
M1 Polarized Tumor-Associated Macrophages (TAMs) as Promising Prognostic Signature in Stage I–II Gastric Adenocarcinomas

 , ,
, , 

Abstract
:1. Introduction
2. Results
2.1. Incidence and Clinical Manifestations of Gastric Cancers with TAMs
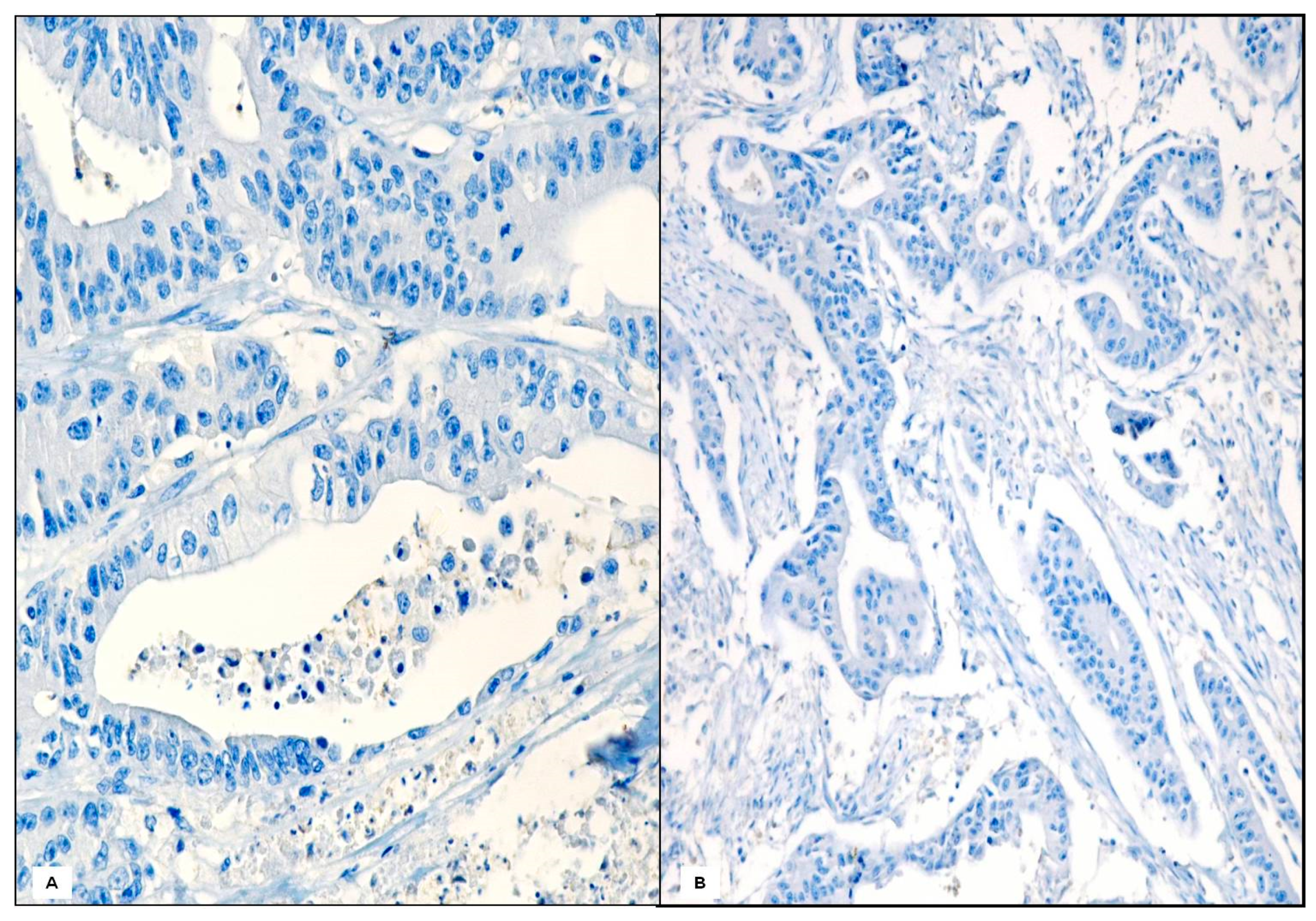
2.2. Histological Findings
2.3. Comparison of Clinicopathologic Parameters in Case and Control Groups
3. Discussion
4. Materials and Methods
4.1. Case Selection
4.2. Case-Control Study and Matching
4.3. Immunohistochemistry
4.4. Follow-Up
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Podlaha, O.; Riester, M.; De, S.; Michor, F. Evolution of the cancer genome. Trends Genet. 2012, 28, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Dvorak, H.F.; Weaver, V.M.; Tlsty, T.D.; Bergers, G. Tumor microenvironment and progression. J. Surg. Oncol. 2011, 103, 468–474. [Google Scholar] [CrossRef] [Green Version]
- Chanmee, T.; Ontong, P.; Konno, K.; Itano, N.; Chanmee, T. Tumor-Associated Macrophages as Major Players in the Tumor Microenvironment. Cancers 2014, 6, 1670–1690. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Tian, T.; Zhang, J. Tumor-Associated Macrophages (TAMs) in Colorectal Cancer (CRC): From Mechanism to Therapy and Prognosis. Int. J. Mol. Sci. 2021, 22, 8470. [Google Scholar] [CrossRef]
- Rihawi, K.; Ricci, A.; Rizzo, A.; Brocchi, S.; Marasco, G.; Pastore, L.; Llimpe, F.; Golfieri, R.; Renzulli, M. Tumor-Associated Macrophages and Inflammatory Microenvironment in Gastric Cancer: Novel Translational Implications. Int. J. Mol. Sci. 2021, 22, 3805. [Google Scholar] [CrossRef] [PubMed]
- Mills, C.D. Anatomy of a Discovery: M1 and M2 Macrophages. Front. Immunol. 2015, 6, 212. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Marchesi, F.; Malesci, A.; Laghi, L.; Allavena, P. Tumour-associated macrophages as treatment targets in oncology. Nat. Rev. Clin. Oncol. 2017, 14, 399–416. [Google Scholar] [CrossRef]
- Condeelis, J.; Pollard, J.W. Macrophages: Obligate Partners for Tumor Cell Migration, Invasion, and Metastasis. Cell 2006, 124, 263–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; McKay, D.; Pollard, J.W.; Lewis, C.E. Diverse Functions of Macrophages in Different Tumor Microenvironments. Cancer Res. 2018, 78, 5492–5503. [Google Scholar] [CrossRef] [Green Version]
- Edin, S.; Wikberg, M.L.; Dahlin, A.; Rutegård, J.; Öberg, Å.; Oldenborg, P.-A.; Palmqvist, R. The Distribution of Macrophages with a M1 or M2 Phenotype in Relation to Prognosis and the Molecular Characteristics of Colorectal Cancer. PLoS ONE 2012, 7, e47045. [Google Scholar] [CrossRef] [Green Version]
- Laforga, J.B.M. Foamy macrophages in pylorocardiac gastric carcinoma: A source of confusion with signet ring cell carcinoma. Histopathology 2003, 43, 98–100. [Google Scholar] [CrossRef]
- Go, Y.; Tanaka, H.; Tokumoto, M.; Sakurai, K.; Toyokawa, T.; Kubo, N.; Muguruma, K.; Maeda, K.; Ohira, M.; Hirakawa, K. Tumor-Associated Macrophages Extend Along Lymphatic Flow in the Pre-metastatic Lymph Nodes of Human Gastric Cancer. Ann. Surg. Oncol. 2015, 23, 230–235. [Google Scholar] [CrossRef]
- Zhu, Q.; Wu, X.; Tang, M.; Wu, L. Observation of tumor-associated macrophages expression in gastric cancer and its clinical pathological relationship. Medicine 2020, 99, e19839. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Sung, J.Y.; Lee, J.; Park, Y.K.; Kim, Y.W.; Kim, G.Y.; Won, K.Y.; Lim, S.J. Polarized CD163+ tumor-associated macrophages are associated with increased angio-genesis and CXCL12 expression in gastric cancer. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 357–365. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Fushida, S.; Yamamoto, Y.; Tsukada, T.; Kinoshita, J.; Oyama, K.; Miyashita, T.; Tajima, H.; Ninomiya, I.; Munesue, S.; et al. Tumor-associated macrophages of the M2 phenotype contribute to pro-gression in gastric cancer with peritoneal dissemination. Gastric Cancer 2016, 19, 1052–1065. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yu, Y.; He, X.; Niu, N.; Li, X.; Zhang, R.; Hu, J.; Ma, J.; Yu, X.; Sun, Y.; et al. Tumor-associated macrophages induce invasion and poor prognosis in human gastric cancer in a cyclooxygenase-2/MMP9-dependent manner. Am. J. Transl. Res. 2019, 11, 6040–6054. [Google Scholar]
- Liu, L.; Ye, Y.; Zhu, X. MMP-9 secreted by tumor associated macrophages promoted gastric cancer metastasis through a PI3K/AKT/Snail pathway. Biomed. Pharmacother. 2019, 117, 109096. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, V.; Castillo, J.; Tarazona, N.; Gimeno-Valiente, F.; Martínez-Ciarpaglini, C.; Cabeza-Segura, M.; Roselló, S.; Roda, D.; Huerta, M.; Cervantes, A.; et al. The role of tumor-associated macrophages in gastric cancer development and their potential as a therapeutic target. Cancer Treat. Rev. 2020, 86, 102015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.K.; Wang, M.; Sun, Y.; Di Costanzo, N.; Mitchell, C.; Achuthan, A.; Hamilton, J.A.; Busuttil, R.A.; Boussioutas, A. Macrophage spatial heterogeneity in gastric cancer defined by multiplex immuno-histochemistry. Nat. Commun. 2019, 10, 3928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chayanon, N.; Heather, H.; Suzie, H.P. Progress in tumor-associated macrophage (TAM)-targeted therapeutics. Adv. Drug Deliv. Rev. 2017, 114, 206–221. [Google Scholar]
- Luo, Q.; Zheng, N.; Jiang, L.; Wang, T.; Zhang, P.; Liu, Y.; Zheng, P.; Wang, W.; Xie, G.; Chen, L.; et al. Lipid accumulation in macrophages confers protumorigenic polarization and immunity in gastric cancer. Cancer Sci. 2020, 111, 4000–4011. [Google Scholar] [CrossRef] [PubMed]
- Nie, K.; Zheng, Z.; Wen, Y.; Pan, J.; Liu, Y.; Jiang, X.; Yan, Y.; Jiang, K.; Liu, P.; Xu, S.; et al. A novel ceRNA axis involves in regulating immune infiltrates and macrophage polarization in gastric cancer. Int. Immunopharmacol. 2020, 87, 106845. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Zhang, Y.; He, F.; Lv, S.; Zhang, X.; Fei, C. Abundance of CD163-Positive Tumor-Associated Macrophages in the Early Gastric Cancer Predicts the Recurrence after Curative Resection. Dig. Dis. 2020, 38, 458–465. [Google Scholar] [CrossRef]
- Oya, Y.; Hayakawa, Y.; Koike, K. Tumor microenvironment in gastric cancers. Cancer Sci. 2020, 111, 2696–2707. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, X.; Wu, F.; Zhou, Y.; Bao, Z.; Li, H.; Zheng, P.; Zhao, S. Gastric cancer-derived mesenchymal stromal cells trigger M2 macrophage polarization that promotes metastasis and EMT in gastric cancer. Cell Death Dis. 2019, 10, 918. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Xu, Y.; Wu, Y.; Huang, X.-Y.; Xie, J.-W.; Wang, J.-B.; Lin, J.-X.; Li, P.; Zheng, C.-H.; Huang, A.-M.; et al. Tumor-infiltrating CD8+ T cells combined with tumor-associated CD68+ macrophages predict postoperative prognosis and adjuvant chemotherapy benefit in resected gastric cancer. BMC Cancer 2019, 19, 920. [Google Scholar] [CrossRef]
- Wei, C.; Yang, C.; Wang, S.; Shi, D.; Zhang, C.; Lin, X.; Liu, Q.; Dou, R.; Xiong, B. Crosstalk between cancer cells and tumor associated macrophages is required for mesenchymal circulating tumor cell-mediated colorectal cancer metastasis. Mol. Cancer 2019, 18, 64. [Google Scholar] [CrossRef]
- Umakoshi, M.; Takahashi, S.; Itoh, G.; Kuriyama, S.; Sasaki, Y.; Yanagihara, K.; Yashiro, M.; Maeda, D.; Goto, A.; Tanaka, M. Macrophage-mediated transfer of cancer-derived components to stromal cells contributes to establishment of a pro-tumor microenvironment. Oncogene 2018, 38, 2162–2176. [Google Scholar] [CrossRef]
- Räihä, M.R.; Puolakkainen, P.A. Tumor-associated macrophages (TAMs) as biomarkers for gastric cancer: A review. Chronic Dis. Transl. Med. 2018, 4, 156–163. [Google Scholar] [CrossRef]
- Shigematsu, H.; Kurita, A.; Omura, Y.; Kubo, Y.; Takashima, S.; Mandai, K. Gastric cancer with sarcoid reactions in the regional lymph nodes, the stomach wall, and the splenic parenchyma: Report of a case. Surg. Today 1999, 29, 549–552. [Google Scholar] [CrossRef]
- Nakamura, M.; Mizuta, E.; Morioka, H.; Nakamura, M.; Isiglo, K. Multiple early gastric cancer associated with sarcoid-like reaction in the regional lymph nodes. J Gastroenterol 2001, 36, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Nakamura, S.; Fujisaki, M.; Hirahata, S.; Hasegawa, H.; Maeda, D.; Suito, T.; Motoori, T.; Joshita, T.; Suzuki, K.; et al. Sarcoid-like reaction in the regional lymph nodes and spleen in gastric carci-noma: A clinicopathologic study of five cases. Gen. Diagn. Pathol. 1997, 142, 347–352. [Google Scholar]
- Zhang, W.-J.; Zhou, Z.-H.; Guo, M.; Yang, L.-Q.; Xu, Y.-Y.; Pang, T.-H.; Gao, S.-T.; Xu, X.-Y.; Sun, Q.; Feng, M.; et al. High Infiltration of Polarized CD163+ Tumor-Associated Macrophages Correlates with Aberrant Expressions of CSCs Markers, and Predicts Prognosis in Patients with Recurrent Gastric Cancer. J. Cancer 2017, 8, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Pan, Y.; Ma, J.; Kang, Z.; Xu, X.; Zhu, Y.; Chen, J.; Zhang, W.; Chang, W.; Zhu, J. Prognostic significance of the infiltration of CD163+macrophages combined with CD66b+neutrophils in gastric cancer. Cancer Med. 2018, 7, 1731–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniyama, D.; Taniyama, K.; Kuraoka, K.; Zaitsu, J.; Saito, A.; Nakatsuka, H.; Sakamoto, N.; Sentani, K.; Oue, N.; Yasui, W. Long-term follow-up study of gastric adenoma; tumor-associated macrophages are associated to carcinoma development in gastric adenoma. Gastric Cancer 2017, 20, 929–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.W.; Liu, L.; Gong, C.Y.; Shi, H.S.; Zeng, Y.H.; Wang, X.Z.; Zhao, Y.W.; Wei, Y.Q. Prognostic significance of tumor-associated macrophages in solid tumor: A me-ta-analysis of the literature. PLoS ONE 2012, 7, e50946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, K.; Cheng, T.; Zhan, J.; Peng, X.; Zhang, Y.; Wen, J.; Chen, X.; Ying, M. Targeting tumor-associated macrophages in the tumor microenvironment. Oncol. Lett. 2020, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Galdiero, M.R.; Marone, G.; Mantovani, A. Cancer Inflammation and Cytokines. Cold Spring Harb. Perspect. Biol. 2018, 10, a028662. [Google Scholar] [CrossRef] [Green Version]
- Jayasingam, S.D.; Citartan, M.; Thang, T.H.; Zin, A.A.M.; Ang, K.C.; Ch’Ng, E.S. Evaluating the Polarization of Tumor-Associated Macrophages into M1 and M2 Phenotypes in Human Cancer Tissue: Technicalities and Challenges in Routine Clinical Practice. Front. Oncol. 2020, 9, 1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avvisati, G.; Tirindelli, M.C.; Annibali, O. Thrombocytopenia and hemorrhagic risk in cancer patients. Crit. Rev. Oncol. 2003, 48, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; He, S.; Liu, X.; Jiang, W.; Ye, T.; Lin, Z.; Sang, Y.; Su, C.; Wan, Y.; Shen, G.; et al. Extravascular Red Blood Cells and Hemoglobin Promote Tumor Growth and Therapeutic Resistance as Endogenous Danger Signals. J. Immunol. 2014, 194, 429–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, M.C.; Breckwoldt, M.O.; Vinchi, F.; Correia, M.P.; Stojanovic, A.; Thielmann, C.M.; Meister, M.; Muley, T.; Warth, A.; Platten, M.; et al. Iron Induces Anti-tumor Activity in Tumor-Associated Macrophages. Front. Immunol. 2017, 8, 1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielmann, C.M.; Costa da Silva, M.; Muley, T.; Meister, M.; Herpel, E.; Muckenthaler, M.U. Iron accumulation in tu-mor-associated macrophages marks an improved overall survival in patients with lung adenocarcinoma. Sci. Rep. 2019, 9, 11326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauwers, G.Y.; Carneiro, F.; Graham, D.Y.; Curado, M.P.; Franceschi, S.; Montgomery, E.; Tatematsu, M.; Hattori, T. Gastric carcinoma. In WHO Classification of Tumours of the Digestive System; Bosman, F.T., Carneiro, F., Hruban, R.H., Theise, N.D., Eds.; WHO Press: Geneva, Switzerland, 2010; pp. 48–58. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Christian Wittekind, C. International Union Against Cancer (UICC): TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | X2 | df | p Value |
|---|---|---|---|
| Lymphovascular invasion | 1.886 | 1 | 0.170 |
| Perineural invasion | 1.788 | 1 | 0.181 |
| Stage | 13.831 | 1 | 0.000 |
| TAMs presence | 4.445 | 1 | 0.035 |
| Variables | β | SE | Exp (β) | p Value |
|---|---|---|---|---|
| Stage | 1.671 | 0.493 | 5.318 | 0.001 |
| TAMs presence | −1.270 | 0.610 | 0.281 | 0.037 |
| Variables | Case (n = 24) | Controls (n= 72) | p Value |
|---|---|---|---|
| Age (years), median | 72 | 72.5 | 0.830 |
| Sex | |||
| Male | 15 | 43 | |
| Female | 9 | 29 | 0.503 |
| Location | |||
| Fundus | 1 | 2 | |
| Corpus | 10 | 29 | |
| Antrum | 13 | 41 | 0.930 |
| Size (mm) median | 52 | 55 | 0.200 |
| Invasion | |||
| T1 | 2 | 6 | |
| T2 | 14 | 42 | |
| T3 | 8 | 24 | 1.000 |
| Lymphovascular invasion | |||
| Absent | 16 | 33 | |
| Present | 8 | 39 | 0.062 |
| Perineural invasion | |||
| Absent | 22 | 68 | |
| Present | 2 | 4 | 0.469 |
| Nodal metastases | |||
| Absent | 17 | 32 | |
| Present | 7 | 40 | 0.022 |
| Stage | |||
| I | 11 | 33 | |
| II | 13 | 39 | 0.592 |
| Helicobacter pylori status | |||
| Presence | 18 | 54 | |
| Absence | 6 | 18 | 0.615 |
| Clinical course | |||
| Alive | 21 | 46 | |
| Death from gastric cancer | 3 | 26 | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ieni, A.; Caruso, R.A.; Pizzimenti, C.; Giuffrè, G.; Irato, E.; Rigoli, L.; Navarra, G.; Fadda, G.; Tuccari, G. M1 Polarized Tumor-Associated Macrophages (TAMs) as Promising Prognostic Signature in Stage I–II Gastric Adenocarcinomas. Gastrointest. Disord. 2021, 3, 207-217. https://doi.org/10.3390/gidisord3040020
Ieni A, Caruso RA, Pizzimenti C, Giuffrè G, Irato E, Rigoli L, Navarra G, Fadda G, Tuccari G. M1 Polarized Tumor-Associated Macrophages (TAMs) as Promising Prognostic Signature in Stage I–II Gastric Adenocarcinomas. Gastrointestinal Disorders. 2021; 3(4):207-217. https://doi.org/10.3390/gidisord3040020
Chicago/Turabian StyleIeni, Antonio, Rosario Alberto Caruso, Cristina Pizzimenti, Giuseppe Giuffrè, Eleonora Irato, Luciana Rigoli, Giuseppe Navarra, Guido Fadda, and Giovanni Tuccari. 2021. "M1 Polarized Tumor-Associated Macrophages (TAMs) as Promising Prognostic Signature in Stage I–II Gastric Adenocarcinomas" Gastrointestinal Disorders 3, no. 4: 207-217. https://doi.org/10.3390/gidisord3040020
APA StyleIeni, A., Caruso, R. A., Pizzimenti, C., Giuffrè, G., Irato, E., Rigoli, L., Navarra, G., Fadda, G., & Tuccari, G. (2021). M1 Polarized Tumor-Associated Macrophages (TAMs) as Promising Prognostic Signature in Stage I–II Gastric Adenocarcinomas. Gastrointestinal Disorders, 3(4), 207-217. https://doi.org/10.3390/gidisord3040020