
Trier Social Stress Test Elevates Blood Pressure, Heart Rate, and Anxiety, But a Singing Test or Unsolvable Anagrams Only Elevates Heart Rate, among Healthy Young Adults

Abstract
:1. Introduction
2. Materials and Methods
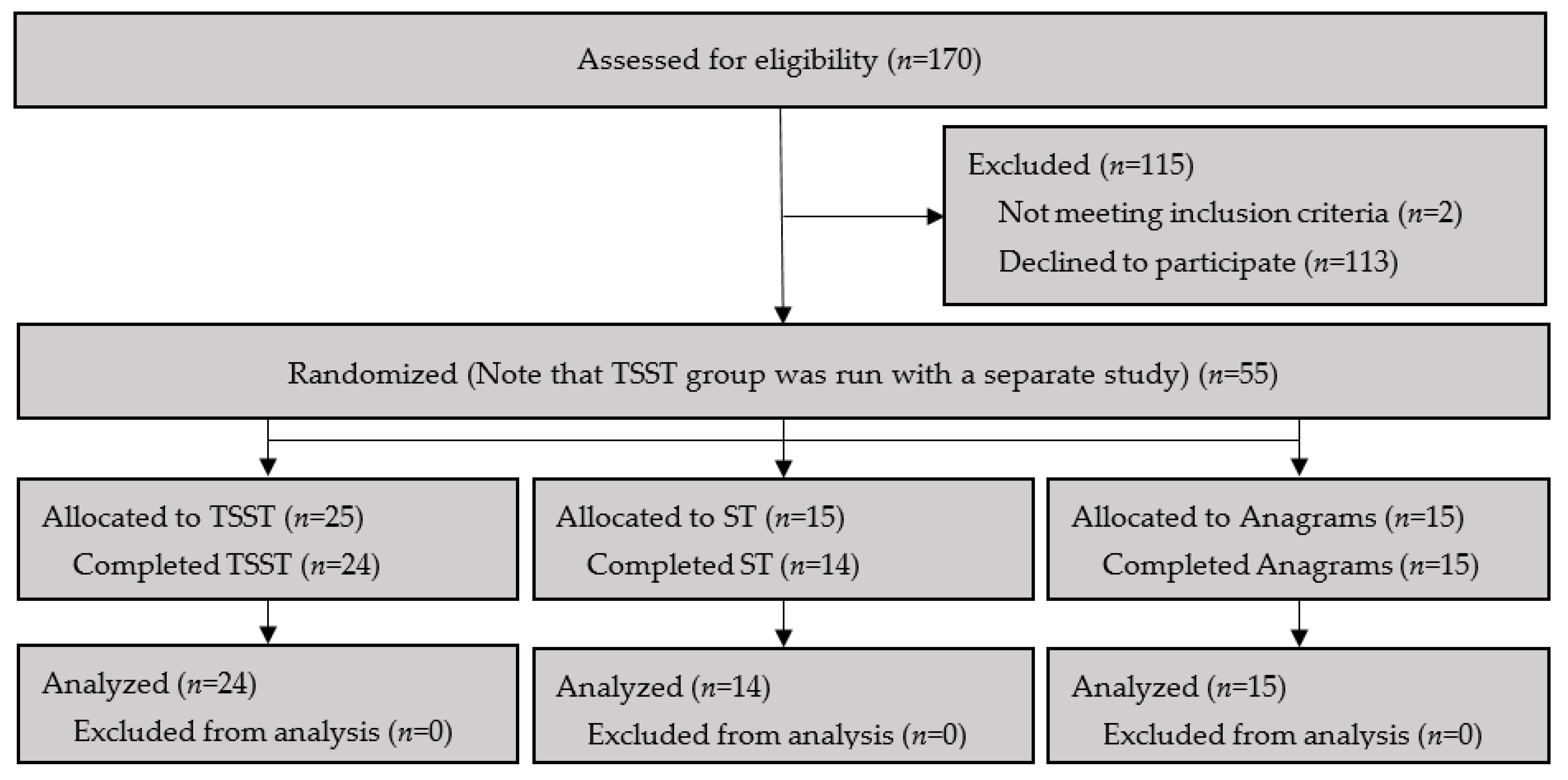
2.1. Participants
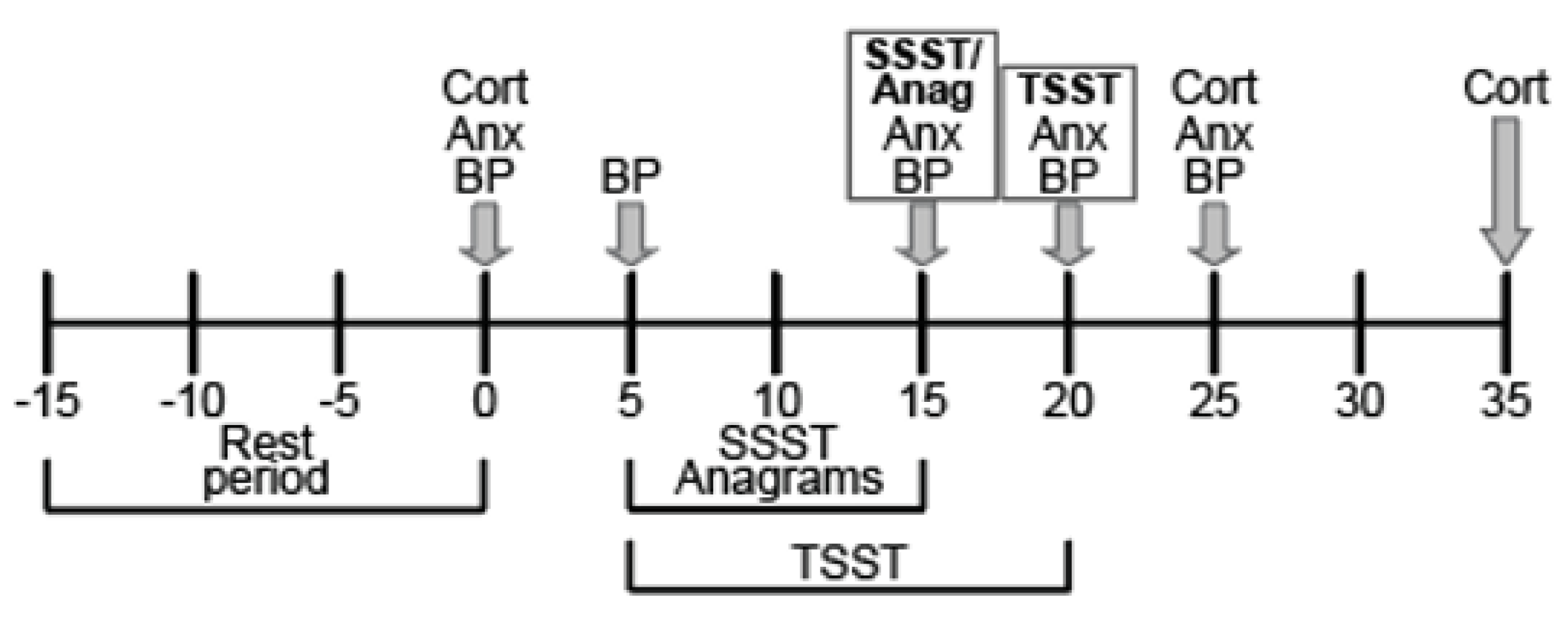
2.2. Experimental Design
2.2.1. Baseline Procedures
2.2.2. TSST Procedure
2.2.3. ST Procedure
2.2.4. Unsolvable Anagram Procedure
2.2.5. Post-Stressor Measurements
2.3. Measures
2.3.1. Cardiovascular Measures
2.3.2. Self-Rated Anxiety Measure
2.3.3. Salivary Cortisol Analysis
2.4. Statistics
3. Results
3.1. Participant Characteristics
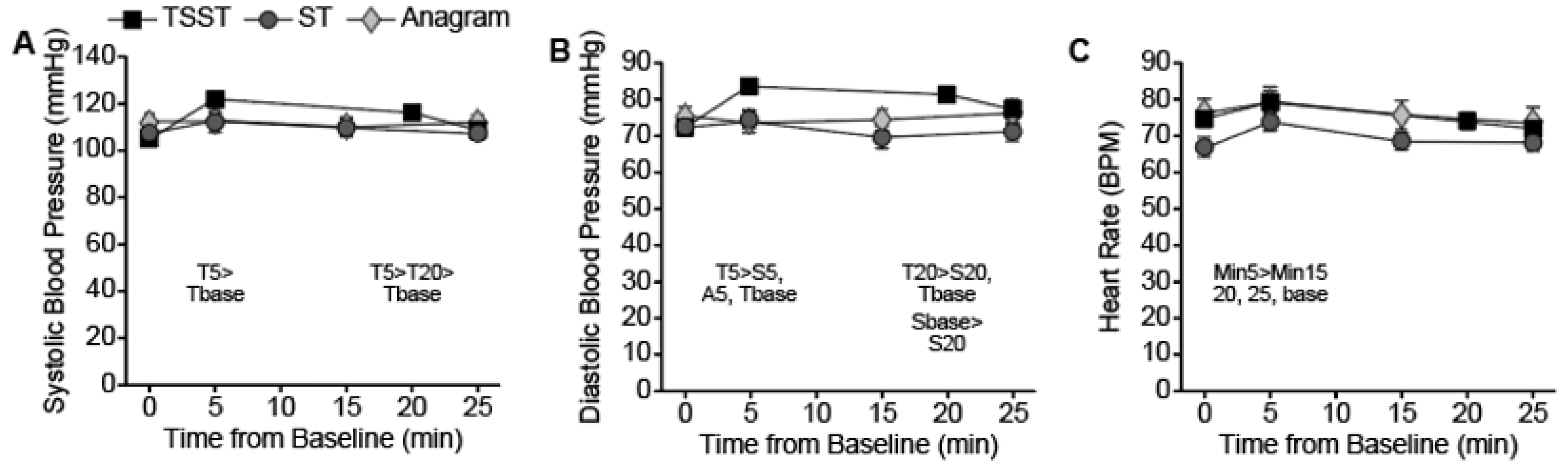
3.2. Cardiovascular Response to Stressors
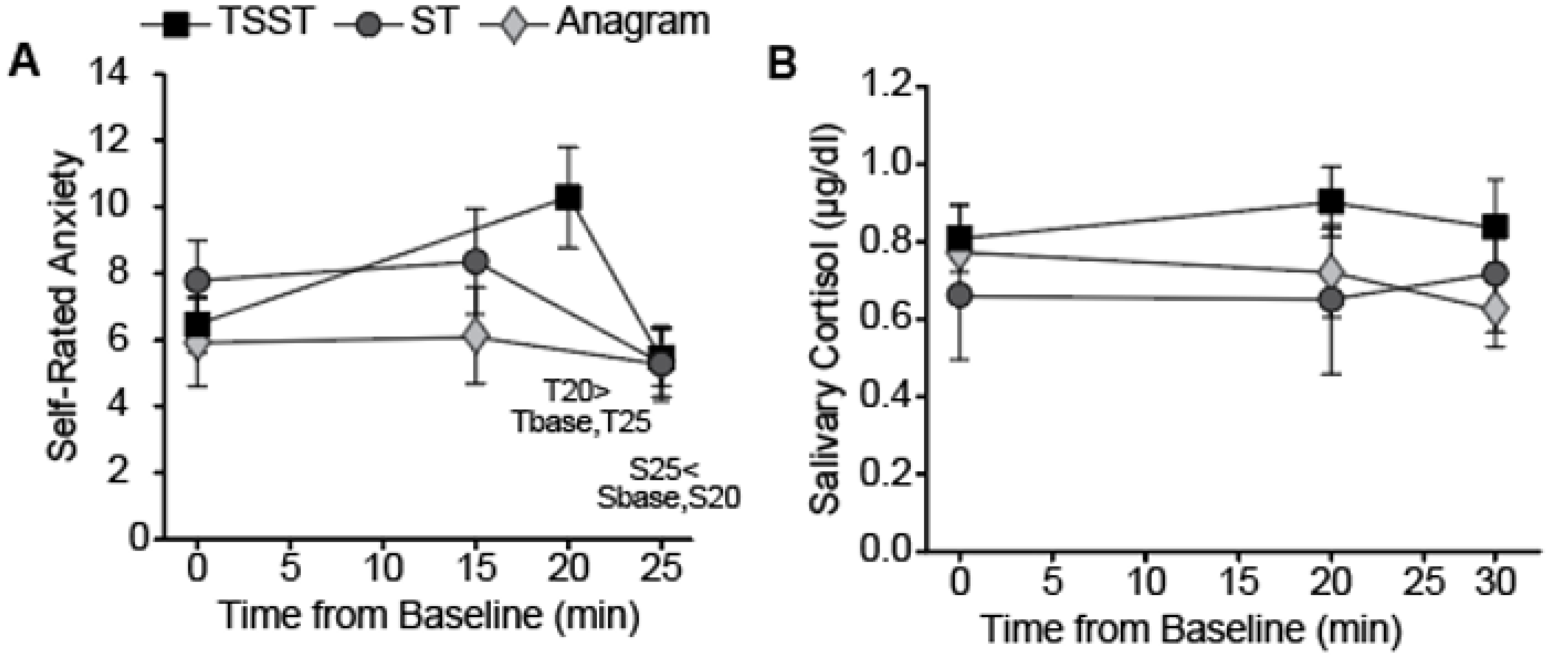
3.3. Self-Rated Anxiety in Response to Stressors
3.4. Salivary Cortisol in Response to Stressors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polivy, J.; Herman, C.P.; McFarlane, T. Effects of Anxiety on Eating: Does Palatability Moderate Distress-Induced Overeating in Dieters? J. Abnorm. Psychol. 1994, 103, 505–510. [Google Scholar] [CrossRef]
- Tryon, M.; DeCant, R.; Laugero, K. Having your cake and eating it too: A habit of comfort food may link chronic social stress exposure and acute stress-induced cortisol hyporesponsiveness. Physiol. Behav. 2013, 114–115, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Geliebter, A.; Gibson, C.D.; Hernandez, D.B.; Atalayer, D.; Kwon, A.; Lee, M.I.; Mehta, N.; Phair, D.; Gluck, M.E. Plasma cortisol levels in response to a cold pressor test did not predict appetite or ad libitum test meal intake in obese women. Appetite 2012, 59, 956–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwerdtfeger, A.; Rosenkaimer, A.-K. Depressive symptoms and attenuated physiological reactivity to laboratory stressors. Biol. Psychol. 2011, 87, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Pomidossi, G.; Casadei, R.; Ravogli, A.; Groppelli, A.; Cesana, B.; Mancia, G. Comparison of the cardiovascular effects of different laboratory stressors and their relationship with blood pressure variability. J. Hypertens. 1988, 6, 481–488. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Pirke, K.-M.; Hellhammer, D.H. The ‘Trier Social Stress Test’ – A Tool for Investigating Psychobiological Stress Responses in a Laboratory Setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.P.; Kennedy, P.J.; Cryan, J.F.; Dinan, T.; Clarke, G. Biological and psychological markers of stress in humans: Focus on the Trier Social Stress Test. Neurosci. Biobehav. Rev. 2014, 38, 94–124. [Google Scholar] [CrossRef]
- Epel, E.; Lapidus, R.; McEwen, B.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2001, 26, 37–49. [Google Scholar] [CrossRef]
- Helminen, E.C.; Morton, M.L.; Wang, Q.; Felver, J.C. A meta-analysis of cortisol reactivity to the Trier Social Stress Test in virtual environments. Psychoneuroendocrinology 2019, 110, 104437. [Google Scholar] [CrossRef]
- Kelly, O.; Matheson, K.; Martinez, A.; Merali, Z.; Anisman, H. Psychosocial Stress Evoked by a Virtual Audience: Relation to Neuroendocrine Activity. CyberPsychol. Behav. 2007, 10, 655–662. [Google Scholar] [CrossRef]
- Childs, E.; Vicini, L.M.; De Wit, H. Responses to the Trier Social Stress Test (TSST) in single versus grouped participants. Psychophysiology 2006, 43, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.T.; Crowell, M.D. Patterns of Autonomic Response During Laboratory Stressors. Psychophysiology 1989, 26, 603–614. [Google Scholar] [CrossRef]
- Giles, G.E.; Mahoney, C.R.; Brunyé, T.T.; Taylor, H.A.; Kanarek, R.B. Stress Effects on Mood, HPA Axis, and Autonomic Response: Comparison of Three Psychosocial Stress Paradigms. PLoS ONE 2014, 9, e113618. [Google Scholar] [CrossRef]
- Lustyk, K.; Olson, K.; Gerrish, W.; Holder, A.; Widman, L. Psychophysiological and neuroendocrine responses to laboratory stressors in women: Implications of mentrual cycle phase and stressor type. Biol. Psychol. 2010, 83, 84–92. [Google Scholar] [CrossRef]
- Skoluda, N.; Strahler, J.; Schlotz, W.; Niederberger, L.; Marques, S.; Fischer, S.; Thoma, M.; Spoerri, C.; Ehlert, U.; Nater, U. Intra-individual psychological and physiological responses to acute laboratory stressors of different intensity. Psychoneuroendocrinology 2015, 51, 227–236. [Google Scholar] [CrossRef]
- Brugnera, A.; Zarbo, C.; Tarvainen, M.P.; Marchettini, P.; Adorni, R.; Compare, A. Heart rate variability during acute psychosocial stress: A randomized cross-over trial of verbal and non-verbal laboratory stressors. Int. J. Psychophysiol. 2018, 127, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B. Memory and arithmetic as laboratory stressors for analyses of cardiovascular reactivity: A cursory assessment. Studia Psychol. 2001, 43, 3–11. [Google Scholar]
- Turner, J.R.; Carroll, U.; Dean, S.; Harris, M.G. Heart rate reactions to standard laboratory challenges and a naturalistic stressor. Int. J. Psychophysiol. 1987, 5, 151–152. [Google Scholar] [CrossRef]
- Royal, J.D.; Kurtz, J.L. I ate what?! The effect of stress and dispositional eating style on food intake and behavioral awareness. Personal. Individ. Differ. 2010, 49, 565–569. [Google Scholar] [CrossRef]
- Starcke, K.; Agorku, J.D.; Brand, M. Exposure to Unsolvable Anagrams Impairs Performance on the Iowa Gambling Task. Front. Behav. Neurosci. 2017, 11, 114. [Google Scholar] [CrossRef]
- Zellner, D.A.; Saito, S.; Gonzalez, J. The effect of stress on men’s food selection. Appetite 2007, 49, 696–699. [Google Scholar] [CrossRef]
- Messay, B.; Marsland, A.S.L. Goal adjustment ability predicts magnitude of emotional and physiological responses to an unsolvable anagram task. Personal. Individ. Differ. 2015, 86, 417–421. [Google Scholar] [CrossRef]
- Weidner, G.; Friend, R.; Ficarrotto, T.J.; Mendell, N.R. Hostility and cardiovascular reactivity to stress in women and men. Psychosom. Med. 1989, 51, 36–45. [Google Scholar] [CrossRef]
- Sigmon, S.T.; Pells, J.J.; Schartel, J.G.; Hermann, B.A.; Edenfield, T.M.; LaMattina, S.M.; Boulard, N.E.; Whitcomb-Smith, S.R. Stress reactivity and coping in seasonal and nonseasonal depression. Behav. Res. Ther. 2007, 45, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, S.S.; Kemeny, M.E. Acute Stressors and Cortisol Responses: A Theoretical Integration and Synthesis of Laboratory Research. Psychol. Bull. 2004, 130, 355–391. [Google Scholar] [CrossRef] [Green Version]
- Ebrouwer, A.-M.; Hogervorst, M.A. A new paradigm to induce mental stress: The Sing-a-Song Stress Test (SSST). Front. Neurosci. 2014, 8, 224. [Google Scholar] [CrossRef] [Green Version]
- Reschke-Hernández, A.E.; Okerstrom, K.L.; Edwards, A.B.; Tranel, D. Sex and stress: Men and women show different cortisol responses to psychological stress induced by the Trier social stress test and the Iowa singing social stress test. J. Neurosci. Res. 2017, 95, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Dickerson, S.S.; Mycek, P.J.; Zaldivar, F. Negative social evaluation, but not mere social presence, elicits cortisol responses to a laboratory stressor task. Health Psychol. 2008, 27, 116–121. [Google Scholar] [CrossRef]
- Klatzkin, R.R.; Gaffney, S.; Cyrus, K.; Bigus, E.; Brownley, K.A. Binge eating disorder and obesity: Preliminary evidence for distinct cardiovascular and psychological phenotypes. Physiol. Behav. 2015, 142, 20–27. [Google Scholar] [CrossRef]
- Zellner, D.A.; Loaiza, S.; Gonzalez, Z.; Pita, J.; Morales, J.; Pecora, D.; Wolf, A. Food selection changes under stress. Physiol. Behav. 2006, 87, 789–793. [Google Scholar] [CrossRef]
- Hostinar, C.E.; McQuillan, M.T.; Mirous, H.J.; Grant, K.E.; Adam, E.K. Cortisol responses to a group public speaking task for adolescents: Variations by age, gender, and race. Psychoneuroendocrinology 2014, 50, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, T.L.; Kemeny, M.E.; Aziz, N. Subjective social status moderates cortisol responses to social threat. Brain, Behav. Immun. 2006, 20, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Kudielka, B.M.; Gaab, J.; Schommer, N.C.; Hellhammer, D.H. Impact of Gender, Menstrual Cycle Phase, and Oral Contraceptives on the Activity of the Hypothalamus-Pituitary-Adrenal Axis. Psychosom. Med. 1999, 61, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Campisi, J.; Bravo, Y.; Cole, J.; Gobeil, K. Acute psychosocial stress differentially influences salivary endocrine and immune measures in undergraduate students. Physiol. Behav. 2012, 107, 317–321. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Dallman, M.F.; Epel, E.S. Comfort food is comforting to those most stressed: Evidence of the chronic stress response network in high stress women. Psychoneuroendocrinology 2011, 36, 1513–1519. [Google Scholar] [CrossRef] [Green Version]
- Geliebter, A.; Carnell, S.; E Gluck, M. Cortisol and ghrelin concentrations following a cold pressor stress test in overweight individuals with and without night eating. Int. J. Obes. 2013, 37, 1104–1108. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, T.L.; Kemeny, M.E.; Aziz, N.; Fahey, J.L. Acute Threat to the Social Self: Shame, Social Self-esteem, and Cortisol Activity. Psychosom. Med. 2004, 66, 915–924. [Google Scholar] [CrossRef] [Green Version]
- Schwabe, L.; Schächinger, H. Ten years of research with the Socially Evaluated Cold Pressor Test: Data from the past and guidelines for the future. Psychoneuroendocrinology 2018, 92, 155–161. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Characteristics | ||||
|---|---|---|---|---|
| Overall | TSST | ST | Anagrams | |
| Age in Years [Mean (SD)] | 21.9 (3.6) | 21.5 (3.9) | 22 (2.1) | 23.4 (4.2) |
| BMI (kg/m2) [Mean (SD)] | 27.4 (6.3) | 26.5 (7.0) | 26.4 (4.4) | 29.6 (6.4) |
| Females [N (%)] | 45 (84.9) | 21 (87.5) | 12 (85.7) | 12 (80) |
| Males [N (%)] | 8 (15.1) | 3 (12.5) | 2 (14.3) | 3 (20) |
| Ethnicity [N (% of condition)] | ||||
| Latinx | 8 (15) | 4 (16.7) | 3 (21.4) | 1 (6.7) |
| Race [N (% of condition)] | ||||
| Black/African American | 29 (55) | 13 (54.2) | 8 (57.1) | 8 (15.3) |
| White/Caucasian | 14 (26) | 4 (16.7) | 5 (35.7) | 5 (33.3) |
| Asian | 3 (6) | 2 (8.3) | 0 (0) | 1 (6.7) |
| Other/Unspecified Race | 7 (13) | 5 (20.8) | 1 (7.1) | 1 (6.7) |
| Measure | Cond | Baseline | Pre-Stress | Post-Stress 1 | Post-Stress 2 | Statistical Results |
|---|---|---|---|---|---|---|
| SBP M(SD) | TSST | 105 (12.2) | 121.8 (9.5) * | 116 (10.3) * | 108.8 (10.8) | CxT F(5.5, 110) = 4.5, p = 0.001; η2 = 22.4% |
| ST | 107.5 (10.9) | 112 (16.8) | 109.6 (14.5) | 107.3 (10.6) | ||
| Anag | 111.8 (14.8) | 112.6 (14.6) | 110.3 (14.3) | 111.9 (14.5) | ||
| DBP M(SD) | TSST | 72.3 (8.7) | 83.5 (9.3) * | 81.3 (10.5) * | 77.2 (13.3) | CxT F(4.9, 122.5) = 5.1, p < 0.001; η2 = 20.5%) |
| ST | 72.6 (10.2) | 74.5 (9.3) # | 69.5 (11.4) | 71.1 (10) | ||
| Anag | 75.4 (9.7) | 73.9 (12.1) # | 74.3 (11.3) | 76.3 (13.1) | ||
| HR M(SD) | TSST | 74.6 (11.3) | 79.3 (15.6) * | 74.1 (11.6) | 71.9 (12.4) | Main of T F(1.9, 96.4) = 11.2, p < 0.001; η2 = 22.3% |
| ST | 66.9 (10.3) | 73.9 (9.7) * | 68.6 (9.4) | 68.1 (8.7) | ||
| Anag | 76.5 (13.5) | 79.2 (16.6) * | 75.7 (15) | 73.8 (15.5) | ||
| Anx M(SD) | TSST | 6.4 (4.2) | 10.3 (7.6) * | 5.5 (4.2) | CxT F(3.5, 88.1) = 2.8, p = 0.04; η2 = 11.3% | |
| ST | 7.8 (4.5) | 8.4 (5.9) | 5.3 (4.2) * | |||
| Anag | 5.9 (4.1) | 6.1 (5.6) | 5.3 (4) | |||
| Cort M(SD) | TSST | 0.81 (0.4) | 0.9 (0.4) | 0.84 (0.6) | CxT ns F(3.2, 77.8) = 0.92, p = 0.44; η2 = 3.8% | |
| ST | 0.66 (0.6) | 0.65 (0.7) | 0.72 (0.6) | |||
| Anag | 0.77 (0.5) | 0.72 (0.4) | 0.63 (0.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sequeira, I.K.; Longmire, A.S.; McKay, N.J. Trier Social Stress Test Elevates Blood Pressure, Heart Rate, and Anxiety, But a Singing Test or Unsolvable Anagrams Only Elevates Heart Rate, among Healthy Young Adults. Psych 2021, 3, 171-183. https://doi.org/10.3390/psych3020015
Sequeira IK, Longmire AS, McKay NJ. Trier Social Stress Test Elevates Blood Pressure, Heart Rate, and Anxiety, But a Singing Test or Unsolvable Anagrams Only Elevates Heart Rate, among Healthy Young Adults. Psych. 2021; 3(2):171-183. https://doi.org/10.3390/psych3020015
Chicago/Turabian StyleSequeira, Isabelle K., Addie S. Longmire, and Naomi J. McKay. 2021. "Trier Social Stress Test Elevates Blood Pressure, Heart Rate, and Anxiety, But a Singing Test or Unsolvable Anagrams Only Elevates Heart Rate, among Healthy Young Adults" Psych 3, no. 2: 171-183. https://doi.org/10.3390/psych3020015
APA StyleSequeira, I. K., Longmire, A. S., & McKay, N. J. (2021). Trier Social Stress Test Elevates Blood Pressure, Heart Rate, and Anxiety, But a Singing Test or Unsolvable Anagrams Only Elevates Heart Rate, among Healthy Young Adults. Psych, 3(2), 171-183. https://doi.org/10.3390/psych3020015