
The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Data Selection and Extraction
2.3. Risk of Bias
3. Results
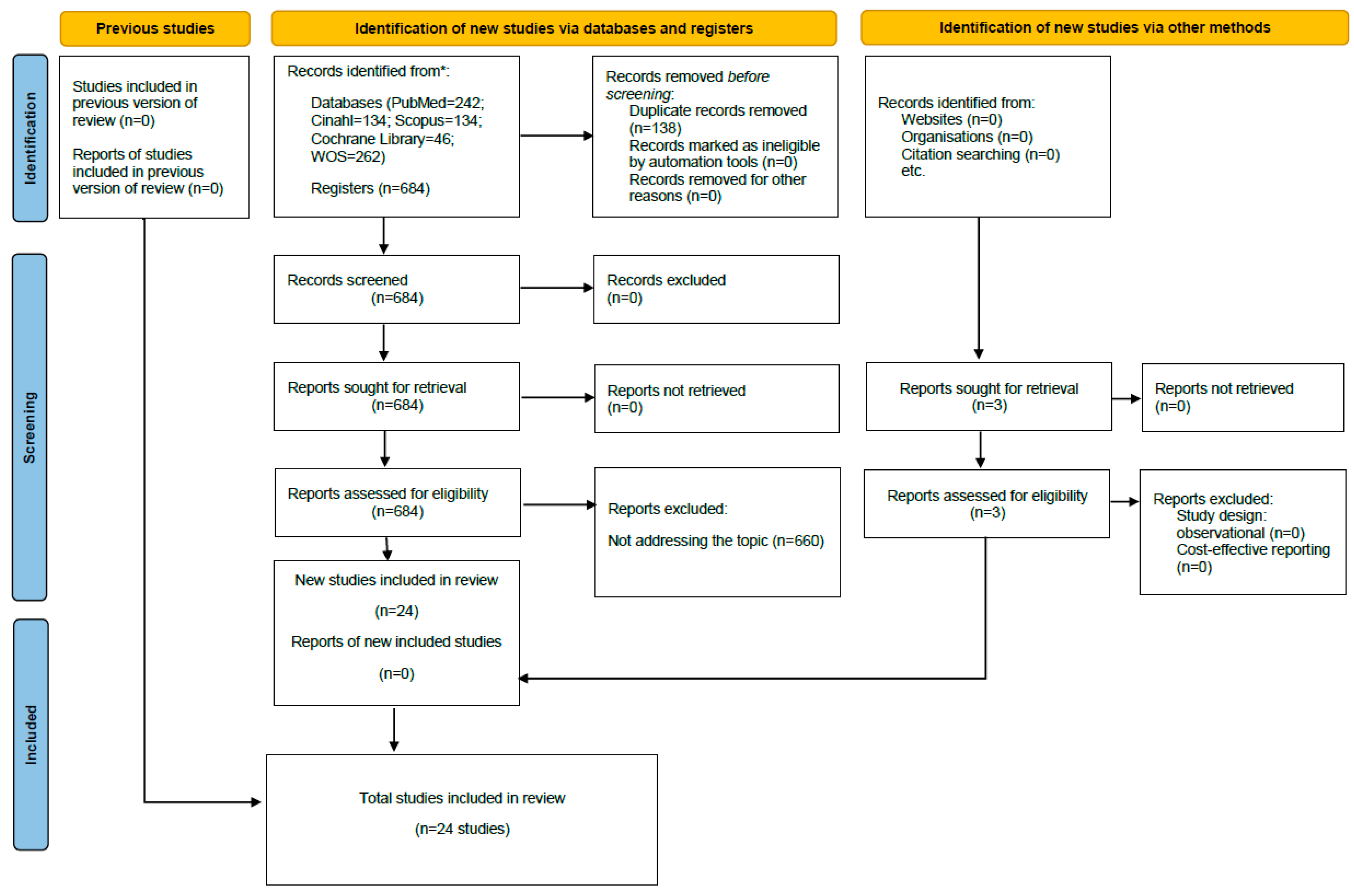
3.1. Results Obtained in the Selection of Articles
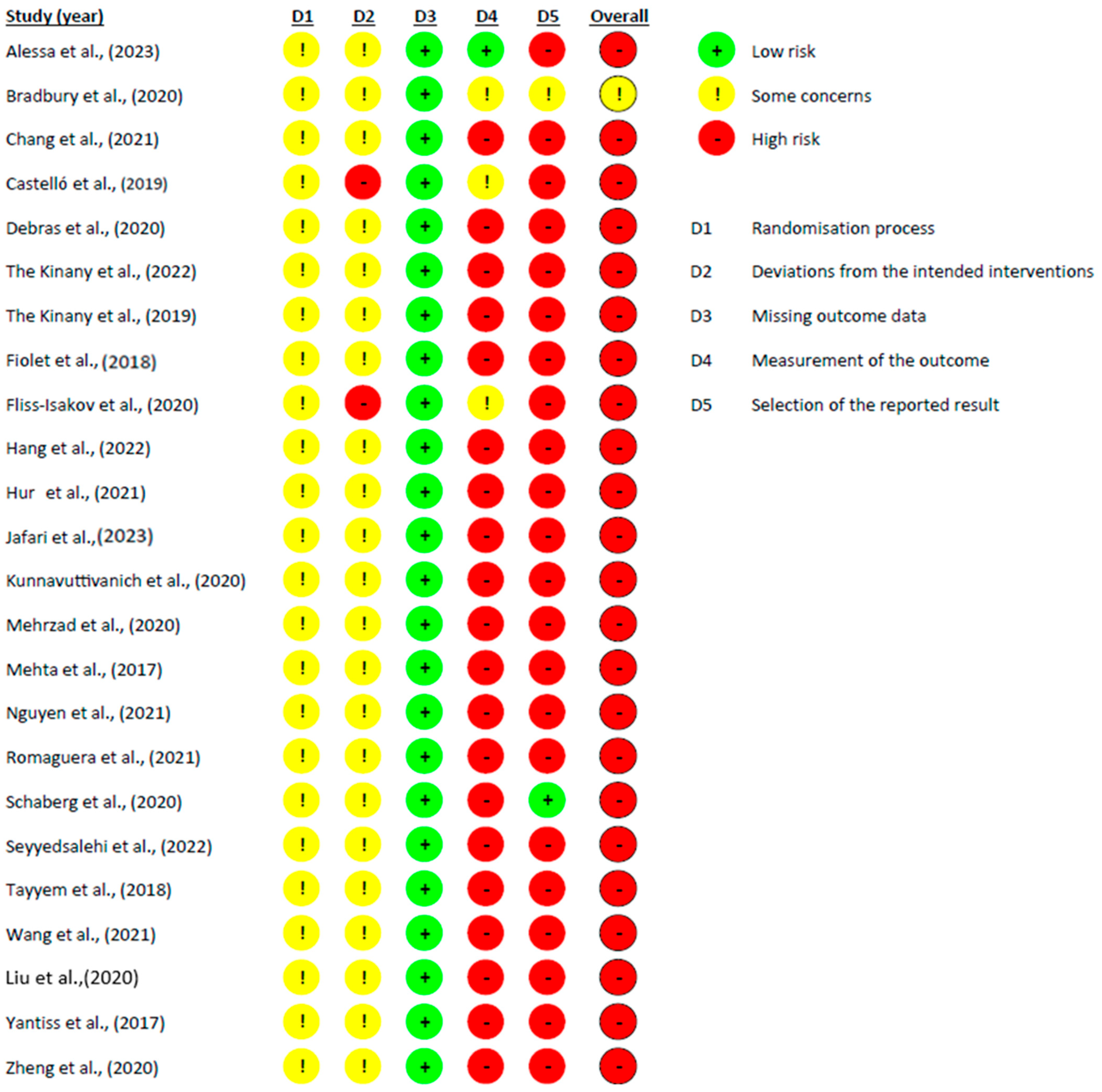
3.2. Bias Risk Assessment of the Selected Studies and Publication Bias
3.3. Descriptive Analysis of the Results Found
3.3.1. Sugar Consumption
3.3.2. Consumption of Red and/or Processed Meats
3.3.3. Fats Consumption
3.3.4. Alcohol Consumption
3.3.5. Other Related Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AC | Alcohol Consumption |
| ALA | Alphalinolenic Acid |
| BMI | Body Mass Index |
| BPA | Bisphenol A |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| CPSS | Perceived Psychological Stress Scale |
| CRC | Colorectal Cancer |
| DHA | Docosahexanoic Acid |
| DHQII | Dietary Health Questionnaire II |
| DNA | Deoxyribonucleic Acid |
| EPA | Eicosapentaenoic Acid |
| FC | Fat Consumption |
| LDL | Low-Density Lipoprotein |
| MeSH | Medical Subject Headings |
| MMQ | Meat Module List |
| OF | Other Factors |
| PUFA | Polyunsaturated Omega-3 Fatty Acids |
| ROB II | Risk of Bias in Non-Randomised Studies of Interventions |
| RPM | Red and/or Processed Meat |
| SC | Sugar Consumption |
| SFA | Saturated Fatty Acids |
| iTFA | Trans Fatty Acids |
| UC | Association between Different Groups of UPF and CRC |
| UPF | Ultra-processed Food |
| VLDL | Very Low-Density Lipoprotein |
| WHO | World Health Organization |
| WOS | Web of Science |
References
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical activity, sedentary behaviour, diet, and cancer: An update and emerging new evidence. Lancet Oncol. 2017, 18, 457–471. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Du, M.; Wang, K.; Khandpur, N.; Rossato, S.L.; Drouin-Chartier, J.; Martínez-Steele, E.; Giovannucci, E.; Song, M.; Zhang, F.F. Association of ultra-processed food consumption with colorectal cancer risk among men and women: Results from three prospective US cohort studies. BMJ 2022, 378, e068921. [Google Scholar] [CrossRef]
- National Cancer Institute. Available online: https://www.cancer.gov/types/colorectal/hp/colorectal-prevention-pdq (accessed on 5 December 2023).
- Islami, F.; Goding Sauer, A.; Miller, K.D.; Siegel, R.L.; Fedewa, S.A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Ma, J.; Soerjomataram, I.; et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J. Clin. 2018, 68, 31–54. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund; American Institute for Cancer Research Diet; Nutrition, Physical Activity; Liver Cancer. Continuous Update Project Report; World Cancer Research Fund, American Institute for Cancer Research: London, UK, 2015; Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 8 December 2023).
- Aburto, T.C.; Romieu, I.; Stern, M.C.; Barquera, S.; Corvalán, C.; Hallal, P.C.; Reynales-Shigematsu, L.M.; Barnoya, J.; Cavalcante, T.M.; Canelo-Aybar, C.; et al. Latin American and the Caribbean Code Against Cancer 1st edition: Weight, physical activity, diet, breastfeeding, and cancer. Cancer Epidemiol. 2023, 86, 102436. [Google Scholar] [CrossRef]
- Inan-Eroglu, E.; Huang, B.H.; Sarich, P.; Nassar, N.; Stamatakis, E. Joint association of alcohol consumption and adiposity with alcohol- and obesity-related cancer in a population sample of 399,575. UK adults. Br. J. Nutr. 2023, 130, 503–512. [Google Scholar] [CrossRef]
- He, Z.J.; Yusufu, W.; Zhang, S.; Luo, M.Y.; Chen, Y.C.; Peng, H.; Wan, X.Y. Association between Dietary Inflammatory Index and Risk of Colorectal Adenomatous Polyps in Kashgar Prefecture of Xinjiang, China. Nutrients 2023, 15, 4067. [Google Scholar] [CrossRef]
- Krautkramer, K.A.; Kreznar, J.H.; Romano, K.A.; Vivas, E.I.; Barrett-Wilt, G.A.; Rabaglia, M.E.; Keller, M.P.; Attie, A.D.; Rey, F.E.; Denu, J.M. Diet-Microbiota Interactions Mediate Global Epigenetic Programming in Multiple Host Tissues. Mol. Cell 2016, 64, 982–992. [Google Scholar] [CrossRef]
- Gertz, C.; Aladedunye, F.; Popp, M.; Matthäus, B. The Impact of Fat Deterioration on Formation of Acrylamide in Fried Foods. Eur. J. Lipid Sci. Technol. 2023, 125, 2200144. [Google Scholar] [CrossRef]
- Shabbir, M.A.; Raza, A.; Anjum, F.M.; Khan, M.R.; Suleria, H.A. Effect of Thermal Treatment on Meat Proteins with Special Reference to Heterocyclic Aromatic Amines (HAAs). Crit. Rev. Food Sci. Nutr. 2015, 55, 82–93. [Google Scholar] [CrossRef]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A.; et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef]
- Cavagnari, B. Non-caloric sweeteners and body weight. Med. B Aires 2019, 79, 115–122. [Google Scholar]
- Laudanno, O.M. Cambios en la microbiota por ultraprocesados: Obesidad, cáncer y muerte premature. Med. B Aires 2023, 83, 278–282. [Google Scholar]
- Göncüoğlu, N.; Kocadağlı, T.; Gökmen, V. Safety concerns of processed foods in terms of neo-formed contaminants and NOVA classification. Curr. Opin. Food Sci. 2022, 47, 100876. [Google Scholar] [CrossRef]
- Trakman, G.L.; Fehily, S.; Basnayake, C.; De Cruz, P.; Russell, E.; Wilson-O’Brien, A.; Kamm, M.A. Diet and gut microbiome in gastrointestinal disease. J. Gastroenterol. Hepatol. 2021, 37, 237–245. [Google Scholar] [CrossRef]
- Godos, J.; Bella, F.; Sciacca, S.; Galvano, F.; Grosso, G. Vegetarianism and breast, colorectal and prostate cancer risk: An overview and meta-analysis of cohort studies. J. Hum. Nutr. Diet. 2017, 30, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Aromataris, E.; Tufanaru, C.; Stern, C.; Porritt, K.; Farrow, J.; Lockwood, C.; Stephenson, M.; Moola, S.; Lizarondo, L.; et al. The development of software to support multiple systematic review types: The Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI). Int. J. Evid. Based Healthc. 2019, 17, 36–43. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011; Available online: https://training.cochrane.org/handbook/current (accessed on 8 December 2023).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Updated February 2021; Cochrane: London, UK, 2021; Available online: https://training.cochrane.org/handbook (accessed on 7 December 2023).
- Alessa, M.; Alarfaj, M.O.; Albenayyan, H.A.; Aleidan, A.A.; Albahrani, F.A.; Bokhuwah, M.A.; Bukhamsin, R.M.; Alzahrani, R.M.; Alkhalifah, M.F.; Alshekhmobarak, L.A.; et al. Awareness of the Link Between the Consumption of Ultra-Processed Food and Colorectal Cancer Risk in Saudi Arabia. Cureus 2023, 15, e33774. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, K.E.; Murphy, N.; Key, T.J. Diet and colorectal cancer in UK Biobank: A prospective study. Int. J. Epidemiol. 2020, 49, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Chang, V.C.; Cotterchio, M.; De, P.; Tinmouth, J. Risk factors for early-onset colorectal cancer: A population-based case–control study in Ontario, Canada. Cancer Causes Control 2021, 32, 1063–1083. [Google Scholar] [CrossRef]
- Castelló, A.; Amiano, P.; De Larrea, N.F.; Martín, V.; Alonso, M.J.; Castaño-Vinyals, G.; Pérez-Gómez, B.; Olmedo-Requena, R.; Guevara, M.; Fernández-Tardón, G.; et al. Low adherence to the western and high adherence to the mediterranean dietary patterns could prevent colorectal cancer. Eur. J. Nutr. 2019, 58, 1495–1505. [Google Scholar] [CrossRef]
- Debras, C.; Chazelas, E.; Srour, B.; Kesse-Guyot, E.; Julia, C.; Zelek, L.; Agaësse, C.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; et al. Total and added sugar intakes, sugar types, and cancer risk: Results from the prospective NutriNet-Santé cohort. Am. J. Clin. Nutr. 2020, 112, 1267–1279. [Google Scholar] [CrossRef]
- The Kinany, K.E.; Huybrechts, I.; Hatime, Z.; Asri, A.E.; Boudouaya, H.A.; Deoula, M.M.S.; Kampman, E.; Rhazi, K.E. Food processing groups and colorectal cancer risk in Morocco: Evidence from a nationally representative case–control study. Eur. J. Nutr. 2022, 61, 2507–2515. [Google Scholar] [CrossRef]
- The Kinany, K.E.; Huybrechts, I.; Kampman, E.; Boudouaya, H.A.; Hatime, Z.; Deoula, M.M.S.; Asri, A.E.; Benslimane, A.; Nejjari, C.; Ibrahimi, S.A.; et al. Concordance with the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention and colorectal cancer risk in Morocco: A large, population-based case–control study. Int. J. Cancer 2019, 145, 1829–1837. [Google Scholar] [CrossRef]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef]
- Fliss-Isakov, N.; Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Shibolet, O.; Kariv, R. Ultra-Processed Food Intake and Smoking Interact in Relation with Colorectal Adenomas. Nutrients 2020, 12, 3507. [Google Scholar] [CrossRef] [PubMed]
- Hang, D.; Wang, L.; Fang, Z.; Du, M.; Wang, K.; He, X.; Khandpur, N.; Rossato, S.L.; Wu, K.; Hu, Z.; et al. Ultra-processed food consumption and risk of colorectal cancer precursors: Results from 3 prospective cohorts. J. Natl. Cancer Inst. 2022, 115, 155–164. [Google Scholar] [CrossRef]
- Hur, J.; Otegbeye, E.E.; Joh, H.K.; Nimptsch, K.; Ng, K.; Ogino, S.; Meyerhardt, J.A.; Chan, A.T.; Willett, W.C.; Wu, K.; et al. Sugar-sweetened beverage intake in adulthood and adolescence and risk of early-onset colorectal cancer among women. Gut 2021, 70, 2330–2336. [Google Scholar] [CrossRef] [PubMed]
- Jafari, F.; Yarmand, S.; Nouri, M.; Nejad, E.T.; Ramezani, A.; Sohrabi, Z.; Rashidkhani, B. Ultra-Processed Food Intake and Risk of Colorectal Cancer: A Matched Case-Control Study. Nutr. Cancer 2023, 75, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Kunnavuttivanich, V.; Pramyothin, P.; Ithimakin, S. Association between dietary patterns and disease recurrence in Thai colorectal cancer patients. Medicine 2020, 99, e19522. [Google Scholar] [CrossRef]
- Mehrzad, J.; Dayyani, M.; Erfanian-Korasani, M. The independent and combined effects of selected risk factors and Arg399Gln XRCC1 polymorphism in the risk of colorectal cancer among an Iranian population. Med. J. Islam. Repub. Iran 2020, 34, 524–531. [Google Scholar] [CrossRef]
- Mehta, R.S.; Song, M.; Nishihara, R.; Drew, D.A.; Wu, K.; Qian, Z.R.; Fung, T.T.; Hamada, T.; Masugi, Y.; da Silv, A.; et al. Dietary Patterns and Risk of Colorectal Cancer: Analysis by Tumor Location and Molecular Subtypes. Gastroenterology 2017, 152, 1944–1953.e1. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Cao, H.; Hur, J.; Mehta, R.S.; Sikavi, D.; Wang, Y.; Ma, W.; Wu, K.; Song, M.; Giovannucci, E.; et al. The Sulfur Microbial Diet Is Associated with Increased Risk of Early-Onset Colon Cancer. Gastroenterology 2021, 161, 1423–1432.e4. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Fernández-Barrés, S.; Gracia-Lavedan, E.; Vendrell, E.; Azpiri, M.; Ruiz, E.; Martín, V.; Gómez-Acebo, I.; Obón-Santacana, M.; Molinuevo, A.; et al. Consumption of ultra-processed foods and drinks and colorectal, breast, and prostate cancer. Clin. Nutr. 2021, 40, 1537–1545. [Google Scholar] [CrossRef]
- Schaberg, M.N.; Smith, K.S.; Greene, M.W.; Frugé, A.D. Characterizing Demographic and Geographical Differences in Health Beliefs and Dietary Habits Related to Colon Cancer Risk in US Adults. Front. Nutr. 2020, 7, 568643. [Google Scholar] [CrossRef] [PubMed]
- Seyyedsalehi, M.S.; Collatuzzo, G.; Rashidian, H.; Hadji, M.; Gholipour, M.; Mohebbi, E.; Kamangar, F.; Pukkala, E.; Huybrechts, I.; Gunter, M.J.; et al. Dietary Ruminant and Industrial Trans-Fatty Acids Intake and Colorectal Cancer Risk. Nutrients 2022, 14, 4912. [Google Scholar] [CrossRef] [PubMed]
- Tayyem, R.F.; Bawadi, H.; Shehadah, I.; Bani-Hani, K.E.; Takruri, H.R.; Al-Jaberi, T.M.; Heath, D.D. Fast Foods, Sweets and Beverage Consumption and Risk of Colorectal Cancer: A Case-Control Study in Jordan. Asian Pac. J. Cancer Prev. 2018, 19, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Nguyen, L.H.; Mehta, R.S.; Song, M.; Huttenhower, C.; Chan, A.T. Association Between the Sulfur Microbial Diet and Risk of Colorectal Cancer. JAMA Netw. Open 2021, 4, e2134308. [Google Scholar] [CrossRef] [PubMed]
- Liu, X. Study on the relationship between diet and environmental exposure-related factors and the incidence of colorectal cancer. Int. J. Clin. Exp. Med. 2020, 13, 8037–8043. [Google Scholar]
- Yantiss, R.K. Persistent Problems in Colorectal Cancer Reporting. Surg. Pathol. Clin. 2017, 10, 961–976. [Google Scholar] [CrossRef]
- Zheng, X.; Hur, J.; Nguyen, L.H.; Liu, J.; Song, M.; Wu, K.; Smith-Warner, S.A.; Ogino, S.; Willett, W.C.; Chan, A.T.; et al. Comprehensive Assessment of Diet Quality and Risk of Precursors of Early-Onset Colorectal Cancer. J. Natl. Cancer Inst. 2020, 113, 543–552. [Google Scholar] [CrossRef]
- Kerschbaum, E.; Nüssler, V. Cancer Prevention with Nutrition and Lifestyle. Visc. Med. 2019, 35, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Viennois, E.; Merlin, D.; Gewirtz, A.T.; Chassaing, B. Dietary Emulsifier-Induced Low-Grade Inflammation Promotes Colon Carcinogenesis. Cancer Res. 2017, 77, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Pietrzyk, Ł. Food properties and dietary habits in colorectal cancer prevention and development. Int. J. Food Prop. 2017, 20, 2323–2343. [Google Scholar] [CrossRef]
- Morze, J.; Danielewicz, A.; Przybyłowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.; Peleteiro, B.; Lunet, N. Modifiable factors and esophageal cancer: A systematic review of published meta-analyses. J. Gastroenterol. 2018, 53, 37–51. [Google Scholar] [CrossRef]
- Michels, N.; van Aart, C.; Morisse, J.; Mullee, A.; Huybrechts, I. Chronic inflammation towards cancer incidence: A systematic review and meta-analysis of epidemiological studies. Crit. Rev. Oncol. Hematol. 2021, 157, 103177. [Google Scholar] [CrossRef]
- Fardet, A.; Druesne-Pecollo, N.; Touvier, M.; Latino-Martel, P. Do alcoholic beverages, obesity and other nutritional factors modify the risk of familial colorectal cancer? A systematic review. Crit. Rev. Oncol. Hematol. 2017, 119, 94–112. [Google Scholar] [CrossRef]
- Farvid, M.S.; Sidahmed, E.; Spence, N.D.; Mante Angua, K.; Rosner, B.A.; Barnett, J.B. Consumption of red meat and processed meat and cancer incidence: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 937–951. [Google Scholar] [CrossRef]
- Kim, S.R.; Kim, K.; Lee, S.A.; Kwon, S.O.; Lee, J.K.; Keum, N.; Park, S.M. Effect of red, processed, and white meat consumption on the risk of gastric cancer: An overall and dose-response meta-analysis. Nutrients 2019, 11, 826. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Moradi-Lakeh, M.; Salehi, M.H.; Nojomi, M.; Kolahdooz, F. Meat, fish, and esophageal cancer risk: A systematic review and dose-response meta-analysis. Nutr. Rev. 2013, 71, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Isaksen, I.M.; Danklel, S.N. Ultra-Processed food consumption and cancer risk: A systematic review and meta-analysis. Clin. Nutr. 2023, 42, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Huang, Y.; Si, C.; Zhu, Q.; Zheng, P.; Zhang, X. Association between ultra-processed food intake and risk of colorectal cancer: A systematic review and meta-analysis. Front. Nutr. 2023, 10, 1170992. [Google Scholar] [CrossRef] [PubMed]
- Lian, Y.; Wang, G.P.; Chen, G.Q.; Chen, H.N.; Zhang, G.Y. Association between ultra-processed foods and risk of cancer: A systematic review and meta-analysis. Front. Nutr. 2023, 10, 1175994. [Google Scholar] [CrossRef] [PubMed]
- Petimar, J.; Smith-Warner, S.A.; Fung, T.T.; Rosner, B.; Chan, A.T.; Hu, F.B.; Giovannucci, E.L.; Tabung, F.K. Recommendation-based dietary indexes and risk of colorectal cancer in the nurses’ health study and health professionals follow-up study. Am. J. Clin. Nutr. 2018, 108, 1092–1103. [Google Scholar] [CrossRef]
- Kim, H.; Giovannucci, E.L. Sex differences in the association of obesity and colorectal cancer risk. Cancer Causes Control. 2017, 28, 1–4. [Google Scholar] [CrossRef]
- Islam, M.R.; Rahman, S.M.; Rahman, M.M.; Pervin, J.; Rahman, A.; Ekström, E.C. Gender and socio-economic stratification of ultra-processed and deep-fried food consumption among rural adolescents: A cross-sectional study from Bangladesh. PLoS ONE 2022, 17, e0272275. [Google Scholar] [CrossRef]
- Dicken, S.J.; Qamar, S.; Batterham, R.L. Who consumes ultra-processed food? A systematic review of sociodemographic determinants of ultra-processed food consumption from nationally representative samples. Nutr. Res. Rev. 2023, 1–41. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors (Year) Country | Objective | Methods Sample | Intervention | Results | Keys Points |
|---|---|---|---|---|---|
| Alessa et al. [21] 2023 Saudi Arabia | Assess the knowledge of the general population in Saudi Arabia about the relationship between UPF and CRC. | Cross-sectional study N = 802 | Survey on sociodemographic, knowledge of UPF, and consumption rate | The study showed that a significant portion of the subjects ate UPF regularly and only a few were aware of its link with CRC. This highlights the need for greater knowledge of the fundamentals of UPF and its impact on health. | UC |
| Bradbury et al. [22] 2020 United Kingdom | To systematically examine the associations of CRC risk with food and food group intake. | Prospective cohort study N = 475,581 | -FFQ Online dietary assessment 24 h | Consumption of processed and red meat at an average level of 76 g/day, which meets the current UK government recommendation (90 g/day), was associated with an increased risk of CRC. Alcohol was also associated with an increased risk of CRC. | AC |
| Chang et al. [23] 2021 Canada | Investigate the associations between various medical, lifestyle, and dietary factors and the risk of early-onset CRC. | Population-based case-control study N = 782 | -FFQ -Self-administered questionnaire on possible risk factors -Questionnaire on strenuous or moderate physical activities | Modifiable factors, particularly sedentary behaviour and an unhealthy diet, including the consumption of sugary beverages, may be associated with the risk of CRC. | SC, RPM, AC |
| Castelló et al. [24] 2018 Spain | To evaluate whether the associations found between three previously identified dietary patterns with breast, prostate, and gastric cancer are also observed for CRC. | Multicase-control study N = 5138 | -Questionnaire on sociodemographic factors, lifestyle, and medical history -FFQ | No effect of the Prudent pattern on the risk of CRC was observed, but high adherence to the Western diet pattern was associated with an increased risk of CRC for men and women. | RPM |
| Debras et al. [25] 2020 France | To study the associations between total and added sugar intake and cancer risk, taking into account the types and sources of sugar. | Prospective cohort study N = 101,279 | -Repeated and validated 24 h dietary records -Questionnaires on demographic, socioeconomic, and lifestyle characteristics | Sugars can represent a modifiable risk factor for CRC, contributing to the current debate on the implementation of sugar taxes, marketing regulation, and other sugar-related policies. | SC |
| The Kinany et al. [26] 2022 Morocco | Investigate the association between the consumption of foods and beverages of different processing categories and the risk of CRC among Moroccan adults. | Case-control study N = 2906 | -FFQ -NOVA classification | The high consumption of UPF was significantly inverse, while the high consumption of processed foods was significantly positive in the association with the risk of CRC. | SC, RPM, FC, OF |
| The Kinany et al. [27] 2019 Morocco | To investigate the associations between adherence to WCRF/AICR cancer prevention recommendations and CRC risk in Morocco. | Population-based case-control study N = 3302 | -FFQ -Physical activity questionnaire and anthropometric measurements | Compared to those with the lowest compliance score, those in the highest WCRF/AICR score category had a statistically significant reduced risk of CRC. | SC, OF |
| Fiolet et al. [28] 2018 France | To evaluate the possible association between UPF consumption and cancer risk. | Prospective population-based cohort study N = 104,980 | -Repeated 24 h dietary records -NOVA classification | A 10% increase in the proportion of UPF in the diet was associated with a significant increase of more than 10% in the risk of CRC. | SC, RPM |
| Fliss- Isakov et al. [29] 2020 Israel | To examine the association between high UPF intake and colorectal adenomas and to test the interaction with smoking. | Case-control study N = 652 | -Colonoscopy -Interview of sociodemographic factors, lifestyle, and medical history -FFQ | The positive association between UPF intake and adenomas was stronger with advanced adenomas and may reflect a potential role of UPF in the progression of CRC. | UC |
| Hang et al. [30] 2023 United Kingdom | The association between ultra-processed food and the risk of CRC. | Prospective observational cohort study N = 142,052 | -Gastrointestinal endoscopy Biannual lifestyle and medical information questionnaires. -FFQ | Higher UPF consumption is associated with an increased risk of CRC precursors. UPF may be a modifiable goal for the early prevention of CRC. | UC |
| Hur et al. [31] 2021 USA (a) | To study the association between sugary drinks and early-onset CRC. | Prospective cohort study N = 116,429 | -FFQ -4 dietary indices: the main diet quality score and three plant-based dietary indices -Indices; and two mechanism-based indices: the Empirical Dietary and Lifestyle Index for Hyperinsulinemia | Higher intake of SSB in adulthood and adolescence was associated with a higher risk of EO-CRC among women. Reducing SSB consumption among adolescents and young adults may serve as a potential strategy to alleviate the increasing burden of EO-CRC. | SC |
| Jafari et al. [32] 2022 Iran | Determine the association between the consumption of UPF and CRC. | Case-control study N = 213 | -FFQ | High intake of UPF is associated with an increased risk of CRC. Furthermore, among eight UPF categories, consumption of processed meat, fast foods, and non-dairy beverages was significantly higher in those who consumed a higher amount of UPF. | UC |
| Kunnavuttivanich et al. [33] 2020 Thailand | Explore the association between eating patterns and disease recurrence among Thai CRC patients. | Retrospective case-control study N = 225 | -FFQ -GPAQ Version 2 Physical Activity Questionnaire | Among CRC patients with Thai diet lifestyles, there was no association between meat/wheat, fast food/processed fruit, or vegetarian diet patterns and CRC recurrence. | SC, FC |
| Mehrzad et al. [34] 2020 Iran | Investigate the independent and combined effects of some selected risk factors and the Arg399Gln XRCC1 polymorphism on CRC. | Case-control study N = 240 | -Blood sample -FFQ | Gastrointestinal disorders, family history of cancer, BMI, and fast food consumption were significantly higher in cases than in controls. | RPM, AC, FC |
| Metha et al. [35] 2017 USA | To test the hypothesis that the associations of prudent diets and Western diets with the risk of CRC may differ depending on the presence of F nucleatum in tumour tissue. | Prospective cohort study N = 173,229 | -FFQ | Diets rich in whole grains and dietary fibre are associated with a lower risk of F nucleatum-positive CRC, but not F nucleatum-negative cancer, which supports a potential role for the gut microbiota in mediating the association between diet and CRC. | RPM, OF |
| Nguyen et al. [36] 2021 USA | Relate the microbial metabolism of dietary sulphur to the incidence of CRC. | Prospective cohort study N = 59,013 | -Lower endoscopy -FFQ Evaluation of dietary intake during adolescence | The findings support the role of dietary interactions with sulphur-metabolising gut bacteria in early-onset colorectal carcinogenesis, possibly beginning in adolescence. | OF, RPM |
| Romaguera et al. [37] 2021 Spain | To study whether the consumption of UPF and beverages is associated with breast, CRC, and prostate cancer. | Multicentre population-based case-control study N = 7834 | -Multi case–control Spain -FFQ -NEW classification | An association was found between the consumption of UPF and beverages and an increased risk of CRC. | UC, SC |
| Schaberg et al. [38] 2020 USA | Characterisation of demographic and geographic differences in health beliefs and dietary habits related to the risk of CRC in adults in the United States. | Prospective observational study N = 838 | -Survey of 12 questions on the HBM Likert scale -DHQII -MMQ -Demographic and anthropometric information questionnaire | The health beliefs about the risk of coronary heart disease are influenced by the individual’s age and eating habits. Furthermore, regional differences in GLV consumption indicate opportunities for health messages focused on risk reduction. | SC, RPM, OF |
| Seyyedsalehi et al. [39] 2022 Iran | Explore the association between dietary trans fatty acid (TFA) intake and the risk of CRC. | Multicentre case–control study N = 4071 | Personal interviews about lifestyle, dietary intake, education, smoking, opium use, socioeconomic status, physical activity, medical history, and NSAID use | Industrial TFAs, such as semisolid/solid hydrogenated oils, can increase the risk of CRC, especially colon and proximal colon cancer. On the contrary, ruminant TFAs do not appear to be associated with CRC. | UC, FC |
| Tayyem et al. [40] 2017 Jordan | To evaluate possible associations between the consumption of different fast foods and beverages and the risk of CRC in a Jordanian population. | Retrospective case-control study N = 501 | -Sociodemographic questionnaires, diet history, anthropometric measurements, and physical activity metres -FFQ | Consumption of some types of fast food, especially falafel, was associated with an increased risk of developing CRC. An elevated risk for potato chips and corn chips was found. | SC, FC |
| Wang et al. [41] 2021 USA | To develop a dietary score that correlates with intestinal bacteria that metabolise sulphur and examine their association with the risk of CRC. | Prospective cohort study N = 214,797 | -Stool samples from consecutive bowel movements 1 to 3 days apart Questionnaires on sample collection, lifestyle, and food frequency | Adherence to the microbial sulphur diet was associated with an increased risk of CRC, suggesting the potential of using dietary modification as a strategy for reducing risk in CRC. | RPM, OF |
| Xingcun Liu. [42] 2020 China | Analyse the relationship between factors related to dietary and environmental exposure and the incidence of CRC. | Case-control study N = 160 | -Patients with CRC received treatments such as surgery or chemotherapy with XELOX -CPSS of 14 items | The incidence of CRC was closely related to eating habits, environmental exposure, and psychological factors. Unhealthy eating habits, poor living environments, history of smoking and drinking, and excessive psychological pressure will increase the risk of CRC. | FC, AC, OF |
| Yantiss et al. [43] 2021 Canada | To examine associations between sugary drinks and the risk of breast, endometrial, ovarian, and/or CRC among women in the Canadian Diet, Lifestyle, and Health Study. | Cohort studies N = 73,909 | -FFQ -Questionnaire on sociodemographic issues, personal medical history, physical activity, height and weight, and hormone replacement therapy | Relatively high SCB intake was associated with an increased risk of endometrial and ovarian cancer, but not breast or CRC. | SC |
| Zheng et al. [44] 2020 USA | Explore the role of poor dietary quality in the increasing incidence of CRC diagnosed before age 50. | Cohort study prospective. N = 116,430 | -FFQ every 4 years -Self-administered questionnaires on demographics, lifestyle factors, and medical diagnoses every 2 years | Poor diet quality was associated with an increased risk of early onset of high malignant high malignant distal and rectal adenomas. These findings provide preliminary but strong support for the role of diet in early-onset CRC. | SC, RPM, FC, OF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caceres-Matos, R.; Castro-Méndez, A.; Domínguez, M.G.; Pabón-Carrasco, D.; Pabón-Carrasco, M. The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review. Gastrointest. Disord. 2024, 6, 164-179. https://doi.org/10.3390/gidisord6010012
Caceres-Matos R, Castro-Méndez A, Domínguez MG, Pabón-Carrasco D, Pabón-Carrasco M. The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review. Gastrointestinal Disorders. 2024; 6(1):164-179. https://doi.org/10.3390/gidisord6010012
Chicago/Turabian StyleCaceres-Matos, Rocío, Aurora Castro-Méndez, Marina García Domínguez, Daniel Pabón-Carrasco, and Manuel Pabón-Carrasco. 2024. "The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review" Gastrointestinal Disorders 6, no. 1: 164-179. https://doi.org/10.3390/gidisord6010012
APA StyleCaceres-Matos, R., Castro-Méndez, A., Domínguez, M. G., Pabón-Carrasco, D., & Pabón-Carrasco, M. (2024). The Influence of Ultra-Processed Food on Colorectal Cancer: A Systematic Review. Gastrointestinal Disorders, 6(1), 164-179. https://doi.org/10.3390/gidisord6010012