
Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Methods
2.2.1. Laboratory Functional Testing
2.2.2. Statistical Analyses
3. Results
3.1. Clinical and Functional Characteristics Study Subjects
3.2. Correlation between Nasal FENO and the Anthropometric Characteristics of the Control Subjects and Clinical Symptoms in Patients with AR
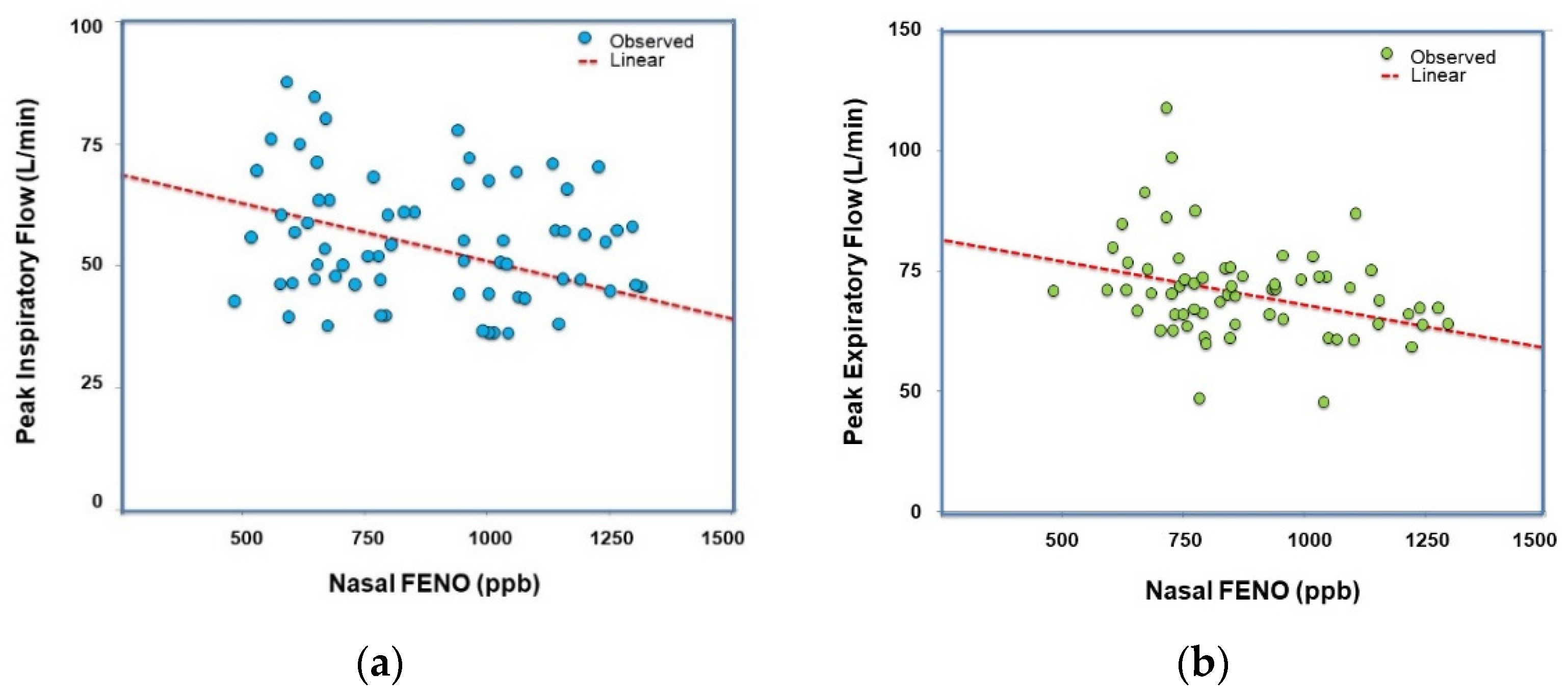
3.3. Correlation between Nasal FENO and Nasal Peak Flow of Study Subjects
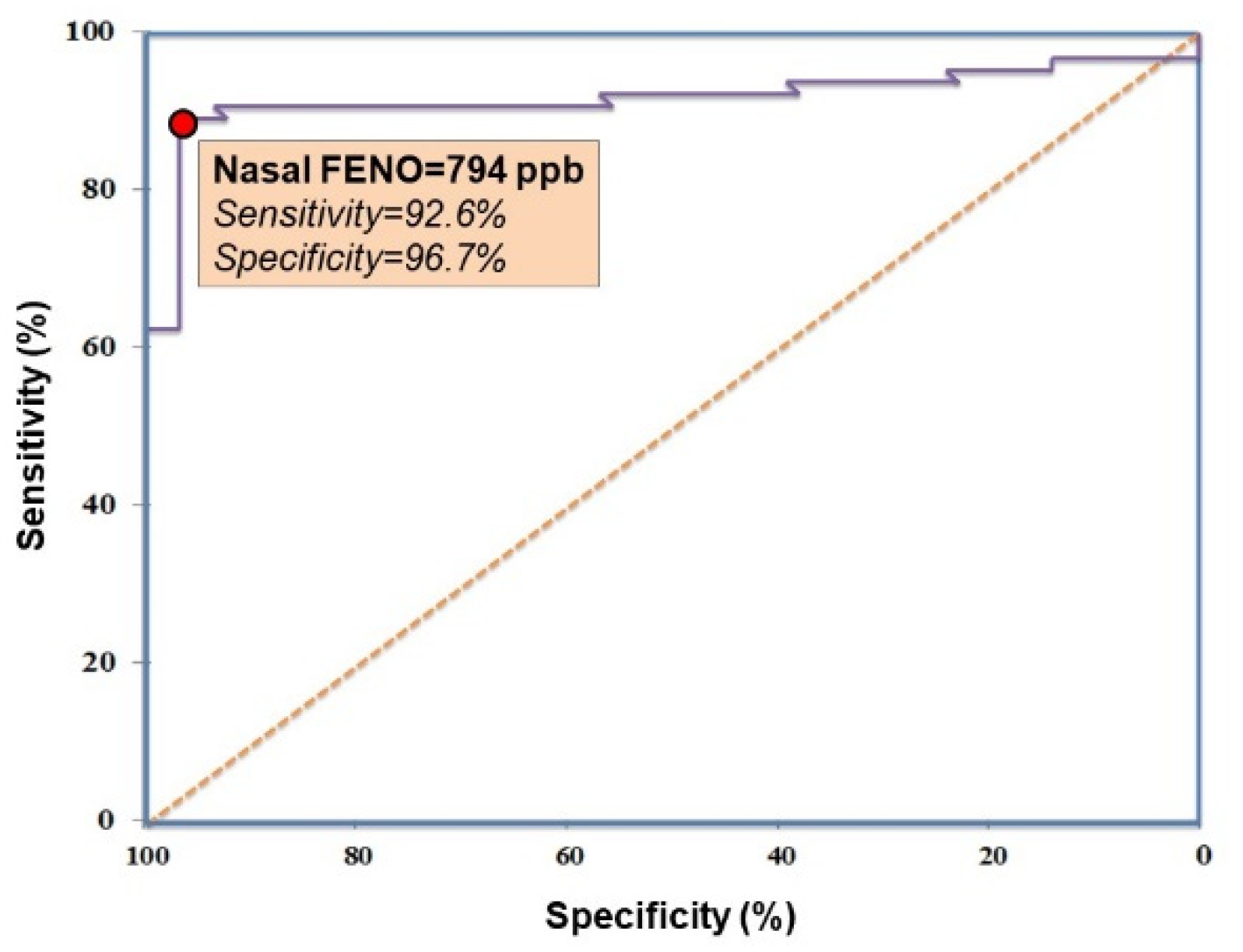
3.4. Cut-Off of Nasal FENO in the Diagnosis of AR in Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Weschta, M.; Deutschle, T.; Riechelmann, H. Nasal fractional exhaled nitric oxide analysis with a novel hand-held device. Rhinol. J. 2008, 46, 23–27. [Google Scholar]
- Bommarito, L.; Guida, G.; Heffler, E.; Badiu, I.; Nebiolo, F.; Usai, A.; De Stefani, A.; Rolla, G. Nasal nitric oxide concentration in suspected chronic rhinosinusitis. Ann. Allergy Asthma Immunol. 2008, 101, 358–362. [Google Scholar] [CrossRef]
- Duong-Quy, S. Clinical Utility Of The Exhaled Nitric Oxide (NO) Measurement With Portable Devices In The Management Of Allergic Airway Inflammation And Asthma. J. Asthma Allergy 2019, 12, 331–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zysman-Colman, Z.N.; Kaspy, K.R.; Alizadehfar, R.; Nykamp, K.R.; Zariwala, M.A.; Knowles, M.R.; Vinh, D.C.; Shapiro, A.J. Nasal Nitric Oxide in Primary Immunodeficiency and Primary Ciliary Dyskinesia: Helping to Distinguish Between Clinically Similar Diseases. J. Clin. Immunol. 2019, 39, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Mahut, B.; Escudier, E.; De Blic, J.; Zerah-Lancner, F.; Coste, A.; Harf, A.; Delclaux, C. Impairment of Nitric Oxide Output of Conducting Airways in Primary Ciliary Dyskinesia. Pediatr. Pulmonol. 2006, 41, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Degano, B.; Génestal, M.; Serrano, E.; Rami, J.; Arnal, J.-F. Effect of Treatment on Maxillary Sinus and Nasal Nitric Oxide Concentrations in Patients With Nosocomial Maxillary Sinusitis. Chest 2005, 128, 1699–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidman, M.D.; Gurgel, R.K.; Lin, S.Y.; Schwartz, S.R.; Baroody, F.M.; Bonner, J.R.; Dawson, D.E.; Dykewicz, M.S.; Hackell, J.M.; Han, J.K.; et al. Clinical practice guideline: Allergic rhinitis executive summary. Otolaryngol Head Neck Surg. 2015, 152, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.N.; Farkas-Szallasi, T.; Weitzberg, E.; Rinder, J.; Lidholm, J.; Änggåard, A.; Hökfelt, T.; Alving, K. High nitric oxide production in human paranasal sinuses. Nat. Med. 1995, 1, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.J.; Dell, S.D.; Gaston, B.; O’Connor, M.; Marozkina, N.; Manion, M.; Hazucha, M.J.; Leigh, M.W. Nasal Nitric Oxide Measurement in Primary Ciliary Dyskinesia. A Technical Paper on Standardized Testing Protocols. Ann. Am. Thorac. Soc. 2020, 17, e1–e12. [Google Scholar] [CrossRef] [PubMed]
- Vo-Thi-Kim, A.; Van-Quang, T.; Nguyen-Thanh, B.; Dao-Van, D.; Duong-Quy, S. The effect of medical treatment on nasal exhaled nitric oxide (NO) in patients with persistent allergic rhinitis: A randomized control study. Adv. Med. Sci. 2020, 65, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Schünemann, H.J.; Hellings, P.; Arnavielhe, S.; Bachert, C.; Bedbrook, A.; Bergmann, K.-C.; Bosnic-Anticevich, S.; Brozek, J.; Calderon, M.; et al. MACVIA clinical decision algorithm in adolescents and adults with allergic rhinitis. J. Allergy Clin. Immunol. 2016, 138, 367–374.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hood, C.M.; Schroter, R.C.; Doorly, D.J.; Blenke, E.J.S.M.; Tolley, N.S. Computational modeling of flow and gas exchange in models of the human maxillary sinus. J. Appl. Physiol. 2009, 107, 1195–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham Van, L.; Duong-Quy, S. Reference values of FENO in respiratory diseases: First large-scale study in Vietnam. J. Funct. Vent. Pulmonol. 2014, 5. [Google Scholar] [CrossRef]
- Society, A.T.; Society, E.R. ATS/ERS Recommendations for Standardized Procedures for the Online and Offline Measurement of Exhaled Lower Respiratory Nitric Oxide and Nasal Nitric Oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Duong-Quy, S.; Hua-Huy, T.; Tran-Mai-Thi, H.-T.; Le-Dong, N.-N.; Craig, T.J.; Dinh-Xuan, A.T. Study of Exhaled Nitric Oxide in Subjects with Suspected Obstructive Sleep Apnea: A Pilot Study in Vietnam. Pulm. Med. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang-Duc, H.; Pham-Huy, Q.; Vu-Minh, T.; Duong-Quy, S. Study of the Correlation between HRCT Semi-quantitative Scoring, Concentration of Alveolar Nitric Oxide, and Clinical-functional Parameters of Systemic Sclerosis-induced Interstitial Lung Disease. Yale J. Biol. Med. 2020, 93, 657–667. [Google Scholar] [PubMed]
- Duong-Quy, S.; Ngo-Minh, X.; Tang-Le-Quynh, T.; Tang-Thi-Thao, T.; Nguyen-Quoc, B.; Le-Quang, K.; Tran-Thanh, D.; Doan-Thi-Quynh, N.; Canty, E.; Do, T.; et al. The use of exhaled nitric oxide and peak expiratory flow to demonstrate improved breathability and antimicrobial properties of novel face mask made with sustainable filter paper and Folium Plectranthii amboinicii oil: Additional option for mask shortage during COVID-19 pandemic. Multidiscip. Respir. Med. 2020, 15, 664. [Google Scholar] [CrossRef] [PubMed]
- Duong-Quy, S.; Le-Thi-Minh, H.; Nguyen-Thi-Bich, H.; Pham-Thu, H.; Thom, V.; Pham-Thi-Hong, N.; Duong-Thi-Ly, H.; Nguyen-Huy, B.; Ngo-Minh, X.; Nguyen-Thi-Dieu, T.; et al. Correlations between exhaled nitric oxide, rs28364072 polymorphism of FCER2 gene, asthma control, and inhaled corticosteroid responsiveness in children with asthma. J. Breath Res. 2020, 15, 016012. [Google Scholar] [CrossRef] [PubMed]
- Dang-Thi-Mai, K.; Le-Dong, N.-N.; Le-Thuong, V.; Tran-Van, N.; Duong-Quy, S. Exhaled Nitric Oxide as a Surrogate Marker for Obstructive Sleep Apnea Severity Grading: An In-Hospital Population Study. Nat. Sci. Sleep 2021, 13, 763–773. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Study Subjects | Patients with AR | Control Subjects | p * |
|---|---|---|---|---|
| Number, subjects (%) | 100 (100.0) | 68 (68.0) | 32 (32.0) | - |
| Age, years | 14 ± 3 (6–17) | 14 ± 3 (6–17) | 13 ± 4 (6–17) | >0.05 |
| Sex, male/female | 1.5 | 1.6 | 1.4 | >0.05 |
| Height, cm | 135 ± 33 (99–169) | 134 ± 35 (99–169) | 136 ± 31 (105–167) | >0.05 |
| Weight, kg | 37 ± 19 (18–57) | 37 ± 18 (18–55) | 38 ± 19 (19–57) | >0.05 |
| BMI, kg/m2 | 16.8 ± 3.3 | 16.7 ± 3.4 | 16.9 ± 3.2 | >0.05 |
| Symptoms of AR | ||||
| Blocked nose, % | NA | 97.0 | 0.0 | NA |
| Itching and sneezing, % | NA | 100.0 | 0.0 | NA |
| Running nose, % | NA | 100.0 | 0.0 | NA |
| Nasal peak flow | ||||
| Peak inspiratory flow, L/min | 72 ± 22 | 67 ± 14 | 98 ± 26 | <0.01 |
| Peak expiratory flow, L/min | 107 ± 23 | 93 ± 24 | 124 ± 22 | <0.01 |
| Nasal FENO, ppb | 618 ± 395 (124–1385) | 985 ± 232 (526–1385) | 229 ± 65 (152–299) | <0.001 |
| Correlation | Anthropometric Parameters (Control Subjects; N = 32) | Symptoms of AR (AR Patients; N = 68) | ||||||
|---|---|---|---|---|---|---|---|---|
| Nasal FENO | Age | Sex | Height | Weight | BMI | Blocked Nose | Itching or Sneezing | Runny Nose |
| R | 0.098 | 0.325 | 0.094 | 0.082 | 0.076 | 0.356 | 0.679 | 0.587 |
| P | 0.124 | 0.079 | 0.141 | 0.325 | 0.328 | 0.001 | 0.0001 | 0.001 |
| Correlation | Control Subjects (N = 32) | AR Patients (N = 68) | ||
|---|---|---|---|---|
| Nasal FENO | Peak Inspiratory Flow | Peak Expiratory Flow | Peak Inspiratory Flow | Peak Expiratory Flow |
| R | 0.095 | 0.074 | −0.462 | −0.378 |
| P | 0.324 | 0.417 | 0.0012 | 0.0016 |
| Nasal FENO Cut-Off (ppb) | Sensitivity (%) | Specificity (%) | Youden Index |
|---|---|---|---|
| 732 | 94.2 | 77.3 | 172.189 |
| 738 | 94.2 | 81.2 | 176.213 |
| 740 | 94.2 | 83.3 | 178.431 |
| 744 | 94.2 | 86.1 | 180.346 |
| 749 | 94.2 | 89.0 | 183.890 |
| 754 | 93.7 | 93.2 | 187.465 |
| 760 | 92.4 | 93.1 | 186.767 |
| 794 | 92.6 | 96.7 | 189.234 |
| 863 | 91.7 | 95.6 | 188.673 |
| 899 | 91.4 | 95.6 | 188.348 |
| 905 | 90.2 | 95.6 | 187.560 |
| 916 | 89.8 | 95.6 | 186.134 |
| 938 | 88.2 | 95.6 | 185.778 |
| 945 | 88.1 | 95.6 | 184.657 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duong-Quy, S.; Nguyen-Thi-Dieu, T.; Tran-Quang, K.; Tang-Thi-Thao, T.; Nguyen-Van, T.; Vo-Pham-Minh, T.; Vu-Tran-Thien, Q.; Bui-Diem, K.; Nguyen-Nhu, V.; Hoang-Thi, L.; et al. Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis. Sinusitis 2021, 5, 123-131. https://doi.org/10.3390/sinusitis5020013
Duong-Quy S, Nguyen-Thi-Dieu T, Tran-Quang K, Tang-Thi-Thao T, Nguyen-Van T, Vo-Pham-Minh T, Vu-Tran-Thien Q, Bui-Diem K, Nguyen-Nhu V, Hoang-Thi L, et al. Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis. Sinusitis. 2021; 5(2):123-131. https://doi.org/10.3390/sinusitis5020013
Chicago/Turabian StyleDuong-Quy, Sy, Thuy Nguyen-Thi-Dieu, Khai Tran-Quang, Tram Tang-Thi-Thao, Toi Nguyen-Van, Thu Vo-Pham-Minh, Quan Vu-Tran-Thien, Khue Bui-Diem, Vinh Nguyen-Nhu, Lam Hoang-Thi, and et al. 2021. "Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis" Sinusitis 5, no. 2: 123-131. https://doi.org/10.3390/sinusitis5020013
APA StyleDuong-Quy, S., Nguyen-Thi-Dieu, T., Tran-Quang, K., Tang-Thi-Thao, T., Nguyen-Van, T., Vo-Pham-Minh, T., Vu-Tran-Thien, Q., Bui-Diem, K., Nguyen-Nhu, V., Hoang-Thi, L., & Craig, T. (2021). Study of Nasal Fractional Exhaled Nitric Oxide (FENO) in Children with Allergic Rhinitis. Sinusitis, 5(2), 123-131. https://doi.org/10.3390/sinusitis5020013