
Explainable Artificial Intelligence (XAI): Concepts and Challenges in Healthcare


Abstract
:1. Introduction
2. Central Concepts of XAI
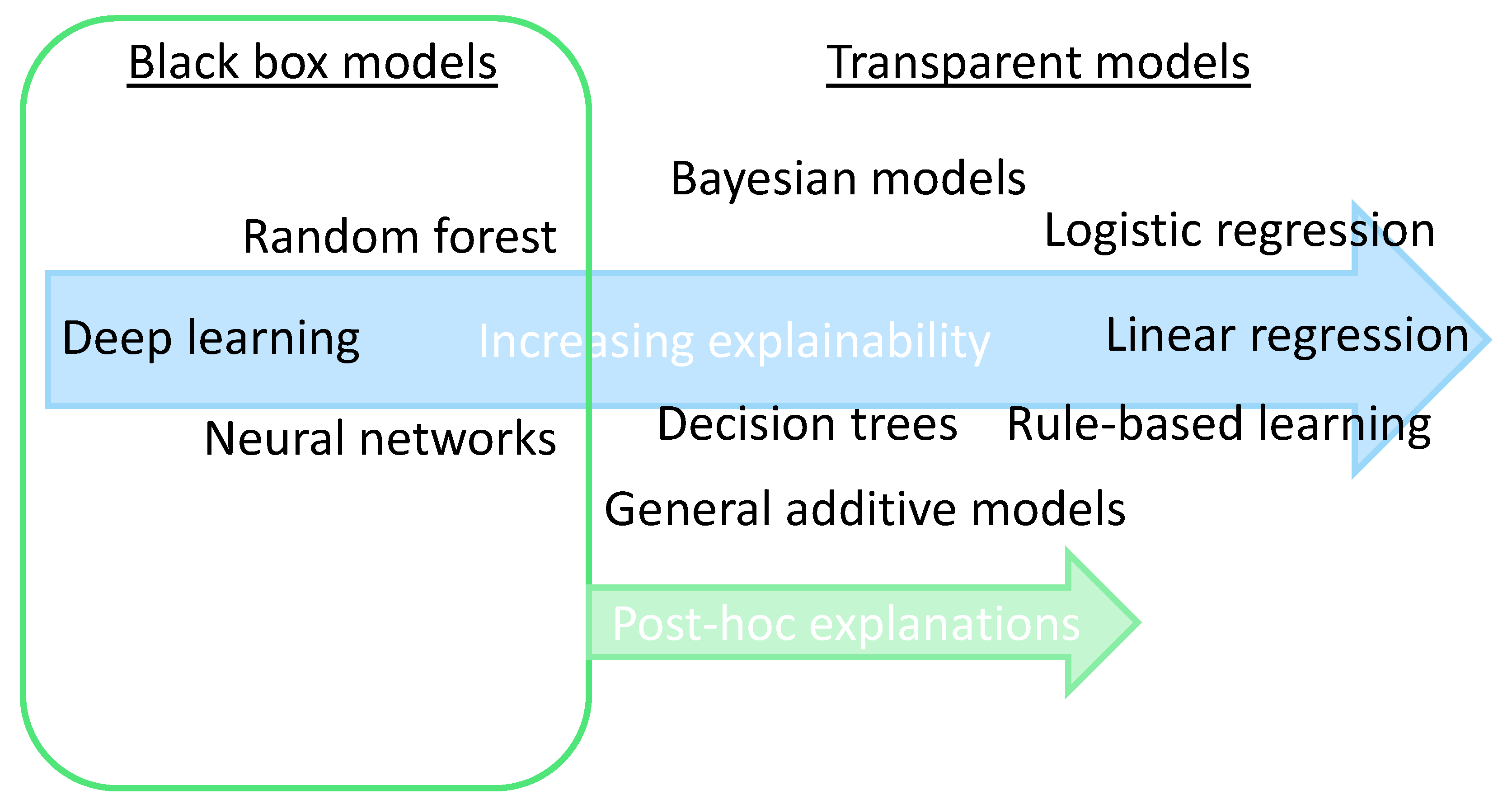
2.1. From “Black Box” to “(Translucent) Glass Box”
2.2. Explainability: Transparent or Post-Hoc
2.3. Collaboration between Humans and AI
2.4. Scientific Explainable Artificial Intelligence (sXAI)
2.5. Explanation Methods: Granular Computing (GrC) and Fuzzy Modeling (FM)
3. Challenges of XAI in Healthcare
3.1. Legal and Regulatory Compliance
3.2. Privacy and Security: A Mixed Bag
3.3. Do Explanations Always Raise Trust?
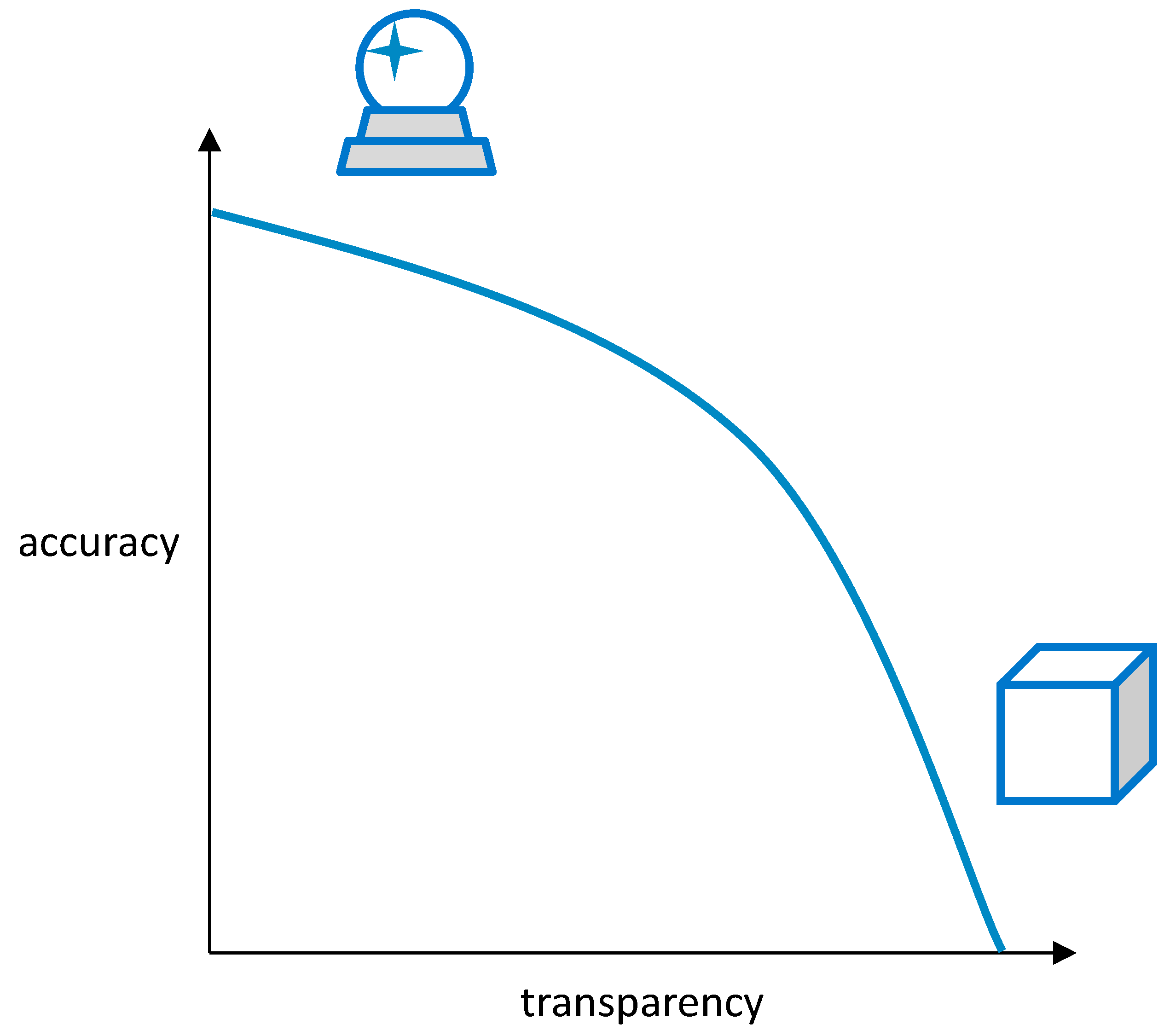
3.4. “Glass Box” vs. “Crystal Ball”: Balance between Explainability and Accuracy/Performance

3.5. How to Measure Explainability?
3.6. Increasing Complexity in the Future
4. Application Examples
5. Discussion
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| API | Application Programming Interface |
| AUC | Area Under the Curve |
| CDS | Clinical Decision Support |
| ChatGPT | Chat Generative Pre-trained Transformer |
| DBN | Deep Belief Network |
| DL | Deep Learning |
| FM | Fuzzy Modeling |
| GAN | Generative Adversarial Network |
| GDPR | General Data Protection Regulation |
| GrC | Granular Computing |
| HIPAA | Health Insurance Portability and Accountability Act |
| MAGDM | Multi-Attribute Group Decision Making |
| ML | Machine Learning |
| MR | Magnetic Resonance |
| NLP | Natural Language Processing |
| NN | Neural Networks |
| PIPL | Personal Information Protective Law |
| PPML | Privacy-Preserving Machine Learning |
| ROC | Receiver Operating Characteristic |
| sXAI | Scientific Explainable Artificial Intelligence |
| XAI | Explainable Artificial Intelligence |
| XSec | Explainable Security |
References
- Joiner, I.A. Chapter 1—Artificial intelligence: AI is nearby. In Emerging Library Technologies; Joiner, I.A., Ed.; Chandos Publishing: Oxford, UK, 2018; pp. 1–22. [Google Scholar]
- Hulsen, T. Literature analysis of artificial intelligence in biomedicine. Ann. Transl. Med. 2022, 10, 1284. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Hulsen, T.; Jamuar, S.S.; Moody, A.; Karnes, J.H.; Orsolya, V.; Hedensted, S.; Spreafico, R.; Hafler, D.A.; McKinney, E. From Big Data to Precision Medicine. Front. Med. 2019, 6, 34. [Google Scholar] [CrossRef] [Green Version]
- Hulsen, T.; Friedecký, D.; Renz, H.; Melis, E.; Vermeersch, P.; Fernandez-Calle, P. From big data to better patient outcomes. Clin. Chem. Lab. Med. (CCLM) 2022, 61, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S. ChatGPT and the Future of Medical Writing. Radiology 2023, 307, e223312. [Google Scholar] [CrossRef] [PubMed]
- Celi, L.A.; Cellini, J.; Charpignon, M.-L.; Dee, E.C.; Dernoncourt, F.; Eber, R.; Mitchell, W.G.; Moukheiber, L.; Schirmer, J.; Situ, J. Sources of bias in artificial intelligence that perpetuate healthcare disparities—A global review. PLoS Digit. Health 2022, 1, e0000022. [Google Scholar] [CrossRef]
- Hulsen, T. Sharing Is Caring-Data Sharing Initiatives in Healthcare. Int. J. Environ. Res. Public Health 2020, 17, 3046. [Google Scholar] [CrossRef]
- Vega-Márquez, B.; Rubio-Escudero, C.; Riquelme, J.C.; Nepomuceno-Chamorro, I. Creation of synthetic data with conditional generative adversarial networks. In Proceedings of the 14th International Conference on Soft Computing Models in Industrial and Environmental Applications (SOCO 2019), Seville, Spain, 13–15 May 2019; Springer: Cham, Switzerlnad, 2020; pp. 231–240. [Google Scholar]
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.Z. XAI-Explainable artificial intelligence. Sci. Robot. 2019, 4, eaay7120. [Google Scholar] [CrossRef] [Green Version]
- Vu, M.T.; Adalı, T.; Ba, D.; Buzsáki, G.; Carlson, D.; Heller, K.; Liston, C.; Rudin, C.; Sohal, V.S.; Widge, A.S.; et al. A Shared Vision for Machine Learning in Neuroscience. J. Neurosci. 2018, 38, 1601–1607. [Google Scholar] [CrossRef] [Green Version]
- Bharati, S.; Mondal, M.R.H.; Podder, P. A Review on Explainable Artificial Intelligence for Healthcare: Why, How, and When? IEEE Trans. Artif. Intell. 2023. [Google Scholar] [CrossRef]
- Sheu, R.-K.; Pardeshi, M.S. A Survey on Medical Explainable AI (XAI): Recent Progress, Explainability Approach, Human Interaction and Scoring System. Sensors 2022, 22, 8068. [Google Scholar] [CrossRef] [PubMed]
- Tjoa, E.; Guan, C. A survey on explainable artificial intelligence (xai): Toward medical xai. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 4793–4813. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Lee, H.; Jung, H.; Kim, H. Essential properties and explanation effectiveness of explainable artificial intelligence in healthcare: A systematic review. Heliyon 2023, 9, e16110. [Google Scholar] [CrossRef] [PubMed]
- Rai, A. Explainable AI: From black box to glass box. J. Acad. Mark. Sci. 2020, 48, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Loyola-Gonzalez, O. Black-box vs. white-box: Understanding their advantages and weaknesses from a practical point of view. IEEE Access 2019, 7, 154096–154113. [Google Scholar] [CrossRef]
- Ribeiro, M.T.; Singh, S.; Guestrin, C. Why should I trust you?: Explaining the predictions of any classifier. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 1135–1144. [Google Scholar] [CrossRef]
- Gerlings, J.; Jensen, M.S.; Shollo, A. Explainable AI, but explainable to whom? An exploratory case study of xAI in healthcare. In Handbook of Artificial Intelligence in Healthcare: Practicalities and Prospects; Lim, C.-P., Chen, Y.-W., Vaidya, A., Mahorkar, C., Jain, L.C., Eds.; Springer International Publishing: Cham, Switzeralnd, 2022; Volume 2, pp. 169–198. [Google Scholar]
- Arrieta, A.B.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; García, S.; Gil-López, S.; Molina, D.; Benjamins, R. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Phillips, P.J.; Hahn, C.A.; Fontana, P.C.; Broniatowski, D.A.; Przybocki, M.A. Four Principles of Explainable Artificial Intelligence; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2020; Volume 18. [Google Scholar]
- Vale, D.; El-Sharif, A.; Ali, M. Explainable artificial intelligence (XAI) post-hoc explainability methods: Risks and limitations in non-discrimination law. AI Ethics 2022, 2, 815–826. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Pradhan, K.B.; Bashar, M.A.; Tripathi, S.; Semwal, J.; Marzo, R.R.; Bhattacharya, S.; Singh, A. Artificial intelligence enabled healthcare: A hype, hope or harm. J. Fam. Med. Prim. Care 2019, 8, 3461–3464. [Google Scholar] [CrossRef]
- Zhang, Y.; Liao, Q.V.; Bellamy, R.K.E. Effect of Confidence and Explanation on Accuracy and Trust Calibration in AI-Assisted Decision Making. In Proceedings of the 2020 Conference on Fairness, Accountability, and Transparency, Barcelona, Spain, 27–30 January 2020; pp. 295–305. [Google Scholar] [CrossRef] [Green Version]
- Antoniadi, A.M.; Du, Y.; Guendouz, Y.; Wei, L.; Mazo, C.; Becker, B.A.; Mooney, C. Current Challenges and Future Opportunities for XAI in Machine Learning-Based Clinical Decision Support Systems: A Systematic Review. Appl. Sci. 2021, 11, 5088. [Google Scholar] [CrossRef]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I.; the Precise, Q.c. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef]
- Durán, J.M. Dissecting scientific explanation in AI (sXAI): A case for medicine and healthcare. Artif. Intell. 2021, 297, 103498. [Google Scholar] [CrossRef]
- Cabitza, F.; Campagner, A.; Malgieri, G.; Natali, C.; Schneeberger, D.; Stoeger, K.; Holzinger, A. Quod erat demonstrandum?—Towards a typology of the concept of explanation for the design of explainable AI. Expert Syst. Appl. 2023, 213, 118888. [Google Scholar] [CrossRef]
- Holzinger, A.; Saranti, A.; Molnar, C.; Biecek, P.; Samek, W. Explainable AI methods—A brief overview. In Proceedings of the xxAI—Beyond Explainable AI: International Workshop, Held in Conjunction with ICML 2020, Vienna, Austria, 12–18 July 2020; Holzinger, A., Goebel, R., Fong, R., Moon, T., Müller, K.-R., Samek, W., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 13–38. [Google Scholar]
- Bargiela, A.; Pedrycz, W. Human-Centric Information Processing through Granular Modelling; Springer Science & Business Media: Dordrecht, The Netherlands, 2009; Volume 182. [Google Scholar]
- Zadeh, L.A. Fuzzy sets and information granularity. In Fuzzy Sets, Fuzzy Logic, and Fuzzy Systems: Selected Papers; World Scientific: Singapore, 1979; pp. 433–448. [Google Scholar]
- Keet, C.M. Granular computing. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 849. [Google Scholar]
- Novák, V.; Perfilieva, I.; Dvořák, A. What is fuzzy modeling. In Insight into Fuzzy Modeling; John Wiley & Sons: Hoboken, NJ, USA, 2016; pp. 3–10. [Google Scholar]
- Mencar, C.; Alonso, J.M. Paving the way to explainable artificial intelligence with fuzzy modeling: Tutorial. In Proceedings of the Fuzzy Logic and Applications: 12th International Workshop (WILF 2018), Genoa, Italy, 6–7 September 2018; Springer International Publishing: Cham, Switzerland, 2019; pp. 215–227. [Google Scholar]
- Zhang, C.; Li, D.; Liang, J. Multi-granularity three-way decisions with adjustable hesitant fuzzy linguistic multigranulation decision-theoretic rough sets over two universes. Inf. Sci. 2020, 507, 665–683. [Google Scholar] [CrossRef]
- Zadeh, L.A. Toward a theory of fuzzy information granulation and its centrality in human reasoning and fuzzy logic. Fuzzy Sets Syst. 1997, 90, 111–127. [Google Scholar] [CrossRef]
- Zhang, C.; Li, D.; Liang, J.; Wang, B. MAGDM-oriented dual hesitant fuzzy multigranulation probabilistic models based on MULTIMOORA. Int. J. Mach. Learn. Cybern. 2021, 12, 1219–1241. [Google Scholar] [CrossRef]
- Zhang, C.; Ding, J.; Zhan, J.; Sangaiah, A.K.; Li, D. Fuzzy Intelligence Learning Based on Bounded Rationality in IoMT Systems: A Case Study in Parkinson’s Disease. IEEE Trans. Comput. Soc. Syst. 2022, 10, 1607–1621. [Google Scholar] [CrossRef]
- Solayman, S.; Aumi, S.A.; Mery, C.S.; Mubassir, M.; Khan, R. Automatic COVID-19 prediction using explainable machine learning techniques. Int. J. Cogn. Comput. Eng. 2023, 4, 36–46. [Google Scholar] [CrossRef]
- Gao, S.; Lima, D. A review of the application of deep learning in the detection of Alzheimer's disease. Int. J. Cogn. Comput. Eng. 2022, 3, 1–8. [Google Scholar] [CrossRef]
- Intersoft Consulting. Recital 58—The Principle of Transparency. Available online: https://gdpr-info.eu/recitals/no-58/ (accessed on 26 March 2023).
- Felzmann, H.; Villaronga, E.F.; Lutz, C.; Tamò-Larrieux, A. Transparency you can trust: Transparency requirements for artificial intelligence between legal norms and contextual concerns. Big Data Soc. 2019, 6, 2053951719860542. [Google Scholar] [CrossRef]
- Schneeberger, D.; Stöger, K.; Holzinger, A. The European legal framework for medical AI. In Proceedings of the International Cross-Domain Conference for Machine Learning and Knowledge Extraction, Dublin, Ireland, 25–28 August 2020; Springer: Cham, Switzerland, 2020; pp. 209–226. [Google Scholar]
- European Commission. On Artificial Intelligence—A European Approach to Excellence and Trust; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- European Commission. Proposal for a Regulation of the European Parliament and of the Council Laying Down Harmonised Rules on Artificial Intelligence (Artificial Intelligence Act) and Amending Certain Union Legislative Acts. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A52021PC0206 (accessed on 26 March 2023).
- Bell, A.; Nov, O.; Stoyanovich, J. Think about the Stakeholders First! Towards an Algorithmic Transparency Playbook for Regulatory Compliance. arXiv 2022, arXiv:2207.01482. [Google Scholar] [CrossRef]
- HHS Office for Civil Rights. Standards for privacy of individually identifiable health information—Final rule. Fed. Regist. 2002, 67, 53181–53273. [Google Scholar]
- HHS Office for Civil Rights. The HIPAA Privacy Rule and Electronic Health Information Exchange in a Networked Environment—Openness and Transparency. Available online: https://www.hhs.gov/sites/default/files/ocr/privacy/hipaa/understanding/special/healthit/opennesstransparency.pdf (accessed on 26 March 2023).
- Creemers, R.; Webster, G. Translation: Personal Information Protection Law of the People’s Republic of China—Effective 1 November 2021. Available online: https://digichina.stanford.edu/work/translation-personal-information-protection-law-of-the-peoples-republic-of-china-effective-nov-1-2021/ (accessed on 26 March 2023).
- Charmet, F.; Tanuwidjaja, H.C.; Ayoubi, S.; Gimenez, P.-F.; Han, Y.; Jmila, H.; Blanc, G.; Takahashi, T.; Zhang, Z. Explainable artificial intelligence for cybersecurity: A literature survey. Ann. Telecommun. 2022, 77, 789–812. [Google Scholar] [CrossRef]
- Tramèr, F.; Zhang, F.; Juels, A.; Reiter, M.K.; Ristenpart, T. Stealing machine learning models via prediction APIs. In Proceedings of the USENIX Security Symposium, Austin, TX, USA, 10–12 August 2016; pp. 601–618. [Google Scholar]
- Kaissis, G.A.; Makowski, M.R.; Rückert, D.; Braren, R.F. Secure, privacy-preserving and federated machine learning in medical imaging. Nat. Mach. Intell. 2020, 2, 305–311. [Google Scholar] [CrossRef]
- Saifullah, S.; Mercier, D.; Lucieri, A.; Dengel, A.; Ahmed, S. Privacy Meets Explainability: A Comprehensive Impact Benchmark. arXiv 2022, arXiv:2211.04110. [Google Scholar]
- Geyer, R.C.; Klein, T.; Nabi, M. Differentially private federated learning: A client level perspective. arXiv 2017, arXiv:1712.07557. [Google Scholar]
- Ivanovs, M.; Kadikis, R.; Ozols, K. Perturbation-based methods for explaining deep neural networks: A survey. Pattern Recognit. Lett. 2021, 150, 228–234. [Google Scholar] [CrossRef]
- Albahri, A.S.; Duhaim, A.M.; Fadhel, M.A.; Alnoor, A.; Baqer, N.S.; Alzubaidi, L.; Albahri, O.S.; Alamoodi, A.H.; Bai, J.; Salhi, A.; et al. A systematic review of trustworthy and explainable artificial intelligence in healthcare: Assessment of quality, bias risk, and data fusion. Inf. Fusion 2023, 96, 156–191. [Google Scholar] [CrossRef]
- Viganò, L.; Magazzeni, D. Explainable security. In Proceedings of the 2020 IEEE European Symposium on Security and Privacy Workshops (EuroS&PW), Genoa, Italy, 7–11 September 2020; pp. 293–300. [Google Scholar]
- Kuppa, A.; Le-Khac, N.A. Black Box Attacks on Explainable Artificial Intelligence(XAI) methods in Cyber Security. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar]
- Kiener, M. Artificial intelligence in medicine and the disclosure of risks. AI Soc. 2021, 36, 705–713. [Google Scholar] [CrossRef]
- Comiter, M. Attacking Artificial Intelligence AI’s Security Vulnerability and What Policymakers Can Do about It; Belfer Center for Science and International Affairs: Cambridge, MA, USA, 2019. [Google Scholar]
- Druce, J.; Harradon, M.; Tittle, J. Explainable artificial intelligence (XAI) for increasing user trust in deep reinforcement learning driven autonomous systems. arXiv 2021, arXiv:2106.03775. [Google Scholar]
- Le Merrer, E.; Trédan, G. Remote explainability faces the bouncer problem. Nat. Mach. Intell. 2020, 2, 529–539. [Google Scholar] [CrossRef]
- Guang, Y.; Qinghao, Y.; Jun, X. Unbox the black-box for the medical explainable AI via multi-modal and multi-centre data fusion: A mini-review, two showcases and beyond. Inf. Fusion 2022, 77, 29–52. [Google Scholar] [CrossRef]
- van der Veer, S.N.; Riste, L.; Cheraghi-Sohi, S.; Phipps, D.L.; Tully, M.P.; Bozentko, K.; Atwood, S.; Hubbard, A.; Wiper, C.; Oswald, M.; et al. Trading off accuracy and explainability in AI decision-making: Findings from 2 citizens’ juries. J. Am. Med. Inform. Assoc. 2021, 28, 2128–2138. [Google Scholar] [CrossRef]
- Sokol, K.; Flach, P. Explainability fact sheets: A framework for systematic assessment of explainable approaches. In Proceedings of the 2020 Conference on Fairness, Accountability, and Transparency, Barcelona, Spain, 27–30 January 2020; pp. 56–67. [Google Scholar]
- Lipton, Z.C. The Mythos of Model Interpretability: In Machine Learning, the Concept of Interpretability is Both Important and Slippery. Queue 2018, 16, 31–57. [Google Scholar] [CrossRef]
- Hoffman, R.R.; Mueller, S.T.; Klein, G.; Litman, J. Metrics for explainable AI: Challenges and prospects. arXiv 2018, arXiv:1812.04608. [Google Scholar]
- Klein, G.; Hoffman, R.R. Macrocognition, mental models, and cognitive task analysis methodology. In Naturalistic Decision Making and Macrocognition; Ashgate Publishing: Farnham, UK, 2008; pp. 57–80. [Google Scholar]
- Fauvel, K.; Masson, V.; Fromont, E. A performance-explainability framework to benchmark machine learning methods: Application to multivariate time series classifiers. arXiv 2020, arXiv:2005.14501. [Google Scholar]
- Larochelle, H.; Erhan, D.; Courville, A.; Bergstra, J.; Bengio, Y. An empirical evaluation of deep architectures on problems with many factors of variation. In Proceedings of the International Conference on Machine Learning (ICML ‘07), Corvallis, OR, USA, 20–24 June 2007; pp. 473–480. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial networks. Commun. ACM 2020, 63, 139–144. [Google Scholar] [CrossRef]
- Huynh, T.D.; Tsakalakis, N.; Helal, A.; Stalla-Bourdillon, S.; Moreau, L. Explainability-by-Design: A Methodology to Support Explanations in Decision-Making Systems. arXiv 2022, arXiv:2206.06251. [Google Scholar]
- Sarkar, A. Is explainable AI a race against model complexity? arXiv 2022, arXiv:2205.10119. [Google Scholar]
- van der Velden, B.H.M.; Kuijf, H.J.; Gilhuijs, K.G.A.; Viergever, M.A. Explainable artificial intelligence (XAI) in deep learning-based medical image analysis. Med. Image Anal. 2022, 79, 102470. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Vedaldi, A.; Zisserman, A. Deep inside convolutional networks: Visualising image classification models and saliency maps. arXiv 2013, arXiv:1312.6034. [Google Scholar]
- Chaddad, A.; Peng, J.; Xu, J.; Bouridane, A. Survey of Explainable AI Techniques in Healthcare. Sensors 2023, 23, 634. [Google Scholar] [CrossRef] [PubMed]
- Manresa-Yee, C.; Roig-Maimó, M.F.; Ramis, S.; Mas-Sansó, R. Advances in XAI: Explanation Interfaces in Healthcare. In Handbook of Artificial Intelligence in Healthcare: Practicalities and Prospects; Lim, C.-P., Chen, Y.-W., Vaidya, A., Mahorkar, C., Jain, L.C., Eds.; Springer International Publishing: Cham, Switzerland, 2022; Volume 2, pp. 357–369. [Google Scholar]
- Khodabandehloo, E.; Riboni, D.; Alimohammadi, A. HealthXAI: Collaborative and explainable AI for supporting early diagnosis of cognitive decline. Future Gener. Comput. Syst. 2021, 116, 168–189. [Google Scholar] [CrossRef]
- Joyce, D.W.; Kormilitzin, A.; Smith, K.A.; Cipriani, A. Explainable artificial intelligence for mental health through transparency and interpretability for understandability. NPJ Digit. Med. 2023, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Asan, O.; Bayrak, A.E.; Choudhury, A. Artificial Intelligence and Human Trust in Healthcare: Focus on Clinicians. J. Med. Internet Res. 2020, 22, e15154. [Google Scholar] [CrossRef] [PubMed]
- Marcus, G. The next decade in AI: Four steps towards robust artificial intelligence. arXiv 2020, arXiv:2002.06177. [Google Scholar]
- Das, A.; Rad, P. Opportunities and challenges in explainable artificial intelligence (xai): A survey. arXiv 2020, arXiv:2006.11371. [Google Scholar]
- Hulsen, T. The ten commandments of translational research informatics. Data Sci. 2019, 2, 341–352. [Google Scholar] [CrossRef]
- Harder, F.; Bauer, M.; Park, M. Interpretable and differentially private predictions. In Proceedings of the AAAI Conference on Artificial Intelligence, New York, NY, USA, 7–12 February 2020; pp. 4083–4090. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manuscript | Measures |
|---|---|
| Sokol and Flach (2020) [65] |
|
| Lipton (2018) [66] |
|
| Hoffman et al. (2018) [67] |
|
| Fauvel et al. (2020) [69] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hulsen, T. Explainable Artificial Intelligence (XAI): Concepts and Challenges in Healthcare. AI 2023, 4, 652-666. https://doi.org/10.3390/ai4030034
Hulsen T. Explainable Artificial Intelligence (XAI): Concepts and Challenges in Healthcare. AI. 2023; 4(3):652-666. https://doi.org/10.3390/ai4030034
Chicago/Turabian StyleHulsen, Tim. 2023. "Explainable Artificial Intelligence (XAI): Concepts and Challenges in Healthcare" AI 4, no. 3: 652-666. https://doi.org/10.3390/ai4030034
APA StyleHulsen, T. (2023). Explainable Artificial Intelligence (XAI): Concepts and Challenges in Healthcare. AI, 4(3), 652-666. https://doi.org/10.3390/ai4030034