
Adaptation of the Aphasia Impact Questionnaire-21 into Greek: A Reliability and Validity Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
1.1. Aphasia and QoL
1.2. Aphasia Assessments and the ICF [17]
1.3. Patient and Public Involvement and the Development of QoL Self-Rating Tools
1.4. Aphasia Impact Questionnaire-21 (AIQ-21)
2. Materials and Methods
2.1. Participation Criteria
2.2. Recruitment
2.3. Sample Size
2.4. Participants
2.5. Data Collection
2.6. Measures
2.7. The Adaptation Processes
2.8. Linguistic Adaptation
2.9. Pilot Study for Group Discrimination
2.10. Data Analysis
2.11. Reliability Analyses
2.12. Translation Reliability
2.13. Internal Consistency
2.14. Validity Analyses
2.15. Criterion Validity
2.16. Construct Validity
2.17. Factor Analysis
2.18. Content Validity
2.19. Known-Groups Validity
3. Results
3.1. Measure Scores
3.2. Results Regarding the Reliability of the AIQ-21-GR
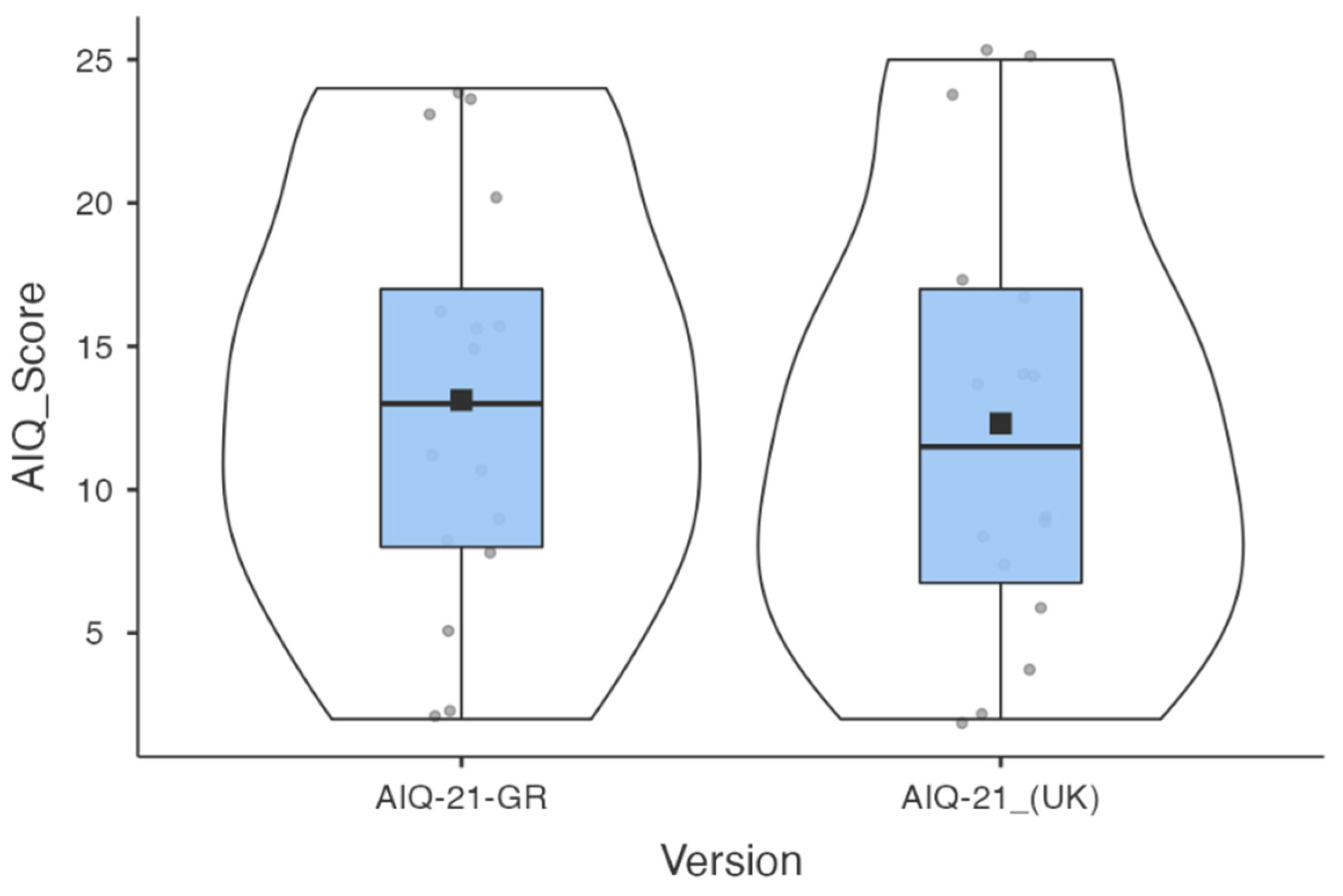
3.2.1. Translation Reliability
- (a)
- Pilot testing for language clarity between Greek and the original English version
- (b)
- Pilot testing of the final GR version for group discrimination
3.2.2. Internal Consistency
3.3. Results Regarding the Validity of the AIQ-21-GR
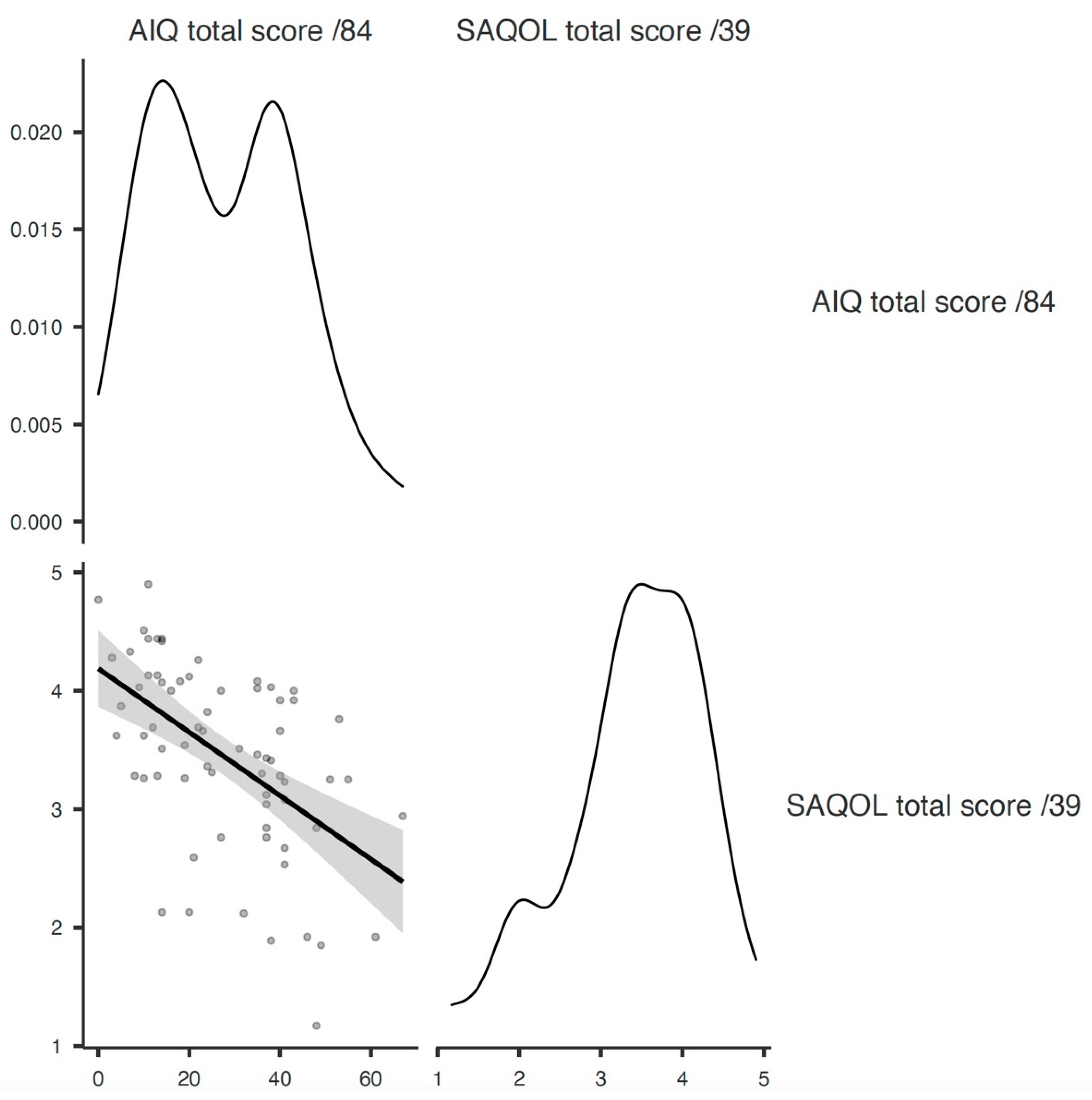
3.3.1. Criterion Validity
3.3.2. Construct Validity
3.3.3. Factor Analysis
3.3.4. Content Validity
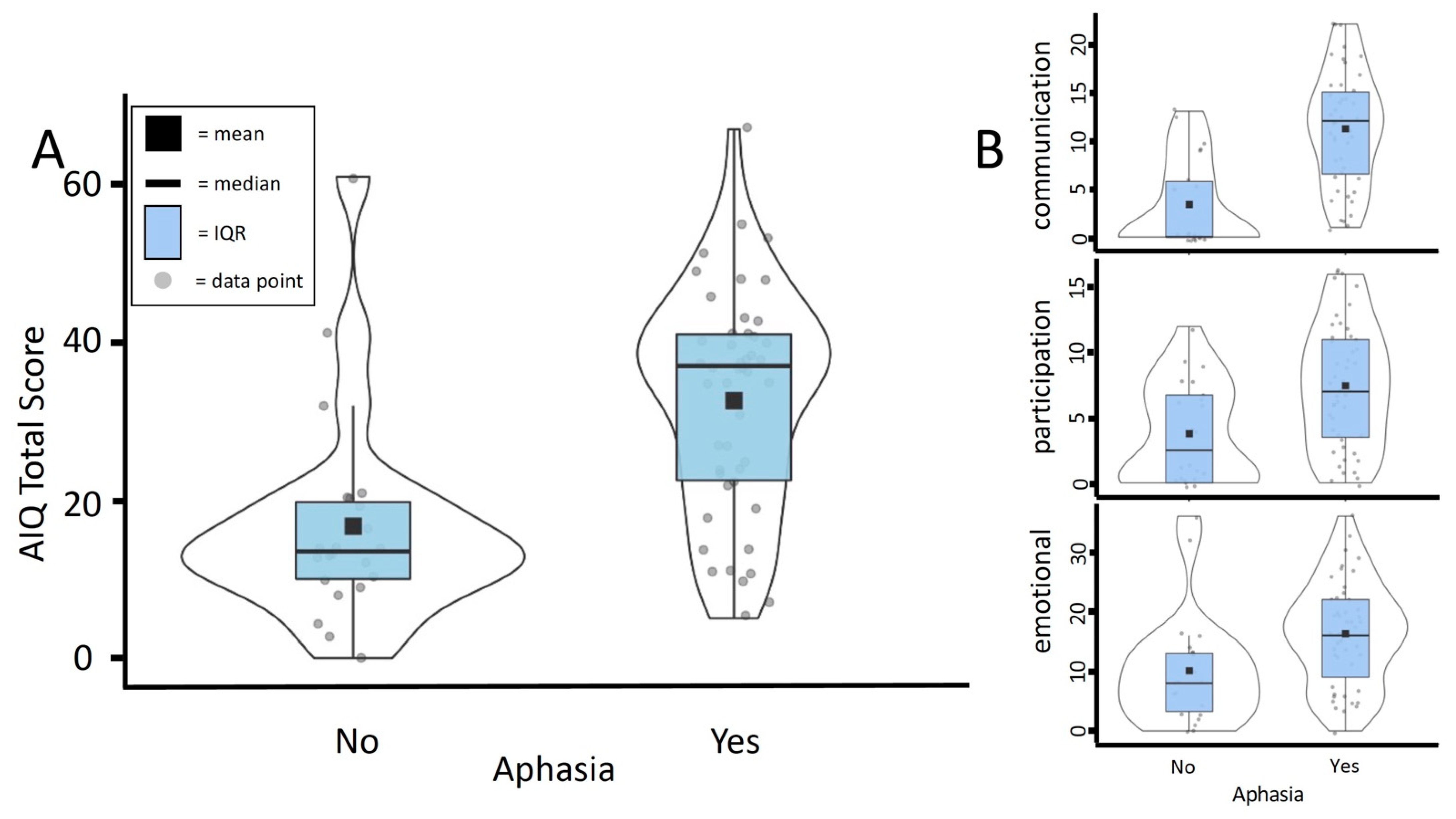
3.3.5. Known-Groups Validity
4. Discussion
4.1. Regarding the Reliability of the AIQ-21-GR
4.2. Regarding the Validity of the AIQ-21-GR
4.3. Patient and Public Involvement
4.4. Clinical Implication
4.5. Limitations of the Study
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdul Aziz, A.F.; Mohd Nordin, N.A.; Ali, M.F.; Abd Aziz, N.A.; Sulong, S.; Aljunid, S.M. The integrated care pathway for post stroke patients (iCaPPS): A shared care approach between stakeholders in areas with limited access to specialist stroke care services. BMC Health Serv. Res. 2017, 17, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul Aziz, A.F.; Mohd Nordin, N.A.; Muhd Nur, A.; Sulong, S.; Aljunid, S.M. The integrated care pathway for managing post stroke patients (iCaPPS©) in public primary care Healthcentres in Malaysia: Impact on quality adjusted life years (QALYs) and cost effectiveness analysis. BMC Geriatr. 2020, 20, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charalambous, M.; Kambanaros, M.; Annoni, J.M. Are People with Aphasia (PWA) Involved in the Creation of Quality of Life and Aphasia Impact-Related Questionnaires? A Scoping Review. Brain Sci. 2020, 10, 688. [Google Scholar] [CrossRef] [PubMed]
- Walters, R.; Collier, J.M.; Carvalho, L.B.; Langhorne, P.; Katijjahbe, A.; Tan, D.; Moodie, M.; Bernhardt, J. Exploring post acute rehabilitation service use and outcomes for working age stroke survivors (≤65 years) in Australia, UK and South East Asia: Data from the international AVERT trial. BMJ Open 2020, 10, e035850. [Google Scholar] [CrossRef]
- Abrahamson, V.; Wilson, P.M. How unmet are unmet needs post-stroke? A policy analysis of the six-month review. BMC Health Serv. Res. 2019, 19, 480. [Google Scholar] [CrossRef] [Green Version]
- Bullier, B.; Cassoudesalle, H.; Villain, M.; Cogne, M.; Mollo, C.; Gabory, I.D.; Glize, B. New factors that affect quality of life in patients with aphasia. Ann. Phys. Rehabil. Med. 2020, 63, 33–37. [Google Scholar] [CrossRef]
- Charalambous, M.; Phylactou, P.; Elriz, T.; Psychogios, L.; Annoni, J.M.; Kambanaros, M. Adaptation of the Scenario Test for Greek-speaking people with aphasia: A reliability and validity study. Int. J. Lang. Commun. Disord. 2022, 57, 865–880. [Google Scholar] [CrossRef]
- Flowers, H.L.; Skoretz, S.A.; Silver, F.L.; Rochon, E.; Fang, J.; Flamand-Roze, C.; Martino, R. Poststroke aphasia frequency, recovery, and outcomes: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2016, 97, 2188–2201.e8. [Google Scholar] [CrossRef]
- Kristinsson, S.; den Ouden, D.B.; Rorden, C.; Newman-Norlund, R.; Neils-Strunjas, J.; Fridriksson, J. Predictors of Therapy Response in Chronic Aphasia: Building a Foundation for Personalized Aphasia Therapy. J. Stroke 2022, 24, 189–206. [Google Scholar] [CrossRef]
- Doedens, W.J.; Meteyard, L. What is Functional Communication? A Theoretical Framework for Real-World Communication Applied to Aphasia Rehabilitation. Neuropsychol. Rev. 2022. [Google Scholar] [CrossRef]
- Annoni, J.M.; Colombo, F. Troubles cognitifs et comporte mentaux après lésion cérébrale: Impact sur la reprise professionnelle [Return to work after brain lesions: Cognitive and behavioral factors]. Rev. Med. Suisse 2011, 7, 944–947. (In French). PMID: 21634144. [Google Scholar] [PubMed]
- Wicht, C.A.; Chavan, C.F.; Annoni, J.-M.; Balmer, P.; Aellen, J.; Humm, A.M.; von Roten, F.C.; Spierer, L.; Medlin, F. Predictors for Returning to Paid Work after Transient Ischemic Attack and Minor Ischemic Stroke. J. Pers. Med. 2022, 12, 1109. [Google Scholar] [CrossRef] [PubMed]
- Manning, M.; MacFarlane, A.; Hickey, A.; Franklin, S. Perspectives of people with aphasia post-stroke towards personal recovery and living successfully: A systematic review and thematic synthesis. PLoS ONE 2019, 14, e0214200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melesse, D.Y.; Mutua, M.K.; Choudhury, A.; Wado, Y.D.; Faye, C.M.; Neal, S.; Boerma, T. Fidelity protocol for the Action Success Knowledge (ASK) trial: A psychosocial intervention administered by speech and language therapists to prevent depression in people with post-stroke aphasia. BMJ Open 2019, 9, e023560. [Google Scholar] [CrossRef] [Green Version]
- Melesse, D.Y.; Mutua, M.K.; Choudhury, A.; Wado, Y.D.; Faye, C.M.; Neal, S.; Boerma, T. Supporting wellbeing through PEeR-Befriending (SUPERB) feasibility trial: Fidelity of peer-befriending for people with aphasia. BMJ Open 2021, 11, e047994. [Google Scholar] [CrossRef]
- Azios, J.H.; Strong, K.A.; Archer, B.; Douglas, N.F.; Simmons-Mackie, N.; Worrall, L. Friendship matters: A research agenda for aphasia. Aphasiology 2021, 36, 317–336. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Classification of Functioning, Disability, and Health: ICF; World Health Organization: Geneva, Switzerland, 2001.
- Charalambous, M.; Kountouris, A.; Phylactou, P.; Triantafyllidou, I.; Annoni, J.-M.; Kambanaros, M. The Views of People Living with Chronic Stroke and Aphasia on Their Potential Involvement as Research Partners: A Thematic Analysis. Res. Involv. Engagem. 2022, 8, 48. [Google Scholar] [CrossRef]
- Hersh, D.; Israel, M.; Shiggins, C. The ethics of patient and public involvement across the research process: Towards partnership with people with aphasia. Aphasiology 2021. [Google Scholar] [CrossRef]
- Simmons-Mackie, N.; Kagan, A.; Victor, J.C.; Carling-Rowland, A.; Mok, A.; Hoch, J.S.; Huijbregts, M.P.; Streiner, D.L. The assessment for living with aphasia: Reliability and construct validity. Int. J. Speech-Lang. Pathol. 2014, 16, 82–94. [Google Scholar] [CrossRef]
- Hula, W.D.; Doyle, P.J.; Stone, C.A.; Hula, S.N.A.; Kellough, S.; Wambaugh, J.L.; Ross, K.B.; Schumacher, J.G.; Jacque, A.S. The Aphasia Communication Outcome Measure (ACOM): Dimensionality, Item Bank Calibration and Initial Validation. J. Speechlang. Hear. Res. 2015, 58, 906–919. [Google Scholar] [CrossRef]
- Babulal, G.M.; Connor, L.T. The measure of stroke environment (MOSE): Development and validation of the MOSE in post-stroke populations with and without aphasia. Top. Stroke Rehabil. 2016, 23, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, K.; Best, W.; Beeke, S.; Cruice, M.; Smith, L.; Willis, E.P.; Ledingham, K.; Sweeney, J.; McVicker, S.J. A concise patient reported outcome measure for people with aphasia: The aphasia impact questionnaire 21. Aphasiology 2018, 33, 1035–1060. [Google Scholar] [CrossRef]
- Byng, S.; Duchan, J.F. Social model philosophies and principles: Their applications to therapies for aphasia. Aphasiology 2005, 19, 906–922. [Google Scholar] [CrossRef]
- Swinburn, K.; Byng, S. The Communication Disability Profile; Connect Press: London, UK, 2006. [Google Scholar]
- Swinburn, K.; Porter, G.; Howard, D. The Comprehensive Aphasia Test; Whurr: London, UK, 2004. [Google Scholar]
- Yaşar, Ε.; Şenol, N.E.G.; Zararsız, E.G.; Birol, N.Y. Adaptation of the Aphasia Impact Questionnaire-21 into Turkish: Reliability and validity study. Neuropsychol. Rehabil. 2021, 32, 1550–1575. [Google Scholar] [CrossRef] [PubMed]
- Hilari, K.; Byng, S.; Lamping, D.L.; Smith, S.C. Stroke and Aphasia Quality of Life Scale-39 (SAQOL-39): Evaluation of acceptability, reliability, and validity. Stroke 2003, 34, 1944–1950. [Google Scholar] [CrossRef] [PubMed]
- Efstratiadou, E.A.; Chelas, E.N.; Ignatiou, M.; Christaki, V.; Papathanasiou, I.; Hilari, K. Quality of life after stroke: Evaluation of the Greek SAQOL-39g. Folia Phoniatr. Logop. 2012, 64, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Kartsona, A.; Hilari, K. Quality of life in aphasia: Greek adaptation of the stroke and aphasia quality of life scale—39 item (SAQOL-39). Eura Med. 2007, 43, 27–35. [Google Scholar]
- Noyan-Erbaş, A.; Toğram, B. Stroke and aphasia quality-of-life scale-39: Reliability and validity of the Turkish version. Int. J. Speech-Lang. Pathol. 2016, 18, 432–438. [Google Scholar] [CrossRef]
- Abma, T.A.; Pittens, C.A.; Visse, M.; Elberse, J.E.; Broerse, J.E. Patient involvement in research programming and implementation. Health Expect 2015, 18, 2449–2464. [Google Scholar] [CrossRef]
- Fullerton, K.J.; McSherry, D.; Stout, R.W. Albert’s test: A neglected test of perceptual neglect. Lancet 1986, 1, 430–432. [Google Scholar] [CrossRef]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, Y.; Demir, C.; Gursoy, K.; Koselerli, R. Analysis of Stroke Statistics in Turkey. Value Health 2015, 18, A402. [Google Scholar] [CrossRef] [Green Version]
- Köseoğlu, T.C.; Bölük, C.; Börü, Ü.; Akin, S.; Yılmaz, A.; Duman, S.; Taşdemir, M. Stroke Prevalence in a Coastal Town on the Black Sea Coast in Turkey: Community Based Study. Neurol. Res. Int. 2018, 2018, 8246123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messinis, L.; Panagea, E.; Papathasopoulos, P.; Kastellakis, A. Boston Diagnostic Aphasia Examination-Short Form in Greek Language; Gotsis: Patras, Greece, 2013. [Google Scholar]
- El Hachioui, H.; Lingsma, H.F.; Van de Sandt-Koenderman, M.W.; Dippel, D.W.; Koudstaal, P.J.; Visch-Brink, E.G. Long-term prognosis of aphasia after stroke. J. Neurol. Neurosurg. Psychiatry 2013, 84, 310–315. [Google Scholar] [CrossRef]
- Fotiou, C.; Grohmann, K.K. A Small Island with Big Differences? Folk Perceptions in the Context of Dialect Levelling and Koineization. Front. Commun. 2022, 6, 770088. [Google Scholar] [CrossRef]
- Schmidt, S.; Bullinger, M. Current issues in cross-cultural quality of life instrument development. Arch. Phys. Med. Rehabil. 2003, 84, S29–S34. [Google Scholar] [CrossRef]
- Terwee, C.B.; Prinsen, C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. 2018, 27, 1159–1170. [Google Scholar] [CrossRef] [Green Version]
- Bonner, N.; Abetz-Webb, L.; Renault, L.; Caballero, T.; Longhurst, H.; Maurer, M.; Christiansen, S.; Zuraw, B. Development and content validity testing of a patient-reported outcomes questionnaire for the assessment of hereditary angioedema in observational studies. Health Qual. Life Outcomes 2015, 13, 92. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- The jamovi project (Version 1.6) [Computer Software]. Available online: https://www.jamovi.org. (accessed on 10 June 2022).
- R Core Team (2020). R: A Language and environment for statistical computing. (Version 4.0) [Computer software]. (R packages retrieved from MRAN snapshot 2020-08-24). Available online: https://cran.r-project.org. (accessed on 1 September 2022).
- Nunnally, J.; Bernstein, I. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Taherdoost, H. Validity and Reliability of the Research Instrument; How to Test the Validation of a Questionnaire/Survey in a Research. Int. J. Acad. Res. Manag. 2016, 5, 28–36. [Google Scholar] [CrossRef]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Hilari, K.; Galante, L.; Huck, A.; Pritchard, M.; Allen, L.; Dipper, L. Cultural adaptation and psychometric testing of The Scenario Test UK for people with aphasia. Int. J. Lang. Commun. Disord. 2018, 53, 748–760. [Google Scholar] [CrossRef] [PubMed]
- Zijlmans, E.; Tijmstra, J.; van der Ark, L.A.; Sijtsma, K. Item-Score Reliability in Empirical-Data Sets and Its Relationship with Other Item Indices. Educ. Psychol. Meas. 2018, 78, 998–1020. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, M.; Wetzel, A. Factor Analysis: A means for theory and instrument development in support of construct validity. Int. J. Med. Educ. 2020, 11, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Kiran, S.; Sandberg, C.; Abbott, K. Treatment for lexical retrieval using abstract and concrete words in persons with aphasia: Effect of complexity. Aphasiology 2009, 23, 835–853. [Google Scholar] [CrossRef] [Green Version]
- Borghi, A.M. A future of Words: Language and Challenge of Abstract concepts. J. Cogn. 2020, 3, 42. [Google Scholar] [CrossRef]
- Binney, R.J.; Zuckerman, B.; Reilly, J. A Neuropsychological Perspective on Abstract Word Representation: From Theory to Treatment of Acquired Language Disorders. Curr. Neurol. Neurosci. Rep. 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilari, K. The impact of stroke: Are people with aphasia different to those without? Disabil. Rehabil. 2011, 33, 211–218. [Google Scholar] [CrossRef]
- Cruice, M.; Aujla, S.; Bannister, J.; Botting, N.; Boyle, M.; Charles, N.; Dhaliwal, V.; Grobler, S.; Hersh, D.; Marshall, J.; et al. Creating a novel approach to discourse treatment through coproduction with people with aphasia and speech and language therapists. Aphasiology 2021, 36, 1159–1181. [Google Scholar] [CrossRef]
- Nichol, L.; Hill, A.J.; Wallace, S.J.; Pitt, R.; Baker, C.; Rodriguez, A.D. Self-management of aphasia: A scoping review. Aphasiology 2019, 33, 903–942. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Population | Incidence Estimate | AIQ-21 Sample Size (n) |
|---|---|---|---|
| United Kingdom | 65,542,579 | 106,000 strokes/year | n = 90 PWA |
| Turkey | 85,561,976 | 400,000 strokes/year | n = 104 (43 PWA + 61 healthy) |
| Greece & Cyprus | 11,606,813 803,147 | 28,000 strokes/year 1000 strokes/year | n = 69 (47 PWA + 22 stroke no aphasia) |
| Characteristics | People with Aphasia (n = 47) | Stroke Survivors without Aphasia (n = 22) |
|---|---|---|
| Gender | ||
| Male | 19 (40%) | 11 (50%) |
| Female | 28 (60%) | 11 (50%) |
| Age | ||
| Mean (sd) | 58.3 (17.5) | 55.7 (18.7) |
| Minimum–Maximum | 22–85 | 20–73 |
| Stroke Type | ||
| Ischemic | 33 (70%) | 11 (50%) |
| Hemorrhagic | 14 (30%) | 11 (50%) |
| Lesion Location | ||
| Left | 40 (85%) | 5 (23%) |
| Right | 7 (15%) | 17 (77%) |
| Hemiplegia | ||
| Left | 5 (10%) | 16 (70%) |
| Right | 37 (80%) | 5 (25%) |
| None | 5 (10%) | 1 (5%) |
| Months Post Stroke Diagnosis | ||
| Mean (sd) | 19. 5 (20.8) | 22.2 (19.7) |
| Range | 6–96 | 6–72 |
| Completed Education | ||
| Primary | 3 (7.5%) | 4 (17.5%) |
| Secondary | 26 (55%) | 9 (40%) |
| College | 1 (2.5%) | 3 (12.5%) |
| Bachelor’s | 15 (30%) | 5 (25%) |
| Master’s | 2 (5%) | 1 (5%) |
| Marital Status | ||
| Married | 30 (60%) | 16 (70%) |
| Single | 10 (31%) | 4 (20%) |
| Divorced | 7 (9%) | 2 (10%) |
| Socioeconomic Status Based on Former Occupation | ||
| Higher managerial | 16 (32%) | 5 (24%) |
| Intermediate occupation | 11 (24%) | 4 (18%) |
| Manual occupation | 9 (20%) | 4 (18%) |
| Unemployed | 11 (24%) | 9 (40%) |
| Percentiles | Whitney-U t-Test | p Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Aphasia | Median | Minimum | Maximum | 25th | 75th | |||
| ASRS BDAE-SF | no | - | - | - | - | - | - | - |
| yes | 3 | 1 | 5 | 2.00 | 4.00 | |||
| AIQ-21-GR total score | no | 13.50 | 0 | 61 | 10.00 | 19.75 | 202 | <0.001 |
| yes | 37 | 5 | 67 | 22.50 | 41.00 | |||
| AIQ-21-GR Communication | no | 0.00 | 0 | 13 | 0.00 | 5.75 | 143 | <0.001 |
| yes | 12 | 1 | 22 | 6.50 | 15.00 | |||
| AIQ-21-GR Emotional state/Well-being | no | 8.00 | 0 | 36 | 3.25 | 13.00 | 285 | 0.003 |
| yes | 16 | 0 | 36 | 9.00 | 22.00 | |||
| AIQ-21-GR Participation | no | 2.50 | 0 | 12 | 0.00 | 6.75 | 283 | 0.002 |
| yes | 7 | 0 | 16 | 3.50 | 11.00 | |||
| SAQOL-39 total score | no | 3.56 | 1.92 | 4.77 | 2.76 | 4.10 | 517 | 1 |
| yes | 3.51 | 1.17 | 4.90 | 3.10 | 4.01 | |||
| SAQOL-39 Communication | no | 5 | 2.71 | 5 | 4.18 | 5 | 210 | <0.001 |
| yes | 3.86 | 1.29 | 5 | 2.86 | 4.21 | |||
| SAQOL-39 Psychosocial | no | 3.84 | 1.88 | 5 | 2.98 | 4.06 | 369 | 0.056 |
| yes | 3.5 | 1.63 | 4.88 | 2.88 | 3.72 | |||
| AIQ-21-GR | Cronbach’s α | |
|---|---|---|
| Overall | 0.914 | |
| Domains | ||
| Communication | 0.887 | |
| Participation | 0.861 | |
| Emotional state/Well-being | 0.892 | |
| items | If item is dropped | Item-rest correlation |
| Item 1 | 0.911 | 0.516 |
| Item 2 | 0.909 | 0.619 |
| Item 3 | 0.911 | 0.513 |
| Item 4 | 0.910 | 0.551 |
| Item 5 | 0.910 | 0.573 |
| Item 6 | 0.909 | 0.594 |
| Item 7 | 0.909 | 0.588 |
| Item 8 | 0.913 | 0.471 |
| Item 9 | 0.909 | 0.611 |
| Item 10 | 0.911 | 0.541 |
| Item 11 | 0.910 | 0.554 |
| Item 12 | 0.911 | 0.507 |
| Item 13 | 0.906 | 0.728 |
| Item 14 | 0.910 | 0.550 |
| Item 15 | 0.912 | 0.475 |
| Item 16 | 0.909 | 0.606 |
| Item 17 | 0.910 | 0.586 |
| Item 18 | 0.909 | 0.622 |
| Item 19 | 0.910 | 0.593 |
| Item 20 | 0.911 | 0.522 |
| Item 21 | 0.914 | 0.378 |
| SAQOL-39 | |||
|---|---|---|---|
| Total Score | Communication | Psychosocial | |
| AIQ-21-GR | |||
| Total Score | −0.572 *** | ||
| Communication | −0.624 *** | ||
| Emotional state/Well-being | −0.516 *** | ||
| AIQ-21-GR | Communication | Participation | Emotional State/Well-Being |
|---|---|---|---|
| Communication | 0.463 *** | 0.479 *** | |
| Participation | 0.460 *** | ||
| Total Score | 0.657 *** | 0.601 *** | 0.732 *** |
| Factor | |||
|---|---|---|---|
| Emotional State/ | Communication | Participation | |
| Well-Being | |||
| Item 1 | 0.923 | ||
| Item 2 | 0.923 | ||
| Item 3 | 0.653 | ||
| Item 4 | 0.552 | ||
| Item 5 | 0.599 | ||
| Item 6 | 0.504 | ||
| Item 7 | 0.694 | ||
| Item 8 | 0.863 | ||
| Item 9 | 0.812 | ||
| Item 10 | 0.642 | ||
| Item 11 | 0.698 | ||
| Item 12 | 0.657 | ||
| Item 13 | 0.698 | ||
| Item 14 | 0.546 | ||
| Item 15 | 0.618 | ||
| Item 16 | 0.836 | ||
| Item 17 | 0.752 | ||
| Item 18 | 0.710 | ||
| Item 19 | 0.688 | ||
| Item 20 | 0.434 | ||
| Item 21 | 0.307 | ||
| Percentiles | ||||
|---|---|---|---|---|
| Group_Adj | Median | 25th | 75th | |
| Relevance | Healthy | 4.00 | 3.25 | 4.75 |
| PWA | 5.00 | 5.00 | 5.00 | |
| SLTs | 4.00 | 4.00 | 5.00 | |
| Stroke no aphasia | 4.00 | 3.75 | 4.25 | |
| Appropriateness | Healthy | 4.00 | 3.25 | 4.00 |
| PWA | 5.00 | 5.00 | 5.00 | |
| SLTs | 4.50 | 4.00 | 5.00 | |
| Stroke no aphasia | 4.00 | 3.75 | 4.25 | |
| Importance | Healthy | 5.00 | 4.25 | 5.00 |
| PWA | 5.00 | 5.00 | 5.00 | |
| SLTs | 5.00 | 5.00 | 5.00 | |
| Stroke no aphasia | 4.00 | 4.00 | 4.25 | |
| Clarity | Healthy | 4.00 | 4.00 | 4.75 |
| PWA | 5.00 | 5.00 | 5.00 | |
| SLTs | 5.00 | 4.00 | 5.00 | |
| Stroke no aphasia | 4.00 | 4.00 | 4.25 | |
| Content | Healthy | 4.00 | 4.00 | 4.75 |
| PWA | 4.50 | 4.00 | 5.00 | |
| SLT | 4.50 | 4.00 | 5.00 | |
| Stroke no aphasia | 4.00 | 4.00 | 4.25 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charalambous, M.; Phylactou, P.; Kountouri, A.; Serafeim, M.; Psychogios, L.; Annoni, J.-M.; Kambanaros, M. Adaptation of the Aphasia Impact Questionnaire-21 into Greek: A Reliability and Validity Study. Clin. Transl. Neurosci. 2022, 6, 24. https://doi.org/10.3390/ctn6040024
Charalambous M, Phylactou P, Kountouri A, Serafeim M, Psychogios L, Annoni J-M, Kambanaros M. Adaptation of the Aphasia Impact Questionnaire-21 into Greek: A Reliability and Validity Study. Clinical and Translational Neuroscience. 2022; 6(4):24. https://doi.org/10.3390/ctn6040024
Chicago/Turabian StyleCharalambous, Marina, Phivos Phylactou, Alexia Kountouri, Marios Serafeim, Loukia Psychogios, Jean-Marie Annoni, and Maria Kambanaros. 2022. "Adaptation of the Aphasia Impact Questionnaire-21 into Greek: A Reliability and Validity Study" Clinical and Translational Neuroscience 6, no. 4: 24. https://doi.org/10.3390/ctn6040024
APA StyleCharalambous, M., Phylactou, P., Kountouri, A., Serafeim, M., Psychogios, L., Annoni, J.-M., & Kambanaros, M. (2022). Adaptation of the Aphasia Impact Questionnaire-21 into Greek: A Reliability and Validity Study. Clinical and Translational Neuroscience, 6(4), 24. https://doi.org/10.3390/ctn6040024