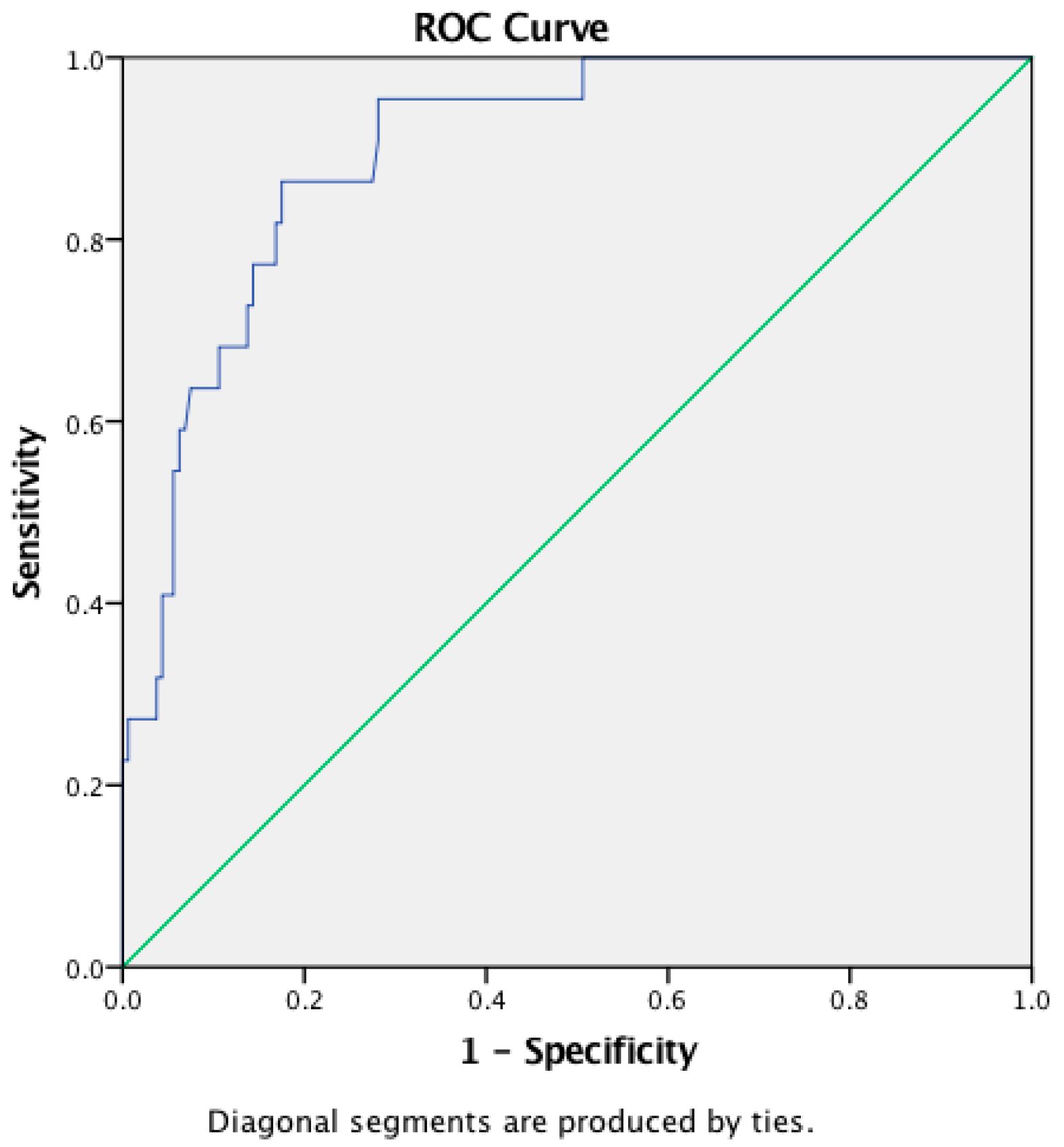
| NLR a | 3.19 (0.86–21.46) | 8.19 (2.9–21.46) | 2.93 (0.86–12.85) | 0.450 c | 0.001 |
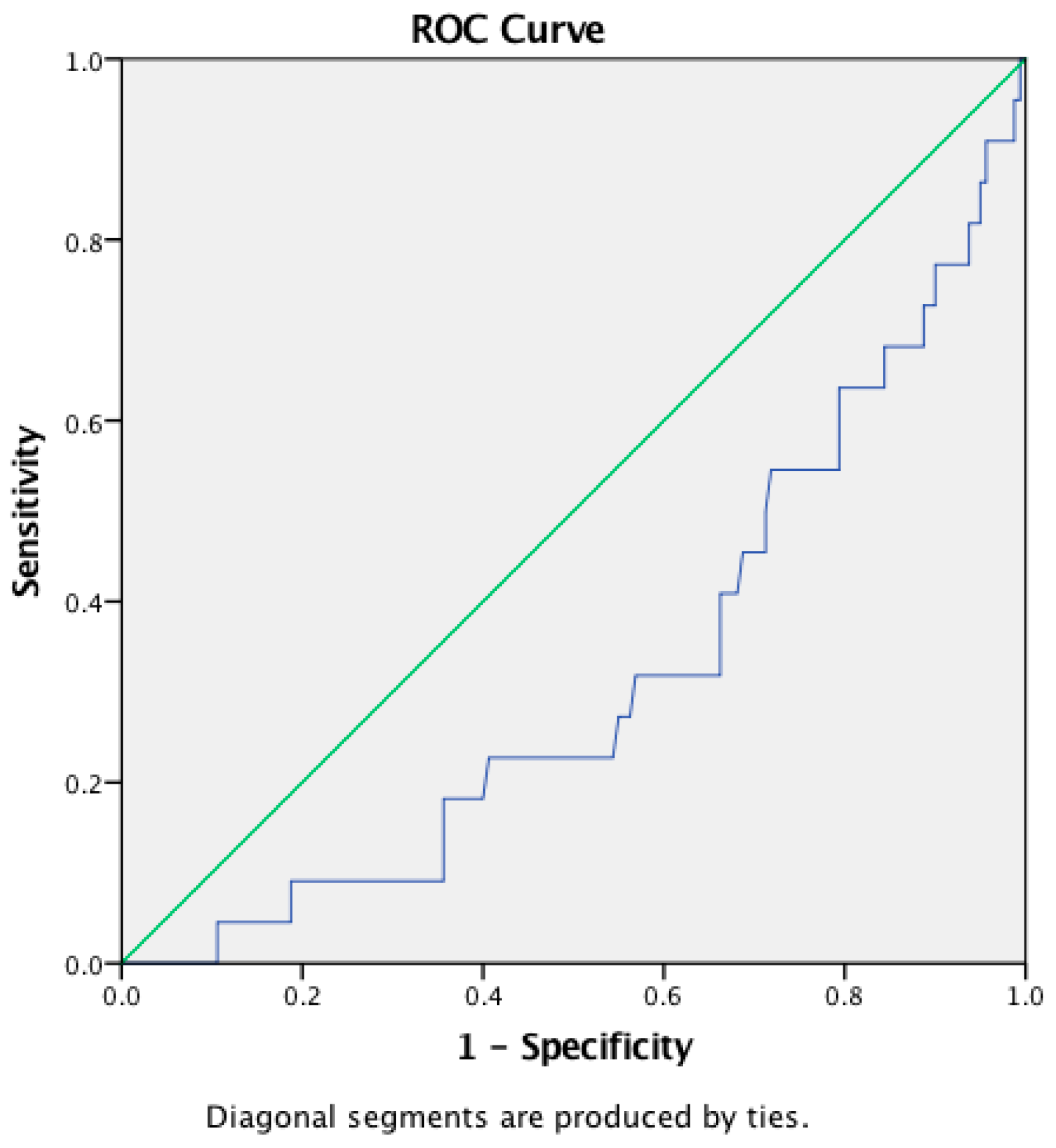
| LMR a | 3 (0.69–8.67) | 2.28 (0.75–4.94) | 3.13 (0.69–8.67) | −0.205 c | 0.005 |
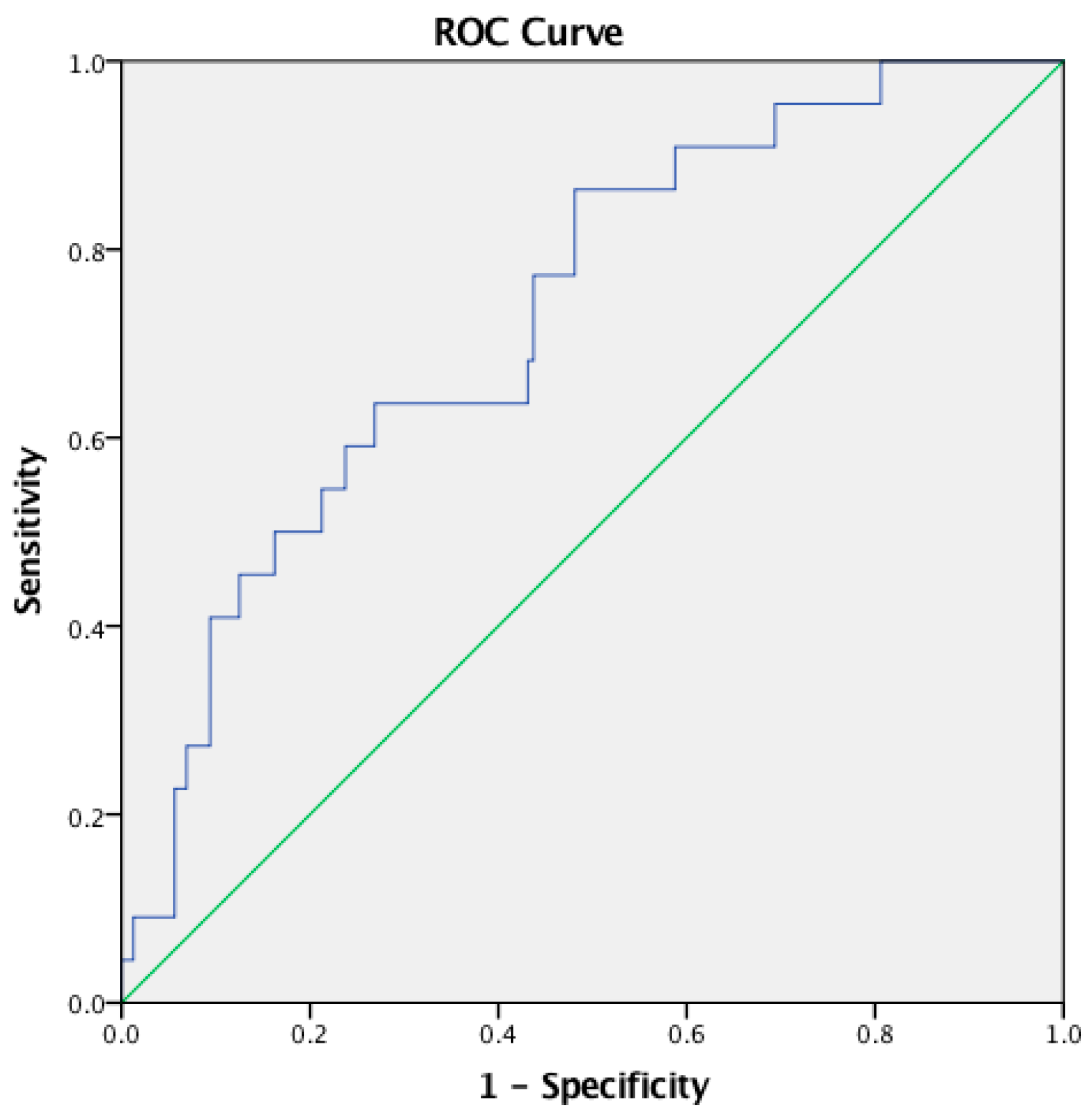
| PLR a | 186.59 (72.96–1,267.65) | 283.97 (126.48–1,267.65) | 173.41 (72.96–893.33) | 0.262 c | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanojo, N.; Damayanti; Utomo, B.; Ervianti, E.; Murtiastutik, D.; Prakoeswa, C.R.S.; Listiawan, M.Y. Diagnostic Value of Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio, and Platelet-to-Lymphocyte Ratio in the Diagnosis of Erythema Nodosum Leprosum: A Retrospective Study. Trop. Med. Infect. Dis. 2022, 7, 39. https://doi.org/10.3390/tropicalmed7030039
Tanojo N, Damayanti, Utomo B, Ervianti E, Murtiastutik D, Prakoeswa CRS, Listiawan MY. Diagnostic Value of Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio, and Platelet-to-Lymphocyte Ratio in the Diagnosis of Erythema Nodosum Leprosum: A Retrospective Study. Tropical Medicine and Infectious Disease. 2022; 7(3):39. https://doi.org/10.3390/tropicalmed7030039
Chicago/Turabian StyleTanojo, Natalia, Damayanti, Budi Utomo, Evy Ervianti, Dwi Murtiastutik, Cita Rosita Sigit Prakoeswa, and Muhammad Yulianto Listiawan. 2022. "Diagnostic Value of Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio, and Platelet-to-Lymphocyte Ratio in the Diagnosis of Erythema Nodosum Leprosum: A Retrospective Study" Tropical Medicine and Infectious Disease 7, no. 3: 39. https://doi.org/10.3390/tropicalmed7030039
APA StyleTanojo, N., Damayanti, Utomo, B., Ervianti, E., Murtiastutik, D., Prakoeswa, C. R. S., & Listiawan, M. Y. (2022). Diagnostic Value of Neutrophil-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio, and Platelet-to-Lymphocyte Ratio in the Diagnosis of Erythema Nodosum Leprosum: A Retrospective Study. Tropical Medicine and Infectious Disease, 7(3), 39. https://doi.org/10.3390/tropicalmed7030039