
Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland


Abstract
:1. Introduction
- conducting an empirical assessment of selected elements of quality of life in cities aspiring to be smart;
- focusing the research on non-technological aspects of life in smart cities;
- filling the research gap on the quality of health care in smart cities in the context of an aging population;
- addressing less attractive and more problematic issues related to smart city development;
- embedding research in 16 cities located in developing economies to assess the status of Smart City implementation in less economically developed countries.
2. Literature Overview
2.1. The Concept and Development of Smart Cities
2.2. Quality of Life for All Stakeholders as a Rationale for Creating a Smart City
2.3. Quality of Life for Seniors in the Smart City
- providing health care services;
- monitoring of and informing about the hygiene practices;
- monitoring the condition of patients using IT and ICT technologies;
- health care education.
3. Materials and Methods
3.1. Research Intentions, Data, and Methods
- conduct empirical research in the social area of SC’s functioning, especially in developing economies that have difficulties in implementing smart urban solutions (they allow to confront the recommendations of theory with practice and formulate improvement recommendations);
- pay more attention to health care as a key determinant of quality of life;
- identify the level of adaptation of cities to the needs of residents at risk of economic and social exclusion, i.e., seniors.
- Assessment of the demographic situation of the surveyed cities.
- Analysis of the level of health care in the surveyed cities.
- Comparison of the results of the demographic assessment with the results of the analysis of the level of health care in the surveyed cities.
- (a)
- the ratio of the population in the post-working age to the population in the working age (Rpw/w) (in Poland, the working age for women is from 18 to 59 and for men from 18 to 64):
- (b)
- the community’s elderly burden factor (EBF):
- (c)
- the percentage of people aged 65 and older in the total population (P%65+):
- (a)
- the number of physicians per 10,000 residents (Rph):
- (b)
- the number of nurses per 10,000 residents (Rn):
- (c)
- the number of hospital beds per 10,000 residents (Rhb):
3.2. Research Sample Characteristics
4. Results
4.1. Seniors in Polish Cities in Demographic Terms
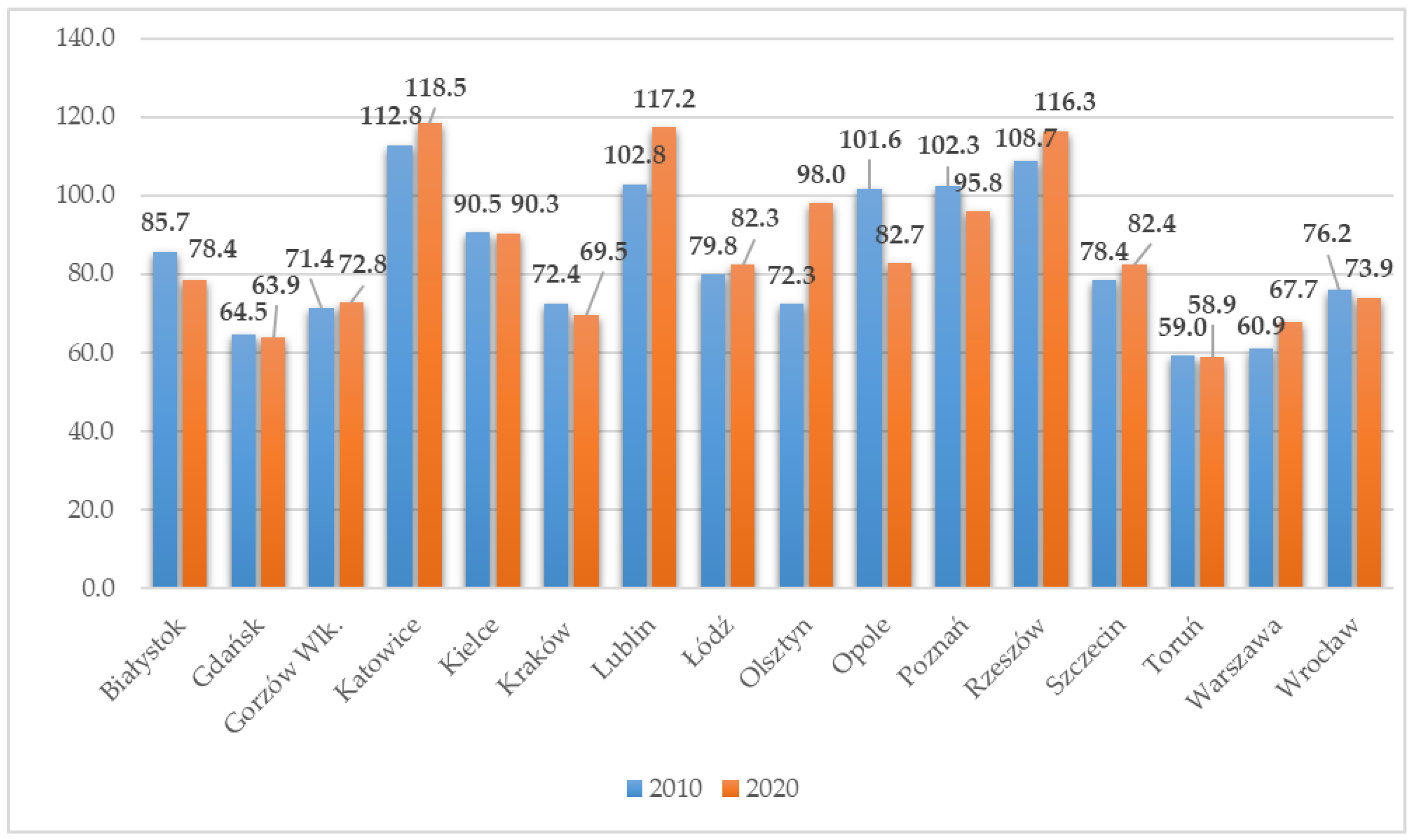
4.2. Health Care in the Context of Aging Urban Communities
5. Discussion
6. Conclusions
- monitor the aging process of urban communities and take measures to reduce its pace and effects;
- adjust the level of health care to demographic processes well in advance, including, above all, increase the number of nurses and reduce the rate of decline in hospital beds;
- identify the needs and expectations of seniors so that they can become full members of urban communities and have the desired quality of life;
- plan organizational and infrastructural social solutions aimed at providing long-term health care for a steadily growing group of seniors.
- assessing the current and prospective quality of life of seniors in smart cities from the perspective of adverse demographic processes and health care;
- filling the research gap on problematic aspects of quality of life in cities;
- addressing the issue of social exclusion of seniors in smart cities;
- identifying the scale and scope of aging of urban communities in Polish entities considered smart or aspiring to the title of smart cities;
- diagnosing the quality of health care in cities considered smart in the context of demographic conditions;
- assessing the effectiveness of measures to adapt health care to the increasing aging of urban communities.
Funding
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.; Jiang, T.; Sun, J.; Fu, Z.; Yu, Y. Sustainable Development of Urbanization: From the Perspective of Social Security and Social Attitude for Migration. Sustainability 2022, 14, 10777. [Google Scholar] [CrossRef]
- Zhang, Q.; Cai, X.; Liu, X.; Yang, X.; Wang, Z. The Influence of Urbanization to the Outer Boundary Ecological Environment Using Remote Sensing and GIS Techniques—A Case of the Greater Bay Area. Land 2022, 11, 1426. [Google Scholar] [CrossRef]
- Przybyłowski, A.; Kałaska, A.; Przybyłowski, P. Quest for a Tool Measuring Urban Quality of Life: ISO 37120 Standard Sustainable Development Indicators. Energies 2022, 15, 2841. [Google Scholar] [CrossRef]
- Dashkevych, O.; Portnov, B.A. Criteria for Smart City Identification: A Systematic Literature Review. Sustainability 2022, 14, 4448. [Google Scholar] [CrossRef]
- Ligarski, M.J.; Wolny, M. Quality of Life Surveys as a Method of Obtaining Data for Sustainable City Development—Results of Empirical Research. Energies 2021, 14, 7592. [Google Scholar] [CrossRef]
- Helbing, D.; Fanitabasi, F.; Giannotti, F.; Hänggli, R.; Hausladen, C.I.; van den Hoven, J.; Mahajan, S.; Pedreschi, D.; Pournaras, E. Ethics of Smart Cities: Towards Value-Sensitive Design and Co-Evolving City Life. Sustainability 2021, 13, 11162. [Google Scholar] [CrossRef]
- Trzpiot, G.; Szołtysek, J. Safety of the Elderly in Smart City. Res. Pap. Wrocław Univ. Econ. 2017, 483, 210–226. [Google Scholar] [CrossRef]
- Tomczyk, Ł.; Klimczuk, A. Inteligentne Miasta Przyjazne Starzeniu—Przykłady z Krajów Grupy Wyszehradzkiej (Smart, Age-Friendly Cities: Examples in the Countries of the Visegrad Group (V4)). Rozw. Reg. Polityka Reg. 2016, 34, 79–97. [Google Scholar]
- Podgórniak-Krzykacz, A.; Przywojska, J.; Wiktorowicz, J. Smart and age-friendly communities in Poland. An analysis of institutional and individual conditions for a new concept of smart development of ageing communities. Energies 2020, 13, 2268. [Google Scholar] [CrossRef]
- Zaman, A.; Thornton, K. Prioritization of local indicators for the development of an age-friendly city: A community perspective. Urban Sci. 2018, 2, 51. [Google Scholar] [CrossRef]
- Morozova, I.A.; Yatsechko, S.S. The Risks of Smart Cities and the Perspectives of Their Management Based on Corporate Social Responsibility in the Interests of Sustainable Development. Risks 2022, 10, 34. [Google Scholar] [CrossRef]
- Schiavo, F.T.; Magalhães, C.F.d. Smart Sustainable Cities: The Essentials for Managers’ and Leaders’ Initiatives within the Complex Context of Differing Definitions and Assessments. Smart Cities 2022, 5, 50. [Google Scholar] [CrossRef]
- Lu, M.-T.; Lu, H.-P.; Chen, C.-S. Exploring the Key Priority Development Projects of Smart Transportation for Sustainability: Using Kano Model. Sustainability 2022, 14, 9319. [Google Scholar] [CrossRef]
- Alshuwaikhat, H.M.; Adenle, Y.A.; Almuhaidib, T. A Lifecycle-Based Smart Sustainable City Strategic Framework for Realizing Smart and Sustainability Initiatives in Riyadh City. Sustainability 2022, 14, 8240. [Google Scholar] [CrossRef]
- Mazhar Rathore, M.; Awais, A.; Anand, P.; Seungmin, R. Urban planning and building smart cities based on the Internet of Things using Big Data analytics. Comput. Netw. 2016, 101, 63–80. [Google Scholar] [CrossRef]
- Adonina, A.; Akhmedova, E.; Kandalova, A. Realization of smart city concept through media technology in architecture and urban space: From utopia to reality. MATEC Web Conf. 2018, 170, 02013. [Google Scholar] [CrossRef]
- Elmaghraby, A.S.; Losavio, M.M. Cyber security challenges in Smart Cities: Safety, security and privacy. J. Adv. Res. 2014, 5, 491–497. [Google Scholar] [CrossRef]
- Manika, S. Mechanisms for innovative-driven solutions in European smart cities. Smart Cities 2020, 3, 527–540. [Google Scholar] [CrossRef]
- Mahmood, O.A.; Abdellah, A.R.; Muthanna, A.; Koucheryavy, A. Distributed Edge Computing for Resource Allocation in Smart Cities Based on the IoT. Information 2022, 13, 328. [Google Scholar] [CrossRef]
- Ullah, I.; Kim, J.-B.; Han, Y.-H. Compound Context-Aware Bayesian Inference Scheme for Smart IoT Environment. Sensors 2022, 22, 3022. [Google Scholar] [CrossRef]
- Pawłowska, B. Intelligent transport as a key component of implementation the sustainable development concept in smart cities. Transp. Econ. Logist. 2018, 9, 7–23. [Google Scholar] [CrossRef]
- Wawer, M.; Grzesiuk, K.; Jegorow, D. Smart Mobility in a Smart City in the Context of Generation Z Sustainability, Use of ICT, and Participation. Energies 2022, 15, 4651. [Google Scholar] [CrossRef]
- Dohn, K.; Kramarz, M.; Przybylska, E. Interaction with City Logistics Stakeholders as a Factor of the Development of Polish Cities on the Way to Becoming Smart Cities. Energies 2022, 15, 4103. [Google Scholar] [CrossRef]
- Bielińska-Dusza, E.; Hamerska, M.; Żak, A. Sustainable Mobility and the Smart City: A Vision of the City of the Future: The Case Study of Cracow (Poland). Energies 2021, 14, 7936. [Google Scholar] [CrossRef]
- Tymkiewicz, J. The Role of an Architect in Creating the Image of an Elderly-Friendly Sustainable Smart City. Buildings 2019, 9, 223. [Google Scholar] [CrossRef]
- Saaty, T.L.; De Paola, P. Rethinking Design and Urban Planning for the Cities of the Future. Buildings 2017, 7, 76. [Google Scholar] [CrossRef]
- Keriwala, N.; Patel, A. Innovative Roadmap for Smart Water Cities: A Global Perspective. Mater. Proc. 2022, 10, 1. [Google Scholar] [CrossRef]
- Yang, H.; Ruan, Z.; Li, W.; Zhu, H.; Zhao, J.; Peng, J. The Impact of Built Environment Factors on Elderly People’s Mobility Characteristics by Metro System Considering Spatial Heterogeneity. ISPRS Int. J. Geo-Inf. 2022, 11, 315. [Google Scholar] [CrossRef]
- Jong, M.; Joss, S.; Schraven, D.; Zhan, C.; Weijnen, M. Sustainable–smart–resilient–low carbon–eco–knowledge cities: Making sense of a multitude of concepts promoting sustainable urbanization. J. Clean. Prod. 2015, 109, 25–38. [Google Scholar] [CrossRef]
- Sabory, N.R.; Senjyu, T.; Danish, M.S.S.; Hosham, A.; Noorzada, A.; Amiri, A.S.; Muhammdi, Z. Applicable Smart City Strategies to Ensure Energy Efficiency and Renewable Energy Integration in Poor Cities: Kabul Case Study. Sustainability 2021, 13, 11984. [Google Scholar] [CrossRef]
- Monfaredzadeha, T.; Krueger, R. Investigating Social Factors of Sustainability in a Smart City. Procedia Eng. 2015, 118, 1112–1118. [Google Scholar] [CrossRef] [Green Version]
- Enserink, B.; Koppenjan, J. Public participation in China: Sustainable urbanization and governance. Manag. Environ. Qual. Int. J. 2007, 18, 459–474. [Google Scholar] [CrossRef]
- Gao, Z.; Wang, S.; Gu, J. Public Participation in Smart-City Governance: A Qualitative Content Analysis of Public Comments in Urban China. Sustainability 2020, 12, 8605. [Google Scholar] [CrossRef]
- Pløger, J. Public participation and the art of governance. Environ. Plan. B Plan. Des. 2001, 28, 219–241. [Google Scholar] [CrossRef]
- Kim, S.-C.; Hong, P.; Lee, T.; Lee, A.; Park, S.-H. Determining Strategic Priorities for Smart City Development: Case Studies of South Korean and International Smart Cities. Sustainability 2022, 14, 10001. [Google Scholar] [CrossRef]
- Parra-Domínguez, J.; López-Blanco, R.; Pinto-Santos, F. Approach to the Technical Processes of Incorporating Sustainability Information—The Case of a Smart City and the Monitoring of the Sustainable Development Goals. Processes 2022, 10, 1651. [Google Scholar] [CrossRef]
- Angelidou, M. Smart city policies: A spatial approach. Cities 2014, 41, S3–S11. [Google Scholar] [CrossRef]
- Mesquitela, J.; Elvas, L.B.; Ferreira, J.C.; Nunes, L. Data Analytics Process over Road Accidents Data—A Case Study of Lisbon City. ISPRS Int. J. Geo-Inf. 2022, 11, 143. [Google Scholar] [CrossRef]
- Zheng, Ch.; Yuan, J.; Zhu, L.; Zhang, Y.; Shao, Q. From digital to sustainable: A scientometric review of smart city literature between 1990 and 2019. J. Clean. Prod. 2020, 258, 120689. [Google Scholar] [CrossRef]
- Lim, Y.; Edelenbos, J.; Gianoli, A. Identifying the results of smart city development: Findings from systematic literature review. Cities 2019, 95, 102397. [Google Scholar] [CrossRef]
- Chica-Olmo, J.; Sánchez, A.; Sepúlveda-Murillo, F.H. Assessing Colombia’s policy of socio-economic stratification: An intra-city study of self-reported quality of life. Cities 2020, 97, 102560. [Google Scholar] [CrossRef]
- Kaklauskas, A.; Zavadskas, E.K.; Radzeviciene, I.; Ubarte, A.; Podviezko, V.; Podvezko, A.; Kuzminske, A.; Banaitis, A.; Binkyte, A.; Bucinskas, V. Quality of city life multiple criteria analysis. Cities 2018, 72 Pt A, 82–93. [Google Scholar] [CrossRef]
- Lom, M.; Pribyl, O. Smart city model based on systems theory. Int. J. Inf. Manag. 2020, 56, 102092. [Google Scholar] [CrossRef]
- Chen, Y.; Ardila-Gomez, A.; Frame, G. Achieving energy savings by intelligent transportation systems investments in the context of smart cities. Transp. Res. Part D Transp. Environ. 2017, 54, 381–396. [Google Scholar] [CrossRef]
- McNeill, D. Global Firms and Smart Technologies: IBM and the Reduction of Cities. Trans. Inst. Br. Geogr. 2015, 40, 562–574. [Google Scholar] [CrossRef]
- Moser, S. New Cities: Old Wine in New Bottles? Dialogues Hum. Geogr. 2015, 5, 31–35. [Google Scholar] [CrossRef]
- Yigitcanlar, T.; Han, H.; Kamruzzaman, Md.; Ioppolo, G.; Sabatini-Marques, J. The making of smart cities: Are Songdo, Masdar, Amsterdam, San Francisco and Brisbane the best we could build? Land Use Policy 2019, 88, 104187. [Google Scholar] [CrossRef]
- Šurdonja, S.; Giuffrè, T.; Deluka-Tibljaš, A. Smart mobility solutions—Necessary precondition for a well-functioning smart city. Transp. Res. Procedia 2020, 45, 604–611. [Google Scholar] [CrossRef]
- Kummitha, R.K.R. Entrepreneurial urbanism and technological panacea: Why Smart City planning needs to go beyond corporate visioning? Technol. Forecast. Soc. Change 2018, 137, 330–339. [Google Scholar] [CrossRef]
- Chamoso, P.; González-Briones, A.; De La Prieta, F.; Venyagamoorthy, G.K.; Corchado, J.M. Smart city as a distributed platform: Toward a system for citizen-oriented management. Comput. Commun. 2020, 15215, 323–332. [Google Scholar] [CrossRef]
- Moustaka, V.; Theodosiou, Z.; Vakali, A.; Kounoudes, A.; Anthopoulos, L.G. Εnhancing social networking in smart cities: Privacy and security borderlines. Technol. Forecast. Soc. Change 2019, 142, 285–300. [Google Scholar] [CrossRef]
- Simonofski, A.; Vallé, T.; Serral, E.; Wautelet, Y. Investigating context factors in citizen participation strategies: A comparative analysis of Swedish and Belgian smart cities. Int. J. Inf. Manag. 2019, 56, 102011. [Google Scholar] [CrossRef]
- Martin, C.J.; Evans, J.; Karvonen, A. Smart and sustainable? Five tensions in the visions and practices of the smart-sustainable city in Europe and North America. Technol. Forecast. Soc. Change 2018, 133, 269–278. [Google Scholar] [CrossRef]
- Marchetti, D.; Oliveira, R.; Figueira, A.R. Are global north smart city models capable to assess Latin American cities? A model and indicators for a new context. Cities 2019, 92, 197–207. [Google Scholar] [CrossRef]
- Kummitha, R.K.R.; Crutzen, N. Smart cities and the citizen-driven internet of things: A qualitative inquiry into an emerging smart city. Technol. Forecast. Soc. Change 2019, 140, 44–53. [Google Scholar] [CrossRef]
- Fu, S. Smart Café Cities: Testing human capital externalities in the Boston metropolitan area. J. Urban Econ. 2007, 61, 86–111. [Google Scholar] [CrossRef]
- Kitchin, R. The Real-Time City? Big Data and Smart Urbanism. Geojournal 2014, 79, 1–14. [Google Scholar] [CrossRef]
- Kitchin, R. Making Sense of Smart Cities: Addressing Present Shortcomings. Camb. J. Reg. Econ. Soc. 2015, 8, 131–136. [Google Scholar] [CrossRef]
- Camero, A.; Alba, E. Smart city and information technology: A review. Cities 2019, 93, 84–94. [Google Scholar] [CrossRef]
- Arribas-Bela, D.; Kourtit, K.; Nijkamp, P. Benchmarking of world cities through Self-Organizing Maps. Cities 2013, 31, 248–257. [Google Scholar] [CrossRef]
- Mourshed, M.; Bucchiarone, A.; Khandokar, F. SMART: A Process-Oriented Methodology for Resilient Smart Cities. In Proceedings of the IEEE International Smart Cities Conference (ISC2), Trento, Italy, 12–15 September 2016; pp. 1–6. [Google Scholar]
- Ismagilova, E.; Hughes, L.; Dwivedi, Y.; Raman, K. Smart cities: Advances in research: An information systems perspective. Int. J. Inf. Manag. 2019, 47, 88–100. [Google Scholar] [CrossRef]
- Etzkowitz, H. The Triple Helix: University–Industry–Government Innovation in Action; Taylor & Francis: New York, NY, USA, 2008. [Google Scholar]
- Borkowska, K.; Osborne, M. Locating the fourth helix: Rethinking the role of civil society in developing smart learning cities. Int. Rev. Educ. 2018, 64, 355–372. [Google Scholar] [CrossRef]
- Grundel, I.; Dahlström, M. A quadruple and quintuple helix approach to regional innovation systems in the transformation to a forestry-based bioeconomy. J. Knowl. Econ. 2016, 7, 963–983. [Google Scholar] [CrossRef]
- Jensen, C.; Trägårdh, B. Narrating the Triple Helix concept in “weak” regions: Lessons from Sweden. Int. J. Technol. Manag. 2004, 27, 513–530. [Google Scholar] [CrossRef]
- Macke, J.; Casagrande, R.M.; Sarate, J.A.R.; Silva, K.A. Smart city and quality of life: Citizens’ perception in a Brazilian case study. J. Clean. Prod. 2018, 182, 717–726. [Google Scholar] [CrossRef]
- Ahvenniemi, H.; Houvila, A.; Pinto-Seppä, I.; Airaksinen, M. What are the differences between sustainable and smart cities? Cities 2017, 60, 234–245. [Google Scholar] [CrossRef]
- Sugandha; Freestone, R.; Favaro, P. The social sustainability of smart cities: A conceptual framework. City Cult. Soc. 2022, 29, 100460. [Google Scholar] [CrossRef]
- Aurigi, A.; Odendaal, N. From “smart in the Box” to “smart in the city”: Rethinking the socially sustainable smart city in context. J. Urban Technol. 2020, 28, 55–70. [Google Scholar] [CrossRef]
- Cohen, A.K.; Schuchter, J.W. Revitalizing communities together: The shared values, goals, and work of education, urban planning, and public health. J. Urban Health 2013, 90, 187–196. [Google Scholar] [CrossRef]
- Van Brussel, S.; Huyse, H. Citizen science on speed? Realising the triple objective of scientific rigour, policy influence and deep citizen engagement in a large-scale citizen science project on ambient air quality in Antwerp. J. Environ. Plan. Manag. 2019, 62, 534–551. [Google Scholar] [CrossRef]
- Corsini, F.; Certomà, C.; Dyer, M.; Frey, M. Participatory energy: Research, imaginaries and practices on people’ contribute to energy systems in the smart city. Technol. Soc. Change 2019, 142, 322–332. [Google Scholar] [CrossRef]
- Nakano, S.; Washizu, A. Will smart cities enhance the social capital of residents? The importance of smart neighborhood management. Cities 2021, 115, 103244. [Google Scholar] [CrossRef]
- Zhu, Y.-Q.; Alamsyah, N. Citizen empowerment and satisfaction with smart city app: Findings from Jakarta. Technol. Forecast. Soc. Change 2022, 174, 121304. [Google Scholar] [CrossRef]
- Yeh, H. The effects of successful ICT-based smart city services: From citizens’ perspectives. Gov. Inf. Q. 2017, 34, 556–565. [Google Scholar] [CrossRef]
- Kopackova, H.; Komarkova, J. Participatory technologies in smart cities: What citizens want and how to ask them. Telemat. Inform. 2020, 47, 101325. [Google Scholar] [CrossRef]
- Marimuthu, M.; D’Souza, C.; Shukla, Y. Integrating community value into the adoption framework: A systematic review of conceptual research on participatory smart city applications. Technol. Forecast. Soc. Change 2022, 181, 121779. [Google Scholar] [CrossRef]
- Bifulco, F.; Tregua, M.; Amitrano, C.C. Co-governing smart cities through living labs. Top evidences from EU. Transylv. Rev. Adm. Sci. 2017, 50E, 21–37. [Google Scholar] [CrossRef]
- Santonen, T.; Creazzo, L.; Griffon, A.; Bódi, Z.; Aversano, P. Cities as Living Labs-Increasing the Impact of Investment in the Circular Economy for Sustainable Cities. 2017. Available online: https://ec.europa.eu/info/sites/default/files/research_and_innovation/groups/rise/cities_as_living_labs.pdf (accessed on 29 August 2022).
- Nguyen, H.T.; Marques, P.; Benneworth, P. Living labs: Challenging and changing the smart city power relations? Technol. Forecast. Soc. Change 2022, 183, 121866. [Google Scholar] [CrossRef]
- Reypens, C.; Lievens, A.; Blazevic, V. Hybrid Orchestration in Multi-stakeholder Innovation Networks: Practices of mobilizing multiple, diverse stakeholders across organizational boundaries. Organ. Stud. 2019, 42, 61–83. [Google Scholar] [CrossRef]
- Miller, K.; Mcadam, R.; Moffett, S.; Alexander, A.; Puthusserry, P. Knowledge transfer in university quadruple helix ecosystems: An absorptive capacity perspective. RD Manag. 2016, 46, 383–399. [Google Scholar] [CrossRef]
- Andrews, R.; Beynon, M.J.; McDermott, A.M. Organizational capability in the public sector: A configurational approach. J. Public Adm. Res. Theory 2016, 26, 239–258. [Google Scholar] [CrossRef]
- Botequilha-Leitão, A.; Díaz-Varela, E.R. Performance based planning of complex urban social-ecological systems: The quest for sustainability through the promotion of resilience. Sustain. Cities Soc. 2020, 56, 102089. [Google Scholar] [CrossRef]
- Mora, L.; Deakin, M.; Reid, A. Strategic principles for smart city development: A multiple case study analysis of European best practices. Technol. Forecast. Soc. Change 2019, 142, 70–97. [Google Scholar] [CrossRef]
- Clement, J.; Manjonb, M.; Crutzen, N. Factors for collaboration amongst smart city stakeholders: A local government perspective. Gov. Inf. Q. 2022, 101746, in press. [Google Scholar] [CrossRef]
- Anand, P.B.; Navío-Marco, J. Governance and economics of smart cities: Opportunities and challenges. Telecommun. Policy 2018, 42, 795–799. [Google Scholar] [CrossRef]
- Vanolo, A. Is there anybody out there? The place and role of citizens in tomorrow’s smart cities. Futures 2016, 82, 26–36. [Google Scholar] [CrossRef]
- Joss, S.; Cook, M.; Dayot, Y. Smart cities: Towards a new citizenship regime? A discourse analysis of the British Smart City standard. J. Urban Technol. 2017, 24, 29–49. [Google Scholar] [CrossRef]
- Shelton, T.; Zook, M.; Wiig, A. The ‘actually existing smart city’. Camb. J. Reg. Econ. Soc. 2015, 8, 13–25. [Google Scholar] [CrossRef]
- Engelbert, J.; van Zoonenb, L.; Hirzalla, F. Excluding citizens from the European smart city: The discourse practices of pursuing and granting smartness. Technol. Forecast. Soc. Change 2019, 142, 347–353. [Google Scholar] [CrossRef]
- Ji, T.; Chen, J.-Ch.; Wei, H.-H.; Su, Y.-Ch. Towards people-centric smart city development: Investigating the citizens’ preferences and perceptions about smart-city services in Taiwan. Sustain. Cities Soc. 2021, 67, 102691. [Google Scholar] [CrossRef]
- Shami, R.M.; Rad, V.B.; Moinifar, M. The structural model of indicators for evaluating the quality of urban smart living. Technol. Forecast. Soc. Change 2022, 176, 121427. [Google Scholar] [CrossRef]
- Obringer, R.; Nateghi, R. What makes a city ‘smart’ in the Anthropocene? A critical review of smart cities under climate change. Sustain. Cities Soc. 2021, 75, 103278. [Google Scholar] [CrossRef]
- Basu, I. Elite discourse coalitions and the governance of ‘smart spaces’: Politics, power and privilege in India’s Smart Cities Mission. Political Geogr. 2019, 68, 77–85. [Google Scholar] [CrossRef]
- Bunders, D.J.; Varró, K. Problematizing data-driven urban practices: Insights from five Dutch ‘smart cities’. Cities 2019, 93, 145–152. [Google Scholar] [CrossRef]
- Grossi, G.; Pianezzi, D. Smart cities: Utopia or neoliberal ideology? Cities 2017, 69, 79–85. [Google Scholar] [CrossRef]
- Jonek-Kowalska, I.; Wolniak, R. Economic opportunities for creating smart cities in Poland. Does wealth matter? Cities 2021, 114, 103222. [Google Scholar] [CrossRef]
- Málovics, G.; Cretan, R.; Méreiné, B.B.; Tóth, J. Urban Roma, segregation and place attachment in Szeged, Hungary. Area 2019, 51, 72–83. [Google Scholar] [CrossRef]
- Su, S.; Pi, J.; Xie, H.; Cai, Z.; Weng, M. Community deprivation, walkability, and public health: Highlighting the social inequalities in land use planning for health promotion. Land Use Policy 2017, 67, 315–326. [Google Scholar] [CrossRef]
- Su, S.; Zhou, H.; Xu, M.; Ru, H.; Wang, W.; Weng, M. Auditing street walkability and associated social inequalities for planning implications. J. Transp. Geogr. 2017, 74, 62–76. [Google Scholar] [CrossRef]
- Hatuka, T.; Zur, H. From smart cities to smart social urbanism: A framework for shaping the socio-technological ecosystems in cities. Telemat. Inform. 2020, 55, 101430. [Google Scholar] [CrossRef]
- Wang, C.; Steinfeld, E.; Maisel, J.; Kang, B. Is your smart city inclusive? Evaluating proposals from the U.S. Department of Transportation’s Smart City Challenge. Sustain. Cities Soc. 2021, 74, 103148. [Google Scholar] [CrossRef]
- Ivan, L.; Beu, D.; van Hoof, J. Smart and Age-Friendly Cities in Romania: An Overview of Public Policy and Practice. Int. J. Environ. Res. Public Health 2020, 17, 5202. [Google Scholar] [CrossRef]
- Antwi-Afari, P.; Owusu-Manu, D.-G.; Ng, S.T.; Asumadu, G. Modeling the smartness or smart development levels of developing countries’ cities. J. Urban Manag. 2021, 10, 369–381. [Google Scholar] [CrossRef]
- Loos, E.; Sourbati, M.; Behrendt, F. The Role of Mobility Digital Ecosystems for Age-Friendly Urban Public Transport: A Narrative Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 7465. [Google Scholar] [CrossRef]
- Ghani, F.; Rachele, J.N.; Washington, S.; Turrell, G. Gender and age differences in walking for transport and recreation: Are the relationships the same in all neighborhoods? Prev. Med. Rep. 2016, 4, 75–80. [Google Scholar] [CrossRef]
- Liu, J.; Liu, L.; Pei, M. Analysis of older people’s walking behavioral intention with the extended theory of planned behavior. J. Transp. Health 2022, 26, 101462. [Google Scholar] [CrossRef]
- Mertens, L.; Van Dyck, D.; Deforche, B.; De Bourdeaudhuij, I.; Brondeel, R.; Van Cauwenberg, J. Individual, social, and physical environmental factors related to changes in walking and cycling for transport among older adults: A longitudinal study. Health Place 2019, 55, 120–127. [Google Scholar] [CrossRef]
- Murray, L. Age-friendly mobilities: A transdisciplinary and intergenerational perspective. J. Transp. Health 2015, 2, 302–307. [Google Scholar] [CrossRef]
- Shi, Z.; Pun-Cheng, L.S.C.; Liu, X.; Lai, J.; Tong, C.; Zhang, A.; Zhang, M.; Shi, W. Analysis of the Temporal Characteristics of the Elderly Traveling by Bus Using Smart Card Data. ISPRS Int. J. Geo-Inf. 2020, 9, 751. [Google Scholar] [CrossRef]
- Howell, A. Resilience as enhancement: Governmentality and political economy beyond ‘responsibilisation’. Politics 2016, 35, 67–71. [Google Scholar] [CrossRef]
- Alam, M.M.; Malik, H.; Khan, M.I.; Pardy, T.; Kuusik, A.; Le Moullec, Y. A survey on the roles of communication technologies in iot-based personalized healthcare applications. IEEE Access 2018, 6, 36611–36631. [Google Scholar] [CrossRef]
- Baali, H.; Djelouat, H.; Amira, A.; Bensaali, F. Empowering technology enabled care using iot and smart devices: A review. IEEE Sens. J. 2017, 18, 1790–1809. [Google Scholar] [CrossRef]
- Gavrilovic, N.; Mishra, A. Software architecture of the internet of things (IoT) for smart city, healthcare and agriculture: Analysis and improvement directions. J. Ambient Intell. Humaniz. Comput. 2021, 12, 1315–1336. [Google Scholar] [CrossRef]
- Oueida, S.; Aloqaily, M.; Ionescu, S. A smart healthcare reward model for resource allocation in smart city. Multimed. Tools Appl. 2019, 78, 24573–24594. [Google Scholar] [CrossRef]
- Vamsi, B.; Doppala, B.P.; Rao, N.T.; Bhattacharyya, D. Comparative analysis of prevalent disease by preprocessing techniques using big data and machine learning: An extensive review. Mach. Intell. Soft Comput. 2021, 1280, 27–38. [Google Scholar]
- Javed, A.R.; Fahad, L.G.; Farhan, A.A.; Abbas, S.; Srivastava, G.; Parizi, R.M.; Khan, M.S. Automated cognitive health assessment in smart homes using machine learning. Sustain. Cities Soc. 2021, 65, 102572. [Google Scholar] [CrossRef]
- Manogaran, G.; Varatharajan, R.; Lopez, D.; Kumar, P.M.; Sundarasekar, R.; Thota, C. A new architecture of internet of things and big data ecosystem for secured smart healthcare monitoring and alerting system. Future Gener. Comput. Syst. 2018, 82, 375–387. [Google Scholar] [CrossRef]
- Xu, B.; Li, L.; Hu, D.; Wu, B.; Ye, C.; Cai, H. Healthcare data analysis system for regional medical union in smart city. J. Manag. Anal. 2018, 5, 334–349. [Google Scholar] [CrossRef]
- Chi, W.-C.; Cheng, W.-C.; Chen, T.-H.; Lin, P.-J. Impact of Using the Intelligent Physical Health Measurement System on Active Aging: A Survey in Taiwan. Healthcare 2021, 9, 1142. [Google Scholar] [CrossRef]
- Rocha, N.; Dias, A.; Santinha, G.; Rodrigues, M.; Queirós, A.; Rodrigues, C. A Systematic Review of Smart Cities’ Applications to Support Active Ageing. Procedia Comput. Sci. 2019, 160, 306–313. [Google Scholar] [CrossRef]
- Plouffe, L.; Kalache, A. Towards Global Age-Friendly Cities: Determining Urban Features that Promote Active Aging. J. Urb. Health 2010, 87, 733–739. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The challenges of urban ageing: Making cities age-friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar]
- Zaineb, L.; Lemlouma, T.; Roose, P.; Weis, F.; Messaoud, H. A genetic-based localization algorithm for elderly people in smart cities. In Proceedings of the 14th ACM International Symposium on Mobility Management and Wireless Access (MobiWac ’16), Malta, 13–17 November 2016. [Google Scholar]
- Fan, C. Construction and Value Study of IT-based Smart Senior Citizens’ Communities. In Proceedings of the Sixth International Conference on Measuring Technology and Mechatronics Automation (ICMTMA), Zhangjiajie, China, 10–11 January 2014. [Google Scholar]
- Nicola, B.; Spencer, N.; King, A.; Crooks, P.; Deakin, J.; Young, S. IoT and smart city services to support independence and wellbeing of older people. In Proceedings of the 25th International Conference on Software, Telecommunications and Computer Networks (SoftCOM), Split, Croatia, 21–23 September 2017. [Google Scholar]
- Zschippig, C.; Kluss, T. Gardening in ambient assisted living. Urban For. Urban Green. 2016, 15, 186–189. [Google Scholar] [CrossRef]
- López-de-Ipiña, D.; Klein, B.; Vanhecke, S.; Perez-Velasco, J. Towards ambient assisted cities and citizens. In Proceedings of the 27th International Conference on Advanced Information Networking and Applications Workshops, Barcelona, Spain, 25–28 March 2013. [Google Scholar]
- Kötteritzsch, A.; Koch, M.; Wallrafen, S. Expand your comfort zone! Smart urban objects to promote safety in public spaces for older adults. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Adjunct, Heidelberg, Germany, 12–16 September 2016. [Google Scholar]
- Trencher, G.; Karvonen, A. Stretching “smart”: Advancing health and well-being through the smart city agenda. Local Environ. 2017, 24, 610–627. [Google Scholar] [CrossRef]
- Casino, F.; Borràs, F.; Martínez-Balleste, A. Healthy routes in the smart city: A context-aware mobile recommender. IEEE Softw. 2017, 34, 42–47. [Google Scholar] [CrossRef]
- Stibe, A.; Larson, K. Persuasive cities for sustainable wellbeing: Quantified communities. In Mobile Web and Intelligent Information Systems, Proceedings of the 13th International Conference, MobiWIS 2016, Vienna, Austria, 22–24 August 2016; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Righi, V.; Sayago, S.; Blat, J. Urban ageing: Technology, agency and community in smarter cities for older people. In Proceedings of the 7th International Conference on Communities and Technologies, Limerick, Ireland, 27–30 June 2015. [Google Scholar]
- Gomes, C.A.; Araújo, L.; Figueiredo, M.; Morais, N.; Pereira, J.; Rito, P.; Ferreira, S.; Gouveia, T. VIAS | Viseu InterAge stories: Developing an app to foster social inclusion and healthy lifestyles. In Proceedings of the 2017 International Symposium on Computers in Education (SIIE), Lisbon, Portugal, 9–11 November 2017. [Google Scholar]
- Liczba Lekarzy i Pielęgniarek na Tysiąc Mieszkańców w Państwach Europy. Polska na Szarym Końcu w Rankingu Pielęgniarek per Capita. Available online: https://www.euractiv.pl/section/bezpieczenstwo-i-obrona/news/liczba-lekarzy-i-pielegniarek-na-tysiac-mieszkancow-w-panstwach-europy-polska-na-szarym-koncu-w-rankingu-pielegniarek-per-capita/ (accessed on 30 August 2022).
- Masik, G.; Sagan, I.; Scott, J.W. Smart City strategies and new urban development policies in the Polish context. Cities 2021, 108, 102970. [Google Scholar] [CrossRef]
- Sikora-Fernandez, D. Smarter cities in a post-socialist country: Example of Poland. Cities 2018, 78, 52–59. [Google Scholar] [CrossRef]
- Sikora-Fernandez, D.; Stawasz, D. The concept of Smart City in the theory and practice of development management. Rom. J. Reg. Sci. 2016, 10, 81–99. [Google Scholar]
- Masik, G.; Gajewski, A. Working towards urban capacity and resilience strategy implementation: Adaptation plans and strategies in Polish cities. Cities 2021, 119, 103381. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City | Inhabitants | Surface | Industry |
|---|---|---|---|
| Białystok | 296,000 | 102 km2 | Electro-mechanical (electronics, machinery and metal), wood, clothing, food, and printing industries |
| Gorzów Wlk. | |||
| Gdańsk | 471,000 | 263 km2 | Shipbuilding, petrochemicals, energy, apparel, metals |
| Katowice | 292,000 | 165 km2 | Mining, business services, automotive |
| Kielce | |||
| Kraków | 782,000 | 327 km2 | Tourism, business services, trade, banking services |
| Lublin | 338,000 | 147 km2 | Energy, chemical, food, tobacco |
| Łódź | |||
| Olsztyn | |||
| Opole | |||
| Poznań | 532,000 | 262 km2 | Electromechanical, chemical, commercial, transportation |
| Rzeszów | |||
| Szczecin | |||
| Toruń | |||
| Warsaw | 517,000 | 517 km2 | Electrical engineering, transportation equipment, chemical, food, printing |
| Wrocław | 643,000 | 293 km2 | Machinery, transportation equipment, food, electro-technical, metal, clothing, and chemical industries |
| Cities | Demographic Indicators | ||
|---|---|---|---|
| Post-Working Age Population per 100 People of Working Age | The Demographic Elderly Burden Factor | The Percentage of People Aged 65 and Older in the Total Population | |
| Białystok | 4.21% | 4.21% | 3.22% |
| Gdańsk | 3.58% | 4.41% | 3.17% |
| Gorzów Wlk. | 5.66% | 6.50% | 5.09% |
| Katowice | 3.77% | 4.06% | 2.99% |
| Kielce | 4.92% | 5.76% | 4.37% |
| Kraków | 3.20% | 3.65% | 2.60% |
| Lublin | 4.35% | 4.93% | 3.75% |
| Łódź | 4.34% | 5.07% | 3.66% |
| Olsztyn | 5.46% | 6.06% | 4.73% |
| Opole | 4.81% | 5.43% | 4.07% |
| Poznań | 4.21% | 5.19% | 3.85% |
| Rzeszów | 4.01% | 4.29% | 3.19% |
| Szczecin | 4.58% | 5.14% | 3.93% |
| Toruń | 5.10% | 5.80% | 4.55% |
| Warsaw | 2.68% | 3.09% | 1.96% |
| Wrocław | 3.72% | 4.38% | 3.11% |
| Cities | Medical Indicator | ||
|---|---|---|---|
| Physicians per 10,000 Residents | Nurses per 10,000 Residents | The Number of Hospital Beds per 10,000 Residents | |
| Białystok | 2.01% | 0.72% | −0.88% |
| Gdańsk | 2.37% | 0.55% | −0.09% |
| Gorzów Wlk. | 0.67% | −0.48% | 0.19% |
| Katowice | 2.92% | 1.20% | 0.49% |
| Kielce | 2.50% | 2.47% | −0.02% |
| Kraków | 2.45% | 2.02% | −0.41% |
| Lublin | 1.50% | 2.72% | 1.32% |
| Łódź | 2.25% | 2.28% | 0.31% |
| Olsztyn | 4.94% | 4.06% | 3.09% |
| Opole | 1.65% | 0.62% | −2.04% |
| Poznań | 3.03% | 0.86% | −0.65% |
| Rzeszów | 3.06% | 2.41% | 0.68% |
| Szczecin | 4.27% | 1.87% | 0.50% |
| Toruń | 3.64% | 0.08% | −0.03% |
| Warsaw | 1.95% | 1.37% | 1.07% |
| Wrocław | 4.07% | 2.31% | −0.29% |
| Cities | Demographic Indicators | Medical Indicator | ||||
|---|---|---|---|---|---|---|
| Elderly Burden Ratio Level | Elderly Burden Ratio Growth Rate | Physicians (Level/Rate of Change) | Nurses (Level/Rate of Change) | Beds (Level/Rate of Change) | Demographic Risk/Medical Resources | |
| Average Value for the Cities under Analysis (2020) | 32.80% | 4.87% | 59.60/2.70% | 115.2/1.56% | 85.5/0.2% | Not Applicable. |
| Białystok | low | average | average/low | low/low | average/negative | low/high |
| Gdańsk | average | average | low/average | low/low | low/negative | average/high |
| Gorzów Wlk. | average | high | low/low | low/negative | low/average | high/high |
| Katowice | high | average | high/high | high/low | high/high | high/low |
| Kielce | high | high | high/average | high/high | average/negative | high/high |
| Kraków | average | low | average/average | average/high | low/negative | low/average |
| Lublin | average | average | high/low | high/high | high/high | average/low |
| Łódź | high | high | average/low | average/high | average/high | high/average |
| Olsztyn | low | high | high/high | average/high | high/high | average/low |
| Opole | average | high | high/low | high/low | average/negative | high/average |
| Poznań | low | high | low/high | low/low | high/negative | average/high |
| Rzeszów | low | average | high/high | high/high | high/high | low/low |
| Szczecin | average | high | high/high | low/average | average/high | high/average |
| Toruń | average | high | low/high | low/low | low/negative | high/high |
| Warsaw | average | low | low/low | low/average | low/high | low/high |
| Wrocław | average | average | average/high | low/high | low/negative | average/average |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jonek-Kowalska, I. Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland. Smart Cities 2022, 5, 1267-1292. https://doi.org/10.3390/smartcities5040065
Jonek-Kowalska I. Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland. Smart Cities. 2022; 5(4):1267-1292. https://doi.org/10.3390/smartcities5040065
Chicago/Turabian StyleJonek-Kowalska, Izabela. 2022. "Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland" Smart Cities 5, no. 4: 1267-1292. https://doi.org/10.3390/smartcities5040065
APA StyleJonek-Kowalska, I. (2022). Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland. Smart Cities, 5(4), 1267-1292. https://doi.org/10.3390/smartcities5040065